Health-Related Disparities among Migrant Children at School Entry in Germany. How does the Definition of Migration Status Matter?

 ,
,
Abstract
1. Introduction
1.1. Question
1.2. Theoretical Framework
2. Materials and Methods
2.1. Dataset
2.2. Variables
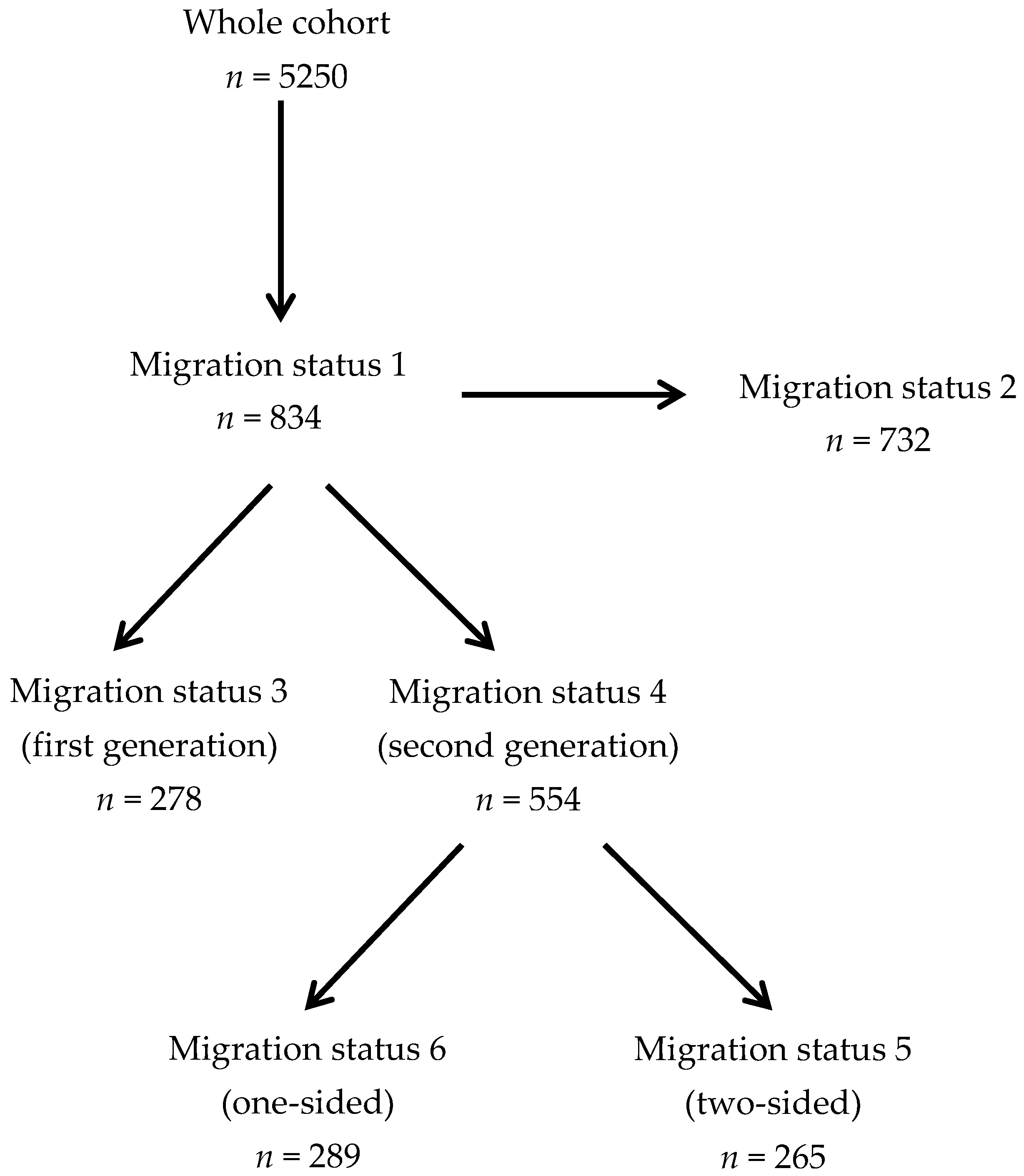
2.3. Definitions of Migration Status
2.4. Statistical Analysis
3. Results
3.1. Socio-Demographic Characteristics
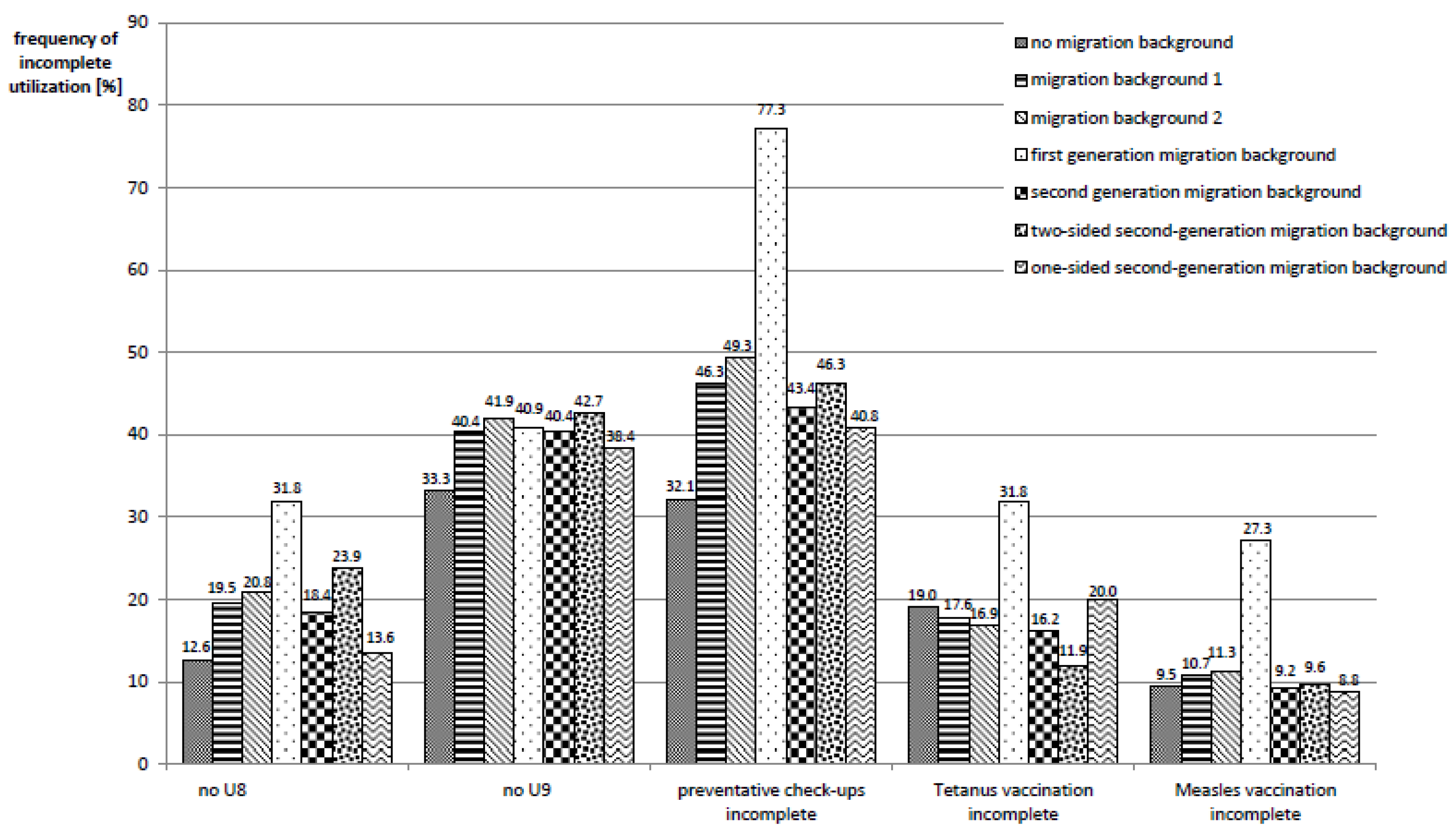
3.2. Health Service Utilization
