Age and Sex Differences in the Use of Emergency Telephone Consultation Services in Saitama, Japan: A Population-Based Observational Study


Abstract
1. Introduction
2. Materials and Methods
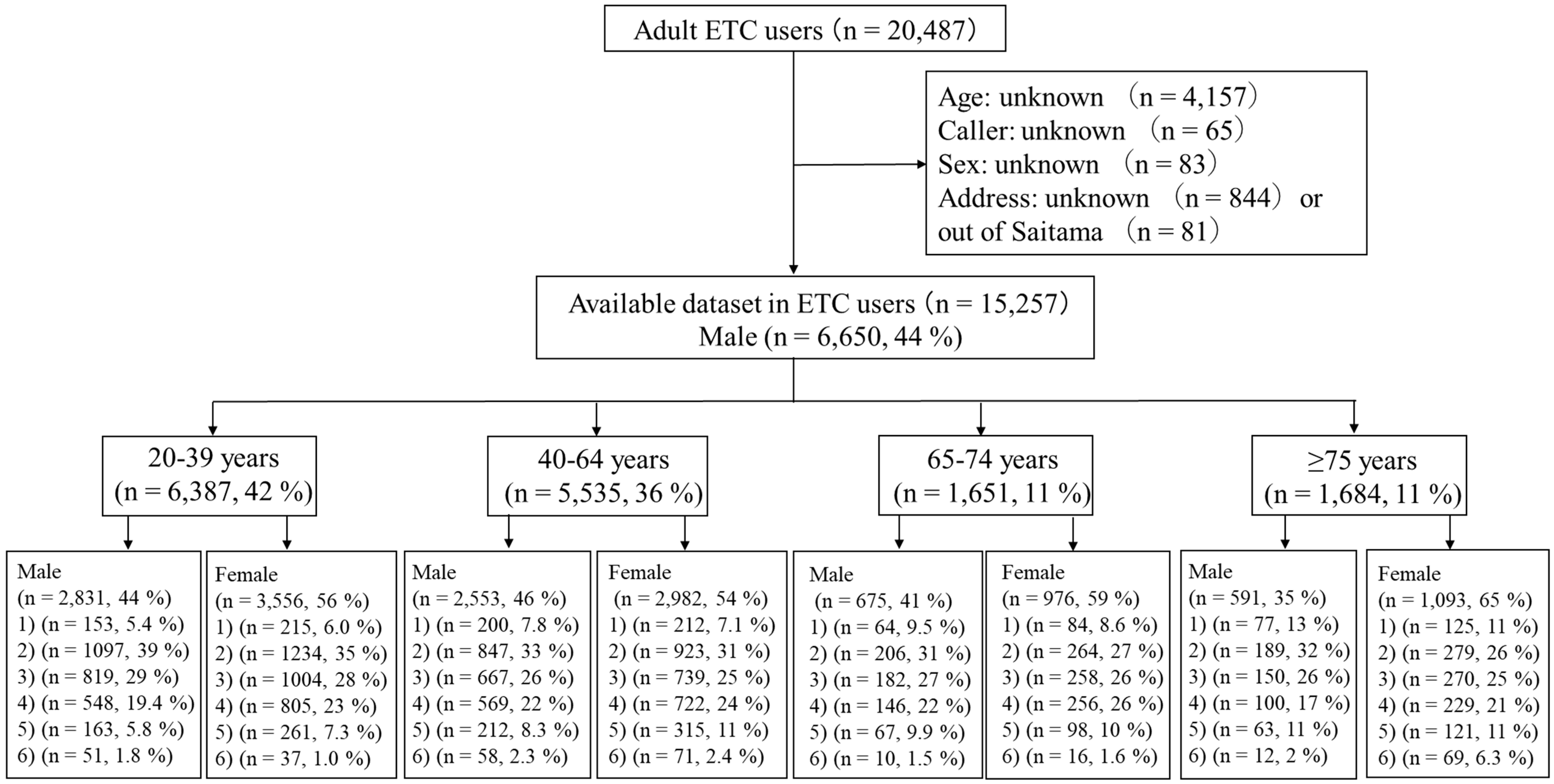
2.1. Study Design and Data Collection
2.2. ETC Services in Saitama Prefecture, Japan
2.3. Statistical Analysis
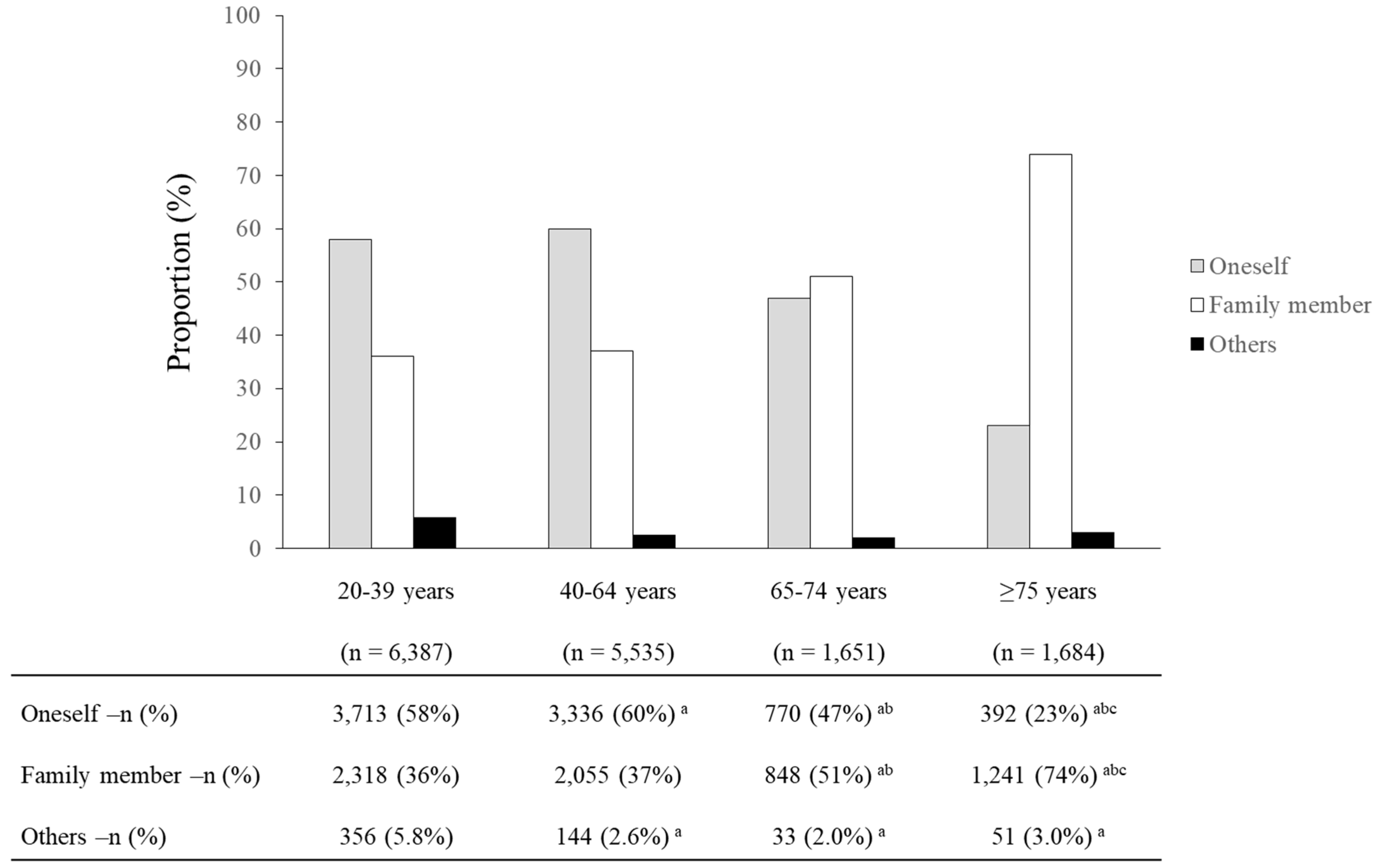
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Morimura, N.; Aruga, T.; Sakamoto, T.; Aoki, N.; Ohta, S.; Ishihara, T.; Kushimoto, S.; Ohta, S.; Ishikawa, H.; Steering Council of Tokyo Emergency Telephone Consultation Centre. The impact of an emergency telephone consultation service on the use of ambulances in Tokyo. Emerg. Med. J. 2011, 28, 64–70. [Google Scholar] [CrossRef] [PubMed]
- Christensen, M.B.; Olesen, F. Out of hours service in Denmark: Evaluation five years after reform. BMJ 1998, 316, 1502–1505. [Google Scholar] [CrossRef] [PubMed]
- Munro, J.; Nicholl, J.; O’Cathain, A.; Knowles, E. Impact of NHS direct on demand for immediate care: Observational study. BMJ 2000, 321, 150–153. [Google Scholar] [CrossRef] [PubMed]
- Turner, V.F.; Bentley, P.J.; Hodgson, S.A.; Collard, P.J.; Drimatis, R.; Rabune, C.; Wilson, A.J. Telephone triage in Western Australia. Med. J. Aust. 2002, 176, 100–103. [Google Scholar] [CrossRef] [PubMed]
