Tuberculosis-Related Hospitalizations in a Low-Incidence Country: A Retrospective Analysis in Two Italian Infectious Diseases Wards

 , ,
, ,  , , ,
, , ,  , and
, and
Abstract
1. Introduction
2. Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| CI | confidence interval |
| DST | drug susceptibility test |
| ECDC | European Center for Disease Prevention and Control |
| EPTB | extrapulmonary tuberculosis |
| ERS | European Respiratory Society |
| HIV | human immunodeficiency virus |
| IGRA | interferon-gamma release assay |
| IQR | interquartile range |
| MDR | multi-drug-resistant |
| MTB | Mycobacterium tuberculosis |
| NTM | nontuberculous mycobacteria |
| PTB | pulmonary tuberculosis |
| SD | standard deviation |
| TB | tuberculosis |
| USA | United States of America |
| XDR | extensively drug-resistant |
| WHO | World Health Organization |
References
- World Health Organization. Global Tuberculosis Report 2018; World Health Organization: Geneva, Switzerland, 2018; Available online: https://www.who.int/tb/publications/global_report/MainReport_18Sept2018.pdf?ua=1 (accessed on 1 November 2019).
- Hollo, V.; Beauté, J.; Ködmön, C.; van der Werf, M.J. Tuberculosis notification rate decreases faster in residents of native origin than in residents of foreign origin in the EU/EEA, 2010 to 2015. Euro Surveill. 2017, 22, 30486. [Google Scholar] [CrossRef] [PubMed]
- Stewart, R.J.; Tsang, C.A.; Pratt, R.H.; Price, S.F.; Langer, A.J. Tuberculosis—United States, 2017. MMWR Morb. Mortal. Wkly. Rep. 2018, 67, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Cowger, T.L.; Wortham, J.M.; Burton, D.C. Epidemiology of tuberculosis among children and adolescents in the USA, 2007–2017: An analysis of national surveillance data. Lancet Public Health 2019, 4, e506–e516. [Google Scholar] [CrossRef]
- Lönnroth, K.; Mor, Z.; Erkens, C.; Bruchfeld, J.; Nathavitharana, R.R.; Van Der Werf, M.J.; Lange, C. Tuberculosis in migrants in low-incidence countries: Epidemiology and intervention entry points. Int. J. Tuberc. Lung Dis. 2017, 21, 624–637. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.openpolis.it/numeri/gli-sbarchi-italia-negli-ultimi-10-anni/fonte: Ministero dell’Interno (accessed on 1 November 2019).
- Scotto, G.; Fazio, V.; Lo Muzio, L. Tuberculosis in the immigrant population in Italy: State-of-the-art review. Infez Med. 2017, 25, 199–209. [Google Scholar] [PubMed]
- Banta, J.E.; Ani, C.; Bvute, K.M.; Lloren, J.I.C.; Darnell, T.A. Pulmonary vs. extra-pulmonary tuberculosis hospitalizations in the US [1998–2014]. J. Infect. Public Health 2019. [Google Scholar] [CrossRef]
- eCDC. European Union Standards for Tuberculosis Care. Available online: https://ecdc.europa.eu/en/all-topics-ztuberculosisprevention-and-control/european-union-standards-tuberculosis-care (accessed on 1 November 2019).
- Compendium of WHO Guidelines and Associated Standards: Ensuring Optimum Delivery of the Cascade of Care for Patients with Tuberculosis, 2nd ed.; World Health Organization: Geneva, Switzerland, 2018; Available online: https://apps.who.int/iris/bitstream/handle/10665/272644/9789241514101-eng.pdf?ua=1 (accessed on 1 November 2019).
