Differences between WHO Growth Standards and China Growth Standards in Assessing the Nutritional Status of Children Aged 0–36 Months Old

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
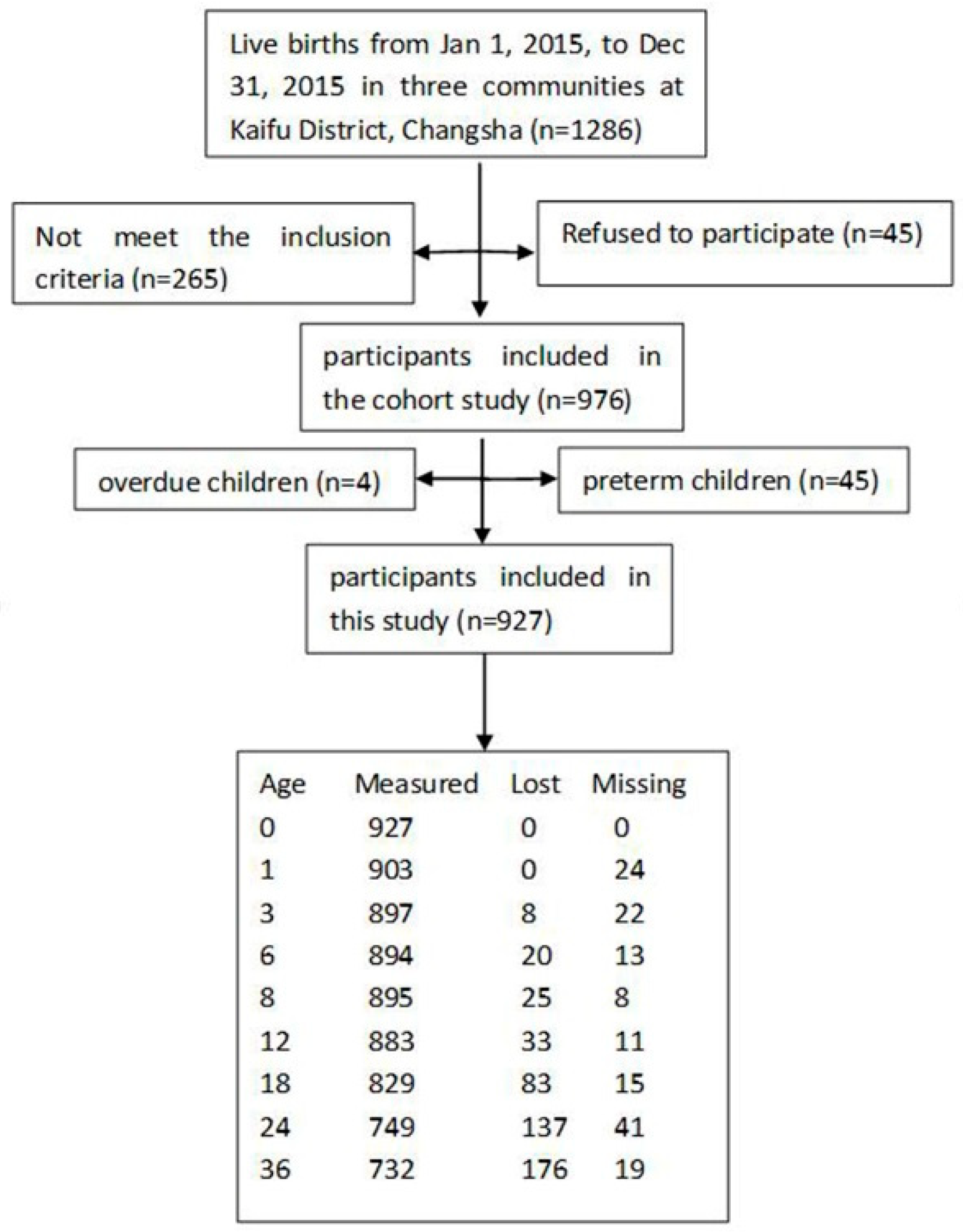
2.1. Study Design and Population
2.2. Data Collection and Calculation
2.3. Definitions
2.4. Statistical Analysis
2.5. Ethical Considerations
3. Results
3.1. Weight and Length/Height
3.2. Z-Scores
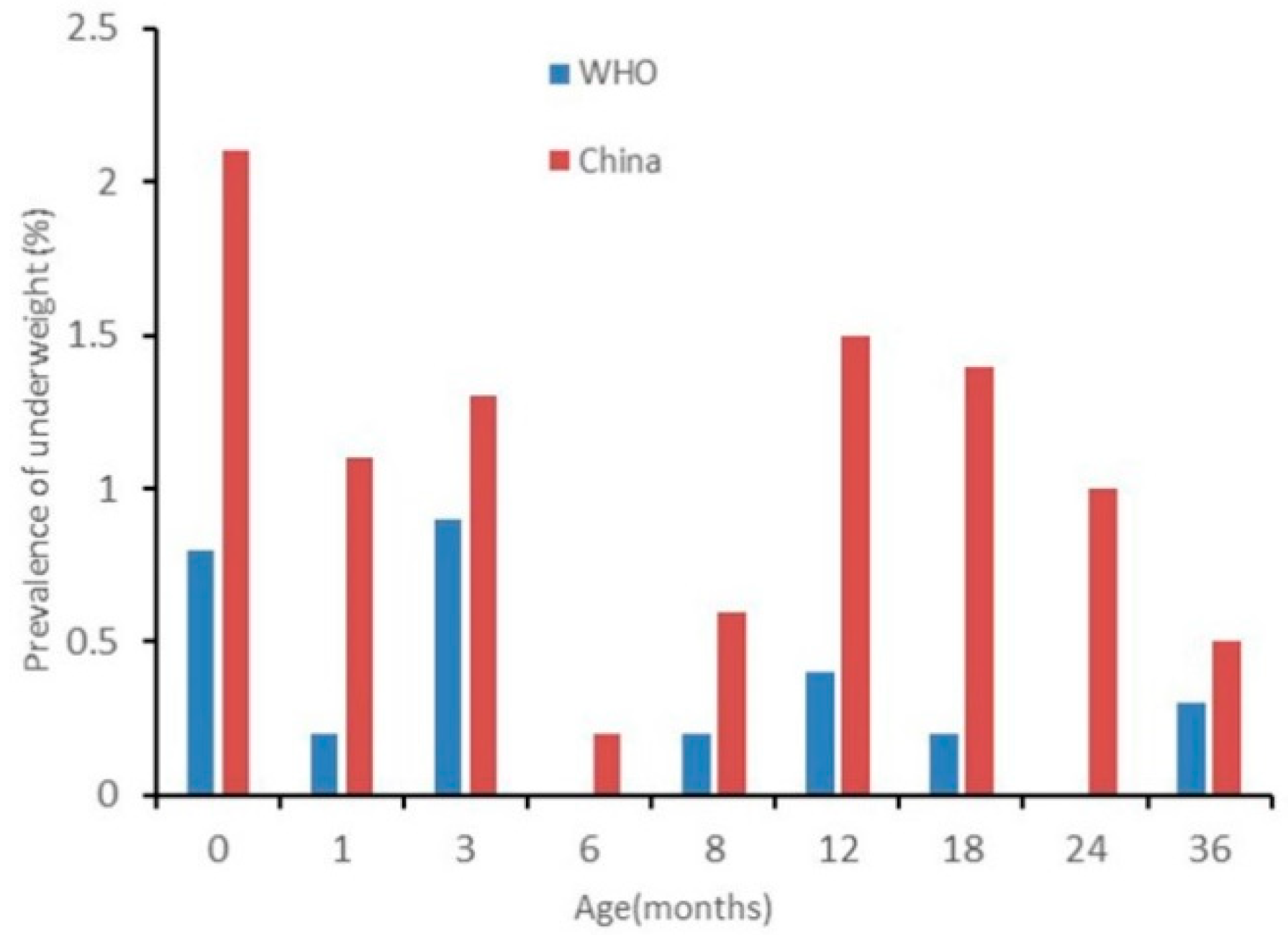
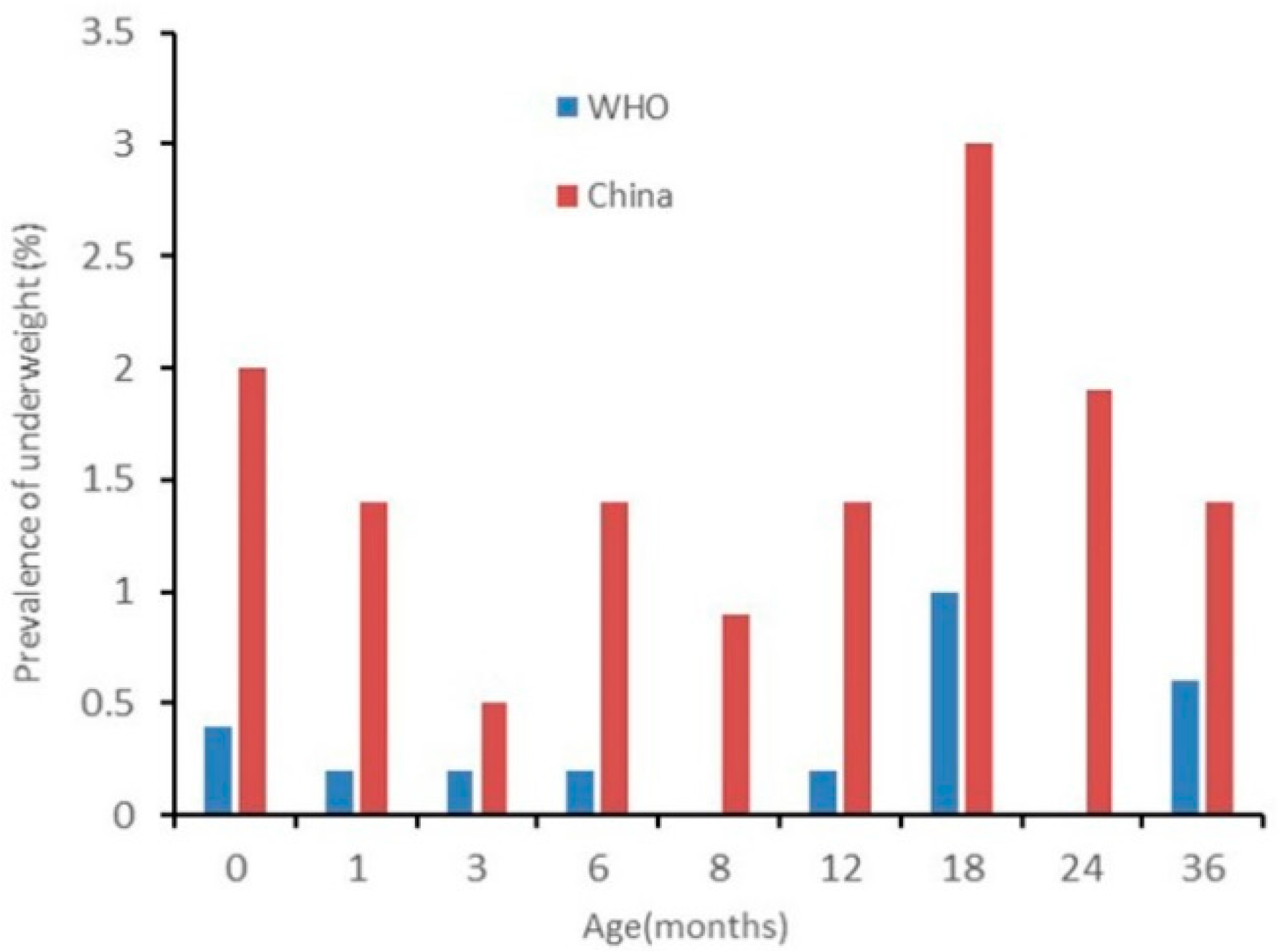
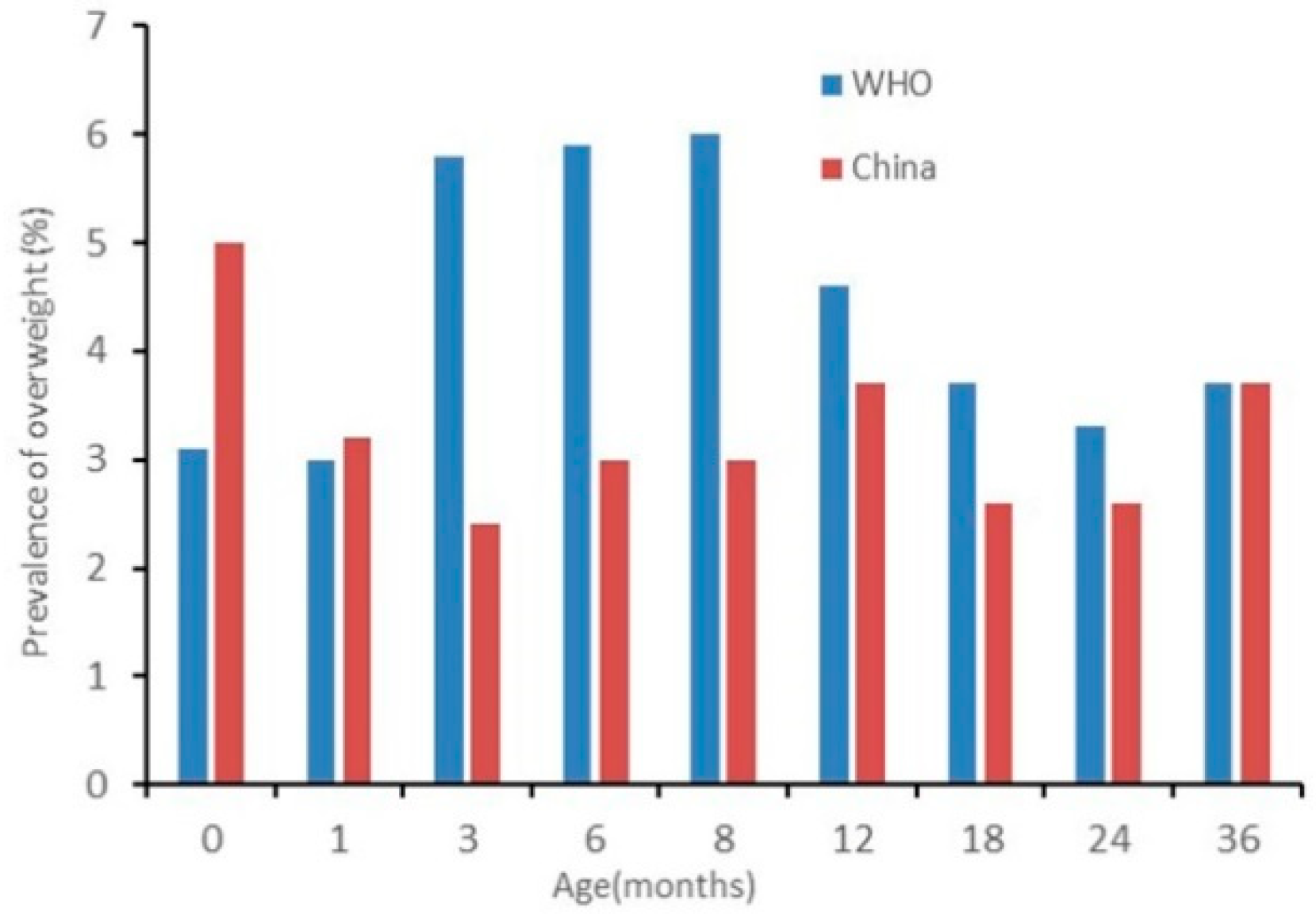
3.3. Nutrition Status
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- WHO. Levels and Trends in Child Malnutrition; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- Bhandari, N.; de Onis, M. The current status of international standards for child growth. Indian J. Med. Res. 2007, 126, 94–96. [Google Scholar] [PubMed]
- WHO Multicentre Growth Reference Study Group. WHO Child Growth Standards: Length/Height-Forage, Weight-for-Age, Weight-for-Length, Weight-for-Height, and Body Mass Index-for-Age: Methods and Development; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- Martinez-Millana, A.; Hulst, J.M.; Boon, M.; Witters, P.; Fernandez-Llatas, C.; Asseiceira, I.; Calvo-Lerma, J.; Basagoiti, I.; Traver, V.; de Boeck, K.; et al. Optimisation of children z-score calculation based on new statistical techniques. PLoS ONE 2018, 13, e0208362. [Google Scholar] [CrossRef] [PubMed]
- Mei, Z.; Grummer-Strawn, L.M. Standard deviation of anthropometric Z-scores as a data quality assessment tool using 2006 WHO growth standards: A cross country analysis. Bull. World Health Organ. 2007, 85, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Ye, G. Children’s Juvenile Hygiene; Version 4; People’s Health Publishing House: Beijing, China, 2001; p. 57. [Google Scholar]
