Why I Can’t, Won’t or Don’t Test for HIV: Insights from Australian Migrants Born in Sub-Saharan Africa, Southeast Asia and Northeast Asia

 , and
, and 
Abstract
:1. Introduction
2. Methods
2.1. Research Team and Steering Group
2.2. Project Advisory Group
2.3. Focus Group Facilitators
2.4. Participant Eligibility and Recruitment
2.5. Study Setting
2.6. Methodology
2.7. Ethical Considerations
2.8. Focus Group Guide Development
2.9. Data Collection and Analysis
2.10. Demographics of Participants
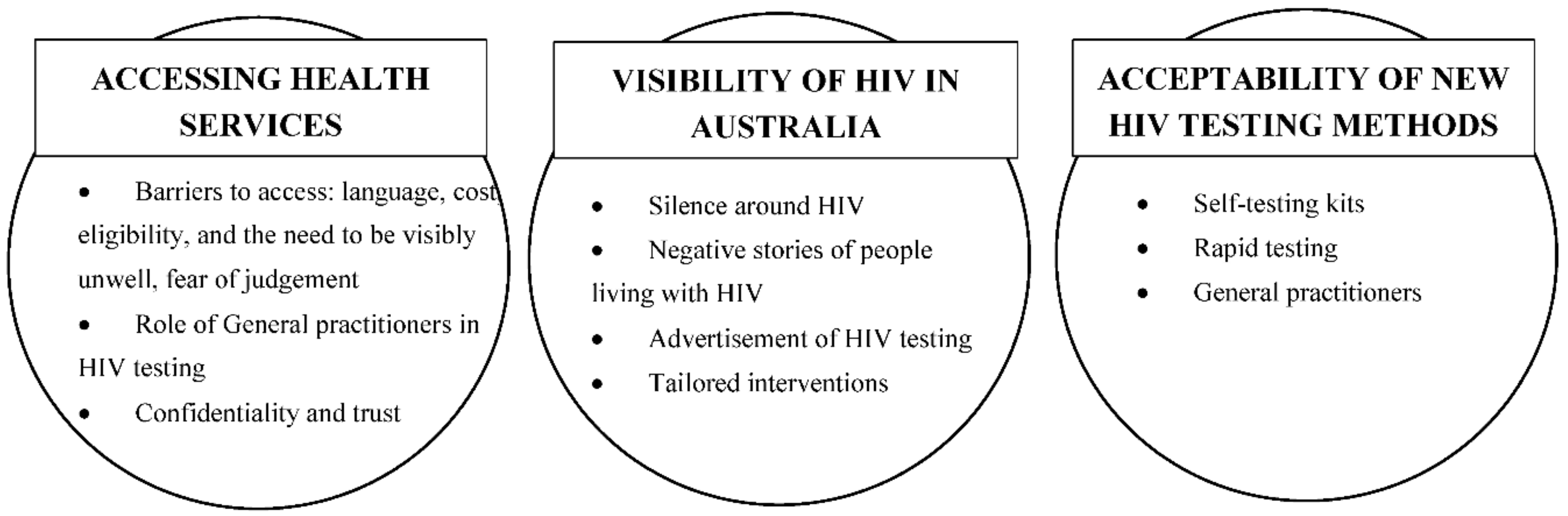
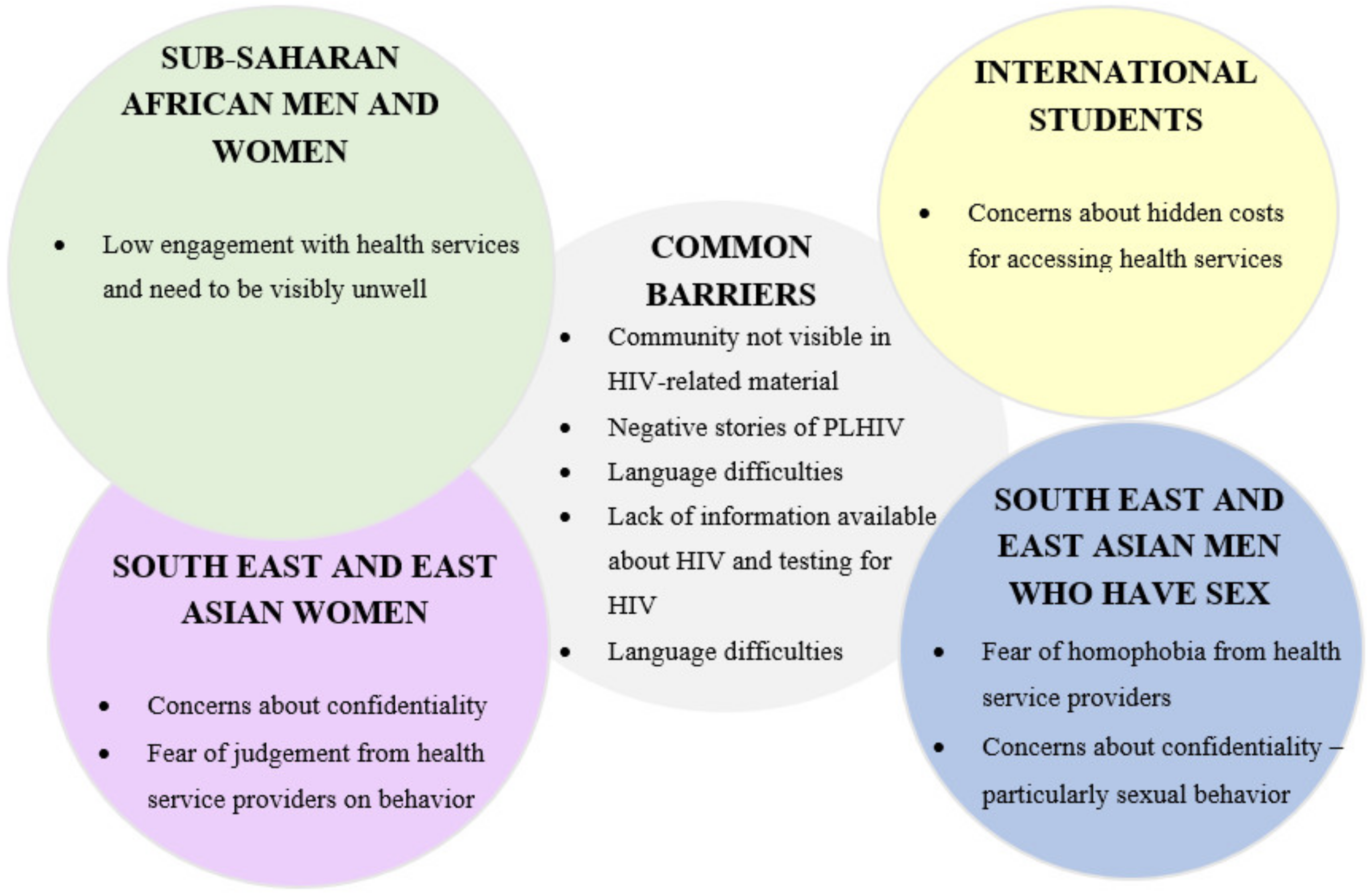
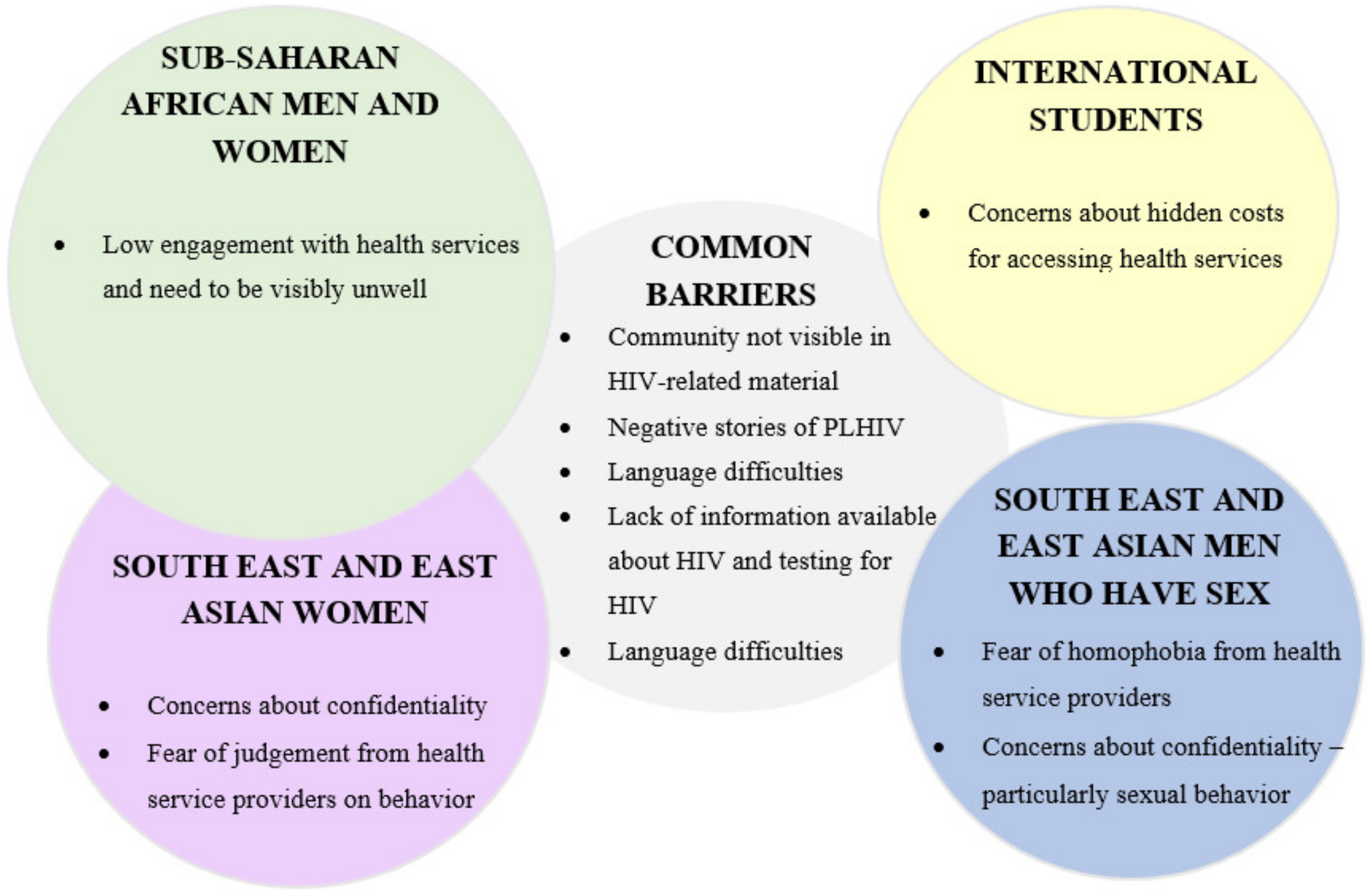
3. Results
3.1. Accessing Health Services
“I came here like four years ago, I’m a Chinese student, so I’ve only been to GP like once because it’s extremely expensive.”M, China (Asian MSM group, international student)
“…they are probably too professional … your thing (illness) is so pressing, but you still have to go through that process of making appointments, while you have to feel the pain.”M, Botswana (African mixed gender group, international student)
“… (I’m) here for ten years and I don’t have malaria or anything, I don’t go to a doctor. So this is a common thing with us (African men), you only see the doctor when you are sick.”M, South Sudan (African male group)
“We (have) been here, our generation over 6-10 years here and … we are still having language barriers that impacts mostly on those (sexual) health issues.”M, South Sudan (African male group)
3.1.1. Role of General Practitioners in HIV Testing
“…she (GP) doesn’t deem me to be in the high-risk category, but it would be nice to just have the (HIV) test done.”F, Malaysia (Asian female group)
“Because there is a certain judgement involved with the questions, your GP will (think) ‘Is she a slut? Is she a drug addict? How many men has she slept with?”F, Malaysia (Asian female group)