- Forbes, B.A.; Banaiee, N.; Beavis, K.G.; Brown-Elliott, B.A.; Della Latta, P.; Elliott, L.B.; Elliott, L.B.; Hall, G.S.; Hanna, B.; Perkins, M.D.; et al. Laboratory Detection and Identification of Mycobacteria; Approved Guideline, 1st ed.; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2008. [Google Scholar]
- Gilbert, R.L.; Antoine, D.; French, C.E.; Abubakar, I.; Watson, J.M.; Jones, J.A. The impact of immigration on tuberculosis rates in the United Kingdom compared with other European countries. Int. J. Tuberc. Lung Dis. 2009, 13, 645–651. [Google Scholar]
- González-García, A.; Fortún, J.; Elorza Navas, E.; Martín-Dávila, P.; Tato, M.; Gómez-Mampaso, E.; Moreno, S. The changing epidemiology of tuberculosis in a Spanish tertiary hospital (1995–2013). Medicine (Baltim.) 2017, 96, e7219. [Google Scholar] [CrossRef]
- Baussano, I.; Mercadante, S.; Pareek, M.; Lalvani, A.; Bugiani, M. High Rates of Mycobacterium tuberculosis among Socially Marginalized Immigrants in Low-Incidence Area, 1991–2010, Italy. Emerg. Infect. Dis. 2013, 19, 1437–1445. [Google Scholar] [CrossRef]
- Ingrosso, L.; Vescio, F.; Giuliani, M.; Migliori, G.B.; Fattorini, L.; Severoni, S.; Rezza, G. Risk Factors for Tuberculosis in Foreign-Born People (FBP) in Italy: A Systematic Review and Meta-Analysis. PLoS ONE 2014, 9, e94728. [Google Scholar] [CrossRef]
- Lombardi, G.; Dal Monte, P.; Denicolò, A.; Tadolini, M.; Martelli, G.; Bacchi Reggiani, M.L.; Viale, P.; Landini, M.P. Trend of microbiologically-confirmed tuberculosis in a low-incidence setting with high immigration rates. BMC Public Health 2014, 14, 340. [Google Scholar] [CrossRef] [PubMed]
- Odone, A.; Riccò, M.; Morandi, M.; Borrini, B.M.; Pasquarella, C.; Signorelli, C. Epidemiology of tuberculosis in a low-incidence Italian region with high immigration rates: Differences between not Italy-born and Italy-born TB cases. BMC Public Health 2011, 11, 376. [Google Scholar] [CrossRef] [PubMed]
- Odone, A.; Tillmann, T.; Sandgren, A.; Williams, G.; Rechel, B.; Ingleby, D.; Noori, T.; Mladovsky, P.; McKee, M. Tuberculosis among migrant populations in the European Union and the European Economic Area. Eur. J. Public Health 2015, 25, 506–512. [Google Scholar] [CrossRef] [PubMed]
- Peto, H.M.; Pratt, R.H.; Harrington, T.A.; LoBue, P.A.; Armstrong, L.R. Epidemiology of Extrapulmonary Tuberculosis in the United States, 1993–2006. Clin. Infect. Dis. 2009, 49, 1350–1357. [Google Scholar] [CrossRef] [PubMed]
- Villa, S.; Codecasa, L.R.; Faccini, M.; Pontello, M.M.; Ferrarese, M.; Castellotti, P.F.; Senatore, S.; Lamberti, A.; Mazzola, E.; Perno, C.F.; et al. Tuberculosis among asylum-seekers in Milan, Italy: Epidemiological analysis and evaluation of interventions. Eur. Respir. J. 2019, 54, 1900896. [Google Scholar] [CrossRef]
- Birchall Jenny; Part of the BRIDGE Team; Institute of Development Studies (IDS). Available online: https://www.rosavzw.be/digidocs/dd-001417_2016_Gender_Age_Migration_IDS.pdf (accessed on 1 November 2019).
