Learning by Doing and Training Satisfaction: An Evaluation by Health Care Professionals



Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Universe and Sample
2.3. Instrument
- Satisfaction with the training methodology, comprising two variables: (a) Participants’ opinions concerning the Learning by Doing method, in comparison with other training techniques that they had experienced (e.g., classroom teaching, workshops, conferences, etc.). Response options were 1-‘Yes’ (satisfied) or 0-‘No’ (not satisfied); and, (b) the degree of knowledge/skills retention, as an indicator of being able to utilize the information at work. Results were in accordance with a Likert scale from 0 (none), the lowest retention level, to 3 (a lot), the highest. The dimension combined the above variables and gave values between 0 and 4.
- Satisfaction with the training program. Target variables were: (a) The instructor; (b) the course content; (c) the didactic approach; (d) time invested in the course; and, (e) program management by the institution. Response options for the five variables were 1-‘Yes’ (satisfied) or 0-‘No’ (not satisfied). The results for the variables were integrated to give an overall value for the dimension between 0 (no satisfaction) and 5 (completely satisfied).
- Satisfaction with the improvement in professional competence. The following variables [22] were measured by means of a Likert scale from 0 (no satisfaction) to 3 (completely satisfied): (a) Acquisition of new knowledge/skills; (b) usefulness for work; (c) applicability of knowledge/skills; (d) improvement of professional knowledge/skills; and, (e) cascade training (transmission of knowledge and skills to other colleagues. This section of the questionnaire included the option of adding supplementary comments. The overall value for the dimension was a score between 0 and 9 (the higher the score, the more positive the evaluation).
- Satisfaction with the improvement in quality of care. Participants were asked if they felt that their skills in the areas of diagnosis, treatment, and care had improved after they had taken the course. Scores were 0 (no) or 1 (yes).
- Satisfaction with the economic repercussions. Two variables were considered: (a) Optimization of recourses—participants were asked if they thought the application of what they had learnt on the course would lead to better use of the resources of the health center where they worked; response options were 0 (no), or 1 (yes); and, (b) impact on expenditure—participants were asked if they thought the course had an impact on the expenditure of their health center or service; response options were 0 (an increase in expenditure), 1 (no impact), or 2 (reduction). The overall value for the two variables was given on a scale of 0–3.
2.4. Ethics Approval And Consent to Participate
3. Results
3.1. Descriptive Results
- Satisfaction with the training methodology: (a) All participants (100%) recognized the positive effects of the Learning by Doing methodology compared to other training programs; (b) 70.1% stated they felt that they had improved their knowledge and skills and 20.4% believed they had improved ‘a lot’. The average score (0 to 4) was 3.11 with a standard deviation of 0.54.
- Satisfaction with the training program: The percentages for satisfaction were very high in all the variables—93.8% for the instructor; 94.4% for course content; 96.2% for didactic approach; 87.1% for time invested in the course; and, 95.1% for program management by the institution. The average score for general satisfaction (0 to 5) was 4.67 with a standard deviation of 0.82.
- Satisfaction with the improvement in professional competence: (a) Acquisition of new knowledge/skills—59.7% were very satisfied, and 35.2% were quite satisfied; (b) 99.5% of the sample stated that the course was very useful for their work; (c) applicability—only 13.2% said that they could not apply the knowledge/skills they had learnt, mainly due to the lack of patients, equipment, or time; (d) 91.6% believed that the course had led to an improvement of their professional knowledge and skills; and, (e) 79.6% said they were able to transmit their new knowledge and skills to their colleagues. The average score (0 to 9) for the variables related to professional competence was 7.49 with a standard deviation of 1.31.
- Satisfaction with the improvement in quality of care: 95.7% said that they felt the course had improved their diagnostic, treatment, and care skills at work (scores of 0 = no and 1 = yes).
- Satisfaction with the economic repercussions: (a) 79% gave a positive response regarding better use of resources; (b) 73.7% believed that the training course would not lead to an increase in health care expenses. The average score (0 to 3) was 1.25 with a standard deviation of 1.11.
3.2. Inferential Results
- Satisfaction with the improvement in quality of care had a statistically significant relationship with a positive evaluation of the improvement of competence and satisfaction with the applicability of the knowledge and skills that were learnt on the training course.