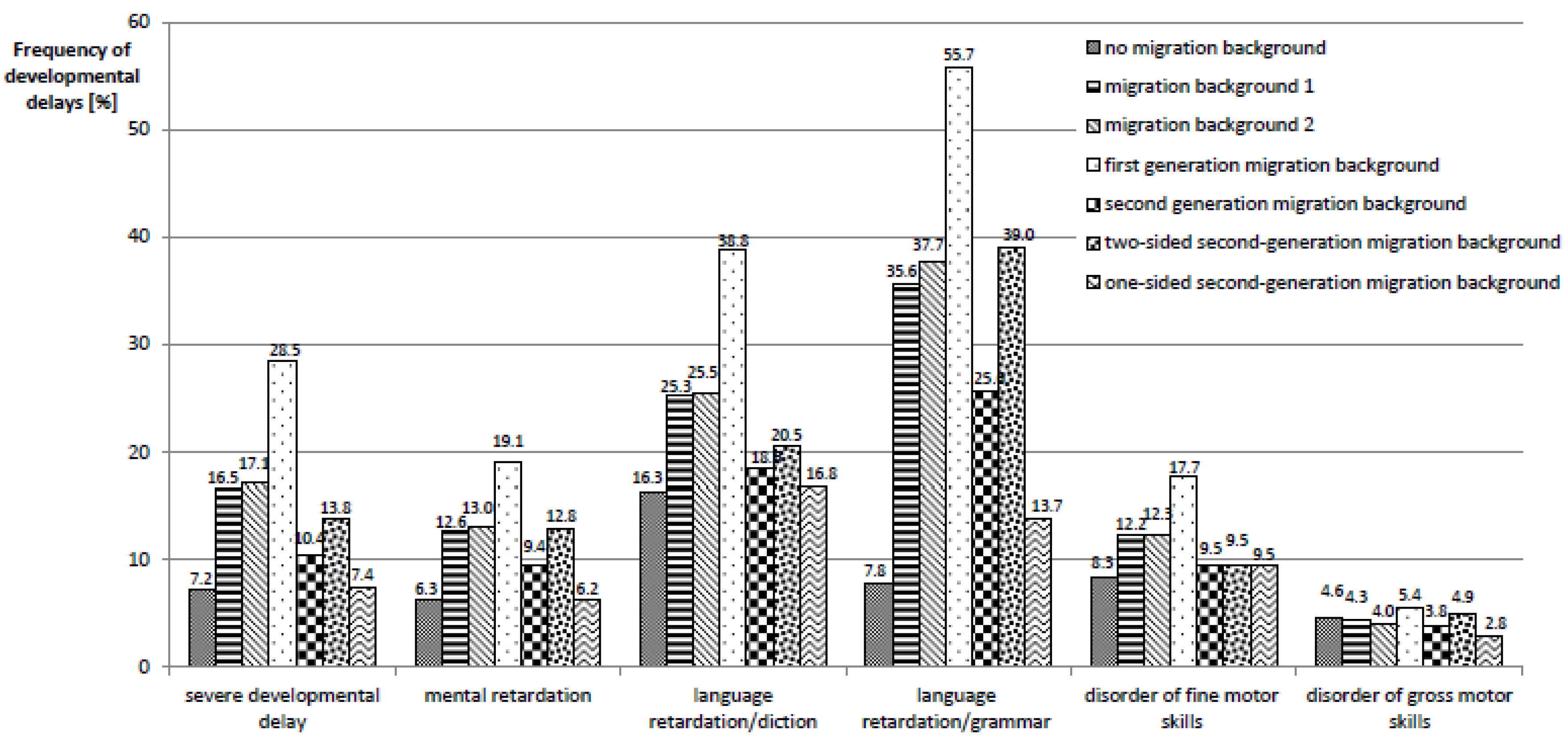
3.3. Health Outcomes
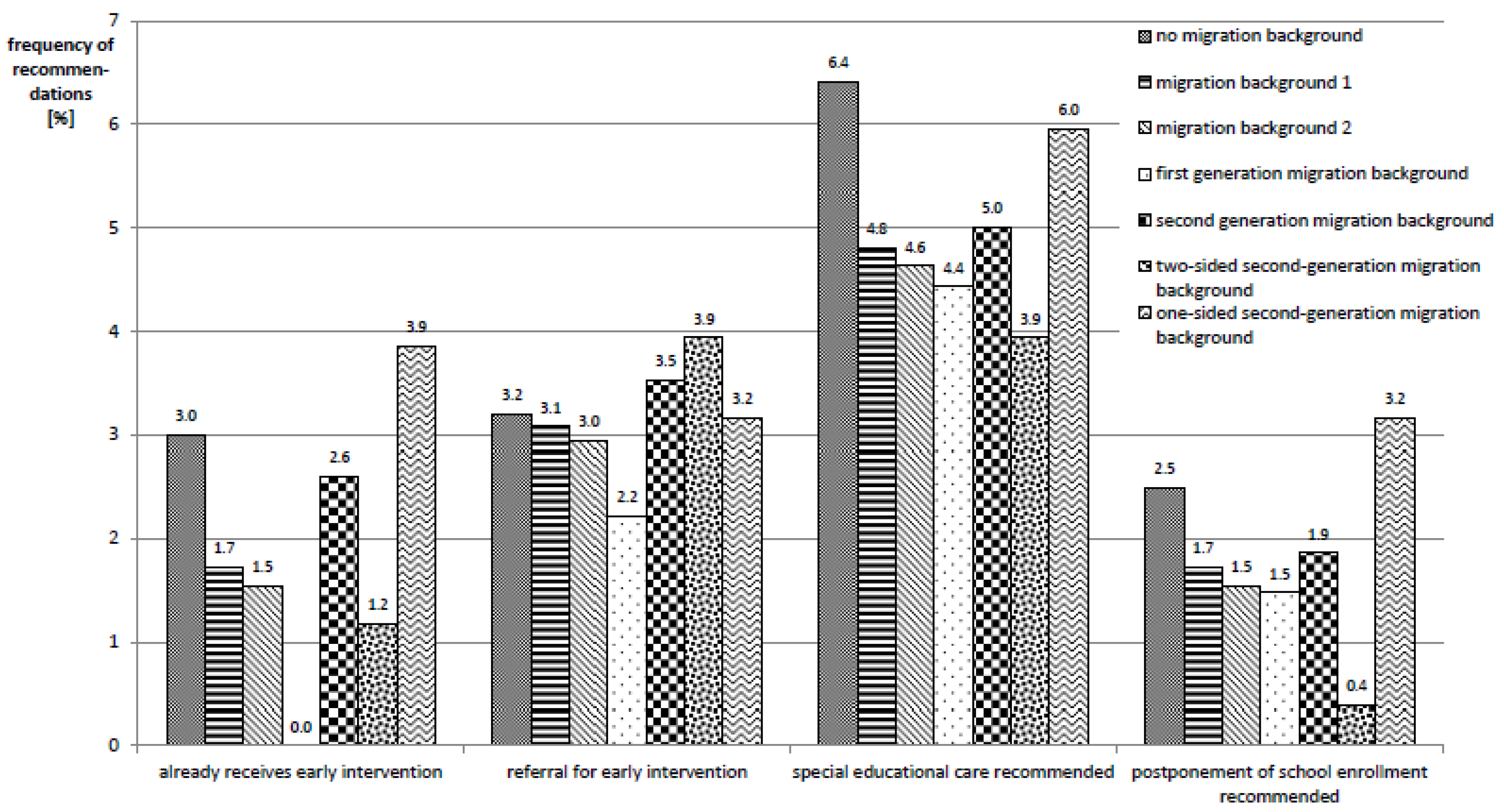
3.4. Multivariate Analyses
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- EUROSTAT. Migration and Migration Population Statistics. Available online: www.europa.eu/eurostat/statisticsexplained/index.php?title=Migration_and_migrant_population_statistics (accessed on 8 December 2019).
- Pew Research Center. Immigrant Share in U.S. Nears Record High but Remains Below That of Many Other Countries. Available online: https://www.pewresearch.org/fact-tank/2019/01/30/immigrant-share-in-u-s-nears-record-high-but-remains-below-that-of-many-other-countries/ (accessed on 8 December 2019).
- Instituto Nacional de Estadística y Geografía. 2015. Available online: https://web.archive.org/web/20151210212235/http://www.inegi.org.mx/est/contenidos/proyectos/encuestas/hogares/especiales/ei2015/doc/eic2015_resultados.pdf (accessed on 8 December 2019).