“(HIV is) seen as an African disease… you go to the hospital and you say ‘hey doc, I think I’ve got HIV’, they might judge you.”F, Kenya (African women’s group, international student)
3.1.2. Confidentiality and Trust
“…I had to hand over Medicare— would my parents be notified? Would they find out?... they say it’s anonymous, but they could track me, I just signed documents, my names on paper… it tells people I’m having sex (with men).”M, Indonesia (Asian MSM group)
3.2. Visibility of HIV in Australia
3.2.1. Negative Stories of HIV
“I remember one of my friends asked “so what if you find HIV positive, what do you do?”…“you get locked up, isolated areas” …you find you’re HIV positive, you get isolated, you don’t stay in the community, that’s what they say, you don’t see your family and stuff.”M, South Sudan (African male group)
3.2.2. Advertisement of HIV Testing
“Where do you test? …if I have problems, I see a physician here, I see a dentist….I haven’t seen any poster of HIV. No testing centres… nobody is dealing with the HIV.”M, Tanzania (African mixed gender group, international student)
“You can’t share it (HIV knowledge) as freely as back home. Because at home (Kenya)… there is free testing. It’s unacceptable (that) in Australia it’s not free… when you google “free (sexually transmitted infections) places to test in Australia” it only brings up two tests—that’s gonorrhea and chlamydia.”F, Kenya (African women’s group)
3.2.3. Tailored Interventions
“(We need) something about us, not about them (gay man).”—F, Africa (African mixed gender group)
“I think the international people they, they are quite lost in the message of HIV; it’s more Australian people.”M, China (Asian MSM group)
“They (community outsiders) just come in with a PowerPoint… it would be good to have more employed staff from similar cultures because they would understand how to communicate the message.”F, Africa (SSA mixed gender group)
3.3. Acceptability of New HIV Testing Methods