- Shekelle, P.; Roland, M. Nurse-led telephone-advice lines. Lancet 1999, 354, 88–89. [Google Scholar] [CrossRef]
- Barber, J.W.; King, W.D.; Monroe, K.W.; Nichols, M.H. Evaluation of emergency department referrals by telephone triage. Pediatrics 2000, 105, 819–821. [Google Scholar] [CrossRef]
- North, F.; Carkey, P. A retrospective study of adult telephone triage calls in a US call centre. J. Telemed. Telecare 2009, 15, 165–170. [Google Scholar] [CrossRef]
- De Coster, C.; Quan, H.; Elford, R.; Li, B.; Mazzei, L.; Zimmer, S. Follow-through after calling a nurse telephone advice line: A population-based study. Fam. Pract. 2010, 27, 271–278. [Google Scholar] [CrossRef]
- Hansen, E.H.; Hunskaar, S. Telephone triage by nurses in primary care out-of-hours services in Norway: An evaluation study based on written case scenarios. BMJ Qual. Saf. 2011, 20, 390–396. [Google Scholar] [CrossRef][Green Version]
- Kaminsky, E.; Carlsson, M.; Holmström, I.K.; Larsson, J.; Fredriksson, M. Goals of telephone nursing work—The managers’ perspectives: A qualitative study on Swedish Healthcare Direct. BMC Health Serv. Res. 2014, 14, 188. [Google Scholar] [CrossRef]
