Factors Leading Municipal Authorities to Implement Preventive Interventions for Lyme Disease

 , , and
, , and
Abstract
1. Introduction
1.1. Preventive Interventions for Lyme Disease (PILD)
1.2. Theoretical Models Explaining the Implementation of PILD
1.3. TPB Constructs
1.4. Background Factors: Perceived Severity and Vulnerability
1.5. The Present Study
- (1)
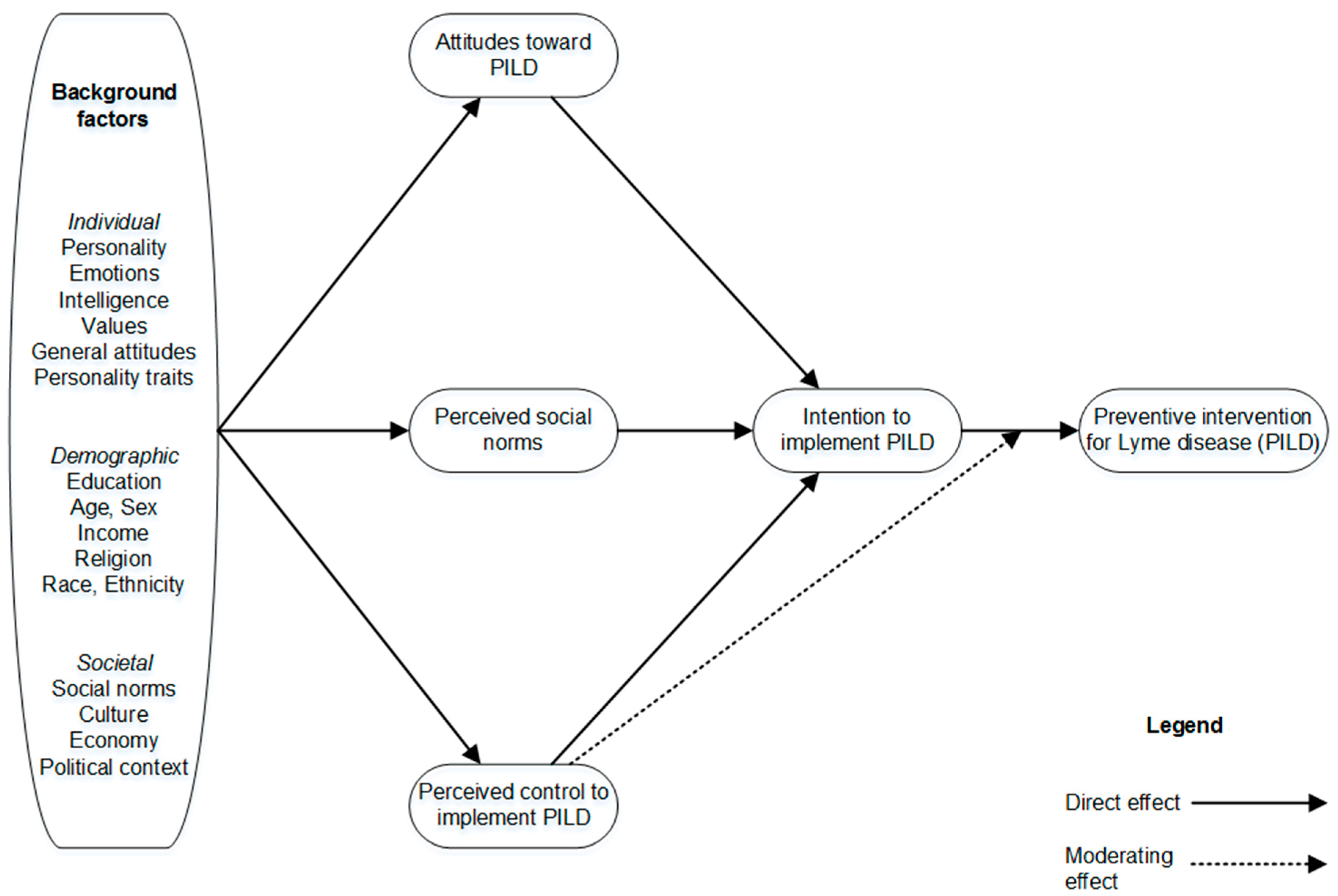
- Intention to implement PILD is the immediate antecedent of these interventions.