“I didn’t even know you could go to the GP to test these things (HIV)… I’m thirty years old, and I didn’t even know this—it’s something so basic.”M, Indonesia (Asian MSM group)
3.3.1. Self-Testing Kits
“…I do it myself, after testing I am positive, what do I do? What is the next step?”F, Botswana (African mixed gender group)
“I think most Chinese, especially gay people, prefer buying (a) HIV kit from the internet—it’s very convenient in China and it protects your privacy to some extent… and I will know the result in just two or three minutes.”M, China (Asian MSM group)
“Myself, I prefer home testing because (I am) scared of telling GP (about sexual behavior) and would die of embarrassment.”M, South Sudan (African male group)
“But I reckon it would take a lot of blood from the body every 3 months, sometimes they take like two syringes worth.”M, Asia (Asian MSM group)
3.3.2. Rapid Testing
“(I) kind of, regret to take the (venipuncture HIV) test. ‘Oh my god why do I have to suffer like this?’ I want the rapid test, I want to make it fast especially if that’s my first test… I think about the different people I’ve been with over the seven days … ‘Am I positive, am I negative’ … (it) wasn’t a good (experience) for me.”M, Asia (Asian MSM group)
3.3.3. General Practitioners
“(A) routine blood test… HIV (test) for general overall health, you know with blood pressure, cholesterol, the diabetes, the heart disease… it’s better us taking control over our own health… and then the HIV blood test becomes part of that as well.”F, Africa (African mixed gender group)
4. Discussion
4.1. Overview of Findings
4.2. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- United Nations. International Migration Report 2017 (ST/ESA/SER.A/403); United Nations: New York, NY, USA, 2017. [Google Scholar]
- Australian Bureau of Statistics. 3412.0 - Migration, Australia, 2015-16. Available online: http://www.abs.gov.au/ausstats/abs@.nsf/mf/3412.0/ (accessed on 14 June 2018).
