Prevention of Cardiovascular Disease and Cancer Mortality by Achieving Healthy Dietary Goals for the Swedish Population: A Macro-Simulation Modelling Study

 ,
,
Abstract
1. Introduction
2. Materials and Methods
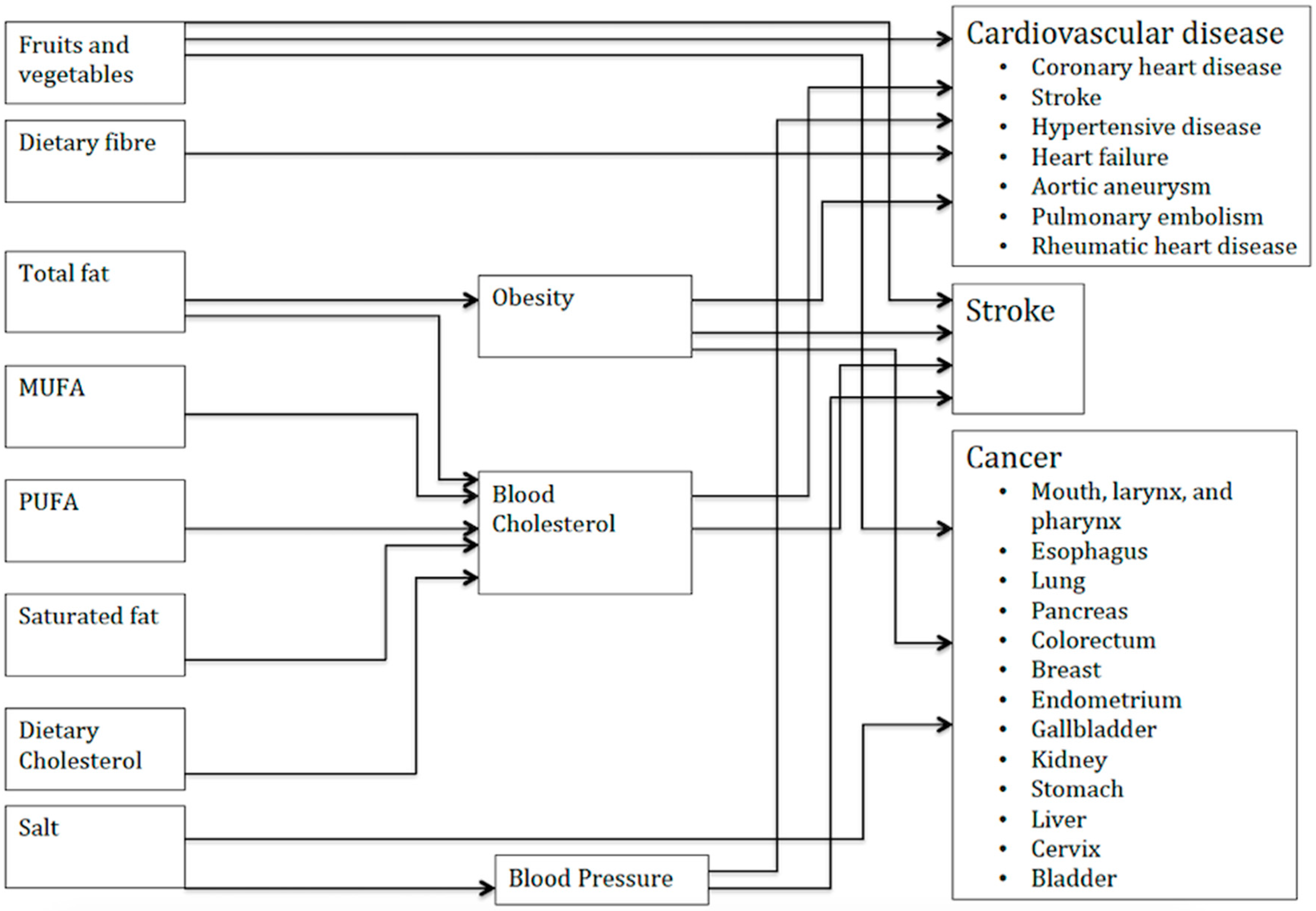
2.1. The Simulation Model
- Combined changes in the risks for individuals are multiplicative. For example, if one extra serving of vegetables reduces the risk of cardiovascular diseases by 12% and reducing salt intake by 1 gram per day reduces the risk by 10%, then both of these behaviour changes jointly reduce the risk of cardio-vascular disease (CVD) death by 20.8% (1 − (1 − 0.12) × (1 − 0.10)).