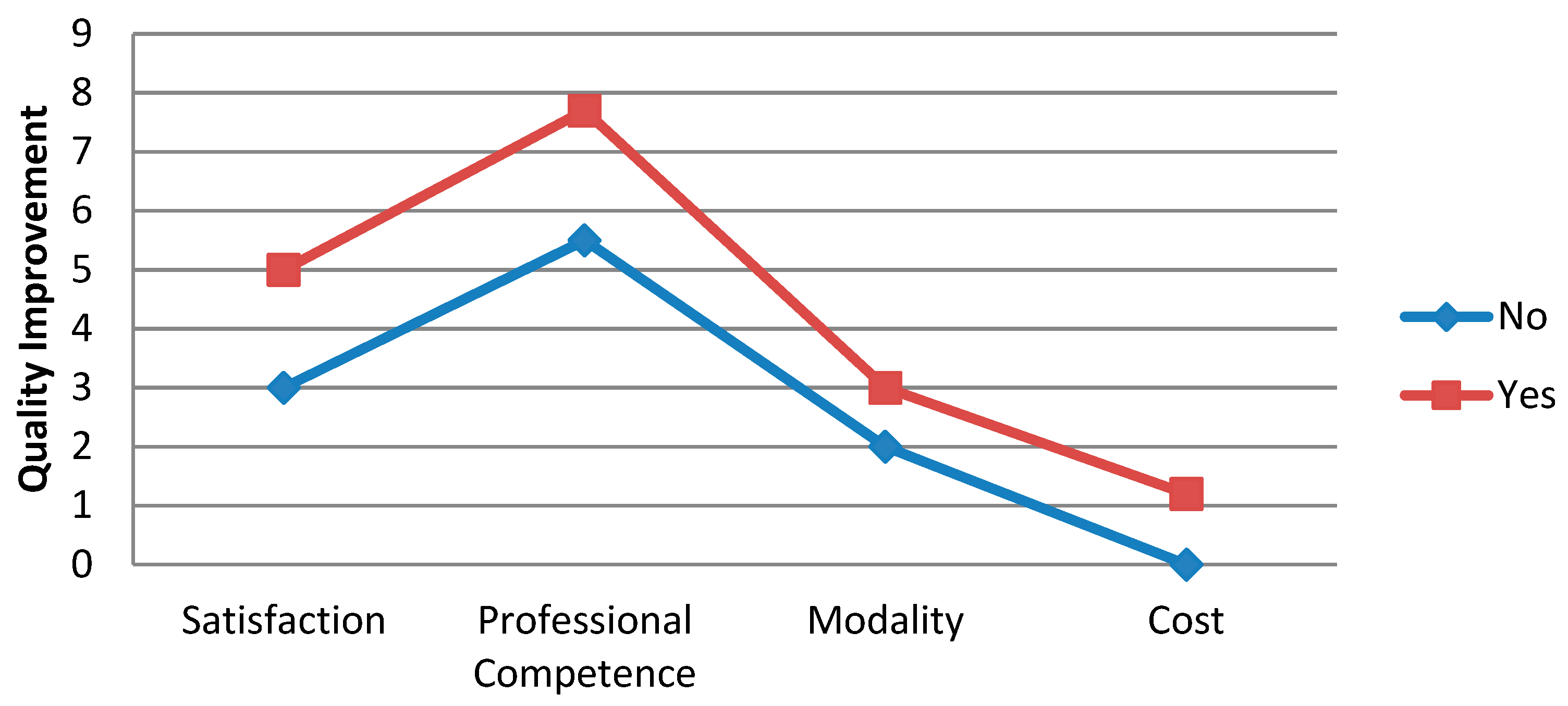
- A total of 98% of participants were satisfied with the course and believed that they had improved their professional competence, were able to apply the new knowledge and skills at work, and/or had improved the quality of care. Participants that were not satisfied with the course and did not feel that their professional competence had improved gave a mean score of 2.83 (1.72); this contrasts with those that were satisfied and felt their professional skills had improved who gave a mean score of 4.75 (0.66). Differences were statistically significant (p = 0.000).
- The analysis confirmed a relationship between satisfaction with the applicability of the knowledge and skills learnt on the course and satisfaction with the improvement in quality of care; 92.2% of participants were in agreement and responses were consistent.
