Injury Prevention in Amateur Soccer: A Nation-Wide Study on Implementation and Associations with Injury Incidence


Abstract
1. Introduction
2. Methods
2.1. Prevention Programmes
2.2. Study Design
2.3. Questionnaire
2.4. Statistical Analysis
3. Results
3.1. Injury Prevention in Swiss Amateur Soccer
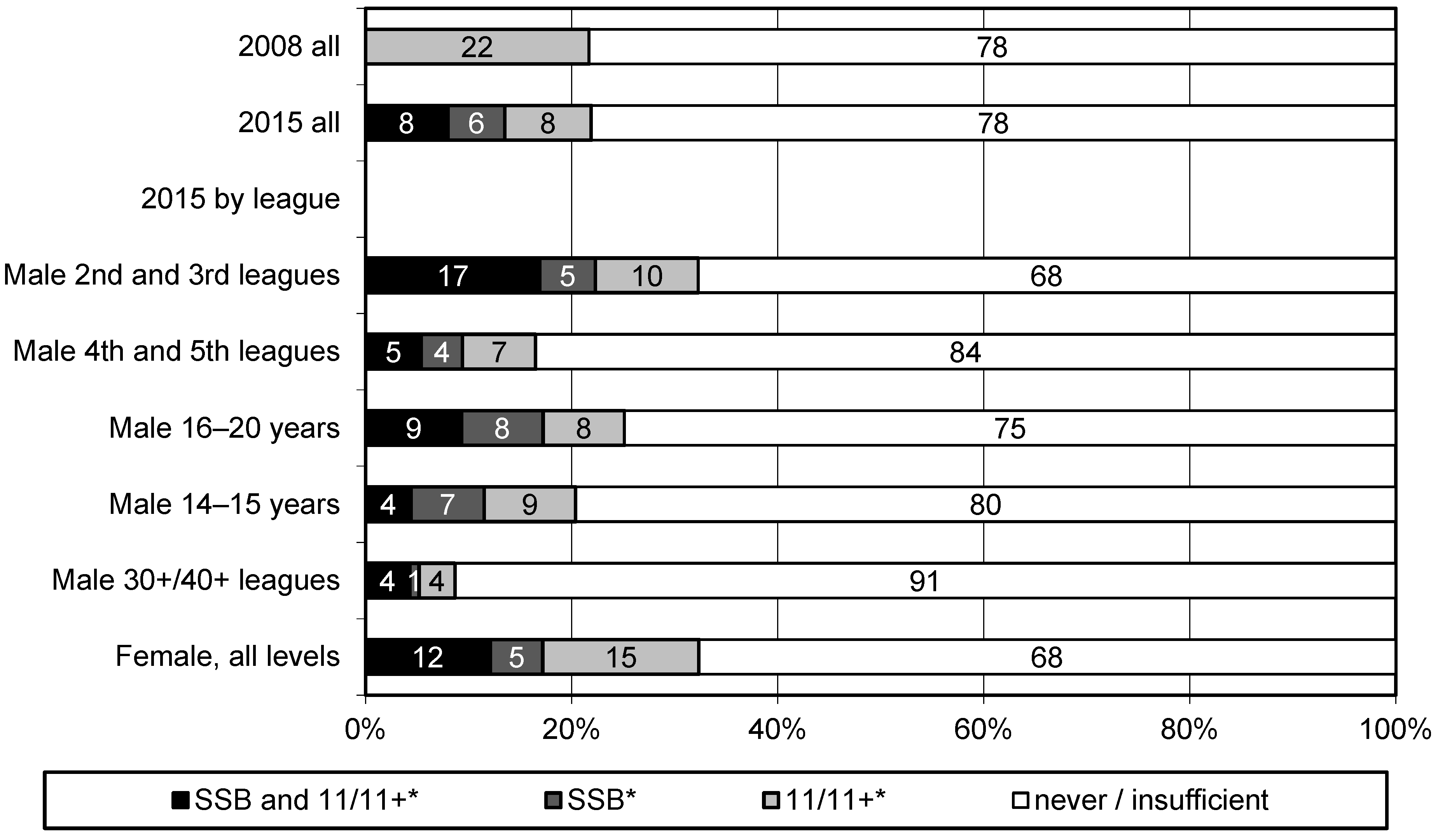
3.2. Implementation of Prevention Programmes
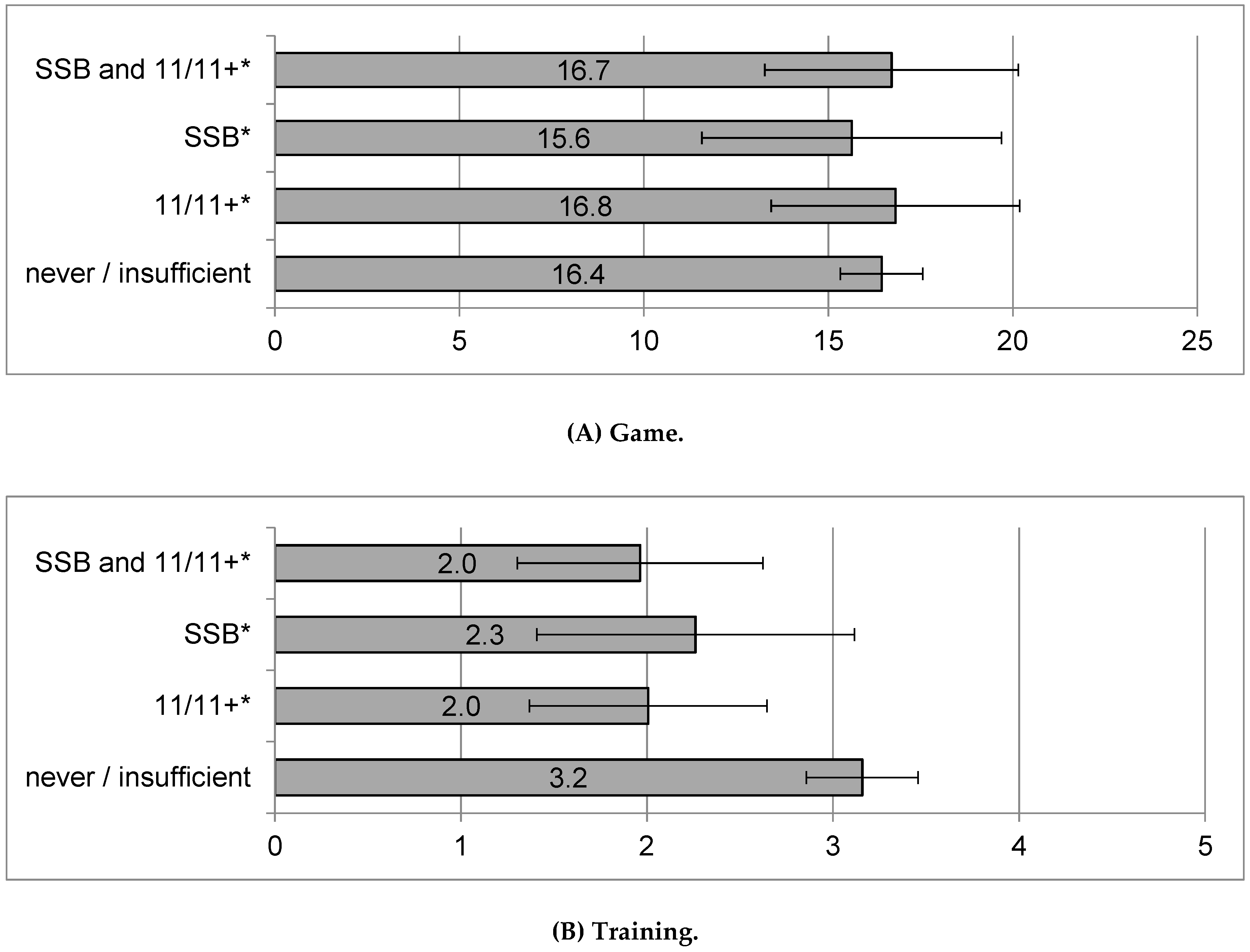
3.3. Association between Injury Incidence and the Implementation of a Prevention Programme
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lamprecht, M.; Fischer, A.; Stamm, H. Sport Schweiz 2014: Sportaktivität und Sportinteresse der Schweizer Bevölkerung; Bundesamt für Sport (BASPO): Magglingen, Switzerland, 2014. [Google Scholar]
- Bangsbo, J.; Hansen, P.R.; Dvorak, J.; Krustrup, P. Recreational football for disease prevention and treatment in untrained men: A narrative review examining cardiovascular health, lipid profile, body composition, muscle strength and functional capacity. Br. J. Sports Med. 2015, 49, 568–576. [Google Scholar] [CrossRef] [PubMed]