- Stewart, D.E.; Do, B.N. Health needs of migrant Vietnamese women in south-west Brisbane: An exploratory study. Aust. J. Soc. Issues 2003, 38, 247–261. [Google Scholar] [CrossRef]
- Mengesha, Z.B.; Perz, J.; Dune, T.; Ussher, J. Refugee and migrant women’s engagement with sexual and reproductive health care in Australia: A socio-ecological analysis of health care professional perspectives. PLoS ONE 2017, 12, e0181421. [Google Scholar] [CrossRef] [PubMed]
- Ross, J.; Cunningham, C.O.; Hanna, D.B. HIV outcomes among migrants from low-income and middle-income countries living in high-income countries: A review of recent evidence. Curr. Opin. Infect. Dis. 2018, 31, 25–32. [Google Scholar] [CrossRef] [PubMed]
- The Kirby Institute. HIV, viral hepatitis and sexually transmissible infections in Australia: Annual Surveillance Report 2018; Kirby Institute, UNSW Sydney: Sydney, NSW, Australia, 2018. [Google Scholar]
- Department of Health Australian Government. Seventh National HIV Strategy 2014 - 2017; Commonwealth of Australia: Canberra, ACT, Australia, 2014.
- Crawford, G.; Lobo, R.; Brown, G.; Langdon, P. HIV and Mobility in Australia: Road Map for Action; Western Australian Centre for Health Promotion Research and Australian Research Centre in Sex, Health and Society: Perth, WA, Australia, 2014. [Google Scholar]
- Gray, C.; Crawford, G.; Reid, A.; Lobo, R. HIV knowledge and use of health services among people from South East Asia and sub-Saharan Africa living in Western Australia. Health Promot. J. Aust. 2018, 29, 274. [Google Scholar] [CrossRef]
- Crawford, G.; Lobo, R.; Brown, G.; Macri, C.; Smith, H.; Maycock, B. HIV, Other Blood-Borne Viruses and Sexually Transmitted Infections amongst Expatriates and Travellers to Low-and Middle-Income Countries: A Systematic Review. Int. J. Environ. Res. Public Health 2016, 13, 1249. [Google Scholar] [CrossRef]
- Crawford, G.; Lobo, R.; Brown, G.; Maycock, B. The influence of population mobility on changing patterns of HIV acquisition: Lessons for and from Australia. Health Promot. J. Aust. 2016, 27, 153–154. [Google Scholar] [CrossRef] [PubMed]
- Agu, J.; Lobo, R.; Crawford, G.; Chigwada, B. Migrant Sexual Health Help-Seeking and Experiences of Stigmatization and Discrimination in Perth, Western Australia: Exploring Barriers and Enablers. Int. J. Environ. Res. Public Health 2016, 13, 485. [Google Scholar] [CrossRef] [PubMed]
- Rade, D.; Crawford, G.; Lobo, R.; Gray, C.; Brown, G. Sexual Health Help-Seeking Behavior among Migrants from Sub-Saharan Africa and South East Asia living in High Income Countries: A Systematic Review. Int. J. Environ. Res. Public Health 2018, 15, 1311. [Google Scholar] [CrossRef]
- Drummond, P.D.; Mizan, A.; Brocx, K.; Wright, B. Barriers to accessing health care services for West African refugee women living in Western Australia. Healthc. Women Int. 2011, 32, 206–224. [Google Scholar] [CrossRef] [PubMed]
- Drummond, P.D.; Mizan, A.; Wright, B. HIV/AIDS knowledge and attitudes among West African immigrant women in Western Australia. Sex. Health 2008, 5, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Korner, H. Late HIV diagnosis of people from culturally and linguistically diverse backgrounds in Sydney: The role of culture and community. AIDS Care 2007, 19, 168–178. [Google Scholar] [CrossRef]
- Åkerman, E.; Essén, B.; Westerling, R.; Larsson, E. Healthcare-seeking behaviour in relation to sexual and reproductive health among Thai-born women in Sweden: A qualitative study. Cult. Health Sex. 2017, 19, 194–207. [Google Scholar] [CrossRef]