4. Discussion
Limitations and Future Work
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Health Systems Governance for Universal Health Coverage Action Plan; WHO Publications: Geneva, Switzerland, 2014. [Google Scholar]
- Cunnigham, F.C.; Ferguson-Hill, S.; Matthews, V.; Bailie, R. Leveraging quality improvement through use of the Systems Assessment Tools in Indigenous primary health care services: A mix methods study. BMC Health Serv. Res. 2016, 16, 583. [Google Scholar]
- Donabedian, A. Evaluating the quality of medical care. Milbank Q. 2005, 83, 691–729. [Google Scholar] [CrossRef]
- Ellet, J.D.; Campbell, J.A.; Gonsalves, W.C. Patient satisfaction in a student-run free medical clinic. Fam Med. 2010, 42, 16–18. [Google Scholar]
- Schoenfelder, T.; Klewer, J.; Kugler, J. Determinants of patient satisfaction: A study of among 39 hospitals in an in-patient setting in Germany. Int. J. Qual. Health Care 2011, 23, 503–509. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Ciordia, I.; Guillén-Grima, F.; Burgos, A.; Aguinaga, I. Satisfacción laboral y factores de mejora en profesionales de atención primaria. Anales del Sistema Sanitario de Navarra 2013, 36, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Robbins, S.P. Comportamiento Organizacional; Pearson Educación: Madrid, Spain, 2004. [Google Scholar]
- Güleryüz, G.; Güney, S.; Aydın, E.M.; Aşan, Ö. The mediating effect of job satisfaction between emotional intelligence and organisational commitment of nurses: A questionnaire survey. Int. J. Nurs. Stud. 2008, 45, 1625–1635. [Google Scholar] [CrossRef] [PubMed]
- Casas, J.; Repullo, J.R.; Lorenzo, S.; Cañas, J.J. Dimensiones y medición de la calidad de vida laboral en profesionales sanitarios. Rev. Admin. Sanit. 2002, 6, 143–160. [Google Scholar]
- Mingote-Adán, J.; Moreno-Jiménez, B.; Gálvez-Herrero, M. Desgaste profesional y salud de los profesionales médicos: Revisión y propuestas de prevención. Med. Clín. 2004, 123, 265–270. [Google Scholar] [CrossRef]
- Martín, M.C.; Fernández, F.B.; Gómez, R.N.; Martínez, F.C. Prevalencia y factores asociados al burnout en un área de salud. Aten Primaria 2001, 27, 313–317. [Google Scholar] [CrossRef][Green Version]
- Sobrequés, J.; Cebriá, J.; Segura, J.; Rodríguez, C.; García, M.; Juncosa, S. La satisfacción laboral y el desgaste profesional de los médicos de atención primaria. Aten Primaria 2003, 31, 227–233. [Google Scholar] [CrossRef][Green Version]
- Grau, A.; Suñer, R.; García, M.M. Desgaste profesional en el personal sanitario y su relación con los factores personales y ambientales. Gac Sanit. 2005, 19, 463–470. [Google Scholar] [CrossRef][Green Version]
- Salcedo, J.A. Control y evaluación de recursos humanos. In Motivación Saludable: Los Recursos Humanos en el Sector de la Salud; Lázaro, P., Marín, I., Eds.; Universidad Internacional Menéndez Pelayo; Fundación SB: Santander, Spain, 2015; pp. 283–292. [Google Scholar]
- Halldorsdottir, S.; Einarsdottir, E.J.; Edvardsson, I.R. Effects of cutbacks on motivating factors among nurses in primary health care. Scand. J. Caring Sci. 2018, 32, 397–406. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Seco, E.; Coll-Benejam, J.M.; Torrent-Quetglas, M.; Linares-Pou, L. Influencia del clima laboral en la satisfacción de los profesionales sanitarios. Aten Primaria 2006, 37, 209–214. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Ruzafa-Martínez, M.; Madrigal-Torres, M.; Velandrino-Nicolás, A.; López-Iborra, L. Satisfacción laboral de los profesionales de enfermería españoles que trabajan en hospitales ingleses. Gac Sanit. 2008, 22, 434–442. [Google Scholar] [CrossRef] [PubMed]
