How Do Type 2 Diabetes Patients Value Urban Integrated Primary Care in China? Results of a Discrete Choice Experiment

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Setting
2.2. DCE Design
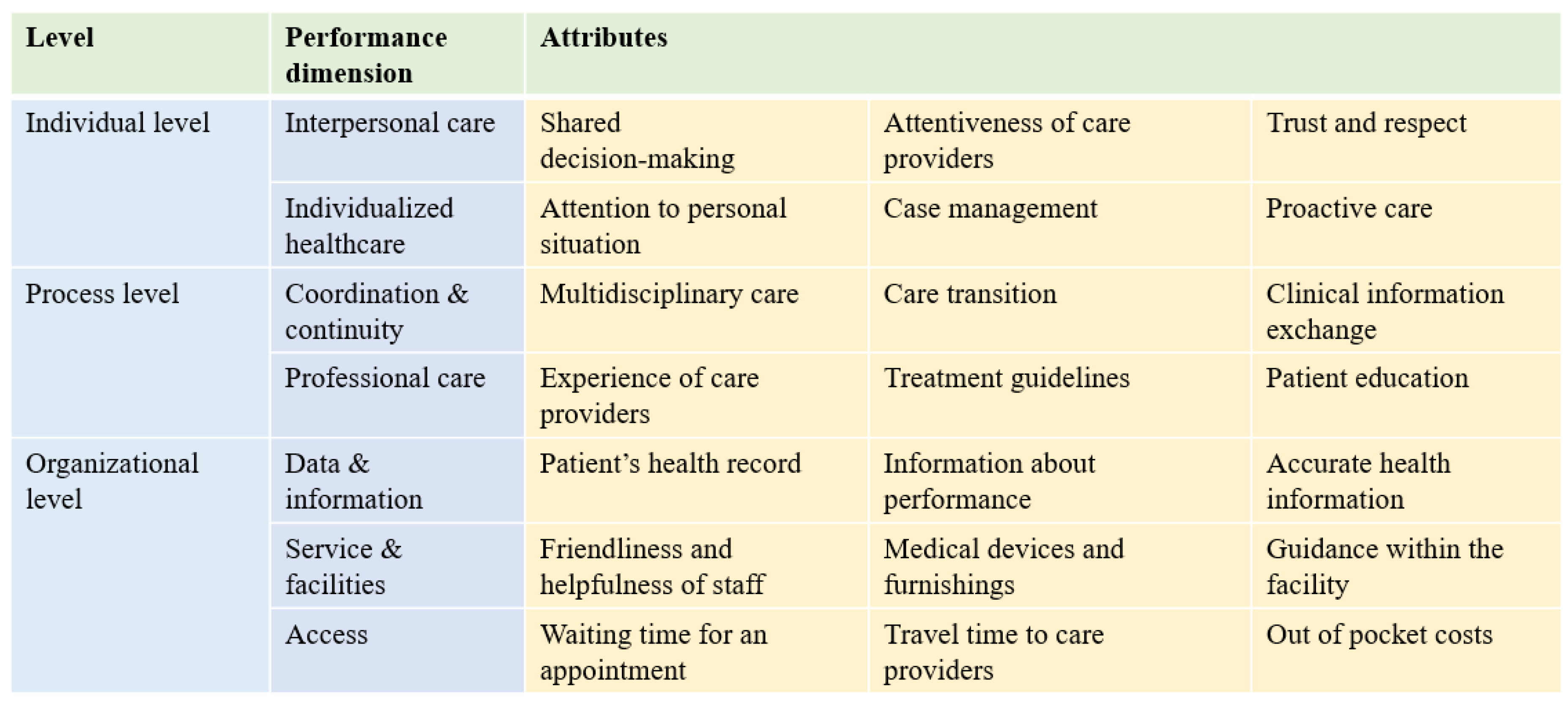
2.2.1. Attributes and Levels
2.2.2. Questionnaire
2.2.3. Sampling and Data Collection
2.3. Data Analysis
2.3.1. Willingness to Pay
2.3.2. Impact of Policy Change
3. Results
3.1. Respondents’ Characteristics
3.2. Preferences for CHS Attributes and Willingness to Pay
3.3. Impact of Policy Change
4. Discussion
4.1. Interpretation of the Results
4.2. Strengths and Limitations
5. Conclusions
6. Data Availability
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- National Diabetes Study Group. A mass survey of diabetes mellitus in a population of 300,000 in 14 provinces and municipalities in China. Chin. J. Intern. Med. 1981, 20, 678–683. (In Chinese) [Google Scholar]
- He, X.W.; Pan, J.; Pan, M.X.; Wang, J.; Dong, J.; Yuan, H.; Zhou, L.; Chen, M.; Chen, Y.; Lu, Y.; et al. Dietary and physical activity of adult patients with type 2 diabetes in Zhejiang province of eastern China: Data from a cross-sectional study. J. Diabetes Investig. 2016, 7, 529–538. [Google Scholar] [CrossRef]
- Chan, J.C.; Zhang, Y.Y.; Ning, G. Diabetes in China: A societal solution for a personal challenge. Lancet Diabetes Endocrinol. 2014, 2, 969–979. [Google Scholar] [CrossRef]
- Institute for Health Metrics and Evaluation. GBD 2016. University of Washington. Available online: https://vizhub.healthdata.org/gbd-compare/ (accessed on 8 May 2019).
