Implementation of 3D Printing Technology in the Field of Prosthetics: Past, Present, and Future

 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Contemporary Issues
2.1. Prosthetic Limb Abandonment
2.2. Appearance
2.3. Function and Control
3. A New Approach to Prosthetic Limb Design
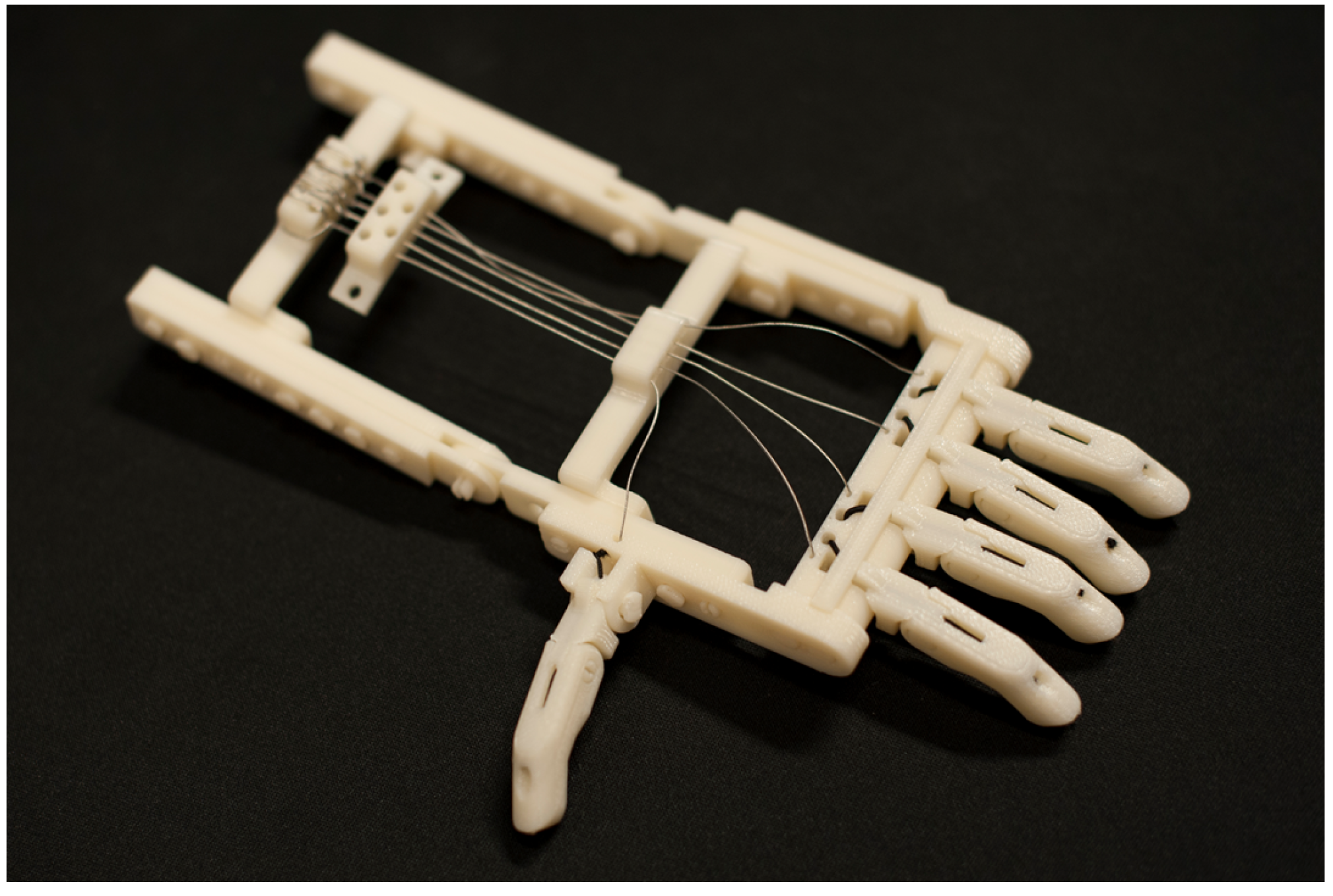
3.1. The Rise of 3D Printed Prosthetic Arms
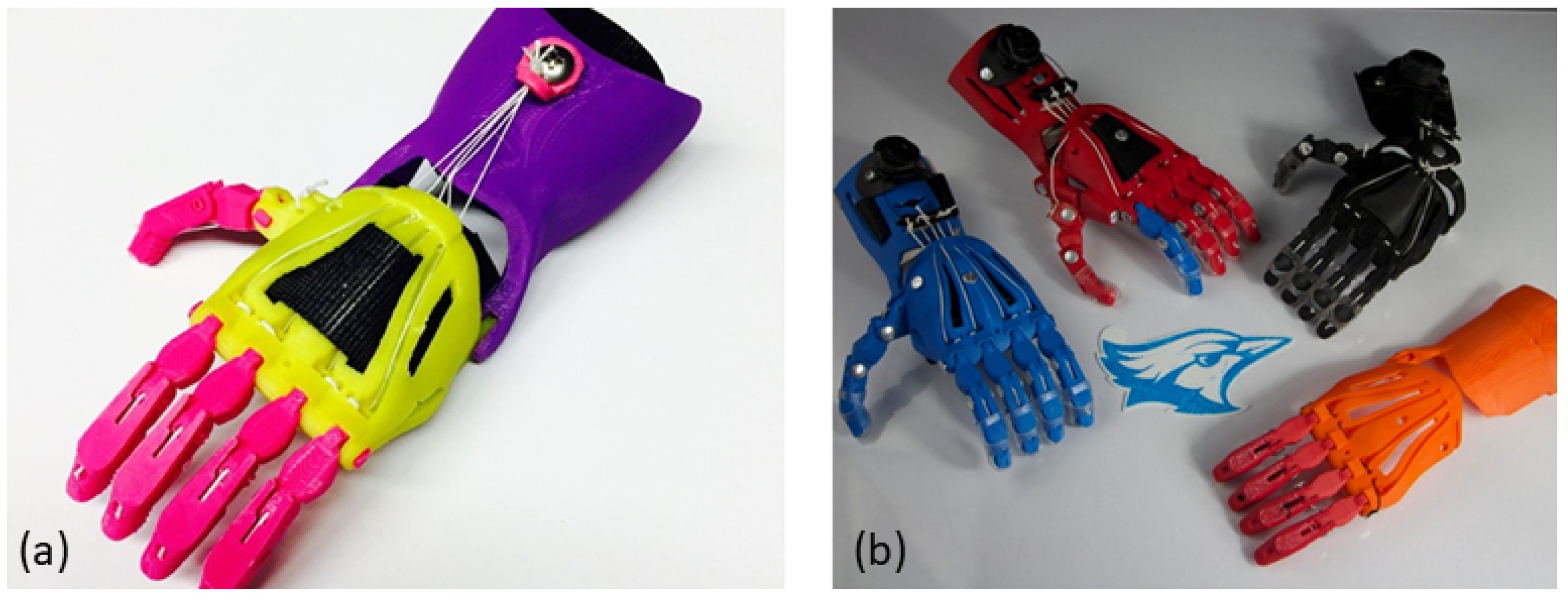
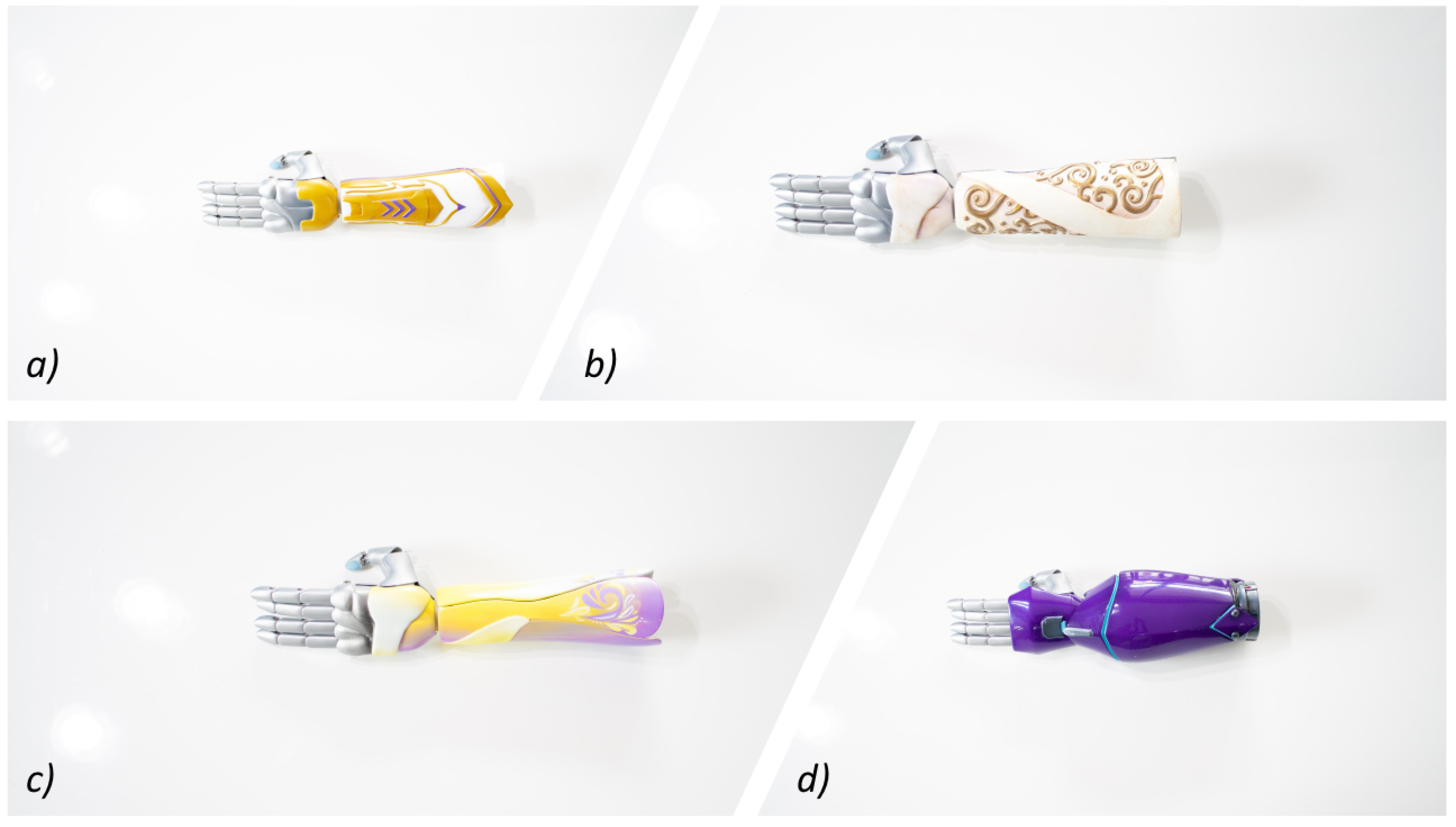
3.2. Appearance-Cooperative Expression