- Australian Burreau of Statistics. Australia’s Population by Country of Birth. Available online: https://www.abs.gov.au/ausstats/abs@.nsf/Latestproducts/3412.0Main%20Features22017-18 (accessed on 8 December 2019).
- Institute of Medicine (U.S.). Race, Ethnicity, and Language Data: Standardization for Health Care Quality Improvement; National Academies Press: Washington, DC, USA, 2009. [Google Scholar]
- Solé-Auró, A.; Crimmins, E.M. Health of immigrants in European countries. Int. Migr. Rev. 2008, 42, 861–876. [Google Scholar] [CrossRef] [PubMed]
- Rechel, B.; Mladovsky, P.; Ingleby, D.; Mackenbach, J.P.; McKee, M. Migration and health in an increasingly diverse Europe. Lancet 2013, 381, 1235–1245. [Google Scholar] [CrossRef]
- Bhugra, D. Migration and mental health. Acta Psychiatr. Scand. 2004, 109, 243–258. [Google Scholar] [CrossRef] [PubMed]
- Hudelson, P.; Dominice, D.M.; Perneger, T.; Durieux-Paillard, S.A. “Migrant friendly hospital” initiative in Geneva, Switzerland: Evaluation of the effects on staff knowledge and practices. PLoS ONE 2014, 9, e106758. [Google Scholar] [CrossRef] [PubMed]
- Alidu, L.; Grunfeld, E. A systematic review of acculturation, obesity and health behaviours among migrants to high-income countries. Psychol. Health 2018, 33, 724–745. [Google Scholar] [CrossRef]
- Razum, O.; Geiger, I.; Zeeb, H.; Ronellenfitsch, U. Health care for migrants. Deutsches Ärzteblatt 2004, 101, 2882–2887. [Google Scholar]
- European Centre for Disease Prevention and Control. Assessing the Burden of Key Infectious Diseases Affecting Migrant Populations in the EU/EEA; ECDC Technical Report; ECDC: Stockholm, Sweden, 2014. [Google Scholar]
- Hemminki, K. Immigrant health, our health. Eur. J. Public Health 2014, 24, 92–95. [Google Scholar] [CrossRef]
- Führer, A. “Da muss sich jemand anders drum kümmern”—Die medizinische Versorgung von Asylsuchenden als Herausforderung für eine bio-psycho-soziale Medizin. Gesundheitswesen 2019. [Google Scholar] [CrossRef]
- Rosenkötter, N.; van Dongen, M.; Hellmeier, W.; Simon, K.; Dagnelie, P.C. The influence of migratory background and parental education on health care utilisation of children. Eur. J. Pediatrics 2012, 171, 1533–1540. [Google Scholar] [CrossRef][Green Version]
- Brzoska, P.; Razum, O. Mortality and morbidity patterns among immigrants residing in Germany. In Migration, Health and Survival: International Perspectives; Trovato, F., Ed.; Edward Elgar: Cheltenham, UK, 2017; pp. 214–233. [Google Scholar]
- Brzoska, P. Disparities in health care outcomes between immigrants and the majority population in Germany: A trend analysis, 2006–2014. PLoS ONE 2018, 13, e0191732. [Google Scholar] [CrossRef]
- Le Thi, T.G.; Heißenhuber, A.; Schneider, T.; Schulz, R.; Herr, C.E.W.; Nennstiel-Ratzel, U.; Hölscher, G. The impact of migration background on the health outcomes of preschool children: Linking a cross-sectional survey to the school entrance health examination database in Bavaria, Germany. Gesundheitswesen 2019, 81, e34–e42. [Google Scholar]
- Robert Koch Institut. Kinder- und Jugendgesundheitssurvey (KiGGS) 2003–2006: Kinder und Jugendliche mit Migrationshintergrund in Deutschland; RKI: Berlin, Germany, 2008. [Google Scholar]
- Knipper, M. Migrationshintergrund? Plädoyer für eine zeitgemäße Beachtung der sozialen und kulturellen Hintergründe von Kindergesundheit in Deutschland. In Schwerpunktthema Migrantinnen und Migranten in der Pädiatrie; Bundesverband der Kinder- und Jugendärzte, e.V., Ed.; BVKJ: Köln, Germany, 2013; pp. 65–69. [Google Scholar]
- Schenk, L.; Bau, A.-M.; Borde, T.; Butler, J.; Lampert, T.; Neuhauser, H.; Razum, O.; Weilandt, C. A basic set of indicators for mapping migrant status. Recommendations for epidemiological practice. Bundesgesundheitsblatt 2006, 49, 853–860. [Google Scholar] [CrossRef] [PubMed]
- Oberwöhrmann, S.; Bettge, S.; Hermann, S. Einheitliche Erfassung des Migrationshintergrundes bei den Einschulungsuntersuchungen; Senatsverwaltung für Gesundheit und Soziales Berlin: Berlin, Germany, 2013. [Google Scholar]
- Kemper, T. Zur Landesspezifischen Erfassung des Migrationshintergrunds in der Schulstatistik-(k)ein Gemeinsamer Nenner in Sicht? Schumpeter Discussion Papers: Wuppertal, Germany, 2016. [Google Scholar]
- Nguyen, V.-K. The Republic of Therapy: Triage and Sovereignty in West Africa’s Time of AIDS; Duke University Press: Durham, NC, USA, 2010. [Google Scholar]
- Bauer, S. Politik mit Kategorien: Zur Produktion von Differenz in Epidemiologie und Biomedizin. In Gemachte Differenz: Kontinuitäten biologischer “Rasse”-Konzepte; AG gegen Rassismus in den Lebenswissenschaften, Ed.; Unrast: Münster, Germany, 2009; pp. 278–301. [Google Scholar]
- Mays, V.M.; Ponce, N.A.; Washington, D.L.; Cochran, S.D. Classification of race and ethnicity: Implications for public health. Annu. Rev. Public Health 2003, 24, 83–110. [Google Scholar] [CrossRef]
- Statistisches Bundesamt. Bevölkerung mit Migrationshintergrund—Ergebnisse des Mikrozensus 2017; Statistisches Bundesamt: Berlin, Germany, 2017.