- Garza, C.; de Onis, M. Rationale for developing a new international growth reference. Food Nutr. Bull. 2004, 25, S5–S14. [Google Scholar] [CrossRef] [PubMed]
- Department of Maternal and Child Health and Community Health, Ministry of Health. Growth Standard and Growth Curve of Chinese Children; Second military Medical University Press: Shanghai, China, 2009; pp. 36–140. [Google Scholar]
- Garza, C.; Onyango, A.W.; Rolland-Cachera, M.F. WHO growth standards for infants and young children. Arch. Pediatr. 2009, 16, 47–53. [Google Scholar]
- Wang, Y.; Chen, C.; He, W. Analysis of children’s nutritional status based on WHO children growth standard in China. Wei Sheng Yan Jiu 2007, 36, 203–206. [Google Scholar]
- WHO Working Group on the Growth Reference Protocol and WHO Task Force on Methods for the Natural Regulation of Fertility. Growth patterns of breastfed infants in seven countries. Acta Paediatr. 2000, 89, 215–222. [Google Scholar] [CrossRef]
- Huang, X.; Chang, J.; Feng, W.; Xu, Y.; Xu, T.; Tang, H.; Wang, H.; Pan, X. Development of a New Growth Standard for Breastfed Chinese Infants: What Is the Difference from the WHO Growth Standards? PLoS ONE 2016, 11, e0167816. [Google Scholar] [CrossRef]
- Zong, X.; Li, H.; Zhu, Z. Secular trends in height and weight for healthy Han children aged 0 to 7 years in China, 1975–2005. Am. J. Hum. Biol. 2011, 23, 209–215. [Google Scholar] [CrossRef]
- Zhang, Y.Q.; Li, H.; Wu, H.H.; Zong, X.N. Secular trends in weight, height and weight for height among children under 7 years in nine cities of China, 1975–2015: Results from five repeated cross-sectional surveys. BMJ Open 2019, 9, e029201. [Google Scholar] [CrossRef]
- Institute of Pediatrics of Chinese Academy of Medical Sciences. The first national survey of Chinese children and adolescents 0–18 years in 1975. Natl. Med. J. China 1977, 57, 720–725. [Google Scholar]