3.3. Function–Electromyography
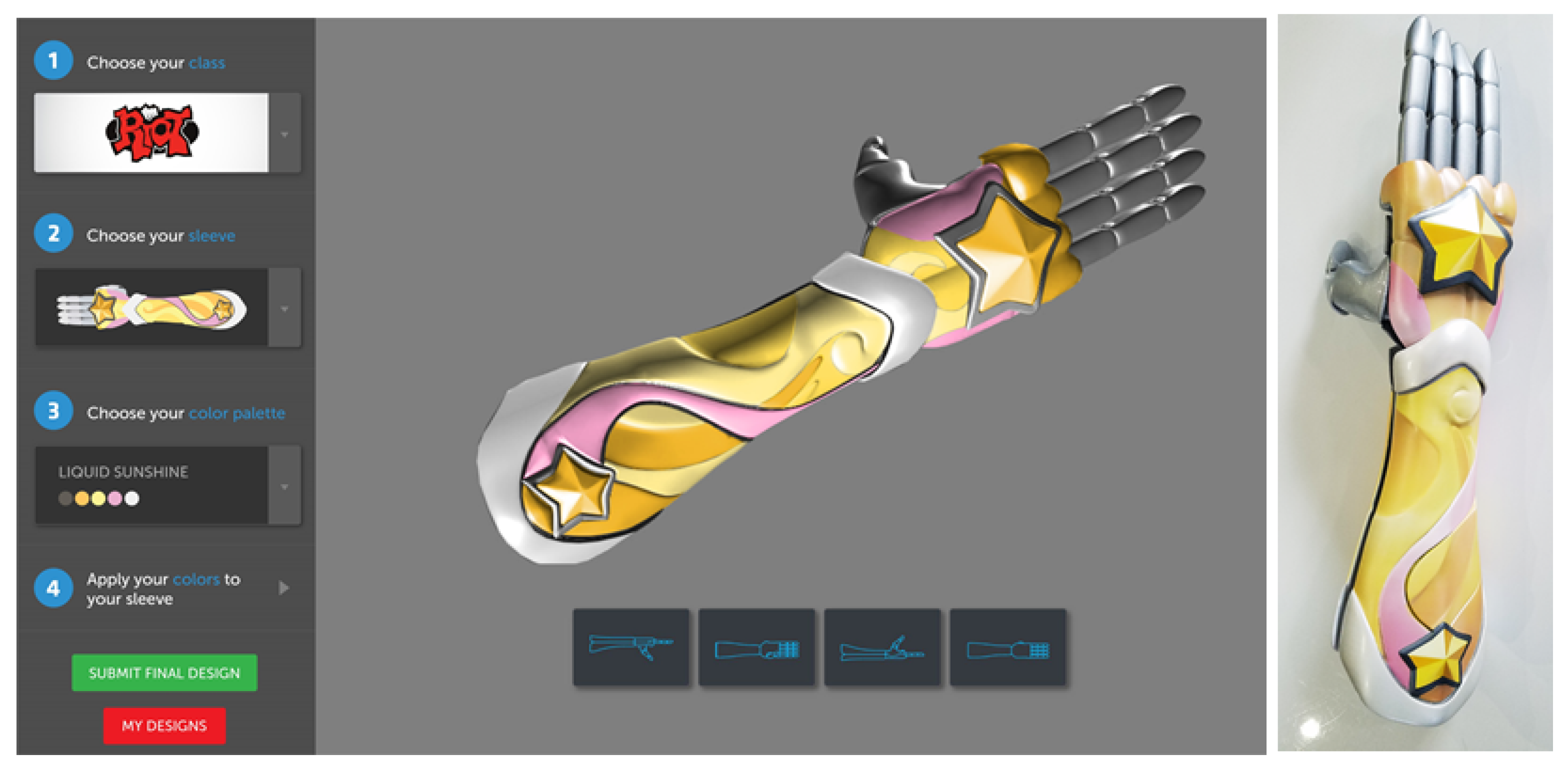
3.4. Control-Gamification and Training
3.5. Comfort and Durability
4. Discussion of Regulatory Framework
- ‘yes’
- ‘no’
- ‘I get help/avoid doing it’
- or ‘not applicable’.