- Campbell, C.; Silver, I.; Sherbino, J.; Cate, O.T.; Holmboe, E.S. Competency-based continuing professional development. Med. Teach. 2010, 32, 657–662. [Google Scholar] [CrossRef] [PubMed]
- Escribà-Agüir, V.; Artazcoz, L.; Pérez-Hoyos, S. Efecto del ambiente psicosocial y de la satisfacción laboral en el síndrome de burnout en médicos especialistas. Gac Sanit. 2008, 22, 300–308. [Google Scholar] [CrossRef] [PubMed]
- Pades, A.; Homar, C. El estrés de los estudiantes en las prácticas clínicas de enfermería. Rev. ROL Enferm. 2006, 29, 577–582. [Google Scholar]
- Morales, S.; Gascón, S.; Martínez, B.; Amores, M.; Bolea, M. La turnicidad como factor de riesgo psicosocial en personal hospitalario. In Proceedings of the II Simposium Internacional de Prevención de Riesgos Profesionales y Salud Ocupacional, Santiago de Chile, Chile, 30 November–2 December 2005; p. ORP.65. [Google Scholar]
- Miller, G.E. The assesment of clinical skills/competence/performance. Acad. Med. 1990, 65, 63–67. [Google Scholar] [CrossRef]
- Garafalo, L. Continuing Nursing Education and Outcomes: Making a Difference in Patient Care. J. Contin. Educ. Nurs. 2016, 47, 103–105. [Google Scholar]
- Gracia-Perez, M.L.; Gil-Lacruz, M. The impact of continuing training program on the perceived improvement in quality of health care delivered by health care professionals. Eval. Program Plann. 2018, 66, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Headrick, I.A.; Ogrinc, G.; Hoffman, K.G.; Stevenson, K.M.; Shalaby, M.; Beard, A.S.; Thöme, K.E.; Coleman, M.T.; Baum, K.D. Exemplary care and learning sites: A model for achieving continual improvement in care and learning in the clinical setting. Acad. Med. 2016, 91, 354–359. [Google Scholar] [CrossRef] [PubMed]
- Fernández, A.; Porcel, A.M.; Nuviala, A.; Pérez, R.J.; Tamayo, J.; Grao, A.; González, J.J. Estudio comparativo entre una metodología de aprendizaje tradicional respecto a una metodología de aprendizaje basada en el “learning by doing” para la consecución de competencias específicas. Revista UPO Innova 2012, I, 159–166. [Google Scholar]
- Dewey, J. Democracia y Educación; Ediciones Morata: Madrid, Spain, 1995. [Google Scholar]
- Kolb, D. Experiential Learning: Experience as the Source of Learning Development; Prentice Hall: Englewood Cliffs, NJ, USA, 1984. [Google Scholar]
- Borgnakke, K. Ethnographic Studies and Analysis of a Recurrent Theme: Learning by doing. Eur. Educ. Res. J. 2004, 3, 539–565. [Google Scholar] [CrossRef]
- McEwen, L.A.; Griffths, J.; Schultz, K. Developing and successfully implementing a competency-based portfolio assessment system in a postgraduate family medicine residency program. Acad. Med. 2015, 90, 1515–1526. [Google Scholar] [CrossRef] [PubMed]
- Ackerman, S.L.; Boscardin, C.; Karliner, L.; Handley, M.A.; Cheng, S.; Gaither, T.; Hagey, J.; Hennein, L.; Malik, F.; Shaw, B.; et al. The Action Research Program: Experiential Learning in Systems-Based Practice for First Year Medical Students. Teach. Learn. Med. 2016, 28, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Biencinto, C.; Carballo, R. Revisión de modelos de evaluación del impacto de la formación en el ámbito sanitario: De lo general a lo específico. Revista Electrónica de Investigación Educativa, RELIEVE 2004, 10, 101–116. [Google Scholar] [CrossRef][Green Version]
- Chacón-Moscoso, S.; Holgado-Tello, F.P.; López-García, J.M.; Sanduvete-Chaves, S. Evaluación de la Formación Continua: Fundamentos Teóricos y Herramientas Metodológicas; Universidad de Sevilla, Secretariado de Publicaciones: Sevilla, Spain, 2006. [Google Scholar]