- Zhang, Y.Q.; Li, H.; Wu, H.H.; Zong, X.N.; Zhu, Z.H.; Pan, Y.; Li, J.; Zheng, X.-R.; Wei, M.; Tong, M.-L.; et al. The 5th national survey on the physical growth and development of children in the nine cities of China: Anthropometric measurements of Chinese children under 7 years in 2015. Am. J. Phys. Anthropol. 2017, 163, 497–509. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Ji, C.Y.; Zong, X.N.; Zhang, Y.Q. Height and weight standardized growth charts for Chinese children and adolescents aged 0 to 18years. Zhonghua Er Ke Za Zhi 2009, 47, 487–492. [Google Scholar] [PubMed]
- Li, H.; Capital Institute of Pediatrics, Coordinating Study Group of Nine Cities on the Physical Growth and Development of Children. Growth standardized values and curves based on weight, length/height and head circumference for Chinese children under 7 years of age. Zhonghua Er Ke Za Zhi 2009, 47, 173–178. [Google Scholar] [PubMed]
- Coordinating Study Group of Nine Cities on Physical Growth and Development of Children. Capital Institute of Pediatrics. A national survey on growth of children under 7 years of age in nine cities of China, 2005. Zhonghua Er Ke Za Zhi 2007, 45, 609–614. [Google Scholar]
- Onis, M.; Onyango, A. The Centers for Disease Control and Prevention 2000 growth charts and the growth of breastfed infants. Acta Paediatr. 2007, 92, 413–419. [Google Scholar] [CrossRef]
- Department of Health and Human Services. 2000 CDC Growth Charts for the United States: Methods and Development; Centers for Disease Control and Prevention: Hyattsville, MD, USA, 2000. [Google Scholar]
- World Health Organization. The WHO Child Growth Standards [EB/OL]. Available online: http://www.who.int/childgrowth/standards/en/ (accessed on 1 July 2016).
- Natale, V.; Rajagopalan, A. Worldwide variation in human growth and the World Health Organization growth standards: A systematic review. BMJ Open 2014, 4, e003735. [Google Scholar] [CrossRef]