- ‘one hand’
- ‘both hands’
- ‘with the involved hand supporting but not holding’
- ‘both hands, with the involved hand holding the object’.
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Thurston, A.J. Paré and prosthetics: the early history of artificial limbs. ANZ J. Surg. 2007, 77, 1114–1119. [Google Scholar] [CrossRef] [PubMed]
- Zuo, K.J.; Olson, J.L. The evolution of functional hand replacement: From iron prostheses to hand transplantation. Plast. Surg. 2014, 22, 44–51. [Google Scholar] [CrossRef]
- Norton, K. A brief history of prosthetics. InMotion 2007, 17, 11–13. [Google Scholar]
- Cordella, F.; Ciancio, A.L.; Sacchetti, R.; Davalli, A.; Cutti, A.G.; Guglielmelli, E.; Zollo, L. Literature review on needs of upper limb prosthesis users. Front. Neurosci. 2016, 10, 209. [Google Scholar] [CrossRef]
- Atkins, D.J.; Heard, D.C.; Donovan, W.H. Epidemiologic overview of individuals with upper-limb loss and their reported research priorities. JPO J. Prosthet. Orthot. 1996, 8, 2–11. [Google Scholar] [CrossRef]
- Ziegler-Graham, K.; MacKenzie, E.J.; Ephraim, P.L.; Travison, T.G.; Brookmeyer, R. Estimating the prevalence of limb loss in the United States: 2005 to 2050. Arch. Phys. Med. Rehabil. 2008, 89, 422–429. [Google Scholar] [CrossRef] [PubMed]
- Frontera, W.R.; Silver, J.K. Fondamenti di Medicina Fisica e Riabilitativa; Verduci: Rome, Italy, 2004. [Google Scholar]
- International Clearinghouse for Birth Defects Surveillance and Research Annual Report 2010; Technical Report; International Clearinghouse for Birth Defects Surveillance and Research: Rome, Italy, 2011.
- Stoll, C.; Alembik, Y.; Dott, B.; Roth, M.P. Associated malformations in patients with limb reduction deficiencies. Eur. J. Med. Genet. 2010, 53, 286–290. [Google Scholar] [CrossRef]
- Cignini, P.; Giorlandino, C.; Padula, F.; Dugo, N.; Cafà, E.V.; Spata, A. Epidemiology and risk factors of amniotic band syndrome, or ADAM sequence. J. Prenat. Med. 2012, 6, 59. [Google Scholar]
- Kim, K.; Wang, Y.; Kirby, R.S.; Druschel, C.M. Prevalence and trends of selected congenital malformations in New York State, 1983 to 2007. Birth Defects Res. Part A Clin. Mol. Teratol. 2013, 97, 619–627. [Google Scholar] [CrossRef] [PubMed]
- Parker, S.E.; Mai, C.T.; Canfield, M.A.; Rickard, R.; Wang, Y.; Meyer, R.E.; Anderson, P.; Mason, C.A.; Collins, J.S.; Kirby, R.S.; et al. Updated national birth prevalence estimates for selected birth defects in the United States, 2004–2006. Birth Defects Res. Part A Clin. Mol. Teratol. 2010, 88, 1008–1016. [Google Scholar] [CrossRef]
- Stoll, C. The northeastern France birth defects monitoring system. Prog. Clin. Biol. Res. 1985, 163, 157–162. [Google Scholar]
- Vasluian, E.; van der Sluis, C.K.; van Essen, A.J.; Bergman, J.E.; Dijkstra, P.U.; Reinders-Messelink, H.A.; de Walle, H.E. Birth prevalence for congenital limb defects in the northern Netherlands: A 30-year population-based study. BMC Musculoskelet. Disord. 2013, 14, 323. [Google Scholar] [CrossRef] [PubMed]
- Raichle, K.A.; Hanley, M.A.; Molton, I.; Kadel, N.J.; Campbell, K.; Phelps, E.; Ehde, D.; Smith, D.G. Prosthesis use in persons with lower-and upper-limb amputation. J. Rehabil. Res. Dev. 2008, 45, 961. [Google Scholar] [CrossRef]
- Wright, T.W.; Hagen, A.D.; Wood, M.B. Prosthetic usage in major upper extremity amputations. J. Hand Surg. 1995, 20, 619–622. [Google Scholar] [CrossRef]