- Oja, P.; Titze, S.; Kokko, S.; Kujala, U.M.; Heinonen, A.; Kelly, P.; Koski, P.; Foster, C. Health benefits of different sport disciplines for adults: Systematic review of observational and intervention studies with meta-analysis. Br. J. Sports Med. 2015, 49, 434–440. [Google Scholar] [CrossRef]
- Polinder, S.; Haagsma, J.; Panneman, M.; Scholten, A.; Brugmans, M.; Van Beeck, E. The economic burden of injury: Health care and productivity costs of injuries in the Netherlands. Accid. Anal. Prev. 2016, 93, 92–100. [Google Scholar] [CrossRef]
- Sammelstelle für die Statistik der Unfallversicherung UVG [Swiss Accident Insurance Database]. Unfallstatistik UVG. Available online: https://www.unfallstatistik.ch/d/publik/publikationen_d.htm (accessed on 19 April 2018).
- Hagglund, M.; Walden, M.; Ekstrand, J. Injury recurrence is lower at the highest professional football level than at national and amateur levels: Does sports medicine and sports physiotherapy deliver? Br. J. Sports Med. 2016, 50, 751–758. [Google Scholar] [CrossRef] [PubMed]
- Hammes, D.; Aus Der Funten, K.; Kaiser, S.; Frisen, E.; Dvorak, J.; Meyer, T. Injuries of veteran football (soccer) players in Germany. Res. Sports Med. 2015, 23, 215–226. [Google Scholar] [CrossRef] [PubMed]
- Van Beijsterveldt, A.M.; Steffen, K.; Stubbe, J.H.; Frederiks, J.E.; van de Port, I.G.; Backx, F.J. Soccer injuries and recovery in Dutch male amateur soccer players: Results of a prospective cohort study. Clin. J. Sport Med. 2014, 24, 337–342. [Google Scholar] [CrossRef]
- Junge, A.; Lamprecht, M.; Stamm, H.; Hasler, H.; Bizzini, M.; Tschopp, M.; Reuter, H.; Wyss, H.; Chilvers, C.; Dvorak, J. Countrywide campaign to prevent soccer injuries in Swiss amateur players. Am. J. Sports Med. 2011, 39, 57–63. [Google Scholar] [CrossRef]
- SFV. Wettspielreglement (WR) Ausgabe Juli 2018. Available online: http://org.football.ch/portaldata/28/Resources/dokumente/de/02_wettspielreglement_und_spielregeln/2.1_Wettspielreglement_(Juli_2018).pdf (accessed on 12 September 2018).