- Pineda, P. Evaluación del impacto de la formación en las organizaciones. Revista Educar 2000, 27, 119–133. [Google Scholar]
- Gracia-Pérez, M.L. Evaluación del Impacto Formativo: Dimensiones y Modelos: Una Experiencia en la Sanidad de Aragón. Ph.D. Thesis, University of Zaragoza, Zaragoza, Spain, 2015. [Google Scholar]
- Argimón, J.M.; Jiménez, J. Métodos de Investigación en Clínica y Epidemiología; Elsevier: Madrid, Spain, 2004. [Google Scholar]
- Wellings, C.A.; Gendek, M.A.; Gallagher, S.E. Evaluating Continuing Nursing Education. J. Nur. Prof. Dev. 2017, 33, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Lapkin, S.; Levett-Jones, T.; Gilligan, C.A. A systematic review of the effectiveness of interprofessional education in health professional programs. Nurse Educ. Today 2013, 33, 90–102. [Google Scholar] [CrossRef]
- Wildeman, M.A.; Fles, R.; Adham, M.; Mayangsari, I.D.; Luirink, I. Short-term effect of different teaching methods on nasopharyngeal carcinoma for general practitioners in Jakarta, Indonesia. PLoS ONE 2012, 3, 1–7. [Google Scholar] [CrossRef][Green Version]
- Moll, A.; Lambert, S.; Visker, J.; Dunseith, N.; Wang, A.; Azim, S. A case study activity to assess nursing students’ perceptions of their interprofessional healthcare team’s collaborative decision-making process. J. Interprof. Educ. Prac. 2019, 14, 18–21. [Google Scholar] [CrossRef]
- Sick, B.; Hager, K.D.; Uden, D.; Friederich, C.; Kim, H.M.; Branch-Mays, G.; Pittenger, A. Using a guided reflection tool and debriefing session to learn from interprofessional team interactions in clinical settings. J. Interprof. Educ. Prac. 2019, 14, 53–57. [Google Scholar] [CrossRef]
- Kilby, K.A.; Grajny, A.M.; Guarino, A.J.; Paniszyn, L.A.; McErlean, M. Experiental learning exercise to achieve objective assessment of interprofessional education. J. Interprof. Educ. Prac. 2019, 14, 48–50. [Google Scholar]
- Hollamby, J.; Taylor, I.; Berragan, E.; Taylor, D.; Morgan, J. Preparing students for safe practice using an interprofessional ward simulation. J. Interprof. Educ. Prac. 2019, 14, 78–82. [Google Scholar] [CrossRef]
- Yoshino, Y.; Willott, C.; Gendenjamtz, E.; Surenkhorloo, A.; Islam, M.; Sakashita, R. Outcome Evaluation of Web Based Learning and Continuing Education Program for Maternal and Child Health Nursing and Other Professionals in Mongolia. Cent Asian J. Med. Sci. 2018, 4, 253–263. [Google Scholar]
- Tylre, S.; Bourbon, E.; Co, S.; Day, N.; Fineran, C. Clinical Competency, Self-Efficacy, and Job Satisfaction Perceptions of the Staff Nurse. J. Nurses Profess. Dev. 2012, 28, 32–35. [Google Scholar] [CrossRef]
- Meldahl, M.L.; Acaster, S.; Hayes, R.P. Exploration of oncologists’ attitudes toward and perceived value of patient reported outcomes. Qual. Life Res. 2013, 22, 725–731. [Google Scholar] [CrossRef] [PubMed]
- Rice, S.; Winter, S.R.; Doherty, S.; Milner, M. Advantages and Disadvantages of Using Internet-Based Survey Methods in Aviation-Related Research. J. Aviat. Technol. Eng. 2017, 7, 58–65. [Google Scholar] [CrossRef]
- Hernán, M.; Gutiérrez, J.L.; Lineros, C.; Ruiz, C.; Rabadán, A. Los pacientes y la calidad de los servicios de atención primaria de salud. Opinión de los profesionales de los centros de salud de la Bahía de Cádiz y La Janda. Aten Primaria 2002, 30, 425–434. [Google Scholar] [CrossRef]
- Harkanen, M.; Voutilainen, A.; Turunen, E.; Vehvilainen-Julkunen, K. Systematic review and meta-analysis of educational interventions designed to improve medication administration skills and safety of registered nurses. Nurse Educ. Today 2016, 41, 36–43. [Google Scholar] [CrossRef]