- Führer, A.; Eichner, F. Statistics and sovereignty: The workings of biopower in epidemiology. Glob. Health Action 2015, 8, 28262. [Google Scholar] [CrossRef]
- Foucault, M.; Senellart, M.; Ewald, F.; Fontana, A. Security, Territory, Population: Lectures at the Collège de France, 1977–1978; Palgrave Macmillan: Basingstoke, UK; New York, NY, USA, 2007. [Google Scholar]
- Goffman, E. Stigma: Notes on the Management of Spoiled Identity; Simon & Schuster: New York, NY, USA, 1986. [Google Scholar]
- Hacking, I. Making up people. In Reconstructing Individualism; Heller, T., Sosna, M., Wellbery, D., Eds.; Standford University Press: Stanford, CA, USA, 1986; pp. 161–171. [Google Scholar]
- Foucault, M. The subject and power. Crit. Inq. 1982, 8, 777–795. [Google Scholar] [CrossRef]
- Hacking, I. Rewriting the Soul. Multiple Personality and the Sciences of Memory; Princeton University Press: Princeton, NJ, USA, 1998. [Google Scholar]
- Will, A.-K. 10 Jahre Migrationshintergrund in der Repräsentativstatistik: Ein Konzept auf dem Prüfstand. Leviathan 2016, 44, 9–35. [Google Scholar] [CrossRef]
- Bollig, S.; Tervooren, A. The order of family as a preventive resource. Informal developmental diagnostic in pediatric and school entry check-ups using the example of exploring children´s television viewing. J. Sociol. Educ. Social. 2009, 29, 157–173. [Google Scholar]
- Franze, M.; Gottschling, A.; Hoffmann, W. The “Dortmund Developmental Screening for Preschools” as the basis for developmental promotion in preschools in Mecklenburg-West Pomerania. First results of the pilot project “Children in Preschools” referring to the acceptance of DESK 3–6 by preschool teachers. Bundesgesundheitsblatt 2010, 53, 1290–1297. [Google Scholar]
- Hespe-Jungesblut, K.; Jahn, N.; Bruns-Philipps, E.; Zühlke, C. Ärztliche Untersuchung vor Schulbeginn lohnt sich. Pädiatrie Hautnah 2013, 25, 41–46. [Google Scholar] [CrossRef]
- Mossakowski, K.; Nickel, S.; Schäfer, I.; Süß, W.; Trojan, A.; Werner, S. Diagnosis of an urban quarter: Data and approaches for a quarter-oriented prevention programme in the public health sector. Präv. Gesundheitsf. 2007, 2, 82–89. [Google Scholar] [CrossRef]
- Weßling, A. School entrance examination: Prospects for a data-based health promotion in school and community. Gesundheitswesen 2000, 62, 383–900. [Google Scholar] [CrossRef] [PubMed]
- Kelle, H. Schuleingangsuntersuchungen im Spannungsfeld von Individualdiagnostik und Epidemiologie: Eine Praxisanalyse. Diskurs Kindheits- und Jugendforschung 2011, 6, 247–262. [Google Scholar]
- Spannenkrebs, M.; Crispin, A.; Krämer, D. The new preschool examination in Baden-Wurtemberg: What determinants influence the school medical evaluation special need for language promotion in childhood development? Gesundheitswesen 2013, 75, 838–847. [Google Scholar] [PubMed]
- Kelle, H. Bedeutungswandel der ärztlichen Schuleingangsuntersuchungen. Grundsch. Aktuell 2006, 9, 24–26. [Google Scholar]
- Führer, A.; Wienke, A.; Tiller, D. Die Schuleingangsuntersuchung als subsidiäre Vorsorgeuntersuchung. Präv. Gesundheitsf. 2018, 143, 198–204. [Google Scholar] [CrossRef]
- Führer, A.; Wienke, A.; Wiermann, S.; Gröger, C.; Tiller, D. Risk-based approach to school entry examinations in Germany—A validation study. BMC Pediatrics 2019, 19, 448. [Google Scholar] [CrossRef]
- Böhm, A.; Ellsässer, G.; Lüdecke, K. The Brandenburg social index: A tool for health and social reporting at regional and communal levels in the analysis of data of school beginners. Gesundheitswesen 2007, 69, 555–559. [Google Scholar] [CrossRef]
- Robert Koch Institut. Impfkalender (Standardimpfungen) für Säuglinge, Kinder, Jugendliche und Erwachsene 2018/2019. Epidemiol. Bull. 2018, 34, 338. [Google Scholar]
- Arbeitsgruppe Standardisierung im KJÄD 2011/2012. Handreichung für die Schuleingangsuntersuchung in Sachsen-Anhalt. 2013. Available online: https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&ved=2ahUKEwj58qPAjdPmAhX2wsQBHUT1C-cQFjAAegQIARAC&url=https%3A%2F%2Fverbraucherschutz.sachsen-anhalt.de%2Ffileadmin%2FBibliothek%2FPolitik_und_Verwaltung%2FMS%2FLAV_Verbraucherschutz%2Fservice%2Fgbe%2Fberichte%2F2018_12_Handreichung_SEU_Auszug_ohne_SEBES.pdf&usg=AOvVaw0XAa0tUnih9uSGJCOK40Dd (accessed on 26 December 2019).