- Al Attar, W.S.; Soomro, N.; Pappas, E.; Sinclair, P.J.; Sanders, R.H. How Effective are F-MARC Injury Prevention Programs for Soccer Players? A Systematic Review and Meta-Analysis. Sports Med. 2016, 46, 205–217. [Google Scholar] [CrossRef] [PubMed]
- Barengo, N.C.; Meneses-Echavez, J.F.; Ramirez-Velez, R.; Cohen, D.D.; Tovar, G.; Bautista, J.E. The impact of the FIFA 11+ training program on injury prevention in football players: A systematic review. Int. J. Environ. Res. Public Health 2014, 11, 11986–12000. [Google Scholar] [CrossRef]
- Faude, O.; Rommers, N.; Rössler, R. Exercise-based injury prevention in football. Ger. J. Exerc. Sport Res. 2018, 48, 157–168. [Google Scholar] [CrossRef]
- Thorborg, K.; Krommes, K.K.; Esteve, E.; Clausen, M.B.; Bartels, E.M.; Rathleff, M.S. Effect of specific exercise-based football injury prevention programmes on the overall injury rate in football: A systematic review and meta-analysis of the FIFA 11 and 11+ programmes. Br. J. Sports Med. 2017, 51, 562–571. [Google Scholar] [CrossRef]
- Emery, C.A.; Meeuwisse, W.H. The effectiveness of a neuromuscular prevention strategy to reduce injuries in youth soccer: A cluster-randomised controlled trial. Br. J. Sports Med. 2010, 44, 555–562. [Google Scholar] [CrossRef]
- Rossler, R.; Donath, L.; Verhagen, E.; Junge, A.; Schweizer, T.; Faude, O. Exercise-based injury prevention in child and adolescent sport: A systematic review and meta-analysis. Sports Med. 2014, 44, 1733–1748. [Google Scholar] [CrossRef]
- Steffen, K.; Emery, C.A.; Romiti, M.; Kang, J.; Bizzini, M.; Dvorak, J.; Finch, C.F.; Meeuwisse, W.H. High adherence to a neuromuscular injury prevention programme (FIFA 11+) improves functional balance and reduces injury risk in Canadian youth female football players: A cluster randomised trial. Br. J. Sports Med. 2013, 47, 794–802. [Google Scholar] [CrossRef]
- Steffen, K.; Myklebust, G.; Olsen, O.E.; Holme, I.; Bahr, R. Preventing injuries in female youth football—A cluster-randomized controlled trial. Scand. J. Med. Sci. Sports 2008, 18, 605–614. [Google Scholar] [CrossRef]
- Hammes, D.; Aus der Funten, K.; Kaiser, S.; Frisen, E.; Bizzini, M.; Meyer, T. Injury prevention in male veteran football players—A randomised controlled trial using “FIFA 11+”. J. Sports Sci. 2015, 33, 873–881. [Google Scholar] [CrossRef]
- Soligard, T.; Nilstad, A.; Steffen, K.; Myklebust, G.; Holme, I.; Dvorak, J.; Bahr, R.; Andersen, T.E. Compliance with a comprehensive warm-up programme to prevent injuries in youth football. Br. J. Sports Med. 2010, 44, 787–793. [Google Scholar] [CrossRef]
- Van Tiggelen, D.; Wickes, S.; Stevens, V.; Roosen, P.; Witvrouw, E. Effective prevention of sports injuries: A model integrating efficacy, efficiency, compliance and risk-taking behaviour. Br. J. Sports Med. 2008, 42, 648–652. [Google Scholar] [CrossRef]
- Bizzini, M.; Junge, A.; Dvorak, J. Implementation of the FIFA 11+ football warm up program: How to approach and convince the Football associations to invest in prevention. Br. J. Sports Med. 2013, 47, 803–806. [Google Scholar] [CrossRef]
- Gianotti, S.; Hume, P.A.; Tunstall, H. Efficacy of injury prevention related coach education within netball and soccer. J. Sci. Med. Sport 2010, 13, 32–35. [Google Scholar] [CrossRef]
- Klugl, M.; Shrier, I.; McBain, K.; Shultz, R.; Meeuwisse, W.H.; Garza, D.; Matheson, G.O. The Prevention of Sport Injury: An Analysis of 12,000 Published Manuscripts. Clin. J. Sport Med. 2010, 20, 407–412. [Google Scholar] [CrossRef]
- Donaldson, A.; Lloyd, D.G.; Gabbe, B.J.; Cook, J.; Finch, C.F. We have the programme, what next? Planning the implementation of an injury prevention programme. Inj. Prev. 2017, 23, 273–280. [Google Scholar] [CrossRef]
- Dvorak, J.; Junge, A. “The 11”. The Prevention Programme; FIFA Medical Assessment and research centre (F-MARC): Zurich, Switzerland, 2014. [Google Scholar]
- Bizzini, M.; Junge, A.; Dvorak, J. THE “11+”. A Complete Warm-Up Programme to Prevent Injuries. Manual; FIFA Medical Assessment and Research Centre (F-MARC): Zurich, Switzerland, 2017. [Google Scholar]
- Suva. Sport Basics: Neues Präventionsprogramm für Ballsport. Available online: https://www.suva.ch/material/dokumentationen/trainingsprogramm-sport-basics-88255.d-35770-35770 (accessed on 17 June 2018).