- Thomas, F.; Aggleton, P.; Anderson, J. “If I cannot access services, then there is no reason for me to test”: The impacts of health service charges on HIV testing and treatment amongst migrants in England. AIDS Care 2010, 22, 526–531. [Google Scholar] [CrossRef]
- Korner, H. ‘If I had my residency I wouldn’t worry’: Negotiating migration and HIV in Sydney, Australia. Ethn. Health 2007, 12, 205–225. [Google Scholar] [CrossRef]
- Lindkvist, P.; Johansson, E.; Hylander, I. Fogging the issue of HIV - Barriers for HIV testing in a migrated population from Ethiopia and Eritrea. BMC Public Health 2015, 15. [Google Scholar] [CrossRef] [PubMed]
- McMichael, C.; Gifford, S. “It is good to know now...before it‘s too late“: Promoting sexual health literacy amongst resettled young people with refugee backgrounds. Sex. Cult. Interdiscip. Q. 2009, 13, 218–236. [Google Scholar] [CrossRef]
- Manirankunda, L.; Loos, J.; Alou, T.A.; Colebunders, R.; Nöstlinger, C. “It’s better not to know“: Perceived barriers to HIV voluntary counseling and testing among sub-Saharan African migrants in Belgium. Aids Educ. Prev. 2009, 21, 582–593. [Google Scholar] [CrossRef] [PubMed]
- Adedimeji, A.A.; Asibon, A.; O’Connor, G.; Carson, R.; Cowan, E.; McKinley, P.; Leider, J.; Mallon, P.; Calderon, Y. Increasing HIV testing among African immigrants in ireland: Challenges and opportunities. J. Immigr. Minor. Health 2015, 17, 89–95. [Google Scholar] [CrossRef]
- Ussher, J.M.; Rhyder-Obid, M.; Perz, J.; Rae, M.; Wong, T.W.; Newman, P. Purity, privacy and procreation: Constructions and experiences of sexual and reproductive health in Assyrian and Karen women living in Australia. Sex. Cult. Interdiscip. Q. 2012, 16, 467–485. [Google Scholar] [CrossRef]
- Blondell, S.J.; Kitter, B.; Griffin, M.P.; Durham, J. Barriers and Facilitators to HIV Testing in Migrants in High-Income Countries: A Systematic Review. AIDS Behav. 2015, 19, 2012–2024. [Google Scholar] [CrossRef]
- McGregor, S.; Mlambo, E.; Gunaratnam, P.; Wilson, D.; Guy, R. HIV knowledge, Risk Behaviour and Testing: A community Survey in People from Culturally and Linguistically Diverse (CALD) Backgrounds in NSW, Australia; The Kirby Institute, UNSW Sydney: Sydney, NSW, Australia, 2017. [Google Scholar]
- National HIV Testing Policy Expert Reference Committee. National HIV Testing Policy, 2011; Department of Health and Ageing: Canberra, ACT, Australia, 2011. [Google Scholar]
- Chen, M.Y.; Bilardi, J.E.; Lee, D.; Cummings, R.; Bush, M.; Fairley, C.K. Australian men who have sex with men prefer rapid oral HIV testing over conventional blood testing for HIV. Int. J. Std. AIDS 2010, 21, 428–430. [Google Scholar] [CrossRef]
- Conway, D.P.; Guy, R.; Davies, S.C.; Couldwell, D.L.; McNulty, A.; Smith, D.E.; Keen, P.; Cunningham, P.; Holt, M. Rapid HIV testing is highly acceptable and preferred among high-risk gay and bisexual men after implementation in Sydney sexual health clinics. PLoS ONE 2015, 10, e0123814. [Google Scholar] [CrossRef]
- Chan, D.; Stewart, M.; Smith, M.; Price, T.; Lusk, J.; Ooi, C.; Read, P.; Finlayson, R. The rise of targeted HIV oral rapid testing in Australia. Med. J. Aust. 2015, 202, 251–255. [Google Scholar] [CrossRef] [PubMed]
- Australian Federation of AIDS Organisations. Getting tested for HIV. Available online: https://www.afao.org.au/about-hiv/getting-tested-for-hiv/ (accessed on 14 February 2019).