- Fire and Disaster Management Agency (FDMA). White Paper on Fire Service 2018. Available online: https://www.fdma.go.jp/publication/hakusho/h30/items/part2_section4.pdf (accessed on 29 November 2019). (In Japanese)
- Statistics Bureau of Japan. The 2015 Population Census of Japan. Available online: https://www.stat.go.jp/data/kokusei/2015/index.html (accessed on 17 May 2019).
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef]
- Moyal, A. The gendered use of the telephone: An Australian case study. Media Cult. Soc. 1992, 14, 51–72. [Google Scholar] [CrossRef]
- Smoreda, Z.; Licoppe, C. Gender-specific use of the domestic telephone. Soc. Psychol. Q. 2000, 63, 238–252. [Google Scholar] [CrossRef]
- Claisse, G.; Rowe, F. Domestic telephone habits and daily mobility. Transp. Res. Part A Policy Pract. 1993, 27, 277–290. [Google Scholar] [CrossRef]
- Nakamura, I. Telephone community. Matsuyama Univ. J. 1999, 11, 307–328. (In Japanese) [Google Scholar]
- Tokuda, Y.; Abe, T.; Ishimatsu, S.; Hinohara, S. Ambulance transport of the oldest old in Tokyo: A population-based study. J. Epidemiol. 2010, 20, 468–472. [Google Scholar] [CrossRef]
- Fire and Disaster Management Agency (FDMA). Overview of the 2017 White Paper on Fire Service. Available online: http://www.kaigai-shobo.jp/pdf/20190531_White_paper30_eng.pdf (accessed on 29 November 2019).