- Roelants, M.; Hauspie, R.; Hoppenbrouwers, K. Breastfeeding, growth and growth standards: Performance of the WHO growth standards for monitoring growth of Belgian children. Ann. Hum. Biol. 2010, 37, 2–9. [Google Scholar] [CrossRef]
- De Onis, M.; Onyango, A.; Borghi, E.; Siyam, A.; Blössner, M.; Lutter, C. Worldwide implementation of the WHO Growth Standards. Public Health Nutr. 2012, 15, 1603–1610. [Google Scholar] [CrossRef]
- Kalatozishvili, P.; Davituliani, N.; Phagava, H.; Beridze, V.; Pagava, K. Physical development of children in orphanages. Georgian Med. News 2016, 256–257, 67–71. [Google Scholar]
- El Mouzan, M.I.; Shaffi, A.; Salloum, A.A.; Alqurashi, M.M.; Al Herbish, A.; Al Omer, A. Z-score growth reference data for Saudi preschool children. Ann. Saudi Med. 2017, 37, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H.; Ishii, H.; Yamada, T.; Akazawa, K.; Nagata, S.; Yamashiro, Y. Growth of Japanese breastfed infants compared to national references and World Health Organization growth standards. Acta Paediatr. 2013, 102, 739–743. [Google Scholar] [CrossRef] [PubMed]
- Inokuchi, M.; Matsuo, N.; Takayama, J.I.; Hasegawa, T. WHO 2006 Child Growth Standards overestimate short stature and underestimate overweight in Japanese children. J. Pediatr. Endocrinol. Metab. 2018, 31, 33–38. [Google Scholar] [CrossRef]
- Juliusson, P.B.; Roelants, M.; Hoppenbrouwers, K.; Hauspie, R.; Bjerknes, R. Growth of Belgian and Norwegian children compared to the WHO growth standards: Prevalence below −2 SD and above +2 SD and the effect of breastfeeding. Arch. Dis. Child. 2011, 96, 916–921. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Duan, Y.; Ma, G.; Yang, X.; Yin, S. Comparison of the China growth charts with the WHO growth standards in assessing malnutrition of Children. BMJ Open 2015, 5, e006107. [Google Scholar] [CrossRef] [PubMed]