- (2)
- Municipal officers’ intention to implement PILD should increase to the extent that they hold favorable attitudes toward such interventions, think that significant others support these interventions (i.e., perceived social norm), and perceive that the municipality has control over them.
- (3)
- Valois et al. [54] showed that Quebec’s municipal officers have little control over the adoption of adaptive interventions for heat and flooding. Thus, we expect the relationship between municipal officers’ intention to implement PILD and their actual implementation of PILD to be moderated by the perceived barriers and perceived behavioral control (i.e., municipal officers’ perceptions of the degree to which their municipality is capable of, or have control over, implementing a given intervention). More specifically, we formulated the hypothesis that when municipal officers believe that their municipality actually has control over the implementation of PILD, they will tend to act in accordance with their intentions.
- (4)
- A high level of perceived risk (vulnerability) represented by Lyme disease and a high level of perceived impacts of Lyme disease (severity) on health is expected to be positively related to intentions to implement PILD. The effects are expected to be indirect, operating via attitude toward PILD, perceived social norms regarding PILD, and perceived control to implement PILD.
2. Materials and Methods
2.1. Participants
2.2. Questionnaire
2.2.1. Proximal Determinants of Intention and Implementation of PILD
2.2.2. Background Factors
2.2.3. Dependent Variables
2.2.4. Creation of the PILD Index
2.3. Statistical Analysis
2.3.1. Determinants of Municipal Authorities’ Implementation of PILD
3. Results
3.1. Descriptive Statistics
3.2. Test of the TPB Model with HBM Constructs without Moderating Effect
3.3. Test of the TPB Model with HBM Constructs with Moderating Effect
4. Discussion
4.1. Implementation of Preventive Interventions for Lyme Disease by Municipal Authorities
4.2. Factors Leading Some Municipalities to Be Active in Lyme Disease Prevention
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- INSPQ Maladies Vectorielles et Zoonoses—Mon Climat, Ma Santé. Available online: http://www.monclimatmasante.qc.ca/maladies-vectorielles-et-zoonoses.aspx (accessed on 24 October 2018).
- Costello, A.; Abbas, M.; Allen, A. Managing the health effects of climate change (Correction to: The Lancet 2009, 373, 1693–1733). Lancet 2009, 373, 2200. [Google Scholar]
- Gage, K.L.; Burkot, T.R.; Eisen, R.J.; Hayes, E.B. Climate and Vectorborne Diseases. Am. J. Prev. Med. 2008, 35, 436–450. [Google Scholar] [CrossRef]
- Ogden, N.H.; Lindsay, L.R.; Morshed, M.; Sockett, P.N.; Artsob, H. The emergence of Lyme disease in Canada. Can. Med Assoc. J. 2009, 180, 1221–1224. [Google Scholar] [CrossRef] [PubMed]
- Aguero-Rosenfeld, M.E.; Wang, G.; Schwartz, I.; Wormser, G.P. Diagnosis of Lyme Borreliosis. Clin. Microbiol. Rev. 2005, 18, 484–509. [Google Scholar] [CrossRef] [PubMed]
- Bouchard, C.; Leonard, E.; Koffi, J.K.; Pelcat, Y.; Peregrine, A.; Chilton, N.; Rochon, K.; Lysyk, T.; Lindsay, L.R.; Ogden, N.H. The increasing risk of Lyme disease in Canada. Can. Vet. J. 2015, 56, 693. [Google Scholar] [PubMed]
- Leighton, P.A.; Koffi, J.K.; Pelcat, Y.; Lindsay, L.R.; Ogden, N.H. Predicting the speed of tick invasion: An empirical model of range expansion for the Lyme disease vector Ixodes scapularis in Canada. J. Appl. Ecol. 2012, 49, 457–464. [Google Scholar] [CrossRef]
- Brownstein, J.; Holford, T.; Fish, D. Effect of climate change on Lyme Disease risk in North America. Ecohealth 2005, 2, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Bouchard, C.; Beauchamp, G.; Leighton, P.A.; Lindsay, R.; Bélanger, D.; Ogden, N.H. Does high biodiversity reduce the risk of Lyme disease invasion? Parasites Vectors 2013, 6, 195. [Google Scholar] [CrossRef] [PubMed]
- Ogden, N.H.; Bouchard, C.; Kurtenbach, K.; Margos, G.; Lindsay, L.R.; Trudel, L.; Nguon, S.; Milord, F. Active and passive surveillance and phylogenetic analysis of Borrelia burgdorferi elucidate the process of Lyme disease risk emergence in Canada. Environ. Health Perspect. 2010, 118, 909. [Google Scholar] [CrossRef] [PubMed]
- MSSS Tableau des cas Humains—Bilan 2018—Maladie de Lyme—Professionnels de la santé—MSSS. Available online: http://www.msss.gouv.qc.ca/professionnels/zoonoses/maladie-lyme/tableau-des-cas-humains-bilan/ (accessed on 24 October 2018).