- Changes in risk follow a log-linear, dose-response relationship except for obesity, which follows a J-shaped curve. For example, a change in consumptions of fruits and vegetables from 2 to 3 servings has the same effect on relative risk as a change in consumption from 7 to 8 servings. However, an upper threshold has been included, above which there are no additional health benefits. The upper thresholds are based on the range of data collected in the meta-analyses used to parameterise the models. It is unlikely that the effects of different food components are independent and additive. By combining parameters multiplicatively, the PRIME model estimates the overlap in estimated changes in risk of cause-specific mortality as they relate to changes in different dietary components (i.e., the outcome of changing several dietary components simultaneously is less than the sum of its parts and can never exceed 100% risk reduction).
2.2. Actual Intake
2.3. Recommended Intake
2.4. Population Statistics
2.5. Uncertainty Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Mithril, C.; Dragsted, L.O.; Meyer, C.; Blauert, E.; Holt, M.K.; Astrup, A. Guidelines for the new Nordic diet. Public Health Nutr. 2012, 15, 1941–1947. [Google Scholar] [CrossRef] [PubMed]
- Becker, W. Dietary guidelines and patterns of food and nutrient intake in Sweden. Br. J. Nutr. 1999, 81 (Suppl. S1), S113–S117. [Google Scholar] [CrossRef]
- Livsmedelsverket [National Food Agency, Sweden]. Vad äter Svenskarna? Livsmedels-Och Näringsintag Bland Vuxna i Sverige; Livsmedelsverket: Uppsala, Sweden, 2012.
- Jordbruksverket [The Swedish Board of Agriculture]. Livsmedelskonsumtionen i Siffror– Hur Har Konsumtionen Utvecklats de Senaste Femtio åren Och Varför? Jordbruksverket: Jönköping, Sweden, 2015.
- Mozaffarian, D. Dietary and Policy Priorities for Cardiovascular Disease, Diabetes, and Obesity: A Comprehensive Review. Circulation 2016, 133, 187–225. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Bella, F.; Godos, J.; Sciacca, S.; Del Rio, D.; Ray, S.; Galvano, F.; Giovannucci, E.L. Possible role of diet in cancer: Systematic review and multiple meta-analyses of dietary patterns, lifestyle factors, and cancer risk. Nutr. Rev. 2017, 75, 405–419. [Google Scholar] [CrossRef] [PubMed]
- Doll, R. Chronic and degenerative disease: Major causes of morbidity and death. Am. J. Clin. Nutr. 1995, 62, 1301S–1305S. [Google Scholar] [CrossRef] [PubMed]
- Beaglehole, R.; Bonita, R.; Horton, R.; Adams, C.; Alleyne, G.; Asaria, P.; Baugh, V.; Bekedam, H.; Billo, N.; Casswell, S. Priority actions for the non-communicable disease crisis. Lancet 2011, 377, 1438–1447. [Google Scholar] [CrossRef]
- Di Cesare, M.; Khang, Y.-H.; Asaria, P.; Blakely, T.; Cowan, M.J.; Farzadfar, F.; Guerrero, R.; Ikeda, N.; Kyobutungi, C.; Msyamboza, K.P.; et al. Inequalities in non-communicable diseases and effective responses. Lancet 2013, 381, 585–597. [Google Scholar] [CrossRef]
- Odegaard, K.; Borg, S.; Persson, U.; Svensson, M. The Swedish cost burden of overweight and obesity–evaluated with the PAR approach and a statistical modelling approach. Int. J. Pediatr. Obes. 2008, 3 (Suppl. 1), 51–57. [Google Scholar] [CrossRef]
- Sanson-Fisher, R.W.; Bonevski, B.; Green, L.W.; D’Este, C. Limitations of the Randomized Controlled Trial in Evaluating Population-Based Health Interventions. Am. J. Prev. Med. 2007, 33, 155–161. [Google Scholar] [CrossRef]