- Aiken, L.H.; Patrician, P.A. Measuring organizational traits of hospitals: The Revised Nursing Work Index. Nurs Res. 2000, 49, 146–153. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Means Comparison | Applicability of Knowledge/Skills | Improvement of Knowledge/Skills i | Transmission of Knowledge/Skills | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Dimensions of Satisfaction | Likert | Response | Values | p Value | Likert | Response | Values | p Value | Likert | Response | Values | p Value |
| Course programme | 0–5 | No | 4.09 (1.41) | 0.013 | 0–5 | No | 3.64 (1.87) | 0.005 | 0–5 | No | 2.83 (1.72) | 0.000 |
| Yes | 4.76 (0.64) | Yes | 4.77 (0.55) | Yes | 4.75 (0.66) | |||||||
| Training methodology | 0–4 | No | 2.25 (0.50) | 0.154 | 0–4 | No | 2.67 (0.49) | 0.003 | 0–4 | No | 2.25 (0.50) | 0.003 |
| Yes | 3.11 (0.54) | Yes | 3.15 (0.52) | Yes | 3.15 (0.54) | |||||||
| Improvement of Professional Competence | 0–7 | No | 5.65 (1.37) | 0.000 | 0–7 | No | 4.69 (0.95) | 0.000 | 0–8 | No | 5.50 (2.07) | 0.007 |
| Yes | 6.67 (1.05) | Yes | 6.72 (1.05) | Yes | 7.70 (1.12) | |||||||
| Economic impact | 0–3 | No | 0.53 (1.01) | 0.001 | 0–2 | No | 0.20 (0.42) | 0.000 | 0–2 | No | 0.14 (0.38) | 0.001 |
| Yes | 1.33 (1.10) | Yes | 1.30 (1.11) | Yes | 1.34 (1.12) | |||||||
| Perceived Improvement in Quality of Health Care | Improvement of Knowledge/Skills | Total | |
| No | Yes | ||
| No | (4) | (3) | (7) |
| 28.60% | 2.00% | 4.30% | |
| Yes | (10) | (146) | (156) |
| 71.40% | 98% | 95.70% | |
| Total | (14) | (1.49) | (163) |
| 100% | 100% | 100% | |
| Perceived Improvement in Quality of Health Care | Applicability of Knowledge/Kills | Total | |
| No | Yes | ||
| No | (4) | (3) | (7) |
| 40.00% | 2.00% | 4.40% | |
| Yes | (6) | (147) | (153) |
| 60.00% | 98.00% | 95.60% | |
| Total | (10) | (150) | (160) |
| 100% | 100% | 100% | |
| Independent Variables | p Value | CRUDE OR (95% CI) | P | ADJUSTED OR (95% CI) |
|---|---|---|---|---|
| Satisfaction | 0.001 | 3.125 (1.602–6.095) | 0.329 | 1.772 (0.562–5.588) |
| Training methodology | 0.006 | 25.802 (2.588–257.268) | 0.034 | 16.479 (1.244–218.353) |
| Professional competence | 0.001 | 2.999 (1.603–5.612) | 0.874 | 0.916 (0.310–218.353) |
| Economic impact | 0.019 | 12.744 (1.524–106.544) | 0.161 | 7.174 (0.456–112.959) |
| Area Under Curve | 0.930 (0–1) | |||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gil-Lacruz, M.; Gracia-Pérez, M.L.; Gil-Lacruz, A.I. Learning by Doing and Training Satisfaction: An Evaluation by Health Care Professionals. Int. J. Environ. Res. Public Health 2019, 16, 1397. https://doi.org/10.3390/ijerph16081397
Gil-Lacruz M, Gracia-Pérez ML, Gil-Lacruz AI. Learning by Doing and Training Satisfaction: An Evaluation by Health Care Professionals. International Journal of Environmental Research and Public Health. 2019; 16(8):1397. https://doi.org/10.3390/ijerph16081397
Chicago/Turabian StyleGil-Lacruz, Marta, María Luisa Gracia-Pérez, and Ana Isabel Gil-Lacruz. 2019. "Learning by Doing and Training Satisfaction: An Evaluation by Health Care Professionals" International Journal of Environmental Research and Public Health 16, no. 8: 1397. https://doi.org/10.3390/ijerph16081397
APA StyleGil-Lacruz, M., Gracia-Pérez, M. L., & Gil-Lacruz, A. I. (2019). Learning by Doing and Training Satisfaction: An Evaluation by Health Care Professionals. International Journal of Environmental Research and Public Health, 16(8), 1397. https://doi.org/10.3390/ijerph16081397