- IPCC Annex II: Glossary. Climate Change 2014: Impacts, Adaptation, and Vulnerability. Part B: Regional Aspects. Contribution of Working Group II to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change [Barros, V. R., Field C. B., Dokken D. J. et al. (eds.)]; Agard, J., Schipper, L.F., Birkmann, J., Campos, M., Dubeux, C., Nojiri, Y., Olsson, L., Osman-Elasha, B., Pelling, M., Prather, M.J., et al., Eds.; Cambridge University Press: Cambridge, UK; New York, NY, USA, 2014; pp. 1757–1776. [Google Scholar]
- Smith, K.R.; Woodward, A.; Campbell-Lendrum, D.; Chadee, D.D.; Honda, Y.; Qiyong, L.; Olwoch, J.M.; Revich, B.; Sauerborn, R. Human Health: Impacts, Adaptation, and Co-Benefits. In Climate Change 2014: Impacts, Adaptation, and Vulnerability. Part A: Global and Sectoral Aspects. Contrubtion of Working Group II to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change; Confalonieri, U., Haines, A., Eds.; Cambridge University Press: Cambridge, UK; New York, NY, USA, 2014; Volume 1, pp. 709–754. [Google Scholar]
- Bélanger, D.; Abdous, B.; Gosselin, P.; Valois, P. An adaptation index to high summer heat associated with adverse health impacts in deprived neighborhoods. Clim. Chang. 2015, 132, 279–293. [Google Scholar]
- Araos, M.; Austin, S.E.; Berrang-Ford, L.; Ford, J.D. Public Health Adaptation to Climate Change in Large Cities: A Global Baseline. Int. J. Health Serv. 2016, 46, 53–78. [Google Scholar] [CrossRef] [PubMed]
- Austin, S.E.; Ford, J.D.; Berrang-Ford, L.; Araos, M.; Parker, S.; Fleury, M.D. Public health adaptation to climate change in Canadian jurisdictions. Int. J. Environ. Res. Public Health 2015, 12, 623–651. [Google Scholar] [CrossRef]
- Beard, C.B.; Eisen, R.J.; Barker, C.M.; Garofalo, J.F.; Hahn, M.; Hayden, M.; Monaghan, A.J.; Ogden, N.H.; Schramm, P.J. Ch. 5: Vectorborne Diseases; U.S. Global Change Research Program: Washington, DC, USA, 2016; pp. 129–156.