- Fone, D.; Hollinghurst, S.; Temple, M.; Round, A.; Lester, N.; Weightman, A.; Roberts, K.; Coyle, E.; Bevan, G.; Palmer, S. Systematic review of the use and value of computer simulation modelling in population health and health care delivery. J. Public Health 2003, 25, 325–335. [Google Scholar] [CrossRef]
- Homer, J.B.; Hirsch, G.B. System dynamics modeling for public health: Background and opportunities. Am. J. Public Health 2006, 96, 452–458. [Google Scholar] [CrossRef]
- Sun, X.; Faunce, T. Decision-analytical modelling in health-care economic evaluations. Eur. J. Health Econom. 2008, 9, 313–323. [Google Scholar] [CrossRef]
- Scarborough, P.; Harrington, R.A.; Mizdrak, A.; Zhou, L.M.; Doherty, A. The Preventable Risk Integrated ModEl and Its Use to Estimate the Health Impact of Public Health Policy Scenarios. Scientifica 2014, 2014, 21. [Google Scholar] [CrossRef]
- Scarborough, P.; Nnoaham, K.E.; Clarke, D.; Capewell, S.; Rayner, M. Modelling the impact of a healthy diet on cardiovascular disease and cancer mortality. J. Epidemiol. Community Health 2012, 66, 420–426. [Google Scholar] [CrossRef]
- Bélanger, M.; Poirier, M.; Jbilou, J.; Scarborough, P. Modelling the impact of compliance with dietary recommendations on cancer and cardiovascular disease mortality in Canada. Public Health 2014, 128, 222–230. [Google Scholar] [CrossRef]
- Irz, X.; Leroy, P.; Réquillart, V.; Soler, L.-G. Economic assessment of nutritional recommendations. J. Health Econom. 2015, 39, 188–210. [Google Scholar] [CrossRef]
- Norden. Nordic Nutrition Recommendations 2012. Part 1: Summary, Principles and Use; Nordic Council of Ministers: Copenhagen, Denmark, 2014. [Google Scholar]
- Livsmedelsverket [National Food Agency, Sweden]. Find Your Way to Eat Greener, Not Too Much and Be Active. Available online: http://www.livsmedelsverket.se/globalassets/english/food-habits-health-environment/dietary-guidelines/kostraden-eng-a4-utskriftversion.pdf?id=8199 (accessed on 28 January 2019).
- McKee, L.H.; Latner, T.A. Underutilized sources of dietary fiber: A review. Plant Foods Hum. Nutr. 2000, 55, 285–304. [Google Scholar] [CrossRef]
- Hendriksen, M.A.; van Raaij, J.M.; Geleijnse, J.M.; Breda, J.; Boshuizen, H.C. Health gain by salt reduction in europe: A modelling study. PLoS ONE 2015, 10, e0118873. [Google Scholar] [CrossRef]
- Sjogren, P.; Becker, W.; Warensjo, E.; Olsson, E.; Byberg, L.; Gustafsson, I.B.; Karlstrom, B.; Cederholm, T. Mediterranean and carbohydrate-restricted diets and mortality among elderly men: A cohort study in Sweden. Am. J. Clin. Nutr. 2010, 92, 967–974. [Google Scholar] [CrossRef]
- Sofi, F.; Macchi, C.; Abbate, R.; Gensini, G.F.; Casini, A. Mediterranean diet and health status: An updated meta-analysis and a proposal for a literature-based adherence score. Public Health Nutr. 2014, 17, 2769–2782. [Google Scholar] [CrossRef]
- Scarborough, P.; Morgan, R.D.; Webster, P.; Rayner, M. Differences in coronary heart disease, stroke and cancer mortality rates between England, Wales, Scotland and Northern Ireland: The role of diet and nutrition. BMJ Open 2011, 1, e000263. [Google Scholar] [CrossRef] [PubMed]
- Roswall, N.; Sandin, S.; Löf, M.; Skeie, G.; Olsen, A.; Adami, H.-O.; Weiderpass, E. Adherence to the healthy Nordic food index and total and cause-specific mortality among Swedish women. Eur. J. Epidemiol. 2015, 30, 509–517. [Google Scholar] [CrossRef] [PubMed]
- Ni Mhurchu, C.; Eyles, H.; Genc, M.; Scarborough, P.; Rayner, M.; Mizdrak, A.; Nnoaham, K.; Blakely, T. Effects of Health-Related Food Taxes and Subsidies on Mortality from Diet-Related Disease in New Zealand: An Econometric-Epidemiologic Modelling Study. PLoS ONE 2015, 10, e0128477. [Google Scholar] [CrossRef] [PubMed]