- Fuller, C.W.; Ekstrand, J.; Junge, A.; Andersen, T.E.; Bahr, R.; Dvorak, J.; Hagglund, M.; McCrory, P.; Meeuwisse, W.H. Consensus statement on injury definitions and data collection procedures in studies of football (soccer) injuries. Br. J. Sports Med. 2006, 40, 193–201. [Google Scholar] [CrossRef]
- Knowles, S.B.; Marshall, S.W.; Guskiewicz, K.M. Issues in estimating risks and rates in sports injury research. J. Athl. Train. 2006, 41, 207–215. [Google Scholar]
- Field, A. Discovering Statistics Using IBM SPSS Statistics, 4th ed.; SAGE Publications Ltd.: London, UK, 2013. [Google Scholar]
- Gebert, A.; Gerber, M.; Puhse, U.; Faude, O.; Stamm, H.; Lamprecht, M. Changes in injury incidences and causes in Swiss amateur soccer between the years 2004 and 2015. Swiss Med. Wkly. 2018, 148, w14690. [Google Scholar] [CrossRef]
- Bogardus, R.; Martin, R.; Richman, A.; Kulas, A. Applying the Socio-Ecological Model to barriers to implementation of ACL injury prevention programs: A systematic review. Sport Health Sci. 2017. [Google Scholar] [CrossRef]
- McCall, A.; Dupont, G.; Ekstrand, J. Injury prevention strategies, coach compliance and player adherence of 33 of the UEFA Elite Club Injury Study teams: A survey of teams’ head medical officers. Br. J. Sports Med. 2016, 50, 725–730. [Google Scholar] [CrossRef]
- Sewry, N.; Verhagen, E.; Lambert, M.; van Mechelen, W.; Viljoen, W.; Readhead, C.; Brown, J. Exercise-Based Interventions for Injury Prevention in Tackle Collision Ball Sports: A Systematic Review. Sports Med. 2017, 47, 1847–1857. [Google Scholar] [CrossRef]
- Dvorak, J.; Junge, A. Football injuries and physical symptoms. A review of the literature. Am. J. Sports Med. 2000, 28, S3–S9. [Google Scholar] [CrossRef]
- McNoe, B.M.; Chalmers, D.J. Injury prevention behaviour in community-level soccer players. J. Sci. Med. Sport 2011, 14, 482–488. [Google Scholar] [CrossRef]
- Zech, A.; Wellmann, K. Perceptions of football players regarding injury risk factors and prevention strategies. PLoS ONE 2017, 12, e0176829. [Google Scholar] [CrossRef]
- Van Beijsterveldt, A.M.; van de Port, I.G.; Krist, M.R.; Schmikli, S.L.; Stubbe, J.H.; Frederiks, J.E.; Backx, F.J. Effectiveness of an injury prevention programme for adult male amateur soccer players: A cluster-randomised controlled trial. Br. J. Sports Med. 2012, 46, 1114–1118. [Google Scholar] [CrossRef]
- Ekegren, C.L.; Gabbe, B.J.; Finch, C.F. Injury surveillance in community sport: Can we obtain valid data from sports trainers? Scand. J. Med. Sci. Sports 2015, 25, 315–322. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Preventive Measures | 2004 % (95% CI) | 2008 % (95% CI) | 2015 % (95% CI) |