- Razum, O.; Zeeb, H.; Meesmann, U.; Schenk, L.; Bredehorst, M.; Brzoska, P.; Dercks, T.; Glodny, S.; Menkhaus, S.; Salman, R.; et al. Migration und Gesundheit. Schwerpunktbericht der Gesundheitsberichterstattung des Bundes; Gesundheitsberichterstattung des Bundes: Berlin, Germany, 2008. [Google Scholar]
- Mauz, E.; Lange, M.; Houben, R.; Hoffmann, R.; Allen, J.; Gößwald, A.; Hölling, H.; Lampert, T.; Lange, C.; Poethko-Müller, C.; et al. Cohort profile: KiGGS cohort longitudinal study on the health of children, adolescents and young adults in Germany. Int. J. Epidemiol. 2019. [Google Scholar] [CrossRef]
- Greenland, S.; Thomas, D.C. On the need for the rare disease assumption in case-control studies. Am. J. Epidemiol. 1982, 116, 547–553. [Google Scholar] [CrossRef]
- Wasserstein, R.L.; Schirm, A.L.; Lazar, N.A. Moving to a world beyond “p < 0.05”. Am. Stat. 2019, 73, 1–19. [Google Scholar]
- Amrhein, V.; Greenland, S.; McShane, B. Scientists rise up against statistical significance. Nature 2019, 567, 305–307. [Google Scholar] [CrossRef] [PubMed]
- AGENS. Gute Praxis Sekundärdatenanalyse (GPS): Leitlinien und Empfehlungen; AGENS: Köln, Germany, 2014. [Google Scholar]
- Stich, P.; Mikolajczyk, R.; Krämer, A. Determinanten des Teilnahmeverhaltens bei Kindervorsorgeuntersuchungen (U1–U8): Eine gesundheitswissenschaftliche Analyse zur Gesundheitsversorgung im Kindesalter. Praev. Gesundheitsf. 2009, 4, 265–271. [Google Scholar] [CrossRef]
- Schäfer, P.; Schöler, H.; Roos, J.; Grün-Nolz, P.; Engler-Thümmel, H. Einschulungsuntersuchung 2002 in Mannheim – Sprachentwicklungsstand bei Schulbeginn. Gesundheitswesen 2003, 2003, 676–682. [Google Scholar]
- Zhou, Y.; Lengerke, T.; Walter, U.; Dreier, M. Migration background and childhood overweight in the Hannover Region in 2010–2014: A population-based secondary data analysis of school entry examinations. Eur. J. Pediatrics 2018, 177, 753–763. [Google Scholar] [CrossRef]
- Achat, H.M.; Stubbs, J.M. Socio-economic and ethnic differences in the prevalence of overweight and obesity among school children. J. Paediatrics Child Health 2014, 50, E77–E84. [Google Scholar] [CrossRef]
- Waters, E.; Ashbolt, R.; Gibbs, L.; Booth, M.; Magarey, A.; Gold, L.; Kai Lo, S.; Gibbons, K.; Green, J.; O’Connor, T.; et al. Double disadvantage: The influence of ethnicity over socioeconomic position on childhood overweight and obesity: Findings from an inner urban population of primary school children. Int. J. Pediatric Obes. 2008, 3, 196–204. [Google Scholar] [CrossRef]
- El-Sayed, A.M.; Scarborough, P.; Galea, S. Ethnic inequalities in obesity among children and adults in the UK: A systematic review of the literature. Obes. Rev. 2011, 12, e516–e534. [Google Scholar] [CrossRef]
- Abraído-Lanza, A.F.; Armbrister, A.N.; Flórez, K.R.; Aguirre, A.N. Toward a theory-driven model of acculturation in public health research. Am. J. Public Health 2006, 96, 1342–1346. [Google Scholar] [CrossRef]
- Tanenbaum, M.L.; Commissariat, P.; Kupperman, E.; Baek, R.N.; Gonzalez, J.S. Acculturation. In Encyclopedia of Behavioral Medicine; Gellman, M.D., Turner, J.R., Eds.; Springer: New York, NY, USA, 2013; pp. 12–14. [Google Scholar]
- Bundesweite Arbeitsgemeinschaft der Psychosozialen Zentren für Flüchtlinge und Folteropfer. Traumatisiert. Ausgegrenzt. Unterversorgt.: Versorgungsbericht zur Situation von Flüchtlingen und Folteropfern in den Bundesländern Sachsen, Sachsen-Anhalt und Thüringen; Baff e.V.: Berlin, Germany, 2014. [Google Scholar]