- Ma, R.C.W. Epidemiology of diabetes and diabetic complications in China. Diabetologia 2018, 61, 1249–1260. [Google Scholar] [CrossRef]
- Global Report on Diabetes; World Health Organization: Geneva, Switzerland, 2016.
- Yip, W.; Hsiao, W.C. What drove the cycles of Chinese health system reforms? Health Syst. Reform 2015, 1, 52–61. [Google Scholar] [CrossRef]
- Yip, W.; Hsiao, W.C. Harnessing the privatisation of China’s fragmented healthcare delivery. Lancet 2014, 384, 805–818. [Google Scholar] [CrossRef]
- Wang, L.M.; Gao, P.; Zhang, M.; Huang, Z.; Zhang, D.; Deng, Q.; Li, Y.; Zhao, Z.; Qin, X.; Jin, D.; et al. Prevalence and ethnic pattern of diabetes and prediabetes in China in 2013. JAMA 2017, 317, 2515–2523. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.L.; Xu, Z.L.; Jia, J.T.; Xie, Y.; Wang, H.X.; Qi, X.Y. Detection of prediabetes and undiagnosed type 2 diabetes: A large population-based study. Can. J. Diabetes 2012, 36, 108–113. [Google Scholar] [CrossRef]
- Wang, S.Y.; Marquez, P.; Langenbrunner, J. Toward a Healthy and Harmonious Life in China: Stemming the Rising Tide of Non-Communicable Diseases: Human Development Unit; The World Bank: Washington, DC, USA, 2011. [Google Scholar]
- Chen, Z. Launch of the health-care reform plan in China. Lancet 2009, 373, 1322–1324. [Google Scholar] [CrossRef]
- Ministry of Health. Ministry of Finance and National Population and Family Planning Commission. Promoting the Equalization of Basic Public Health Services; Ministry of Health: Beijing, China, 2009. (In Chinese)
- Zhao, Y.H.; Crimmins, E.M.; Hu, P. Prevalence, diagnosis, and management of diabetes mellitus among older Chinese: Results from the China Health and Retirement Longitudinal Study. Int. J. Public Health 2016, 61, 347–356. [Google Scholar] [CrossRef]
- World Health Organization. Integrated Health Services—What and Why? WHO: Geneva, Switzerland, 2008. [Google Scholar]
- People-Centred and Integrated Health Services: An Overview of the Evidence: Interim Report; World Health Organization: Geneva, Switzerland, 2015; Available online: http://apps.who.int/iris/bitstream/handle/10665/155004/ (accessed on 16 May 2019).