- Shah, M.N.; Glushak, C.; Karrison, T.G.; Mulliken, R.; Walter, J.; Friedmann, P.D.; Hayley, D.C.; Chin, M.H. Predictors of emergency medical services utilization by elders. Acad. Emerg. Med. 2003, 10, 52–58. [Google Scholar] [CrossRef]
- Dickinson, E.T.; Verdile, V.P.; Kostyun, C.T.; Salluzzo, R.F. Geriatric use of emergency medical services. Ann. Emerg. Med. 1996, 27, 199–203. [Google Scholar] [CrossRef]
- Hashizume, A.; Kurosu, M.; Kaneko, T. The choice of communication media and the use of mobile phone among senior users and young users. In Computer–Human Interaction; APACHE 2008. Lecture Notes in Computer Science; Lee, S., Choo, H., Ha, S., Shin, I.C., Eds.; Springer: Berlin, Germany, 2008; Volume 5068, pp. 427–436. [Google Scholar]
- David, O.J. NHS Direct and older people. Age Ageing 2005, 34, 499–501. [Google Scholar] [CrossRef]
- Report by the Comptroller and Auditor General, NHS Direct in England; The Stationery Office: London, UK, 25 January 2002; Available online: https://www.nao.org.uk/wp-content/uploads/2002/01/0102505.pdf (accessed on 29 November 2019).
- St George, I.; Cullen, M.; Gardiner, L.; Karabatsos, G. Universal telenursing triage in Australia and New Zealand—A new primary health service. Aust. Fam. Physician 2008, 37, 476–479. [Google Scholar]
- Miura, K.; Nagai, M.; Ohkubo, T. Epidemiology of hypertension in Japan: Where are we now? Circ. J. 2013, 77, 2226–2231. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Internal Affairs and Communication, Japan, White Paper 2014 Information and Communication in Japan. Available online: http://www.soumu.go.jp/johotsusintokei/whitepaper/ja/h26/pdf/n5300000.pdf (accessed on 29 November 2019). (In Japanese).
- Mitsutake, S.; Shibata, A.; Ishii, K.; Okazaki, K.; Oka, K. Developing Japanese version of the eHealth Literacy Scale (eHEALS). Nihon Koshu Eisei Zasshi 2011, 58, 361–371. (In Japanese) [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Sex | Total | 20–39 Years | 40–64 Years | 65–74 Years | ≥75 Years | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| ETC Users/Population | Annual CR | p-Value | ETC Users/Population | Annual CR | ETC Users/Population | Annual CR | ETC Users/Population | Annual CR | ETC Users/Population | Annual CR | |
| Men | 6650/2,943,898 | 2.3 | <0.001 * | 2831/859,561 | 3.3 | 2553/1,271,521 | 2.0 a | 675/491,988 | 1.4 a,b | 591/320,828 | 1.8 a,c |
| Women | 8607/2,999,236 | 2.9 | 3556/809,714 | 4.4 | 2982/1,213,603 | 2.5 a | 976/530,622 | 1.8 a,b | 1,093/445,297 | 2.5 a,c | |
| Overall | Men | Women | |||||
|---|---|---|---|---|---|---|---|
| Rank | Symptom/Event (n, %) | Annual CR | Symptom/Event (n, %) | Annual CR | Symptom/Event (n, %) | Annual CR | |
| 20–39 years (n = 1,669,275) | 1 | Fever (1107, 17.3%) | 0.66 | Fever (527, 18.6%) | 0.61 | Fever (580, 16.3%) | 0.72 |