- Herberts, P.; Körner, L.; Caine, K.; Wensby, L. Rehabilitation of unilateral below-elbow amputees with myoelectric prostheses. Scand. J. Rehabil. Med. 1980, 12, 123–128. [Google Scholar]
- Davidson, J. A survey of the satisfaction of upper limb amputees with their prostheses, their lifestyles, and their abilities. J. Hand Ther. 2002, 15, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Schoppen, T.; Boonstra, A.; Groothoff, J.W.; de Vries, J.; Göeken, L.N.; Eisma, W.H. Physical, Mental, and Social Predictors of Functional Outcome in Unilateral Lower-Limb Amputees1. Arch. Phys. Med. Rehabil. 2003, 84, 803–811. [Google Scholar] [CrossRef]
- Pezzin, L.E.; Dillingham, T.R.; MacKenzie, E.J.; Ephraim, P.; Rossbach, P. Use and satisfaction with prosthetic limb devices and related services 1. Arch. Phys. Med. Rehabil. 2004, 85, 723–729. [Google Scholar] [CrossRef]
- Buffart, L.M.; Roebroeck, M.E.; Van Heijningen, V.G.; Pesch-Batenburg, J.M.; Stam, H.J. Evaluation of arm and prosthetic functioning in children with a congenital transverse reduction deficiency of the upper limb. J. Rehabil. Med. 2007, 39, 379–386. [Google Scholar] [CrossRef]
- Tolsma, M.; Meeuwisse-de Vries, B.; Pesch-Batenburg, J.; Rol, M.; Arendzen, J.; Roebroeck, M.; et al. Level of functioning of adolescents and young adults with a congenital reduction deficiency of the upper limb. [Het niveau van functioneren van adolescenten en jongvolwassenen met een congenitaal reductiedefect van de arm]. Revalidata 2003, 25, 18–21. [Google Scholar]
- Kuyper, M.; Breedijk, M.; Mulders, A.; Post, M.; Prevo, A. Prosthetic management of children in The Netherlands with upper limb deficiencies. Prosthet. Orthot. Int. 2001, 25, 228–234. [Google Scholar] [CrossRef] [PubMed]
- Silcox, D.H.; Rooks, M.D.; Vogel, R.R.; Fleming, L.L. Myoelectric prostheses. A long-term follow-up and a study of the use of alternate prostheses. JBJS 1993, 75, 1781–1789. [Google Scholar] [CrossRef]
- Biddiss, E.; Chau, T. Upper-limb prosthetics: Critical factors in device abandonment. Am. J. Phys. Med. Rehabil. 2007, 86, 977–987. [Google Scholar] [CrossRef] [PubMed]
- Allin, S.; Eckel, E.; Markham, H.; Brewer, B.R. Recent trends in the development and evaluation of assistive robotic manipulation devices. Phys. Med. Rehabil. Clin. 2010, 21, 59–77. [Google Scholar] [CrossRef] [PubMed]
- Pullin, G. Design Meets Disability; MIT Press: Cambridge, MA, USA, 2009. [Google Scholar]
- Donovan-Hall, M.; Yardley, L.; Watts, R. Engagement in activities revealing the body and psychosocial adjustment in adults with a trans-tibial prosthesis. Prosthet. Orthot. Int. 2002, 26, 15–22. [Google Scholar] [CrossRef]
- Gallagher, P.; Maclachlan, M. Adjustment to an artificial limb: A qualitative perspective. J. Health Psychol. 2001, 6, 85–100. [Google Scholar] [CrossRef] [PubMed]
- Murray, C.D. The social meanings of prosthesis use. J. Health Psychol. 2005, 10, 425–441. [Google Scholar] [CrossRef]
- Murray, C.D. Being like everybody else: The personal meanings of being a prosthesis user. Disabil. Rehabil. 2009, 31, 573–581. [Google Scholar] [CrossRef]
- Biddiss, E.; Beaton, D.; Chau, T. Consumer design priorities for upper limb prosthetics. Disabil. Rehabil. Assist. Technol. 2007, 2, 346–357. [Google Scholar] [CrossRef]