- Clark, M.D.; Deternann, D.; Petrou, S.; Moro, D.; de Bekker-Grob, E.W. Discrete Choice Experiments in Health Economics: A Review of the Literature. Pharm. Econ. 2014, 32, 883–902. [Google Scholar] [CrossRef] [PubMed]
- Kleij, K.S.; Tangermann, U.; Amelung, V.E.; Krauth, C. Patients’ preferences for primary health care-a systematic literature review of discrete choice experiments. BMC Health Serv. Res. 2017, 17, 476–488. [Google Scholar] [CrossRef] [PubMed]
- Verelst, F.; Willem, L.; Kessels, R.; Beutels, P. Individual decisions to vaccinate one’s child or oneself: A discrete choice experiment rejecting free-riding motives. Soc. Sci. Med. 2018, 207, 106–116. [Google Scholar] [CrossRef] [PubMed]
- Deternann, D.; Lambooij, M.S.; de Bekker-Grob, E.W.; Hayen, P.A.; Varkevisser, M.; Schut, F.T.; deWit, G.A. What health plans do people prefer? The trade-off between premium and provider choice. Soc. Sci. Med. 2016, 165, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Mühlbacher, A.C.; Bethge, S. Preferences for supply network works: Characteristics of integrated supplying programs and their influence on the patient use. Das. Gesundh. 2015, 77, 340–350. (In German) [Google Scholar]
- Mühlbacher, A.C.; Bethge, S.; Reed, S.D.; Schulman, K.A. Patient preferences for features of health care delivery systems: A discrete-choice experiment. Health Serv. Res. 2015, 51, 704–727. [Google Scholar] [CrossRef]
- The National Health and Family Planning Commission and the State Council held the Onsite Promotion Meeting of Medical Consortia in Shenzhen; National Health and Family Planning Commission of the People’s Republic of China: Beijing, China, 2017. Available online: http:// www.nhfpc.gov.cn/zhuz/xwfb/201709/295f949f5b3f483a9267d922b2aca6a1.shtml (accessed on 13 May 2019).
- Wang, X.; Sun, X.Z.; Stephen, B.; Gong, F.; Pim, V.; Chen, L.; Zhang, Y.; Huang, Y.; Yang, H. People-centered integrated care in urban China. B World Health Organ. 2018, 96, 843–852. [Google Scholar] [CrossRef]
- Zhang, D.; Mou, J.; Cheng, J.Q.; Griffiths, S.M. Public health services in Shenzhen: A case study. Public Health 2011, 125, 15–19. [Google Scholar] [CrossRef]
- Zhang, T.; Lv, C.; Li, L.; Chen, S.; Liu, S.; Wang, C.; Su, B. Plasma miR-126 is a potential biomarker for early prediction of type 2 diabetes mellitus in susceptible individuals. Biomed. Res. Int. 2013. [Google Scholar] [CrossRef]
- Statistic Yearbook of Shenzhen in 2015; Shenzhen Bureau of Statistics: Shenzhen, China, 2016. Available online: http://www.sztj.gov.cn/xxgk/zfxxgkml/tjsj/tjnj/201701/P020181106396578077129.pdf (accessed on 13 May 2019).
- Abiiro, G.A.; Leppert, G.; Mbera, G.B.; Robyn, P.J.; De Allegri, M. Developing attributes and attribute-levels for a discrete choice experiment on micro health insurance in rural Malawi. BMC Health Serv. Res. 2014, 14, 235. [Google Scholar] [CrossRef]
- Juhnke, C.; Mühlbacher, A.C. Patient-centredness in integrated healthcare delivery systems-needs, expectations and priorities for organized healthcare systems. Int. J. Integr. Care 2013, 13, 1–14. [Google Scholar] [CrossRef]
- Dong, Y.Q.; Qian, Y.; Wang, X.X.; Dong, M.; Wuxi Center for Disease Control and Prevention. Direct economic burden of elderly patients with chronic diseases in communities of Wuxi city. Chin. J. Cont. Chronic. Dis. 2015, 23, 175–181. [Google Scholar]
- Kuhfeld, W.F. Marketing Research Methods in SAS: Experimental Design, Choice, Conjoint and Graphical Techniques; SAS Institute: Cary, NC, USA, 2010. [Google Scholar]
- Edgar, A.L.; Amarech, G.O.; Catherine, D.; Regien, B. What’s influences where they seek care? Caregivers’ perspectives for under-five child healthcare services in urban slums of Malawi: A discrete choice experiment. PLoS ONE 2018, 13, e0189940. [Google Scholar] [CrossRef]
- Revelt, D.; Train, K. Mixed logit with repeated choices: Household’s choices of appliance efficiency level. Rev. Econ. Stat. 1998, 80, 647–657. [Google Scholar] [CrossRef]
- Wang, X.; Sun, X.Z.; Gong, F.F.; Huang, Y.; Chen, L.; Zhang, Y.; Stephen, B. The Luohu Model: A Template for Integrated Urban Healthcare Systems in China. Int. J. Integr. Care 2018, 18, 3. [Google Scholar] [CrossRef]
- World Health Organization. WHO Global Strategy on People-Centred and Integrated Health Services: Interim Report; World Health Organization: Geneva, Switzerland, 2015; Available online: http://www.who.int/iris/handle/10665/155002 (accessed on 20 May 2019).