- Heeren, M.; Wittmann, L.; Ehlert, U.; Schnyder, U.; Maier, T.; Müller, J. Psychopathology and resident status—Comparing asylum seekers, refugees, illegal migrants, labor migrants, and residents. Compr. Psychiatry 2014, 55, 818–825. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Migration Status 1 | Migration Status 2 | Migration Status 3 | Migration Status 4 | Migration Status 5 | Migration Status 6 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No | Yes | No | Yes | No | Yes | No | Yes | No | Yes | No | Yes | |
| Sex | ||||||||||||
| Male | 50.5% | 49.8% | 50.7% | 48.2% | 50.4% | 50.7% | 50.5% | 49.3% | 50.4% | 50.2% | 50.5% | 48.5% |
| Female | 49.5% | 50.2% | 49.3% | 51.9% | 49.6% | 49.3% | 49.5% | 50.7% | 49.6% | 49.8% | 49.5% | 51.5% |
| Age (years) | ||||||||||||
| 4 | 7.7% | 6.6% | 7.6% | 6.9% | 7.6% | 6.7% | 7.7% | 6.5% | 7.7% | 4.8% | 7.6% | 7.8% |
| 5 | 84.8% | 85.8% | 84.8% | 86.2% | 85.0% | 84.7% | 84.9% | 86.3% | 84.8% | 89.9% | 84.8% | 83.6% |
| 6 | 7.4% | 7.6% | 7.5% | 6.9% | 7.4% | 8.6% | 7.4% | 7.2% | 7.5% | 5.3% | 7.5% | 8.6% |
| Socio-Economic Status * | ||||||||||||
| High | 46.4% | 38.5% | 46.7% | 35.4% | 46.2% | 24.9% | 46.4% | 44.6% | 45.5% | 38.7% | 45.3% | 49.3% |
| Medium | 34.9% | 28.3% | 34.7% | 29.3% | 34.4% | 25.4% | 34.9% | 29.7% | 34.3% | 28.0% | 34.5% | 31.0% |
| Low | 18.7% | 33.1% | 18.7% | 35.4% | 19.5% | 49.8% | 18.7% | 25.7% | 20.2% | 33.3% | 20.3% | 19.8% |
| Type of Child Care | ||||||||||||
| Kindergarten | 96.8% | 85.1% | 96.6% | 84.9% | 96.8% | 60.3% | 96.8% | 96.0% | 95.2% | 94.7% | 95.0% | 97.0% |
| At home | 3.0% | 14.7% | 3.2% | 15.0% | 3.1% | 39.2% | 3.0% | 4.0% | 4.7% | 5.3% | 4.8% | 3.0% |
| Nanny | 0.2% | 0.2% | 0.2% | 0.2% | 0.1% | 0.5% | 0.2% | . | 0.2% | . | 0.2% | . |
| Parents’ Marital Status | ||||||||||||
| No information | 0.2% | 0.3% | 0.2% | 0.3% | 0.2% | 0.2% | 0.4% | 0.2% | 1.0% | 0.2% | . | |
| Single mother | 22.4% | 18.4% | 22.2% | 19.0% | 22.3% | 10.5% | 22.3% | 21.9% | 22.2% | 12.1% | 21.8% | 29.5% |
| Mother and new partner | 6.3% | 3.2% | 6.2% | 3.0% | 6.0% | 1.9% | 6.3% | 3.8% | 6.0% | 1.5% | 6.0% | 5.6% |
| Both parents | 68.6% | 76.8% | 68.9% | 76.3% | 67.0% | 87.6% | 68.6% | 72.0% | 69.1% | 85.0% | 69.5% | 61.9% |
| other | 2.6% | 1.3% | 2.6% | 1.4% | 2.6% | 2.6% | 1.9% | 2.5% | 0.5% | 2.5% | 3.0% | |
| Number of Siblings | ||||||||||||
| <3 | 88.3% | 80.2% | 88.2% | 79.5% | 87.7% | 75.1% | 87.7% | 82.3% | 87.3% | 83.1% | 87.4% | 81.7% |
| ≥3 | 11.7% | 19.9% | 11.8% | 20.5% | 12.3% | 24.9% | 12.4% | 17.7% | 12.7% | 16.9% | 12.6% | 18.3% |
| Mother’s Country of Origin | Migration Status 1 | Migration Status 2 | Migration Status 3 | Migration Status 4 | Migration Status 5 | Migration Status 6 |
|---|---|---|---|---|---|---|
| Germany | 206 (24.8%) | 159 (21.8%) | 16 (5.8%) | 190 (34.4%) | 1 (0.4%) | 189 (65.6%) |
| Syria | 150 (18.0%) | 144 (19.7%) | 119 (42.8%) | 31 (5.6%) | 31 (11.7%) | 0 |
| Russia | 48 (5.8%) | 42 (5.8%) | 6 (2.2%) | 42 (7.6%) | 27 (10.2%) | 15 (5.2%) |
| Turkey | 42 (5.1%) | 39 (5.3%) | 2 (0.7%) | 40 (7.2%) | 40 (15.1%) | 0 |
| Vietnam | 41 (4.9%) | 41 (5.6%) | 2 (0.7%) | 39 (7%) | 33 (12.5%) | 6 (2.1%) |
| Poland | 24 (2.9%) | 21 (2.9%) | 11 (4%) | 13 (2.4%) | 3 (1.1%) | 10 (3.5%) |
| Ukraine | 22 (2.6%) | 20 (2.7%) | 6 (2.2%) | 16 (2.9%) | 13 (4.9%) | 3 (1%) |
| Iraq | 19 (2.3%) | 16 (2.2%) | 1 (0.4%) | 18 (3.3%) | 17 (6.4%) | 1 (0.4%) |
| Kosovo | 18 (2.2%) | 18 (2.5%) | 2 (0.7%) | 16 (2.9%) | 15 (5.7%) | 1 (0.4%) |
| Kazakhstan | 15 (1.8%) | 11 (1.5%) | 1 (0.4%) | 14 (2.5%) | 11 (4.2%) | 3 (1%) |
| Father’s Country of Origin | ||||||
| Syria | 158 (19%) | 149 (20.5%) | 120 (43.3%) | 38 (6.9%) | 32 (12.1%) | 6 (2.1%) |
| Germany | 110 (13.3%) | 85 (11.7%) | 22 (7.9%) | 88 (16%) | 1 (0.4%) | 87 (30.4%) |
| Nigeria | 56 (6.8%) | 51 (7%) | 3 (1.1%) | 53 (9.6%) | 8 (3%) | 45 (15.7%) |