- Vignerová, J.; Shriver, L.; Paulová, M.; Brabec, M.; Procházka, B.; Riedlová, J. Growth of Czech Breastfed Infants in Comparison with the Health Organization Standards. Cent. Eur. J. Public Health 2015, 23, 32–38. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Noël, C.; Nicola, L.H. Should the UK use WHO growth charts? Paediatr. Child Health 2010, 20, 151–156. [Google Scholar]
- Grummer-Strawn, L.M.; Reinold, C.; Krehs, N.F. Use of World Health Organization and CDC Growth Charts for Children Aged 0–59 Months in the United States. MMWR Recomm. Rep. 2010, 59, 1–14. [Google Scholar]
- Meyers, A.; Joyce, K.; Coleman, S.M.; Cook, J.T.; Cutts, D.; de Cuba, S.E.; Heeren, T.C.; Rose-Jacobs, R.; Black, M.M.; Casey, P.H.; et al. Health of children classified as underweight by CDC reference but normal by WHO standard. Pediatrics 2013, 131, e1780–e1787. [Google Scholar] [CrossRef]
- Kuczmarski, R.J.; Ogden, C.L.; Guo, S.S.; Grummer-Strawn, L.M.; Flegal, K.M.; Mei, Z.; Wei, R.; Curtin, L.R.; Roche, A.F.; Johnson, C.L. 2000 CDC Growth Charts for the United States: Methods and development. Vital Health Stat. 2002, 246, 1–190. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (month) | Weight (kg) | Length/Height (cm) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Boy | Girl | Boy | Girl | |||||||||
| 1 | 2 | 3 | 1 | 2 | 3 | 1 | 2 | 3 | 1 | 2 | 3 | |
| 0 | 3.42 | 3.32 * | 3.3 * | 3.31 | 3.21 * | 3.2 * | 50.0 | 50.4 * | 49.9 * | 50.0 | 49.7 * | 49.1 * |
| 1 | 4.66 | 4.51 * | 4.5 * | 4.44 | 4.20 * | 4.2 * | 55.2 | 54.8 * | 54.7 * | 54.3 | 53.7 * | 53.7 * |
| 3 | 6.86 | 6.70 * | 6.4 * | 6.45 | 6.13 * | 5.8 * | 62.4 | 62.0 * | 61.4 * | 61.2 | 60.6 * | 59.8 * |
| 6 | 8.40 | 8.41 | 7.9 * | 7.94 | 7.77 * | 7.3 * | 68.4 | 68.4 | 67.6 * | 66.9 | 66.8 | 65.7 * |
| 8 | 9.18 | 9.05 * | 8.6 * | 8.63 | 8.41 * | 7.9 * | 71.5 | 71.2 * | 70.6 * | 70.1 | 69.6 * | 68.7 * |
| 12 | 10.03 | 10.05 | 9.6 * | 9.53 | 9.40 * | 8.9 * | 76.1 | 76.5 * | 75.7 * | 74.9 | 75.0 | 74.0 * |