- Amelung, V.; Viktoria, S.; Nicholas, G. Handbook of Integrated Care; Springer: Basel, Switzerland, 2017. [Google Scholar] [CrossRef]
- Maureen, R.M. Common challenges faced in EU-funded projects on integrated care for vulnerable persons. Int. J. Integr. Care 2017, 17, 17. [Google Scholar] [CrossRef] [PubMed]
- Gregory, M. Developing a patient care coordination center in Trafford, England: Lessons from the International Foundation for Integrated Care/Advancing Quality Alliance integrated care fellowship experience. Int. J. Integr. Care 2015. [Google Scholar] [CrossRef][Green Version]


{kind=link}
| Attribute | Description to Patients | Levels Level | |
|---|---|---|---|
| Attentiveness of care provider | …is how much time they spend helping you understand your health problems and treatment plans. | 1 | always given |
| 2 | often given | ||
| 3 | sometimes given | ||
| Attention to personal situation | …includes considering your work, social, and family situation in finding the most appropriate treatment for you. | 1 | always considered |
| 2 | sometimes considered | ||
| 3 | rarely or never considered | ||
| Multidisciplinary care | …within a single institution refers to doctors with different medical specialties working together on your treatment planning. | 1 | always work together |
| 2 | sometimes work together | ||
| 3 | rarely or never work together | ||
| Experience of care provider | …means the years of professional experience your care provider has. | 1 | >10 years of experience |
| 2 | 5–10 years of experience | ||
| 3 | 0–5 years of experience | ||
| Accurate health information | …refers to your ability to get accurate, reliable, and timely health and medical information. | 1 | very easy to get |
| 2 | somewhat easy to get | ||
| 3 | somewhat difficult to get | ||
| Friendliness and helpfulness of staff | …refers to the staff’s attitude toward you, including how often the staff is friendly and helpful when you have questions or problems. | 1 | always friendly and helpful |
| 2 | often friendly and helpful | ||
| 3 | sometimes friendly and helpful | ||
| Travel time to care provider | …refers to the amount of time you spend traveling to the facility of your care provider. (This does not include visits to the hospital emergency room.) | 1 | 10 min |
| 2 | 20 min | ||
| 3 | 30 min | ||
| Out of pocket costs | …are expenses that you spend for additional services, prescription medicines, and for medical care treatment or testing by a doctor or another care provider per visit. These costs are in addition to the cost of health insurance. | 1 | ¥10 per visit |
| 2 | ¥20 per visit | ||
| 3 | ¥30 per visit | ||
| Characteristics | No. | Percentage (%) |
|---|---|---|
| Age, mean (SD) | 62.94 (9.93) | |
| Gender | ||
| Male | 148 | 48.20 |
| Female | 159 | 51.80 |
| Marital status | ||
| Married | 258 | 84.04 |
| Other marital status | 49 | 15.96 |
| Education | ||
| ≥junior school | 163 | 53.10 |
| High middle school | 80 | 26.06 |
| ≥college | 64 | 20.84 |
| Employment | ||
| Employed | 69 | 22.47 |
| Unemployed † | 238 | 77.53 |
| Income (per year) | ||
| ≤¥20,000 | 78 | 25.41 |
| ¥20,000–50,000 | 128 | 41.70 |
| ¥50,000–100,000 | 74 | 24.10 |
| ≥¥100,000 | 27 | 8.79 |
| Health insurance (Shenzhen) | ||
| Enrolled | 175 | 57.14 |
| Not enrolled ‡ | 132 | 42.86 |
| Diabetes complications | 77 | 25.08 |
| Contract with GP (%) | 97 | 31.60 |
| Overall health status (%) | ||
| Very good, good, fair | 105 | 34.20 |
| Bad or very bad | 202 | 65.80 |
| Years with diabetes, mean (SD) | 8.54 (7.50) | |
| Frequency of visits, mean (SD) | 1.2 (0.99) | |
| Variable † | Regression Labeling | Coefficients ‡ | Willingness to Pay § | 95% Confidence Interval |
|---|---|---|---|---|
| Out-of-pocket cost | opcost | 0.24 * | ||
| Attentiveness of care provider—always given | acp-1 | 0.88 * | 21.89 * | 14.22–29.55 |