- Bilardi, J.E.; Walker, S.; Read, T.; Prestage, G.; Chen, M.Y.; Guy, R.; Bradshaw, C.; Fairley, C.K. Gay and Bisexual Men’s Views on Rapid Self-Testing for HIV. AIDS Behav. 2013, 17, 2093–2099. [Google Scholar] [CrossRef] [PubMed]
- Jamil, M.S.; Prestage, G.; Fairley, C.K.; Grulich, A.E.; Smith, K.S.; Chen, M.; Holt, M.; McNulty, A.M.; Bavinton, B.R.; Conway, D.P.; et al. Effect of availability of HIV self-testing on HIV testing frequency in gay and bisexual men at high risk of infection (FORTH): A waiting-list randomised controlled trial. Lancet HIV 2017, 4, e241–e250. [Google Scholar] [CrossRef]
- Driver, G.; Debattista, J.; Gu, Z.; Lemoire, J.; Hooper, J. HIV testing within the African community using home-based self collection of oral samples. Aust. N. Z. J. Public Health 2017, 44, 446. [Google Scholar] [CrossRef] [PubMed]
- Collaboration for Evidence Research and Impact in Public Health. “I Want to Test but I’m Afraid”: Barriers to HIV Testing among People Born in South East Asia and Sub-Saharan Africa: Final Report; Curtin University: Perth, WA, Australia, 2018. [Google Scholar]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Healthc. 2007, 19, 349–357. [Google Scholar] [CrossRef]
- Halcomb, E.J.; Gholizadeh, L.; DiGiacomo, M.; Phillips, J.; Davidson, P.M. Literature review: Considerations in undertaking focus group research with culturally and linguistically diverse groups. J. Clin. Nurs. 2007, 16, 1000–1011. [Google Scholar] [CrossRef] [PubMed]
- Liamputtong, P. Doing Research in a Cross-Cultural Context: Methodological and Ethical Challenges. In Doing Cross-Cultural Research: Ethical and Methodological Perspectives; Liamputtong, P., Ed.; Springer: Dordrecht, The Netherlands, 2008; pp. 3–20. [Google Scholar]
- Adamson, J.; Donovan, J.L. Research in Black and White. Qual. Health Res. 2002, 12, 816–825. [Google Scholar] [CrossRef]
- Palmer, M.; Larkin, M.; de Visser, R.; Fadden, G. Developing an Interpretative Phenomenological Approach to Focus Group Data. Qual. Res. Psychol. 2010, 7, 99–121. [Google Scholar] [CrossRef]
- Smith, J.A.; Osborn, M. Interpretative phenomenological analysis. Doing Soc. Psychol. Res. 2004, 229–254. [Google Scholar] [CrossRef]
- Husserl, E. Ideas Pertaining to a Pure Phenomenology and to a Phenomenological Philosophy: Second Book Studies in the Phenomenology of Constitution; Springer Science & Business Media: Berlin, Germany, 1990. [Google Scholar]
- Kuljit, H.; Michael, L.; Ivan, B.; John, R. The cultural context of care-giving: Qualitative accounts from South Asian parents who care for a child with intellectual disabilities in the UK. Adv. Ment. Health Intellect. Disabil. 2012, 6, 179–191. [Google Scholar] [CrossRef]
- Walls, J.K.; Hall, S.S. A focus group study of African American students’ experiences with classroom discussions about race at a predominantly White university. Teach. High. Educ. 2017, 1–16. [Google Scholar] [CrossRef]
- Cox, C.M.; Babalola, S.; Kennedy, C.E.; Mbwambo, J.; Likindikoki, S.; Kerrigan, D. Determinants of concurrent sexual partnerships within stable relationships: A qualitative study in Tanzania. BMJ Open 2014, 4, e003680. [Google Scholar] [CrossRef] [PubMed]
- Culley, L.; Hudson, N.; Rapport, F. Using focus groups with minority ethnic communities: Researching infertility in British South Asian communities. Qual. Health Res. 2007, 17, 102–112. [Google Scholar] [CrossRef] [PubMed]
- Dias, S.; Gama, A.; Rocha, C. Immigrant women’s perceptions and experiences of health care services: Insights from a focus group study. J. Public Health 2010, 18, 489–496. [Google Scholar] [CrossRef]
- Colucci, E. On the Use of Focus Groups in Cross-Cultural Research. In Doing Cross-Cultural Research: Ethical and Methodological Perspectives; Liamputtong, P., Ed.; Springer: Dordrecht, The Netherlands, 2008; pp. 233–252. [Google Scholar]
- National Health and Medical Research Council. National Statement on Ethical Conduct in Human Research (2007). Available online: https://www.nhmrc.gov.au/guidelines-publications/e72 (accessed on 20 March 2019).