- Casal, M.; Vaquero, M.; Rinder, H.; Tortoli, E.; Grosset, J.; Rush-Gerdes, S.; Gutierrez, J.; Jarlier, V. A case-control study for multidrug-resistant tuberculosis: Risk factors in four European countries. Microb. Drug Resist. 2005, 11, 62–67. [Google Scholar] [CrossRef]
- Fronti, E.; Vecchia, M.; Scudeller, L.; Praticò, L.; Marone, P.; Muzzi, A.; Minoli, L.; Seminari, E. Epidemiology of Mycobacterium tuberculosis infection in Pavia province, Lombardy, Northern Italy, 1998–2013. New Microbiol. 2016, 39, 264–268. [Google Scholar]
- European Centre for Disease Prevention and Control/WHO Regional Office for Europe. Tuberculosis Surveillance and Monitoring in Europe 2018–2016 Data. Available online: https://www.ecdc.europa.eu/sites/portal/files/documents/ecdc-tuberculosis-surveillance-monitoring-Europe-2018-19mar2018.pdf (accessed on 1 November 2019).
- Sotgiu, G.; Falzon, D.; Hollo, V.; Ködmön, C.; Lefebvre, N.; Dadu, A.; van der Werf, M. Determinants of site of tuberculosis disease: An analysis of European surveillance data from 2003 to 2014. PLoS ONE 2017, 12, e0186499. [Google Scholar] [CrossRef]
- Ade, S.; Harries, A.D.; Trébucq, A.; Ade, G.; Agodokpessi, G.; Adjonou, C.; Azon, S.; Anagonou, S. National profile and treatment outcomes of patients with extrapulmonary tuberculosis in Bénin. PLoS ONE 2014, 9, e95603. [Google Scholar] [CrossRef]
- Tesgaye, F.; Defar, A.; Beyene, T.; Shafi, O.; Klinkenberg, E.; Howe, R. Documentation and treatment outcomes of smear-negative and extra-pulmonary tuberculosis in Ethiopia. Public Health Action 2014, 4 (Suppl. S3), S25–S30. [Google Scholar] [CrossRef]
- Ohene, S.A.; Bakker, M.I.; Ojo, J.; Toonstra, A.; Awudi, D.; Klatser, P. Extra-pulmonary tuberculosis: A retrospective study of patients in Accra, Ghana. PLoS ONE 2019, 14, e0209650. [Google Scholar] [CrossRef] [PubMed]