| 18 | 11.30 | 11.29 | 10.9 * | 10.73 | 10.65 | 10.2 * | 82.6 | 82.7 | 82.3 * | 81.4 | 81.5 | 80.7 * |
| 24 | 12.53 | 12.54 | 12.2 * | 11.98 | 11.92 | 11.5 * | 88.4 | 88.5 | 87.8 * | 87.2 | 87.2 | 86.4 * |
| 36 | 14.97 | 14.65 * | 14.3 * | 14.40 | 14.13 * | 13.9 * | 97.4 | 96.8 * | 96.1 * | 96.2 | 95.6 * | 95.1 * |
| Age (month) | WAZ (Mean ± SD) | LAZ/HAZ (Mean ± SD) | WLZ (Mean ± SD) | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Boy | Girl | Boy | Girl | Boy | Girl | |||||||||||||
| WHO | China | p | WHO | China | p | WHO | China | p | WHO | China | p | WHO | China | p | WHO | China | p | |
| 0 | 0.12 ± 0.80 | 0.22 ± 0.98 | 0.000 | 0.15 ± 0.88 | 0.19 ± 1.03 | 0.000 | 0.06 ± 0.36 | −0.22 ± 0.39 | 0.000 | 0.44 ± 0.32 | 0.14 ± 0.35 | 0.000 | 0.21 ± 1.17 | 0.49 ± 1.10 | 0.000 | −0.21 ± 1.26 | 0.02 ± 1.18 | 0.000 |
| 1 | 0.28 ± 0.80 | 0.25 ± 0.90 | 0.000 | 0.39 ± 0.84 | 0.40 ± 0.96 | 0.077 | 0.22 ± 0.90 | 0.17 ± 0.84 | 0.000 | 0.34 ± 0.86 | 0.32 ± 0.84 | 0.000 | 0.23 ± 1.05 | 0.25 ± 1.00 | 0.000 | 0.21 ± 1.05 | 0.26 ± 1.03 | 0.000 |
| 3 | 0.59 ± 0.88 | 0.17 ± 0.89 | 0.000 | 0.71 ± 0.86 | 0.38 ± 0.93 | 0.000 | 0.47 ± 1.02 | 0.17 ± 0.91 | 0.000 | 0.66 ± 0.98 | 0.26 ± 0.92 | 0.000 | 0.50 ± 1.02 | 0.24 ± 0.96 | 0.000 | 0.48 ± 1.03 | 0.38 ± 1.04 | 0.000 |
| 6 | 0.48 ± 0.90 | −0.05 ± 0.87 | 0.000 | 0.62 ± 0.88 | 0.13 ± 0.97 | 0.000 | 0.35 ± 1.01 | −0.02 ± 0.90 | 0.000 | 0.52 ± 0.94 | 0.05 ± 0.93 | 0.000 | 0.53 ± 0.98 | 0.15 ± 0.93 | 0.000 | 0.63 ± 0.90 | 0.36 ± 0.98 | 0.000 |
| 8 | 0.55 ± 0.92 | 0.09 ± 0.89 | 0.000 | 0.62 ± 0.88 | 0.17 ± 0.98 | 0.000 | 0.40 ± 0.99 | 0.65 ± 0.88 | 0.000 | 0.56 ± 0.97 | 0.76 ± 0.95 | 0.000 | 0.58 ± 0.95 | 0.23 ± 0.92 | 0.000 | 0.59 ± 0.90 | 0.30 ± 0.99 | 0.000 |
| 12 | 0.31 ± 0.91 | −0.07 ± 0.89 | 0.000 | 0.46 ± 0.84 | 0.07 ± 0.96 | 0.000 | 0.14 ± 0.99 | −0.18 ± 0.86 | 0.000 | 0.34 ± 0.94 | −0.04 ± 0.89 | 0.000 | 0.37 ± 0.95 | 0.09 ± 0.95 | 0.000 | 0.46 ± 0.91 | 0.18 ±1.02 | 0.000 |