- Biddiss, E.A.; Chau, T.T. Upper limb prosthesis use and abandonment: A survey of the last 25 years. Prosthet. Orthot. Int. 2007, 31, 236–257. [Google Scholar] [CrossRef]
- Crandall, R.C.; Tomhave, W. Pediatric unilateral below-elbow amputees: Retrospective analysis of 34 patients given multiple prosthetic options. J. Pediatr. Orthop. 2002, 22, 380–383. [Google Scholar] [CrossRef]
- Goffman, E. Stigma: Notes on the Management of Spoiled Identity; Simon and Schuster: New York, NY, USA, 2009. [Google Scholar]
- Frank, G. Beyond stigma: Visibility and self-empowerment of persons with congenital limb deficiencies. J. Soc. Issues 1988, 44, 95–115. [Google Scholar] [CrossRef]
- Huang, J.N.; Park, I.; Ellingson, E.; Littlepage, L.E.; Pellman, D. Activity of the APCCdh1 form of the anaphase-promoting complex persists until S phase and prevents the premature expression of Cdc20p. J. Cell Biol. 2001, 154, 85–94. [Google Scholar] [CrossRef]
- Mason, C.Y.; Thormann, M.S.; Steedly, K.M. How Students with Disabilities Learn in and Through the Arts: An Investigation of Educator Perceptions; VSA Arts: Washington, DC, USA, 2004. [Google Scholar]
- Clements, I.P. How Prosthetic Limbs Work; How Stuff Works. Available online: https://science.howstuffworks.com/prosthetic-limb.htm (accessed on 27 February 2019).
- Ariyanto, M.; Munadi; Haryadi, G.D.; Ismail, R.; Pakpahan, J.A.; Mustaqim, K.A. A low cost anthropomorphic prosthetic hand using DC micro metal gear motor. In Proceedings of the 2016 3rd International Conference on Information Technology, Computer, and Electrical Engineering (ICITACEE), Semarang, Indonesia, 19–20 October 2016; pp. 42–46. [Google Scholar]
- Weir, A.S. Push Button Means for Operating Power-Driven Artificial Hands. U.S. Patent 2,679,649, 1 June 1954. [Google Scholar]
- Carey, S.L.; Lura, D.J.; Highsmith, M.J. Differences in myoelectric and body-powered upper-limb prostheses: Systematic literature review. J. Rehabil. Res. Dev. 2015, 52, 247–263. [Google Scholar] [CrossRef]
- Nelson, V.S.; Flood, K.M.; Bryant, P.R.; Huang, M.E.; Pasquina, P.F.; Roberts, T.L. Limb deficiency and prosthetic management. 1. Decision making in prosthetic prescription and management. Arch. Phys. Med. Rehabil. 2006, 87, 3–9. [Google Scholar] [CrossRef]
- Antfolk, C.; D’Alonzo, M.; Rosen, B.; Lundborg, G.; Sebelius, F.; Cipriani, C. Sensory feedback in upper limb prosthetics. Expert Rev. Med. Devices 2013, 10, 45–54. [Google Scholar] [CrossRef]
- Weiss, L.D.; Weiss, J.M.; Silver, J.K. Easy EMG: A Guide to Performing Nerve Conduction Studies and Electromyography; Elsevier Health Sciences: Amsterdam, The Netherlands, 2015. [Google Scholar]
- Nishikawa, D.; Yu, W.; Maruishi, M.; Watanabe, I.; Yokoi, H.; Mano, Y.; Kakazu, Y. On-line learning based electromyogram to forearm motion classifier with motor skill evaluation. JSME Int. J. Ser. C Mech. Syst. Mach. Elem. Manuf. 2000, 43, 906–915. [Google Scholar] [CrossRef]
- Hernandez Arieta, A.; Katoh, R.; Yokoi, H.; Wenwei, Y. Development of a multi-DOF electromyography prosthetic system using the adaptive joint mechanism. Appl. Bionics Biomech. 2006, 3, 101–111. [Google Scholar] [CrossRef][Green Version]
- Henn, S.; Carpien, C. 3-D Printer Brings Dexterity to Children with No Fingers; National Public Radio. Available online: https://www.npr.org/sections/health-shots/2013/06/18/191279201/3-d-printer-brings-dexterity-to-children-with-no-fingers (accessed on 1 March 2019).