- Pollett, S.; Banner, P.; O’Sullivan, M.V.; Ralph, A.P. Epidemiology, Diagnosis and Management of Extra-Pulmonary Tuberculosis in a Low-Prevalence Country: A Four Year Retrospective Study in an Australian Tertiary Infectious Diseases Unit. PLoS ONE 2016, 11, e0149372. [Google Scholar] [CrossRef] [PubMed]
- Sankar, M.M.; Singh, J.; Diana, S.C.; Singh, S. Molecular characterization of Mycobacterium tuberculosis isolates from North Indian patients with extrapulmonary tuberculosis. Tuberculosis (Edinb) 2013, 93, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Gomes, T.; Vinhas, S.A.; Reis-Santos, B.; Palaci, M.; Peres, R.L.; Aguiar, P.P.; Correa Ribeiro, F.K.; Marques, H.S.; do Valle Dettoni, V.; Johnson, J.L.; et al. Extrapulmonary tuberculosis: Mycobacterium tuberculosis strains and host risk factors in a large urban setting in Brazil. PLoS ONE 2013, 8, e74517. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Overall n = 166 | Italian (n = 52) | Foreign-Born (n = 114) | p-Value & | |
|---|---|---|---|---|---|
| Year of diagnosis, n (%) | 2013 | 17 (10.2) | 3 (5.8) | 14 (12.3) | 0.29 |
| 2014 | 20 (12.1) | 6 (11.5) | 14 (12.3) | ||
| 2015 | 34 (20.5) | 13 (25.0) | 21 (18.4) | ||
| 2016 | 58 (34.9) | 22 (42.3) | 36 (31.6) | ||
| 2017 | 37 (22.3) | 8 (15.4) | 29 (25.4) | ||
| Median (IQR) age, years | 37 (26–55) | 71.5 (44.5–80.0) | 30 (24–40) | <0.0001 | |
| Age >65 years | 31 (18.7) | 31 (59.62) | 0 (0.0) | <0.0001 | |
| Age group, n (%) | 0–24 | 31 (18.7) | 2 (3.9) | 29 (25.4) | 0.001 |
| 25–44 | 74 (44.6) | 11 (21.2) | 63 (55.3) | <0.0001 | |
| 45–64 | 30 (18.1) | 8 (15.4) | 22 (19.3) | 0.55 | |
| 65–79 | 17 (10.2) | 17 (32.7) | 0 (0.0) | <0.0001 | |