- Ogden, N.; Sockett, P.; Fleury, M. Public Health in Canada and Adaptation to Infectious Disease Risks of Climate Change: Are We Planning or Just Keeping Our Fingers Crossed? In Climate Change Adaptation in Developed Nations; Springer: Dordrecht, The Netherlands, 2011; pp. 161–175. [Google Scholar]
- Bulkeley, H.; Broto, V.C.; Edwards, G. Bringing climate change to the city: towards low carbon urbanism? Local Environ. 2012, 17, 545–551. [Google Scholar] [CrossRef]
- Henstra, D. Toward the climate-resilient city: extreme weather and urban climate adaptation policies in two Canadian provinces. J. Comp. Policy Anal. Res. Pract. 2012, 14, 175–194. [Google Scholar] [CrossRef]
- Gore, C.; Robinson, P. Local Government Response to Climate Change: Our Last, Best Hope? In Changing Climates in North American Politics: Institutions, Policymaking and Multilevel Governance; Selin, H., VanDeveer, S.D., Eds.; MIT Press: Cambridge, MA, USA, 2009; pp. 137–158. [Google Scholar]
- Ebi, K.L.; Semenza, J.C. Community-Based Adaptation to the Health Impacts of Climate Change. Am. J. Prev. Med. 2008, 35, 501–507. [Google Scholar] [CrossRef] [PubMed]
- Bulkeley, H.; Tuts, R. Understanding urban vulnerability, adaptation and resilience in the context of climate change. Local Environ. 2013, 18, 646–662. [Google Scholar] [CrossRef]
- Poutiainen, C.; Berrang-Ford, L.; Ford, J.; Heymann, J. Civil society organizations and adaptation to the health effects of climate change in Canada. Public Health 2013, 127, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, E. Local Solutions to A Global Problem?: Canadian Municipal Policy Responses to Climate Change. Ph.D. Thesis, University of British Columbia, Vancouver, BC, Canada, 20 April.
- Aenishaenslin, C.; Michel, P.; Ravel, A.; Gern, L.; Waaub, J.-P.; Milord, F.; Bélanger, D. Acceptability of tick control interventions to prevent Lyme disease in Switzerland and Canada: A mixed-method study. BMC Public Health 2016, 16, 12. [Google Scholar] [CrossRef]
- Piesman, J.; Eisen, L. Prevention of tick-borne diseases. Annu. Rev. Entomol. 2008, 53, 323–343. [Google Scholar] [CrossRef] [PubMed]
- Gould, L.H.; Nelson, R.S.; Griffith, K.S.; Hayes, E.B.; Piesman, J.; Mead, P.S.; Cartter, M.L. Knowledge, attitudes, and behaviors regarding Lyme disease prevention among Connecticut residents, 1999–2004. Vector Borne Zoonotic Dis. 2008, 8, 769–776. [Google Scholar] [CrossRef] [PubMed]
- Aenishaenslin, C.; Michel, P.; Ravel, A.; Gern, L.; Milord, F.; Waaub, J.-P.; Bélanger, D. Factors associated with preventive behaviors regarding Lyme disease in Canada and Switzerland: a comparative study. BMC Public Health 2015, 15, 185–195. [Google Scholar] [CrossRef]
- Phillips, C.B.; Liang, M.H.; Sangha, O.; Wright, E.A.; Fossel, A.H.; Lew, R.A.; Fossel, K.K.; Shadick, N.A. Lyme disease and preventive behaviors in residents of Nantucket Island, Massachusetts. Am. J. Prev. Med. 2001, 20, 219–224. [Google Scholar] [CrossRef]
- Aenishaenslin, C.; Bouchard, C.; Koffi, J.K.; Ogden, N.H. Exposure and preventive behaviours toward ticks and Lyme disease in Canada: Results from a first national survey. Ticks Tick-Borne Dis. 2017, 8, 112–118. [Google Scholar] [CrossRef]
- Aenishaenslin, C.; Bouchard, C.; Koffi, J.K.; Pelcat, Y.; Ogden, N.H. Evidence of rapid changes in Lyme disease awareness in Canada. Ticks Tick-Borne Dis. 2016, 7, 1067–1074. [Google Scholar] [CrossRef] [PubMed]