- Ten Kate, J.; Smit, G.; Breedveld, P. 3D-printed upper limb prostheses: A review. Disabil. Rehabil. Assist. Technol. 2017, 12, 300–314. [Google Scholar] [CrossRef]
- Krassenstein, E. 229 Newly Designed Prosthetic Hands are 3D Printed by Volunteers for Landmark Event This Sunday; Create Education. Available online: https://www.createeducation.com/blog/229-newly-designed-prosthetic-hands-are-3d-printed-by-volunteers-for-landmark-event/ (accessed on 1 March 2019).
- Dally, C.; Johnson, D.; Canon, M.; Ritter, S.; Mehta, K. Characteristics of a 3D-printed prosthetic hand for use in developing countries. In Proceedings of the 2015 IEEE Global Humanitarian Technology Conference (GHTC), Seattle, WA, USA, 9–12 October 2015; pp. 66–70. [Google Scholar]
- Elmansy, R. Designing the 3D-Printed prosthetic hand. Des. Manag. Rev. 2015, 26, 24–31. [Google Scholar]
- Zuniga, J.; Katsavelis, D.; Peck, J.; Stollberg, J.; Petrykowski, M.; Carson, A.; Fernandez, C. Cyborg beast: A low-cost 3d-printed prosthetic hand for children with upper-limb differences. BMC Res. Notes 2015, 8, 10. [Google Scholar] [CrossRef]
- Zuniga, J.M.; Peck, J.; Srivastava, R.; Katsavelis, D.; Carson, A. An open source 3D-printed transitional hand prosthesis for children. JPO J. Prosthet. Orthot. 2016, 28, 103–108. [Google Scholar] [CrossRef]
- Zuniga, J.M.; Carson, A.M.; Peck, J.M.; Kalina, T.; Srivastava, R.M.; Peck, K. The development of a low-cost three-dimensional printed shoulder, arm, and hand prostheses for children. Prosthet. Orthot. Int. 2017, 41, 205–209. [Google Scholar] [CrossRef]
- Schull, J. Enabling the future: Crowdsourced 3D-printed prostheticsas a model for open source assistive TechnologyInnovation and mutual aid. In Proceedings of the 17th International ACM SIGACCESS Conference on Computers & Accessibility, Baltimore, MD, USA, 9–12 October 2015; p. 1. [Google Scholar]
- Jacobs, S.; Schull, J.; White, P.; Lehrer, R.; Vishwakarma, A.; Bertucci, A. e-nabling education: Curricula and models for teaching students to print hands. In Proceedings of the 2016 IEEE Frontiers in Education Conference (FIE), Eire, PA, USA, 12–15 October 2016; pp. 1–4. [Google Scholar]
- Kensing, F.; Blomberg, J. Participatory design: Issues and concerns. Comput. Support. Coop. Work (CSCW) 1998, 7, 167–185. [Google Scholar] [CrossRef]
- Druin, A. The role of children in the design of new technology. Behav. Inform. Technol. 2002, 21, 1–25. [Google Scholar]
- Druin, A. Cooperative inquiry: Developing new technologies for children with children. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, Pittsburgh, PA, USA, 15–20 May 1999; pp. 592–599. [Google Scholar]
- Yip, J.C.; Foss, E.; Bonsignore, E.; Guha, M.L.; Norooz, L.; Rhodes, E.; McNally, B.; Papadatos, P.; Golub, E.; Druin, A. Children initiating and leading cooperative inquiry sessions. In Proceedings of the 12th International Conference on Interaction Design and Children, New York, NY, USA, 24–27 June 2013; pp. 293–296. [Google Scholar]
- Foss, E.; Guha, M.L.; Papadatos, P.; Clegg, T.; Yip, J.; Walsh, G. Cooperative Inquiry extended: Creating technology with middle school students with learning differences. J. Spec. Educ. Technol. 2013, 28, 33–46. [Google Scholar] [CrossRef]
- Foss, E.; Guha, M.L.; Papadatos, P.; Clegg, T.; Yip, J.; Walsh, G. Cooperative Inquiry Design Techniques in a Classroom of Children with Special Learning Needs; University of Maryland: College Park, MD, USA, 2013. [Google Scholar]
- Ottobock 510(k) Premarket Notification. Available online: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfPMN/pmn.cfm?ID=K123795 (accessed on 1 March 2019).