| 18 | 0.25 ± 0.92 | −0.04 ± 0.93 | 0.000 | 0.33 ± 0.85 | 0.01 ± 0.98 | 0.000 | 0.11 ± 1.04 | −0.04 ± 0.90 | 0.000 | 0.24 ± 0.96 | −0.05 ± 0.92 | 0.000 | 0.31 ± 0.97 | 0.03 ± 1.00 | 0.000 | 0.31 ± 0.93 | 0.08 ± 1.06 | 0.000 |
| 24 | 0.23 ± 0.86 | −0.06 ± 0.90 | 0.000 | 0.29 ± 0.83 | −0.02 ± 0.95 | 0.000 | 0.17 ± 0.95 | −0.06 ± 0.82 | 0.000 | 0.25 ± 0.97 | −0.02 ± 0.90 | 0.000 | 0.19 ± 0.94 | 0.02 ± 0.98 | 0.000 | 0.17 ± 0.83 | 0.08 ± 0.96 | 0.000 |
| 36 | 0.30 ± 0.91 | 0.13 ± 0.99 | 0.000 | 0.23 ± 0.89 | 0.09 ± 1.03 | 0.000 | 0.35 ± 0.95 | 0.14 ± 0.91 | 0.000 | 0.30 ± 0.93 | 0.14 ± 0.93 | 0.000 | 0.19 ± 1.04 | 0.10 ± 1.11 | 0.000 | 0.09 ± 1.00 | 0.05 ± 1.14 | 0.000 |
| Age (months) | Underweight n (%) | Stunting n (%) | Wasting n (%) | Overweight n (%) | Obesity n (%) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| WHO | China | p | WHO | China | p | WHO | China | p | WHO | China | p | WHO | China | p | |
| 0 | 6 (0.6) | 19 (2.0) | 0.000 | 2 (0.2) | 2 (0.2) | 1.000 | 58 (6.3) | 29 (3.1) | 0.000 | 22 (2.4) | 31 (3.3) | 0.064 | 6 (0.6) | 11 (1.2) | 0.063 |
| 1 | 2 (0.2) | 11 (1.2) | 0.004 | 4 (0.4) | 4 (0.4) | 1.000 | 24 (2.7) | 22 (2.4) | 0.500 | 29 (3.2) | 29 (3.2) | 1.000 | 5 (0.6) | 6 (0.7) | 1.000 |
| 3 | 5 (0.6) | 8 (0.9) | 0.250 | 6 (0.7) | 9 (1.0) | 0.250 | 9 (1.0) | 12 (1.3) | 0.508 | 54 (6.0) | 33 (3.9) | 0.000 | 6 (0.7) | 5 (0.6) | 1.000 |
| 6 | 1 (0.1) | 7 (0.8) | 0.031 | 5 (0.6) | 8 (0.9) | 0.250 | 2 (0.2) | 7 (0.8) | 0.063 | 59 (6.6) | 42 (4.7) | 0.000 | 4 (0.4) | 1 (0.1) | 0.250 |
| 8 | 1 (0.1) | 7 (0.8) | 0.031 | 2 (0.2) | 2 (0.2) | 1.000 | 1 (0.1) | 5 (0.6) | 0.125 | 52 (5.8) | 33 (3.7) | 0.000 | 7 (0.8) | 4 (0.4) | 0.250 |
| 12 | 3 (0.3) | 13 (1.5) | 0.002 | 2 (0.2) | 6 (0.7) | 0.125 | 7 (0.8) | 14 (1.6) | 0.016 | 35 (4.0) | 27 (3.1) | 0.057 | 6 (0.7) | 3 (0.3) | 0.250 |