- Mowbray, F.; Amlôt, R.; Rubin, G.J. Ticking All the Boxes? A Systematic Review of Education and Communication Interventions to Prevent Tick-Borne Disease. Vector-Borne Zoonotic Dis. 2012, 12, 817–825. [Google Scholar] [CrossRef] [PubMed]
- Fielding, G.; McPherson, M.; Hansen-Ketchum, P.; MacDougall, D.; Beltrami, H.; Dunn, J. Climate change projections and public health systems: Building evidence-informed connections. One Health 2016, 2, 152–154. [Google Scholar] [CrossRef] [PubMed]
- Malouin, R.; Winch, P.; Leontsini, E.; Glass, G.; Simon, D.; Hayes, E.B.; Schwartz, B.S. Longitudinal evaluation of an educational intervention for preventing tick bites in an area with endemic lyme disease in Baltimore County, Maryland. Am. J. Epidemiol. 2003, 157, 1039–1051. [Google Scholar] [CrossRef] [PubMed]
- Daltroy, L.H.; Phillips, C.; Lew, R.; Wright, E.; Shadick, N.A.; Liang, M.H. A Controlled Trial of a Novel Primary Prevention Program for Lyme Disease and Other Tick-Borne Illnesses. Health Educ. Behav. 2006, 34, 531–542. [Google Scholar] [CrossRef] [PubMed]
- Klöckner, C.A. A comprehensive model of the psychology of environmental behaviour—A meta-analysis. Glob. Environ. Chang. 2013, 23, 1028–1038. [Google Scholar] [CrossRef]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Rosenstock, I.M. The Health Belief Model and Preventive Health Behavior. Health Educ. Behav. 1974, 2, 354–386. [Google Scholar] [CrossRef]
- Conner, M.; Norman, P. Predicting Health Behaviour; Open University Press: Maidenhead, Berkshire, UK, 2005. [Google Scholar]
- Grothmann, T.; Patt, A. Adaptive capacity and human cognition: The process of individual adaptation to climate change. Glob. Environ. Chang. 2005, 15, 199–213. [Google Scholar] [CrossRef]
- Unsworth, K.; Russel, S.V.; Lewandowsky, S.; Lawrence, C.; Fielding, K.; Heath, J.; Evans, A.; Hurlstone, M.J.; Mcneill, I.M. What about Me? Factors Affecting Individual Adaptive Coping Capacity across Different Population; National Climate Change Adaptation Research Facility: Gold Coast, Australia, 2013. [Google Scholar]
- Nosek, B.A.; Graham, J.; Lindner, N.M.; Kesebir, S.; Hawkins, C.B.; Hahn, C.; Schmidt, K.; Motyl, M.; Joy-Gaba, J.; Frazier, R. Cumulative and career-stage citation impact of social-personality psychology programs and their members. Personal. Soc. Psychol. Bull. 2010, 36, 1283–1300. [Google Scholar] [CrossRef] [PubMed]
- Ajzen, I. The theory of planned behaviour: Reactions and reflections. Psychol. Health 2011, 26, 1113–1127. [Google Scholar] [CrossRef]
- Gifford, R. Environmental psychology matters. Annu. Rev. Psychol. 2014, 65, 541–579. [Google Scholar] [CrossRef] [PubMed]
- Bouchard, C.; Aenishaenslin, C.; Rees, E.E.; Koffi, J.K.; Pelcat, Y.; Ripoche, M.; Milord, F.; Lindsay, L.R.; Ogden, N.H.; Leighton, P.A. Integrated Social-Behavioral and Ecological Risk Maps to Prioritize Local Public Health Responses to Lyme Disease. Environ. Health Perspect. 2018, 126, 047008. [Google Scholar] [CrossRef] [PubMed]
- Bayles, B.R.; Evans, G.; Allan, B.F. Knowledge and prevention of tick-borne diseases vary across an urban-to-rural human land-use gradient. Ticks Tick-Borne Dis. 2013, 4, 352–358. [Google Scholar] [CrossRef] [PubMed]
- Heller, J.E.; Benito-Garcia, E.; Maher, N.E.; Chibnik, L.B.; Maher, C.P.; Shadick, N.A. Behavioral and attitudes survey about Lyme disease among a Brazilian population in the endemic area of Martha’s Vineyard, Massachusetts. J. Immigr. Minor. Health 2010, 12, 373–383. [Google Scholar] [CrossRef] [PubMed]