| Attentiveness of care provider—often given | acp-2 | 0.43 * | 10.73 * | 4.45–17.00 |
| Attention to personal situation—always considered | aps-1 | 0.93 * | 23.08 * | 15.75–30.41 |
| Attention to personal situation—sometimes considered | aps-2 | 0.56 * | 13.88 * | 7.47–20.29 |
| Multidisciplinary care—always work together | mc-1 | 0.0005 | 0.01 | −5.83–5.86 |
| Multidisciplinary care—sometimes work together | mc-2 | −0.43 | −10.68 | −16.94–4.42 |
| Experience of care provider—over 10 years | ecp-1 | 1.52 * | 37.72 * | 26.20–49.24 |
| Experience of care provider—5–10 years | ecp-2 | 0.87 * | 21.44 * | 13.45–29.43 |
| Accurate health information—always easy to get | ahi-1 | 0.064 | 1.57 | −3.91–7.06 |
| Accurate health information—somewhat easy to get | ahi-2 | −0.22 | −5.51 | −10.83–0.18 |
| Friendliness and helpfulness of staff—always | fh-1 | 0.61 * | 15.10 * | 8.45–21.76 |
| Friendliness and helpfulness of staff—often | fh-2 | 0.10 * | 2.57 * | −8.43–3.30 |
| Travel time to care providers—10 min | tt-1 | 1.62 * | 40.18 * | 29.45–50.90 |
| Travel time to care providers—20 min | tt-2 | 0.72 * | 17.75 * | 10.98–24.52 |
| constant | −0.53 | |||
| Number of observations | 5316 | |||
| Log likelihood | −1556.72 | |||
| LR Chi2 | 571.35 | |||
| Prob > Chi2 | 0.000 | |||
| Pseudo R2 | 0.155 | |||
| Change from Baseline | Change in Probability (%) | Standard Error | p Value |
|---|---|---|---|
| Out-of-pocket cost × 10 | 38.4 | 0.048 | <0.000 * |
| Out-of-pocket cost × 20 | 19.9 | 0.027 | <0.000 * |
| Attentiveness of care provider—always given | 86.9 | 0.157 | <0.000 * |
| Attentiveness of care provider—often given | 57.4 | 0.145 | <0.000 * |
| Attention to personal situation—always considered | 88.6 | 0.161 | <0.000 * |
| Attention to personal situation—sometimes considered | 68.5 | 0.159 | <0.000 * |
| Multidisciplinary care—always work together | 0.9 | 0.203 | 0.996 |
| Multidisciplinary care—sometimes work together | −88.9 | 0.340 | 0.010 |
| Experience of care provider—over 10 years | 91.7 | 0.154 | <0.000 * |
| Experience of care provider—5–10 years | 86.3 | 0.153 | <0.000 * |
| Accurate health information—always easy to get | 10.4 | 0.178 | 0.560 |
| Accurate health information—somewhat easy to get | −41.6 | 0.227 | 0.067 |
| Friendliness and helpfulness of staff—always | 72.25 | 0.159 | <0.000 * |
| Friendliness and helpfulness of staff—often | −18.4 | 0.227 | 0.419 |
| Travel time to care providers—10 min | 89.9 | 0.146 | <0.000 * |
| Travel time to care providers—20 min | 79.1 | 0.160 | <0.000 * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, X.; Song, K.; Zhu, P.; Valentijn, P.; Huang, Y.; Birch, S. How Do Type 2 Diabetes Patients Value Urban Integrated Primary Care in China? Results of a Discrete Choice Experiment. Int. J. Environ. Res. Public Health 2020, 17, 117. https://doi.org/10.3390/ijerph17010117
Wang X, Song K, Zhu P, Valentijn P, Huang Y, Birch S. How Do Type 2 Diabetes Patients Value Urban Integrated Primary Care in China? Results of a Discrete Choice Experiment. International Journal of Environmental Research and Public Health. 2020; 17(1):117. https://doi.org/10.3390/ijerph17010117
Chicago/Turabian StyleWang, Xin, Kuimeng Song, Paiyi Zhu, Pim Valentijn, Yixiang Huang, and Stephen Birch. 2020. "How Do Type 2 Diabetes Patients Value Urban Integrated Primary Care in China? Results of a Discrete Choice Experiment" International Journal of Environmental Research and Public Health 17, no. 1: 117. https://doi.org/10.3390/ijerph17010117
APA StyleWang, X., Song, K., Zhu, P., Valentijn, P., Huang, Y., & Birch, S. (2020). How Do Type 2 Diabetes Patients Value Urban Integrated Primary Care in China? Results of a Discrete Choice Experiment. International Journal of Environmental Research and Public Health, 17(1), 117. https://doi.org/10.3390/ijerph17010117