|---|---|---|---|
| Suva Sport Basics | – | – | 5.7 (4.2–7.3) |
| The 11/11+ | – | 25.6 (22.2–29.0) | 6.5 (4.9–8.2) |
| Warm–up | 80.7 (78.0–83.3) | 72.4 (68.9–75.8) | 67.4 (64.2–70.5) |
| Stretching | 74.9 (72.0–77.8) | 48.0 (44.1–51.9) | 47.8 (44.4–51.1) |
| Cool down | 35.1 (31.9–38.3) | 12.0 (9.5–14.5) | 12.9 (10.7–15.2) |
| Wearing shin guards | 21.6 (18.9–24.4) | 13.4 (10.8–16.1) | 9.8 (7.8–11.8) |
| General strength training | 16.2 (13.7–18.7) | 13.3 (10.6–15.9) | 24.2 (21.4–27.1) |
| Massage | 11.5 (9.3–13.6) | 6.2 (4.3–8.0) | 4.4 (3.1–5.8) |
| Information | 11.0 (8.9–13.1) | 3.3 (1.9–4.7) | 3.4 (2.2–4.6) |
| Core strength training | 10.0 (8.0–11.9) | 7.4 (5.4–9.5) | 20.9 (18.1–23.6) |
| Cardiorespiratory fitness training | 10.0 (8.0–11.9) | 4.4 (2.8–6.0) | 10.1 (8.1–12.2) |
| Rehabilitation and complete recovery | 5.3 (3.8–6.8) | 1.7 (0.7–2.8) | 3.3 (2.1–4.5) |
| Fair play | 4.5 (3.1–5.9) | 2.1 (0.9–3.2) | 3.6 (2.4–4.9) |
| Adjusting footwear | 4.2 (2.8–5.5) | 1.3 (0.4–2.1) | 1.9 (1.0–2.8) |
| Other measures | 14.1 (11.8–16.4) | 11.2 (8.8–13.7) | 18.1 (15.5–20.6) |
| Number of coaches | 864 | 633 | 858 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gebert, A.; Gerber, M.; Pühse, U.; Stamm, H.; Lamprecht, M. Injury Prevention in Amateur Soccer: A Nation-Wide Study on Implementation and Associations with Injury Incidence. Int. J. Environ. Res. Public Health 2019, 16, 1593. https://doi.org/10.3390/ijerph16091593
Gebert A, Gerber M, Pühse U, Stamm H, Lamprecht M. Injury Prevention in Amateur Soccer: A Nation-Wide Study on Implementation and Associations with Injury Incidence. International Journal of Environmental Research and Public Health. 2019; 16(9):1593. https://doi.org/10.3390/ijerph16091593
Chicago/Turabian StyleGebert, Angela, Markus Gerber, Uwe Pühse, Hanspeter Stamm, and Markus Lamprecht. 2019. "Injury Prevention in Amateur Soccer: A Nation-Wide Study on Implementation and Associations with Injury Incidence" International Journal of Environmental Research and Public Health 16, no. 9: 1593. https://doi.org/10.3390/ijerph16091593
APA StyleGebert, A., Gerber, M., Pühse, U., Stamm, H., & Lamprecht, M. (2019). Injury Prevention in Amateur Soccer: A Nation-Wide Study on Implementation and Associations with Injury Incidence. International Journal of Environmental Research and Public Health, 16(9), 1593. https://doi.org/10.3390/ijerph16091593