| ≥80 | 14 (8.4) | 14 (26.9) | 0 (0.0) | <0.0001 | |
| Males, n (%) | 118 (71.1) | 32 (61.5) | 86 (75.4) | 0.07 | |
| Immunodepression, n (%) | 45 (27.1) | 25 (48.1) | 20 (17.5) | <0.0001 | |
| Causes of immunodepression, n (%) | HIV positivity | 14 (31.1) | 4 (16.0) | 10 (50.0) | 0.01 |
| Hematological diseases | 6 (13.3) | 6 (24.0) | 0 (0.0) | 0.02 | |
| Alcohol | 4 (8.9) | 1 (4.0) | 3 (15.0) | 0.20 | |
| Diabetes mellitus | 4 (8.9) | 2 (8.0) | 2 (10.0) | 0.82 | |
| Solid tumor | 4 (8.9) | 4 (16.0) | 0 (0.0) | 0.06 | |
| Malnutrition | 4 (8.9) | 1 (4.0) | 3 (15.0) | 0.20 | |
| Autoimmune disease | 3 (6.7) | 3 (12.0) | 0 (0.0) | 0.11 | |
| Chronic renal failure | 2 (4.4) | 1 (4.0) | 1 (5.0) | 0.87 | |
| Other diseases | 4 (8.9) | 3 (12.0) | 1 (5.0) | 0.41 | |
| Comorbidity *, n (%) | 39 (23.5) | 23 (44.2) | 16 (14.0) | <0.0001 | |
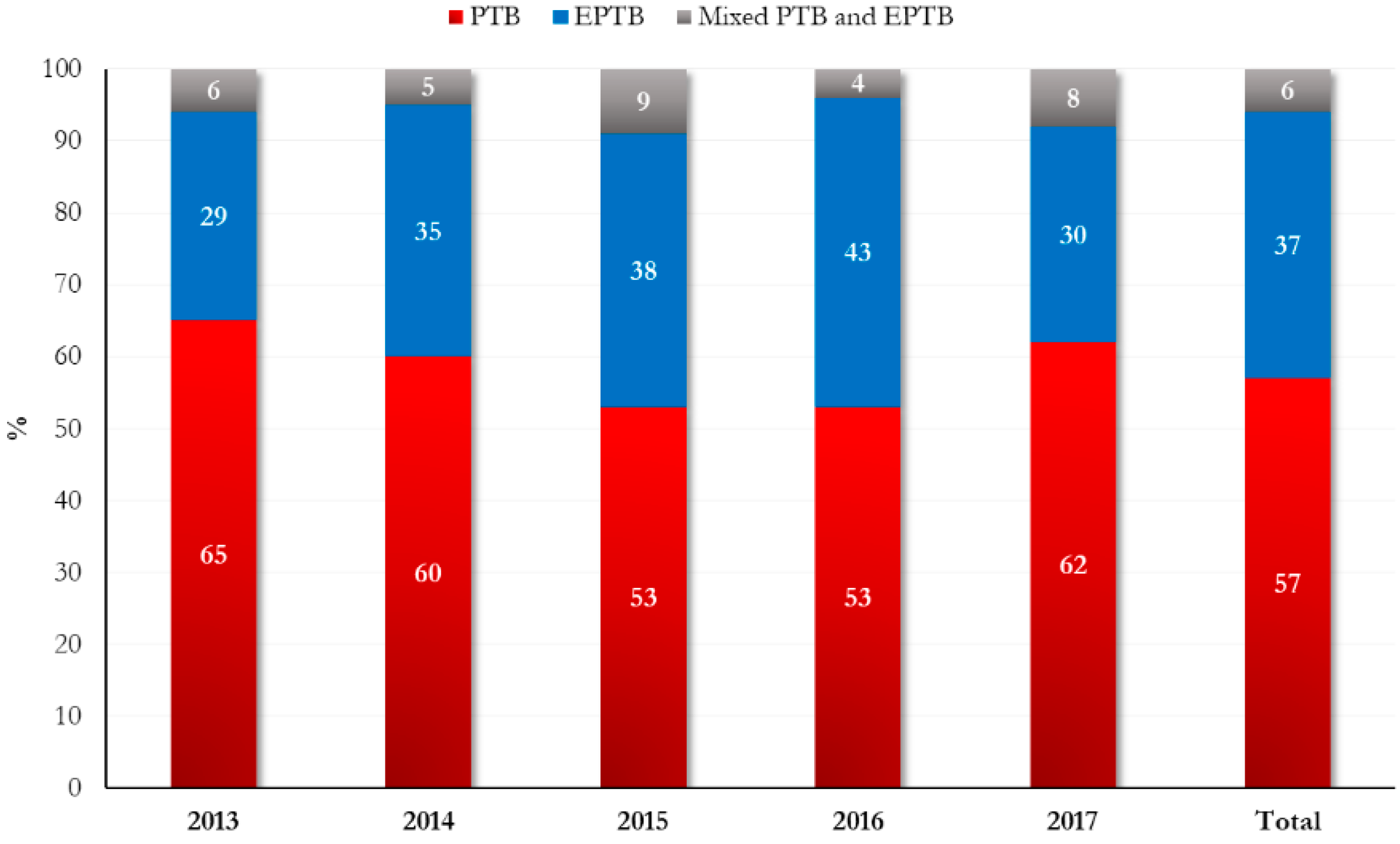
| TB form, n (%) | PTB ** | 95 (57.2) | 32 (61.5) | 63 (55.3) | 0.66 |
| EPTB *** | 61 (36.8) | 18 (34.6) | 43 (37.7) | ||
| PTB and EPTB | 10 (6.0) | 2 (3.9) | 8 (7.0) | ||
| TB drug resistance, n (%) | 16 (13.0) | 1 (2.9) | 15 (17.1) | 0.04 | |
| Variables | Pulmonary (n = 95) | Extrapulmonary (n = 61) | p-Value | |
|---|---|---|---|---|
| Year of diagnosis, n (%) | 2013 | 11 (11.6) | 5 (8.2) | 0.74 |
| 2014 | 12 (12.6) | 7 (11.5) | ||
| 2015 | 18 (19.0) | 13 (21.3) | ||
| 2016 | 31 (32.6) | 25 (41.0) | ||
| 2017 | 23 (24.2) | 11 (18.0) | ||
| Median (IQR) age, years | 39 (29–58) | 32 (24–55) | 0.07 | |
| Age >65 years | 19 (20.0) | 12 (19.7) | 0.96 | |
| Age group, n (%) | 0–24 | 10 (10.5) | 16 (26.2) | 0.13 |
| 25–44 | 48 (50.5) | 23 (37.7) | ||
| 45–64 | 18 (19.0) | 10 (16.4) | ||
| 65–79 | 10 (10.5) | 7 (11.5) | ||
| ≥80 | 9 (9.5) | 5 (8.2) | ||