- Smith, P.A.; Dombrowski, M.; Buyssens, R.; Barclay, P. The Impact of a Custom Electromyograph (EMG) Controller on Player Enjoyment of Games Designed to Teach the Use of Prosthetic Arms. Comput. Games J. 2018, 7, 131–147. [Google Scholar] [CrossRef]
- Manero, A.; Smith, P.A.; Sparkman, J.; Dombrowksi, M.; Courbin, D.; Barclay, P.; Chi, A. Design of neuroprosthetics and virtual training: Utilizing additive manufacturing and gamified simulation to improve pediatric outcomes. In Proceedings of the MRS Proceedings, Phoenix, AZ, USA, 22–26 April 2019. [Google Scholar]
- Diment, L.E.; Thompson, M.S.; Bergmann, J.H. Clinical efficacy and effectiveness of 3D printing: A systematic review. BMJ Open 2017, 7, e016891. [Google Scholar] [CrossRef]
- Campbell, L.; Lau, A.; Pousett, B.; Janzen, E.; Raschke, S.U. HOW INFILL PERCENTAGE AFFECTS THE ULTIMATE STRENGTH OF A 3D-PRINTED TRANSTIBIAL SOCKET. Can. Prosthet. Orthot. J. 2018, 1. [Google Scholar] [CrossRef]
- Song, Y.; Li, Y.; Song, W.; Yee, K.; Lee, K.Y.; Tagarielli, V. Measurements of the mechanical response of unidirectional 3D-printed PLA. Mater. Des. 2017, 123, 154–164. [Google Scholar] [CrossRef]
- Dizon, J.R.C.; Espera, A.H., Jr.; Chen, Q.; Advincula, R.C. Mechanical characterization of 3D-printed polymers. Addit. Manuf. 2018, 20, 44–67. [Google Scholar] [CrossRef]
- Ahn, S.H.; Montero, M.; Odell, D.; Roundy, S.; Wright, P.K. Anisotropic material properties of fused deposition modeling ABS. Rapid Prototyp. J. 2002, 8, 248–257. [Google Scholar] [CrossRef]
- Petrick, I.J.; Simpson, T.W. 3D printing disrupts manufacturing: How economies of one create new rules of competition. Res. Technol. Manag. 2013, 56, 12–16. [Google Scholar] [CrossRef]
- Diment, L.E.; Thompson, M.S.; Bergmann, J.H. Three-dimensional printed upper-limb prostheses lack randomised controlled trials: A systematic review. Prosthet. Orthot. Int. 2018, 42, 7–13. [Google Scholar] [CrossRef]
- Lunsford, C.; Grindle, G.; Salatin, B.; Dicianno, B.E. Innovations with 3-dimensional printing in physical medicine and rehabilitation: A review of the literature. PM&R 2016, 8, 1201–1212. [Google Scholar]
- Sköld, A.; Hermansson, L.N.; Krumlinde-Sundholm, L.; Eliasson, A.C. Development and evidence of validity for the Children’s Hand-use Experience Questionnaire (CHEQ). Dev. Med. Child Neurol. 2011, 53, 436–442. [Google Scholar] [CrossRef]
- Lindner, H.Y.; Eliasson, A.C.; Hermansson, L.M. Influence of standardized activities on validity of Assessment of Capacity for Myoelectric Control. J. Rehabil. Res. Dev. 2013, 50, 1391–1402. [Google Scholar] [CrossRef]
- Lindner, H.Y.; Linacre, J.M.; Norling Hermansson, L.M. Assessment of capacity for myoelectric control: Evaluation of construct and rating scale. J. Rehabil. Med. 2009, 41, 467–474. [Google Scholar] [CrossRef]






© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manero, A.; Smith, P.; Sparkman, J.; Dombrowski, M.; Courbin, D.; Kester, A.; Womack, I.; Chi, A. Implementation of 3D Printing Technology in the Field of Prosthetics: Past, Present, and Future. Int. J. Environ. Res. Public Health 2019, 16, 1641. https://doi.org/10.3390/ijerph16091641
Manero A, Smith P, Sparkman J, Dombrowski M, Courbin D, Kester A, Womack I, Chi A. Implementation of 3D Printing Technology in the Field of Prosthetics: Past, Present, and Future. International Journal of Environmental Research and Public Health. 2019; 16(9):1641. https://doi.org/10.3390/ijerph16091641
Chicago/Turabian StyleManero, Albert, Peter Smith, John Sparkman, Matt Dombrowski, Dominique Courbin, Anna Kester, Isaac Womack, and Albert Chi. 2019. "Implementation of 3D Printing Technology in the Field of Prosthetics: Past, Present, and Future" International Journal of Environmental Research and Public Health 16, no. 9: 1641. https://doi.org/10.3390/ijerph16091641
APA StyleManero, A., Smith, P., Sparkman, J., Dombrowski, M., Courbin, D., Kester, A., Womack, I., & Chi, A. (2019). Implementation of 3D Printing Technology in the Field of Prosthetics: Past, Present, and Future. International Journal of Environmental Research and Public Health, 16(9), 1641. https://doi.org/10.3390/ijerph16091641