| 18 | 5 (0.6) | 18 (2.2) | 0.000 | 7 (0.8) | 8 (1.0) | 1.000 | 6 (0.7) | 16 (1.9) | 0.002 | 26 (3.1) | 21 (2.5) | 0.125 | 3 (0.4) | 2 (0.2) | 1.000 |
| 24 | 0 (0.0) | 11 (1.5) | 0.001 | 4 (0.5) | 6 (0.8) | 0.500 | 7 (0.9) | 14 (1.9) | 0.016 | 16 (2.1) | 17 (2.3) | 1.000 | 1 (0.1) | 1 (0.1) | 1.000 |
| 36 | 3 (0.4) | 7 (1.0) | 0.125 | 2 (0.3) | 5 (0.7) | 0.250 | 9 (1.2) | 18 (2.5) | 0.004 | 24 (3.3) | 29 (4.0) | 0.180 | 3 (0.4) | 5 (0.7) | 0.500 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tian, Q.; Gao, X.; Sha, T.; He, Q.; Cheng, G.; Wu, X.; Yang, F.; Wu, X.; Tang, C.; Xie, Q.; et al. Differences between WHO Growth Standards and China Growth Standards in Assessing the Nutritional Status of Children Aged 0–36 Months Old. Int. J. Environ. Res. Public Health 2020, 17, 251. https://doi.org/10.3390/ijerph17010251
Tian Q, Gao X, Sha T, He Q, Cheng G, Wu X, Yang F, Wu X, Tang C, Xie Q, et al. Differences between WHO Growth Standards and China Growth Standards in Assessing the Nutritional Status of Children Aged 0–36 Months Old. International Journal of Environmental Research and Public Health. 2020; 17(1):251. https://doi.org/10.3390/ijerph17010251
Chicago/Turabian StyleTian, Qianling, Xiao Gao, Tingting Sha, Qiong He, Gang Cheng, Xialing Wu, Fan Yang, Xihong Wu, Cai Tang, Qunhui Xie, and et al. 2020. "Differences between WHO Growth Standards and China Growth Standards in Assessing the Nutritional Status of Children Aged 0–36 Months Old" International Journal of Environmental Research and Public Health 17, no. 1: 251. https://doi.org/10.3390/ijerph17010251
APA StyleTian, Q., Gao, X., Sha, T., He, Q., Cheng, G., Wu, X., Yang, F., Wu, X., Tang, C., Xie, Q., & Yan, Y. (2020). Differences between WHO Growth Standards and China Growth Standards in Assessing the Nutritional Status of Children Aged 0–36 Months Old. International Journal of Environmental Research and Public Health, 17(1), 251. https://doi.org/10.3390/ijerph17010251