| 2 | Abdominal pain (555, 8.7%) | 0.33 | Abdominal pain (205, 7.2%) | 0.24 | Abdominal pain (350, 9.8%) | 0.43 | |
| 3 | Nausea/vomiting (330, 5.2%) | 0.20 | Headache (123, 4.3%) | 0.14 | Nausea/vomiting (236, 6.6%) | 0.29 | |
| 4 | Headache (313, 4.9%) | 0.19 | Laceration (106, 3.7%) | 0.12 | Headache (190, 5.3%) | 0.23 | |
| 5 | Rash/hives (206, 3.2%) | 0.12 | Cold (95, 3.4%) | 0.11 | Rash/hives (124, 3.5%) | 0.15 | |
| 6 | Cold (203, 3.2%) | 0.12 | Nausea/vomiting (94, 3.3%) | 0.11 | Cold (108, 3.0%) | 0.13 | |
| 7 | Laceration (188, 2.9%) | 0.11 | Upper limb problem (90, 3.2%) | 0.10 | Diarrhea (87, 2.4%) | 0.11 | |
| 8 | Upper limb problem (170, 2.6%) | 0.10 | Contusion (83, 2.9%) | 0.10 | Ophthalmology-related (86, 2.4%) | 0.11 | |
| 9 | Diarrhea (164, 2.6%) | 0.10 | Diarrhea (77, 2.7%) | 0.09 | Laceration (8.2, 2.3%) | 0.10 | |
| 10 | Ophthalmology-related (163, 2.6%) | 0.10 | Ophthalmology-related (77, 2.7%) | 0.09 | Upper limb problem (80, 2.2%) | 0.10 | |
| 40–64 years (n = 2,485,124) | 1 | Fever (516, 9.3%) | 0.21 | Fever (261, 10.2%) | 0.21 | Fever (255, 8.6%) | 0.21 |
| 2 | Abdominal pain (393, 7.1%) | 0.16 | Abdominal pain (193, 7.6%) | 0.15 | Abdominal pain (200, 6.7%) | 0.16 | |
| 3 | Headache (235, 4.3%) | 0.09 | Ophthalmology-related (105, 4.1%) | 0.08 | Headache (158, 5.3%) | 0.13 | |
| 4 | Ophthalmology-related (203, 3.7%) | 0.08 | Laceration (93, 3.6%) | 0.07 | Nausea/vomiting (125, 4.2%) | 0.10 | |
| 5 | Nausea/vomiting (186, 3.7%) | 0.07 | Upper limb problem (86, 3.7%) | 0.07 | Ophthalmology-related (98, 3.3%) | 0.08 | |
| 6 | Laceration (173, 3.1%) | 0.07 | Headache (77, 3.0%) | 0.06 | Dizziness (88, 3.0%) | 0.07 | |
| 7 | Upper limb problem (165, 3.0%) | 0.07 | Numbness (76, 3.0%) | 0.06 | Rash/hives (81, 2.7%) | 0.07 | |
| 8 | Rash/hives (150, 2.7%) | 0.06 | Rash/hives (69, 2.7%) | 0.05 | Laceration (80, 2.7%) | 0.07 | |
| 9 | Numbness (147, 2.7%) | 0.06 | Contusion (69, 2.7%) | 0.05 | Upper limb problem (79, 2.6%) | 0.06 | |
| 10 | Dizziness (146, 2.6%) | 0.06 | Problems from ankle to toe (65, 2.5%) | 0.05 | Chest pain (74, 2.5%) | 0.06 | |
| 65–74 years (n = 1,022,610) | 1 | Abdominal pain (107, 6.5%) | 0.10 | Fever (53, 7.9%) | 0.11 | Abdominal pain (69, 7.1%) | 0.13 |
| 2 | Fever (105, 6.4%) | 0.10 | Abdominal pain (38, 5.6%) | 0.08 | Hypertension (55, 5.6%) | 0.10 | |
| 3 | Hypertension (77, 4.7%) | 0.08 | Nausea/vomiting (29, 4.3%) | 0.06 | Fever (52, 5.3%) | 0.10 | |
| 4 | Nausea/vomiting (75, 4.5%) | 0.07 | Dizziness (29, 4.3%) | 0.06 | Nausea/vomiting (46, 4.7%) | 0.09 | |
| 5 | Dizziness (75, 4.5%) | 0.07 | Numbness (25, 3.7%) | 0.05 | Dizziness (46, 4.7%) | 0.09 | |
| 6 | Ophthalmology-related (62, 3.8%) | 0.06 | Consciousness disorder (22, 3.3%) | 0.04 | Ophthalmology-related (41, 4.2%) | 0.08 | |