| Males, n (%) | 65 (68.4) | 45 (73.8) | 0.48 | |
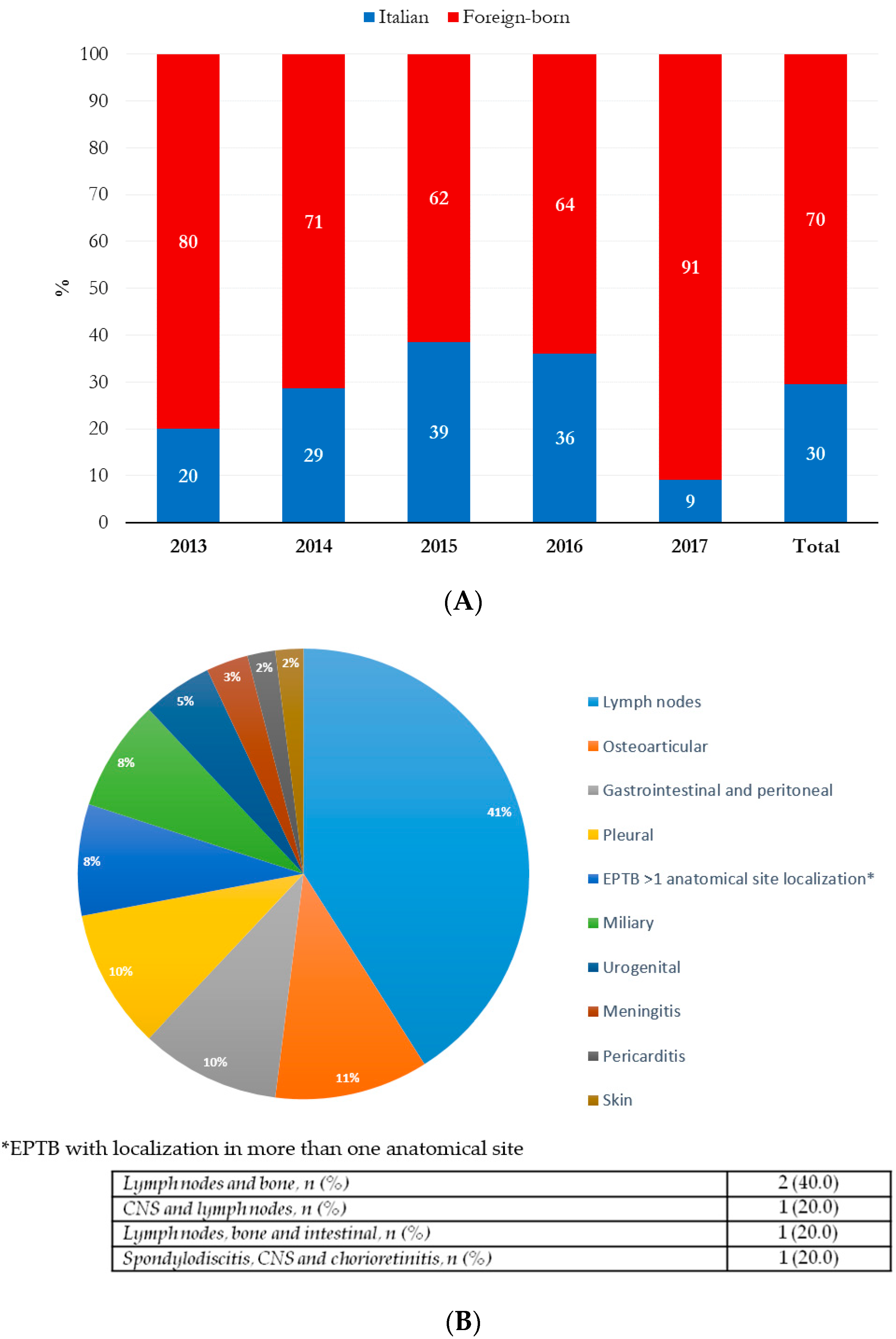
| Geographical area of origin, n (%) | Italy | 32 (33.7) | 18 (29.5) | 0.59 |
| Africa | 19 (20.0) | 24 (39.3) | 0.01 | |
| Europe | 35 (36.8) | 7 (11.5) | 0.001 | |
| Other countries * | 9 (9.5) | 12 (19.7) | 0.07 | |
| Immunodepression, n (%) | 17 (17.9) | 23 (37.7) | 0.006 | |
| Causes of immunodepression, n (%) | HIV positivity | 3 (17.7) | 10 (43.5) | 0.18 |
| Hematological diseases | 1 (5.9) | 5 (21.7) | ||
| Alcohol | 4 (23.5) | 0 (0.0) | ||
| Diabetes mellitus | 2 (11.8) | 2 (8.7) | ||
| Solid tumor | 2 (11.8) | 2 (8.7) | ||
| Malnutrition | 0 (0.0) | 1 (4.4) | ||
| Autoimmune disease | 2 (11.8) | 1 (4.4) | ||
| Chronic renal failure | 1 (5.9) | 1 (4.4) | ||
| Other diseases | 2 (11.8) | 1 (4.4) | ||
| Comorbidity &, n (%) | 16 (16.8) | 21 (34.4) | 0.01 | |
| Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | ||
| Age, years | 1.0 (1.0–1.0) | 0.21 | 1.0 (1.0–1.0) | 0.98 | |
| Age >65 years | 1.0 (0.4–2.2) | 0.96 | - | - | |
| Age groups | 0.9 (0.7–1.1) | 0.29 | - | - | |
| Males | 1.3 (0.6–2.7) | 0.48 | 1.3 (0.6–2.9) | 0.58 | |
| Foreign-born | 1.2 (0.6–2.4) | 0.59 | - | - | |
| Geographical area of origin | Italy | 0.8 (0.4–1.7) | 0.59 | - | - |
| Africa | 2.6 (1.3–5.3) | 0.009 | 0.8 (0.3–2.6) | 0.76 | |
| Eastern Europe | 0.2 (0.1–0.5) | 0.001 | - | - | |
| Other countries * | 2.3 (0.9–5.9) | 0.07 | - | - | |
| European origin | 0.3 (0.2–0.7) | <0.0001 | 0.2 (0.1–0.6) | 0.004 | |
| HIV positivity | 6.0 (1.6–22.8) | 0.008 | 2.3 (0.4–12.1) | 0.33 | |
| Hematological diseases | 8.4 (1.0–73.7) | 0.06 | - | - | |
| Other causes of immunodepression | 1.0 (0.4–2.5) | 0.91 | - | - | |