- Llewellyn, D.M.; Brazier, A.; Brown, R.; Cocker, J.; Evans, M.L.; Hampton, J.; Nutley, B.P.; White, J. Occupational exposure to permethrin during its use as a public hygiene insecticide. Ann. Occup. Hyg. 1996, 40, 499–509. [Google Scholar] [CrossRef]
- Sibbald, B. Larvicide debate marks start of another West Nile virus summer. CMAJ 2003, 168, 1455. [Google Scholar]
- Ajzen, I. The theory of planned behavior. In Handbook of Theories of Social Psychology; Lange, P.A.M., Kruglanski, A.W., Higgins, E.T., Eds.; Sage: London, UK, 2012; Vol. 1, pp. 438–459. [Google Scholar]
- Fishbein, M.; Ajzen, I. Predicting and Changing Behavior: The Reasoned Action Approach; Psychology Press: New York, NY, USA, 2010; ISBN 9780805859249. [Google Scholar]
- Ajzen, I. From intentions to actions: A theory of planned behavior. In Action-Control: From Cognition to Behavior; Kuhl, J., Beckman, J., Eds.; Springer: Heidelberg, Germany, 1985; pp. 11–39. [Google Scholar]
- Valois, P.; Jacob, J.; Mehiriz, K.; Talbot, D.; Renaud, J.-S.; Caron, M. Niveau et Déterminants de L’Adaptation Aux Changements Climatiques Dans Les Municipalités du Québec; OQACC: Québec, QC, Canada, 2017. [Google Scholar]
- Briand, S.; Adam-Poupart, A.; Irace-Cima, A.; Thivierge, K. Cartographie du Risque D’Acquisition de la Maladie de Lyme au Québec: Année 2017; INSPQ: Montreal, QC, Canada, 2017. [Google Scholar]
- Whetten, D.A.; Felin, T.; King, B.G. The Practice of Theory Borrowing in Organizational Studies: Current Issues and Future Directions. J. Manag. 2009, 35, 537–563. [Google Scholar] [CrossRef]
- Papagiannakis, G.; Lioukas, S. Values, attitudes and perceptions of managers as predictors of corporate environmental responsiveness. J. Environ. Manag. 2012, 100, 41–51. [Google Scholar] [CrossRef]
- Sharma, P.; Sharma, S. Drivers of Proactive Environmental Strategy in Family Firms. Bus. Ethics Q. 2011, 21, 309–334. [Google Scholar] [CrossRef]
- Saha, D.; Paterson, R.G. Local Government Efforts to Promote the “Three Es” of Sustainable Development: Survey in Medium to Large Cities in the United States. J. Plan. Educ. Res. 2008, 28, 21–37. [Google Scholar] [CrossRef]
- Samejima, F. Estimation of Latent Ability Using a Response Pattern of Graded Scores (Psychometrika Monograph No. 17); Psychometric Society: Richmond, VA, USA, 1969. [Google Scholar]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide, 7th ed.; Muthén & Muthén: Los Angeles, CA, USA, 2015. [Google Scholar]
- Kline, R. Principles and Practice of Structural Equation Modeling, 3rd ed.; Guildford Publications: New York, NY, USA, 2011; ISBN 1-60623-877-9. [Google Scholar]
- Muthén, B.O.; Muthén, L.K.; Asparouhov, T. Estimator Choices with Categorical Outcomes. Available online: https://www.statmodel.com/download/EstimatorChoices.pdf (accessed on 26 April 2019).
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide, 6th ed.; Muthén & Muthén: Los Angeles, CA, USA, 2010. [Google Scholar]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Modeling: A Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Van Buuren, S.; Groothuis-Oudshoorn, K. mice: Multivariate Imputation by Chained Equations. R. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar] [CrossRef]
- The R Project for Statistical Computing. Available online: https://www.r-project.org/ (accessed on 29 April 2019).