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Brocki, J.M.; Wearden, A.J. A critical evaluation of the use of interpretative phenomenological analysis (IPA) in health psychology. Psychol. Health 2006, 21, 87–108. [Google Scholar] [CrossRef]
- QSR International Pty Ltd. Vivo Qualitative Data Analysis Software. Version 11; QSR International Pty Ltd.: Melbourne, VIC, Australia, 2016. [Google Scholar]
- Morse, J.M.; Barrett, M.; Mayan, M.; Olson, K.; Spiers, J. Verification Strategies for Establishing Reliability and Validity in Qualitative Research. Int. J. Qual. Methods 2002, 1, 13–22. [Google Scholar] [CrossRef]
- Noble, H.; Smith, J. Issues of validity and reliability in qualitative research. Evid. Based Nurs. 2015, 18, 34–35. [Google Scholar] [CrossRef]
- Shangase, P.; Egbe, C.O. Barriers to Accessing HIV Services for Black African Communities in Cambridgeshire, the United Kingdom. J. Community Health 2014, 40, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Bova, C.; Nnaji, C.; Woyah, A.; Duah, A. HIV Stigma, Testing Attitudes and Health Care Access Among African-Born Men Living in the United States. J. Immigr. Minority Health 2016, 18, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Deblonde, J.; De Koker, P.; Hamers, F.F.; Fontaine, J.; Luchters, S.; Marleen, T. Barriers to HIV testing in Europe: A systematic review. Eur. J. Public Health 2010, 20, 422–432. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-del Arco, D.; Monge, S.; Azcoaga, A.; Rio, I.; Hernando, V.; Gonzalez, C.; Alejos, B.; Caro, A.M.; Perez-Cachafeiro, S.; Ramirez-Rubio, O. HIV testing and counselling for migrant populations living in high-income countries: A systematic review. Eur. Public Health 2013, 26, 1039–1045. [Google Scholar] [CrossRef]
- Mengesha, Z.B.; Dune, T.; Perz, J. Culturally and linguistically diverse women’s views and experiences of accessing sexual and reproductive health care in Australia: A systematic review. Sex. Health 2016, 13, 299–310. [Google Scholar] [CrossRef] [PubMed]
- Aung, E.; Blondell, S.J.; Durham, J. Interventions for Increasing HIV Testing Uptake in Migrants: A Systematic Review of Evidence. AIDS Behav. 2017. [Google Scholar] [CrossRef] [PubMed]
- Stangl, A.L.; Lloyd, J.K.; Brady, L.M.; Holland, C.E.; Baral, S. A systematic review of interventions to reduce HIV-related stigma and discrimination from 2002 to 2013: How far have we come? J. Int. Aids Soc. 2013, 16, 18734. [Google Scholar] [CrossRef] [PubMed]
- Dean, J.; Mitchell, M.; Stewart, D.; Debattista, J. Sexual health knowledge and behaviour of young Sudanese Queenslanders: a cross-sectional study. Sex. Health 2017. [Google Scholar] [CrossRef] [PubMed]
- Rogers, C.; Earnest, J. A cross-generational study of contraception and reproductive health among Sudanese and Eritrean women in Brisbane, Australia. Healthc. Women Int. 2014, 35, 334–356. [Google Scholar] [CrossRef] [PubMed]
- Mullens, A.B.; Kelly, J.; Debattista, J.; Phillips, T.M.; Gu, Z.; Siggins, F. Exploring HIV risks, testing and prevention among sub-Saharan African community members in Australia. Int. J. Equity Health 2018, 17, 62. [Google Scholar] [CrossRef] [PubMed]
- Viruell-Fuentes, E.A.; Miranda, P.Y.; Abdulrahim, S. More than culture: Structural racism, intersectionality theory, and immigrant health. Soc. Sci. Med. 2012, 75, 2099–2106. [Google Scholar] [CrossRef] [PubMed]
- Persson, A.; Newman, C. Making monsters: Heterosexuality, crime and race in recent Western media coverage of HIV. Sociol. Health Illn. 2008, 30, 632–646. [Google Scholar] [CrossRef]
- Byrne, E. Godfrey Zaburoni, who infected partner with HIV, has conviction quashed by High Court. ABC News, 6 April 2016. [Google Scholar]
- Ogilvie, L.D.; Burgess-Pinto, E.; Caufield, C. Challenges and approaches to newcomer health research. J. Transcult. Nurs. 2008, 19, 64–73. [Google Scholar] [CrossRef]
- Laverack, G. ‘Leaving No One Behind’: The Challenge of Reaching Migrant Populations. Challenges 2018, 9, 37. [Google Scholar] [CrossRef]
- Hulse, G.K. Australia’s public health response to HIV and HCV: A role for ‘affected’ communities. Drug Alcohol Rev. 1997, 16, 171–176. [Google Scholar] [CrossRef]
- Australian Federation of AIDS Organisations. HIV and Stigma in Australia: A Guide for Religious Leaders; AFAO: Sydney, NSW, Australia, 2014. [Google Scholar]
- Navarro, M.; Navaza, B.; Guionnet, A.; López-Vélez, R. Overcoming Barriers to HIV Prevention and Healthcare Among Sub-Saharan African Migrants in Spain. JMIR Public Health Surveill. 2018, 4. [Google Scholar] [CrossRef]
- Newman, C.E.; Kidd, M.R.; Kippax, S.C.; Reynolds, R.H.; Canavan, P.G.; de Wit, J.B.F. Engaging nonHIV specialist general practitioners with new priorities in HIV prevention and treatment: Qualitative insights from those working in the field. Sex. Health 2013, 10, 193–198. [Google Scholar] [CrossRef]
- Australasian Society for HIV, Viral Hepatitis and Sexual Health. HIV Training. Available online: https://www.ashm.org.au/HIV/training/ (accessed on 19 June 2018).