| Comorbidity & | 2.5 (1.2–5.3) | 0.01 | 3.4 (1.1–10.4) | 0.03 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Campogiani, L.; Compagno, M.; Coppola, L.; Malagnino, V.; Maffongelli, G.; Saraca, L.M.; Francisci, D.; Baldelli, F.; Fontana, C.; Grelli, S.; et al. Tuberculosis-Related Hospitalizations in a Low-Incidence Country: A Retrospective Analysis in Two Italian Infectious Diseases Wards. Int. J. Environ. Res. Public Health 2020, 17, 124. https://doi.org/10.3390/ijerph17010124
Campogiani L, Compagno M, Coppola L, Malagnino V, Maffongelli G, Saraca LM, Francisci D, Baldelli F, Fontana C, Grelli S, et al. Tuberculosis-Related Hospitalizations in a Low-Incidence Country: A Retrospective Analysis in Two Italian Infectious Diseases Wards. International Journal of Environmental Research and Public Health. 2020; 17(1):124. https://doi.org/10.3390/ijerph17010124
Chicago/Turabian StyleCampogiani, Laura, Mirko Compagno, Luigi Coppola, Vincenzo Malagnino, Gaetano Maffongelli, Lavinia Maria Saraca, Daniela Francisci, Franco Baldelli, Carla Fontana, Sandro Grelli, and et al. 2020. "Tuberculosis-Related Hospitalizations in a Low-Incidence Country: A Retrospective Analysis in Two Italian Infectious Diseases Wards" International Journal of Environmental Research and Public Health 17, no. 1: 124. https://doi.org/10.3390/ijerph17010124
APA StyleCampogiani, L., Compagno, M., Coppola, L., Malagnino, V., Maffongelli, G., Saraca, L. M., Francisci, D., Baldelli, F., Fontana, C., Grelli, S., Andreoni, M., Sotgiu, G., Saderi, L., & Sarmati, L. (2020). Tuberculosis-Related Hospitalizations in a Low-Incidence Country: A Retrospective Analysis in Two Italian Infectious Diseases Wards. International Journal of Environmental Research and Public Health, 17(1), 124. https://doi.org/10.3390/ijerph17010124