- Forest-Berard, K.; Cima, A.I.; Thivierge, K.; Briand, S.; Milord, F.; Leighton, P.; Lindsay, R.; Adam-Poupart, A. From Prey to Hunter: Training Park Workers to Carry Out Tick Collection as an Alternative Approach for Lyme Disease Vector Surveillance. In Proceedings of the ISEE Conference Abstracts, Ottawa, ON, Canada, 28 August 2018. [Google Scholar]
- Berrang-Ford, L.; Ford, J.D.; Paterson, J. Are we adapting to climate change? Glob. Environ. Chang. 2011, 21, 25–33. [Google Scholar] [CrossRef]
- Piesman, J.; Beard, C.B. Direct from CDC environmental health service branch: Prevention of Tick-Borne Diseases. J. Environ. Health 2012, 74, 30–35. [Google Scholar] [PubMed]
- Ferguson, C.J. An effect size primer: A guide for clinicians and researchers. Prof. Psychol. Res. Pract. 2009, 40, 532–538. [Google Scholar] [CrossRef]
- Bakhsh, K.; Rauf, S.; Zulfiqar, F. Adaptation strategies for minimizing heat wave induced morbidity and its determinants. Sustain. Cities Soc. 2018, 41, 95–103. [Google Scholar] [CrossRef]
- Bichard, E.; Kazmierczak, A. Are homeowners willing to adapt to and mitigate the effects of climate change? Clim. Chang. 2012, 112, 633–654. [Google Scholar] [CrossRef]
- Liu, T.; Xu, Y.J.; Zhang, Y.H.; Yan, Q.H.; Song, X.L.; Xie, H.Y.; Luo, Y.; Rutherford, S.; Chu, C.; Lin, H.L.; et al. Associations between risk perception, spontaneous adaptation behavior to heat waves and heatstroke in Guangdong province, China. BMC Public Health 2013, 13, 913. [Google Scholar] [CrossRef] [PubMed]
- Huq, S.; Reid, H.; Konate, M.; Rahman, A.; Sokona, Y.; Crick, F. Mainstreaming adaptation to climate change in Least Developed Countries (LDCs): Climate Policy: Vol 4, No 1. Clim. Policy 2004, 4, 25–43. [Google Scholar] [CrossRef]
- Smit, B.; Wandel, J. Adaptation, adaptive capacity and vulnerability. Glob. Environ. Chang. 2006, 16, 282–292. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Quebec Health Region | Response Rate by Region (n/N) a | Percentage of Reported Human Cases of Lyme Disease (Acquired Locally) in 2018 |
|---|---|---|
| Capitale-Nationale | 25/59 (42%) | 0 (0%) |
| Mauricie-Centre du Québec | 34/121 (28%) | 17 (8%) |
| Estrie | 28/89 (31%) | 87 (40%) |
| Montreal | 12/34 (35%) | 1 (0.5%) |
| Outaouais | 27/67 (40%) | 2 (0.9%) |
| Chaudière-Appalaches | 37/136 (27%) | 0 (0%) |
| Laval | 0/1 (0%) | 0 (0%) |
| Lanaudière | 25/57 (44%) | 2 (0.9%) |
| Laurentides | 34/76 (45%) | 2 (0.9%) |
| Montérégie | 71/177 (40%) | 93 (42%) |
| Other b | 15 (6.8%) | |
| TOTAL | 293/817 (36%) | 219 (100%) |
| Municipality Sizes | Number | % |
|---|---|---|
| 1–499 | 42 | 14% |
| 500–999 | 67 | 23% |
| 1000–1999 | 44 | 15% |
| 2000–2999 | 31 | 11% |
| 3000–3999 | 16 | 6% |
| 4000–4999 | 10 | 3% |
| 5000–9999 | 35 | 12% |
| 10,000–49,999 | 30 | 10% |
| 50,000 + | 18 | 6% |
| TOTAL | 293/820 | 100% |
| Questions Used and Preventive Interventions | Scale | Method Used to Create the Score (Min. and Max.) | |
|---|---|---|---|
| Seeking information (PILD-1) | Using the following scale of responses, please indicate if you, or someone else employed by your municipality, has already inquired about... Whether the municipality is located in an area where people are at risk for Lyme disease About ways to better prevent Lyme disease About the impact Lyme disease may have on physical or mental health | (1) Yes, (0) No | Sum of all 3 items (Min = 0; Max = 3) |
| Actions discussed and actions implemented (PILD-2) | Using the following scale, please indicate the extent to which staff in your municipality have, over the last 2 years, (discussed/implemented) the following actions to protect the population from Lyme disease. Separate woodlots from the lawn with wood chips, mulch, or gravel Place children’s games and sandboxes away from the edge of woodland Place children’s games and sandboxes that are near woodlots on a structure made of woodchips or mulch Protect areas surrounding buildings located near wooded areas by pavement, low wall, or plantation container Remove vegetation along walking paths Delineate public access woodlots with gates to keep away deer | (0) Never, (1) To my knowledge this was discussed at an official meeting, (2) This has been implemented | Sum of all 6 items (Min = 0; Max = 12) (6–12) A majority of the actions were implemented. Final score of 2. (1–5) Few actions were implemented or discussed. Final score of 1. (0) Nothing was discussed or implemented. Final score of 0. (Min = 0; Max = 2) |