- Mutch, A.J.; Lui, C.W.; Dean, J.; Mao, L.; Lemoire, J.; Debattista, J.; Howard, C.; Whittaker, A.; Fitzgerald, L. Increasing HIV testing among hard-to-reach groups: Examination of RAPID, a community-based testing service in Queensland, Australia. BMC Health Serv. Res. 2017, 17, 310. [Google Scholar] [CrossRef] [PubMed]
- Hollander, J.A. The Social Contexts of Focus Groups. J. Contemp. Ethnogr. 2004, 33, 602–637. [Google Scholar] [CrossRef]
- Gabriel, P.; Kaczorowski, J.; Berry, N. Recruitment of Refugees for Health Research: A qualitative study to add refugees’ perspectives. Int. J. Environ. Res. Public Health 2017, 14, 125. [Google Scholar] [CrossRef] [PubMed]
- Eklöf, N.; Hupli, M.; Leino-Kilpi, H. Planning focus group interviews with asylum seekers: Factors related to the researcher, interpreter and asylum seekers. Nurs. Inq. 2017, 24, e12192. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Characteristics | Number of Participants | ||
|---|---|---|---|
| Sub-Saharan Africa (n = 35) | Southeast Asia and Northeast Asia (n = 42) | All Participants (n = 77) | |
| Sex * | |||
| Male | 12 | 19 | 31 (40%) |
| Female | 22 | 23 | 45 (60%) |
| Age ** (years) | |||
| 18–24 | 6 | 5 | 11 (15%) |
| 25–29 | 2 | 22 | 24 (32%) |
| 30–34 | 6 | 7 | 13 (18%) |
| 35–39 | 3 | 4 | 7 (9%) |
| 40–44 | 7 | 2 | 9 (12%) |
| 45+ | 11 | 2 | 13 (18%) |
| Years lived in Australia | |||
| <1 year | 6 | 11 | 17 (22%) |
| 1–5 years | 6 | 15 | 21 (27%) |
| 6–10 years | 3 | 8 | 11 (14%) |
| >10 years | 20 | 8 | 28 (36%) |
| Status in Australia *** | |||
| Citizen | 23 | 9 | 32 (43%) |
| Permanent resident | 4 | 6 | 10 (13%) |
| Student visa | 6 | 22 | 29 (39%) |
| Other temporary visa | 0 | 5 | 5 (7%) |
| Education Level **** | |||
| Primary school | 4 | 0 | 4 (5%) |
| High school | 6 | 1 | 7 (9%) |
| Year 12 or equivalent | 4 | 2 | 6 (8%) |
| TAFE certificate/diploma | 4 | 2 | 6 (8%) |
| University postgraduate degree or higher | 15 | 37 | 52 (69%) |
| Sexual identity ***** | |||
| Heterosexual | 18 | 21 | 39 (54%) |
| Homosexual | 1 | 17 | 18 (25%) |
| Bisexual | 0 | 2 | 2 |
| Pansexual | 0 | 1 | 1 |
| Other (not disclosed) | 4 | 1 | 5 (7%) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gray, C.; Lobo, R.; Narciso, L.; Oudih, E.; Gunaratnam, P.; Thorpe, R.; Crawford, G. Why I Can’t, Won’t or Don’t Test for HIV: Insights from Australian Migrants Born in Sub-Saharan Africa, Southeast Asia and Northeast Asia. Int. J. Environ. Res. Public Health 2019, 16, 1034. https://doi.org/10.3390/ijerph16061034
Gray C, Lobo R, Narciso L, Oudih E, Gunaratnam P, Thorpe R, Crawford G. Why I Can’t, Won’t or Don’t Test for HIV: Insights from Australian Migrants Born in Sub-Saharan Africa, Southeast Asia and Northeast Asia. International Journal of Environmental Research and Public Health. 2019; 16(6):1034. https://doi.org/10.3390/ijerph16061034
Chicago/Turabian StyleGray, Corie, Roanna Lobo, Lea Narciso, Enaam Oudih, Praveena Gunaratnam, Rachel Thorpe, and Gemma Crawford. 2019. "Why I Can’t, Won’t or Don’t Test for HIV: Insights from Australian Migrants Born in Sub-Saharan Africa, Southeast Asia and Northeast Asia" International Journal of Environmental Research and Public Health 16, no. 6: 1034. https://doi.org/10.3390/ijerph16061034
APA StyleGray, C., Lobo, R., Narciso, L., Oudih, E., Gunaratnam, P., Thorpe, R., & Crawford, G. (2019). Why I Can’t, Won’t or Don’t Test for HIV: Insights from Australian Migrants Born in Sub-Saharan Africa, Southeast Asia and Northeast Asia. International Journal of Environmental Research and Public Health, 16(6), 1034. https://doi.org/10.3390/ijerph16061034