| 7 | Bite (57, 3.5%) | 0.06 | Hypertension (22, 3.3%) | 0.04 | Bite (38, 3.9%) | 0.07 | |
| 8 | Contusion (50, 3.0%) | 0.05 | Upper limb problem (22, 3.3%) | 0.04 | Contusion (35, 3.6%) | 0.07 | |
| 9 | Numbness (48, 2.9) | 0.05 | Ophthalmology-related (21, 3.3%) | 0.04 | Headache (33, 3.4%) | 0.06 | |
| 10 | Rash/hives (46, 2.9%) | 0.04 | Nose problem (19, 2.8%) | 0.04 | Rash/hives (30, 3.0%) | 0.06 | |
| ≥75 years (n = 766,125) | 1 | Fever (150, 8.9%) | 0.20 | Fever (67, 11.3%) | 0.21 | Fever (83, 7.6%) | 0.19 |
| 2 | Nausea/vomiting (81, 4.8%) | 0.11 | Nausea/vomiting (38, 6.4%) | 0.12 | Contusion (50, 4.6%) | 0.11 | |
| 3 | Hypertension (68, 4.0%) | 0.09 | Consciousness disorder (27, 4.6%) | 0.08 | Hypertension (47, 4.3%) | 0.11 | |
| 4 | Contusion (65, 3.9%) | 0.08 | Abdominal pain (24, 4.1%) | 0.07 | Nausea/vomiting (43, 3.9%) | 0.11 | |
| 5 | Abdominal pain (60, 3.6%) | 0.08 | Hypertension (21, 3.6%) | 0.07 | Head injury (41, 3.8%) | 0.09 | |
| 6 | Consciousness disorder (58, 3.4%) | 0.08 | Numbness (20, 3.4%) | 0.06 | Dizziness (38, 3.5%) | 0.08 | |
| 7 | Dizziness (57, 3.4%) | 0.07 | Dizziness (19, 3.2%) | 0.06 | Abdominal pain (36, 3.3%) | 0.08 | |
| 8 | Head injury (53, 3.1%) | 0.07 | Nose problem (18, 3.0%) | 0.06 | Ophthalmology-related (35, 3.2%) | 0.07 | |
| 9 | Leg problem (51, 3.0%) | 0.07 | Leg problem (16, 2.7%) | 0.05 | Leg problem (35, 3.2%) | 0.07 | |
| 10 | Ophthalmology-related (46, 2.7%) | 0.06 | Contusion (15, 2.5%) | 0.05 | Facial and extremity injury (33, 3.0%) | 0.07 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakamura, A.; Manabe, T.; Teraura, H.; Kotani, K. Age and Sex Differences in the Use of Emergency Telephone Consultation Services in Saitama, Japan: A Population-Based Observational Study. Int. J. Environ. Res. Public Health 2020, 17, 185. https://doi.org/10.3390/ijerph17010185
Nakamura A, Manabe T, Teraura H, Kotani K. Age and Sex Differences in the Use of Emergency Telephone Consultation Services in Saitama, Japan: A Population-Based Observational Study. International Journal of Environmental Research and Public Health. 2020; 17(1):185. https://doi.org/10.3390/ijerph17010185
Chicago/Turabian StyleNakamura, Akihisa, Toshie Manabe, Hiroyuki Teraura, and Kazuhiko Kotani. 2020. "Age and Sex Differences in the Use of Emergency Telephone Consultation Services in Saitama, Japan: A Population-Based Observational Study" International Journal of Environmental Research and Public Health 17, no. 1: 185. https://doi.org/10.3390/ijerph17010185
APA StyleNakamura, A., Manabe, T., Teraura, H., & Kotani, K. (2020). Age and Sex Differences in the Use of Emergency Telephone Consultation Services in Saitama, Japan: A Population-Based Observational Study. International Journal of Environmental Research and Public Health, 17(1), 185. https://doi.org/10.3390/ijerph17010185