| Information to the population (PILD-3) | Using the following scale of response, please indicate whether your municipality has already made available information about Lyme disease, for example on the municipality’s website, via flyers, or information boards at the parks entrance. List of nine types of information made available about Lyme disease, (e.g., on the municipality’s website, in leaflets, or on information boards at park entrances) Areas where people are at risk of acquiring Lyme disease in the area A description of the disease A description of the tick A description of the symptoms Possible protection and prevention measures Tips to remove the tick Information on what to do with the tick once removed References for more information on the disease References about who and when to consult for medical advice | (1) Yes, (0) No | Sum of all 9 items Min = 0; Max = 9 |
| Upstream actions (PILD-4) | Have you, or anyone else employed by your municipality, ever… Read the information provided by the staff of a regional health and social services center about the municipality being located on a territory where people are at risk of contracting Lyme disease Drafted a briefing note regarding Lyme disease to a decision-making (e.g., City Council) or advisory (e.g., Planning Advisory Committee) body Proposed action recommendations for Lyme disease to a decision-making (e.g., City Council) or advisory (e.g., Planning Advisory Committee) body Worked to develop partnerships or collaborations with other organizations (e.g., a health and social services center, department of public health, health and social services ministry) with the aim of dealing with Lyme disease Worked to develop an action plan for the municipality with respect to Lyme disease | (1) Yes, (0) No | Sum of all 5 items Min = 0; Max = 5 |
| Variables | # of Items | M | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. PILD index | 4 | 5.61 | 5.25 | - | ||||||
| 2. Intention | 3 | 2.42 | 0.73 | 0.322 ** | - | |||||
| 3. Attitude | 3 | 2.71 | 0.61 | 0.236 ** | 0.683 ** | - | ||||
| 4. Perceived social norms | 3 | 2.23 | 0.75 | 0.305 ** | 0.415 ** | 0.481 ** | - | |||
| 5. Perceived control (barriers) | 7 | 3.06 | 0.47 | −0.042 | −0.242 * | −0.211 | -0.028 | - | ||
| 6. Perceived vulnerability | 1 | 2.52 | 1.34 | 0.479 ** | 0.131 | 0.131 | 0.075 | 0.059 | - | |
| 7. Perceived severity | 2 | 3.22 | 0.54 | 0.218 ** | 0.157 | 0.213* | 0.161 | −0.029 | 0.230 ** | - |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jacob, J.; Valois, P.; Aenishaenslin, C.; Bouchard, C.; Briand, S.; Talbot, D.; Tessier, M. Factors Leading Municipal Authorities to Implement Preventive Interventions for Lyme Disease. Int. J. Environ. Res. Public Health 2019, 16, 1547. https://doi.org/10.3390/ijerph16091547
Jacob J, Valois P, Aenishaenslin C, Bouchard C, Briand S, Talbot D, Tessier M. Factors Leading Municipal Authorities to Implement Preventive Interventions for Lyme Disease. International Journal of Environmental Research and Public Health. 2019; 16(9):1547. https://doi.org/10.3390/ijerph16091547
Chicago/Turabian StyleJacob, Johann, Pierre Valois, Cécile Aenishaenslin, Catherine Bouchard, Sandie Briand, Denis Talbot, and Maxime Tessier. 2019. "Factors Leading Municipal Authorities to Implement Preventive Interventions for Lyme Disease" International Journal of Environmental Research and Public Health 16, no. 9: 1547. https://doi.org/10.3390/ijerph16091547
APA StyleJacob, J., Valois, P., Aenishaenslin, C., Bouchard, C., Briand, S., Talbot, D., & Tessier, M. (2019). Factors Leading Municipal Authorities to Implement Preventive Interventions for Lyme Disease. International Journal of Environmental Research and Public Health, 16(9), 1547. https://doi.org/10.3390/ijerph16091547