| Turkey | 54 (6.5%) | 51 (7%) | 4 (1.4%) | 50 (9%) | 41 (15.5%) | 9 (3.2%) |
| Russia | 35 (4.2%) | 26 (3.6%) | 3 (1.1%) | 32 (5.8%) | 23 (8.7%) | 9 (3.2%) |
| Vietnam | 34 (4.1%) | 34 (4.7%) | 1 (0.4%) | 33 (6%) | 33 (12.5%) | 0 |
| Iraq | 32 (3.9%) | 29 (4%) | 1 (0.4%) | 31 (5.6%) | 17 (6.4%) | 14 (4.9%) |
| Kosovo | 19 (2.3%) | 19 (2.6%) | 1 (0.4%) | 18 (3.3%) | 16 (6%) | 2 (0.7%) |
| Ukraine | 17 (2.1%) | 16 (2.2%) | 1 (0.4%) | 16 (2.9%) | 12 (4.5%) | 4 (1.4%) |
| India | 16 (1.9%) | 15 (2.1%) | 10 (3.6%) | 6 (1.1%) | 2 (0.8%) | 4 (1.4%) |
| No Preventative Checkup U8 | Incomplete Tetanus Vaccination | Severe Developmental Delay | Special Educational Care Recommended | Referral for Early Intervention | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Crude PR * (95%-CI) | Adjusted PR *,† (95%-CI) | Crude PR * (95%-CI) | Adjusted PR *,† (95%-CI) | Crude PR * (95%-CI) | Adjusted PR *,† (95%-CI) | Crude PR * (95%-CI) | Adjusted PR *,† (95%-CI) | Crude PR * (95%-CI) | Adjusted PR *,† (95%-CI) | |
| Migration status 1 | 1.57 (1.30–1.88) | 1.57 (1.29–1.90) | 2.14 (1.93–2.37) | 2.02 (1.81–2.26) | 2.22 (1.86–2.65) | 1.57 (1.29–1.90) | 0.76 (0.55–1.03) | 0.59 (0.42–0.82) | 0.96 (0.64–1.45) | 0.74 (0.47–1.17) |
| Migration status 2 | 1.66 (1.38–2.01) | 1.61 (1.31–1.98) | 2.25 (2.03–2.49) | 2.13 (1.9–2.38) | 2.32 (1.93–2.77) | 1.58 (1.30–1.93) | 0.72 (0.51–1.01) | 0.56 (0.39–0.79) | 0.93 (0.6–1.44) | 0.69 (0.43–1.13) |
| Migration status 3 | 2.35 (1.51–3.65) | 3.05 (1.97–4.73) | 3.83 (3.49–4.21) | 3.56 (3.2–3.96) | 3.69 (3.01–4.54) | 2.16 (1.73–2.69) | 0.75 (0.45– 1.27) | 0.44 (0.25–0.79) | 0.78 (0.37–1.64) | 0.42 (0.18–1.02) |
| Migration status 4 | 1.49 (1.23–1.82) | 1.47 (1.2–1.81) | 1.28 (1.09–1.5) | 1.31 (1.1–1.55) | 1.47 (1.15–1.89) | 1.14 (0.87–1.51) | 0.76 (0.52–1.1) | 0.68 (0.46–1.00) | 1.06 (0.66–1.7) | 0.95 (0.58–1.58) |
| Migration status 5 | 1.85 (1.45–2.35) | 1.77 (1.36–2.3) | 1.25 (0.99–1.56) | 1.28 (0.99–1.64) | 2.05 (1.54–2.74) | 1.41 (1.02–1.95) | 0.62 (0.35–1.12) | 0.52 (0.29–0.96) | 1.17 (0.62–2.19) | 0.80 (0.38–1.68) |
| Migration status 6 | 1.19 (0.89–1.59) | 1.22 (0.91–1.65) | 1.31 (1.06–1.61) | 1.34 (1.08–1.66) | 0.94 (0.62–1.42) | 0.85 (0.54–1.34) | 0.88 (0.55–1.42) | 0.85 (0.52–1.38) | 0.96 (0.5–1.87) | 1.1 (0.57–2.1) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Führer, A.; Tiller, D.; Brzoska, P.; Korn, M.; Gröger, C.; Wienke, A. Health-Related Disparities among Migrant Children at School Entry in Germany. How does the Definition of Migration Status Matter? Int. J. Environ. Res. Public Health 2020, 17, 212. https://doi.org/10.3390/ijerph17010212
Führer A, Tiller D, Brzoska P, Korn M, Gröger C, Wienke A. Health-Related Disparities among Migrant Children at School Entry in Germany. How does the Definition of Migration Status Matter? International Journal of Environmental Research and Public Health. 2020; 17(1):212. https://doi.org/10.3390/ijerph17010212
Chicago/Turabian StyleFührer, Amand, Daniel Tiller, Patrick Brzoska, Marie Korn, Christine Gröger, and Andreas Wienke. 2020. "Health-Related Disparities among Migrant Children at School Entry in Germany. How does the Definition of Migration Status Matter?" International Journal of Environmental Research and Public Health 17, no. 1: 212. https://doi.org/10.3390/ijerph17010212
APA StyleFührer, A., Tiller, D., Brzoska, P., Korn, M., Gröger, C., & Wienke, A. (2020). Health-Related Disparities among Migrant Children at School Entry in Germany. How does the Definition of Migration Status Matter? International Journal of Environmental Research and Public Health, 17(1), 212. https://doi.org/10.3390/ijerph17010212