- Ludvigsson, J.; Otterblad-Olausson, P.; Pettersson, B.; Ekbom, A. The Swedish personal identity number: Possibilities and pitfalls in healthcare and medical research. Eur. J. Epidemiol. 2009, 24, 659–667. [Google Scholar] [CrossRef] [PubMed]
- Ludvigsson, J.F.; Andersson, E.; Ekbom, A.; Feychting, M.; Kim, J.-L.; Reuterwall, C.; Heurgren, M.; Olausson, P.O. External review and validation of the Swedish national inpatient register. BMC Public Health 2011, 11, 450. [Google Scholar] [CrossRef]
- Briggs, A.D.; Mytton, O.T.; Kehlbacher, A.; Tiffin, R.; Rayner, M.; Scarborough, P. Overall and income specific effect on prevalence of overweight and obesity of 20% sugar sweetened drink tax in UK: Econometric and comparative risk assessment modelling study. BMJ 2013, 347, f6189. [Google Scholar] [CrossRef] [PubMed]
- Scarborough, P.; Allender, S.; Clarke, D.; Wickramasinghe, K.; Rayner, M. Modelling the health impact of environmentally sustainable dietary scenarios in the UK. Eur. J. Clin. Nutr. 2012, 66, 710–715. [Google Scholar] [CrossRef] [PubMed]
- Briggs, A.D.; Mytton, O.T.; Madden, D.; O’Shea, D.; Rayner, M.; Scarborough, P. The potential impact on obesity of a 10% tax on sugar-sweetened beverages in Ireland, an effect assessment modelling study. BMC Public Health 2013, 13, 860. [Google Scholar] [CrossRef]
- Smed, S.; Scarborough, P.; Rayner, M.; Jensen, J.D. The effects of the Danish saturated fat tax on food and nutrient intake and modelled health outcomes: An econometric and comparative risk assessment evaluation. Eur. J. Clin. Nutr. 2016, 70, 681–686. [Google Scholar] [CrossRef]
- Clarke, P.M.; Gray, A.M.; Briggs, A.; Farmer, A.J.; Fenn, P.; Stevens, R.J.; Matthews, D.R.; Stratton, I.M.; Holman, R.R. A model to estimate the lifetime health outcomes of patients with Type 2 diabetes: The United Kingdom Prospective Diabetes Study (UKPDS) Outcomes Model (UKPDS no. 68). Diabetologia 2004, 47, 1747–1759. [Google Scholar] [CrossRef]
- Van Vliet, B.N.; Montani, J.P. The time course of salt-induced hypertension, and why it matters. Int. J. Obes. 2008, 32 (Suppl. 6), S35–S47. [Google Scholar] [CrossRef]
- Eyles, H.; Mhurchu, C.N.; Nghiem, N.; Blakely, T. Food pricing strategies, population diets, and non-communicable disease: A systematic review of simulation studies. PLoS Med 2012, 9, e1001353. [Google Scholar] [CrossRef]
- Thow, A.M.; Downs, S.; Jan, S. A systematic review of the effectiveness of food taxes and subsidies to improve diets: Understanding the recent evidence. Nutr. Rev. 2014, 72, 551–565. [Google Scholar] [CrossRef]
- Bandoni, D.H.; Sarno, F.; Jaime, P.C. Impact of an intervention on the availability and consumption of fruits and vegetables in the workplace. Public Health Nutr. 2011, 14, 975–981. [Google Scholar] [CrossRef]
- Krogholm, K.S.; Bredsdorff, L.; Alinia, S.; Christensen, T.; Rasmussen, S.E.; Dragsted, L.O. Free fruit at workplace intervention increases total fruit intake: A validation study using 24 h dietary recall and urinary flavonoid excretion. Eur. J. Clin. Nutr. 2010, 64, 1222–1228. [Google Scholar] [CrossRef]
- Nordstrom, J.; Thunstrom, L. The impact of tax reforms designed to encourage healthier grain consumption. J. Health Econ. 2009, 28, 622–634. [Google Scholar] [CrossRef] [PubMed]
- Nordstrom, J.; Thunstrom, L. Economic policies for healthier food intake: The impact on different household categories. Eur. J. Health Econom. 2011, 12, 127–140. [Google Scholar] [CrossRef]


{kind=link}
| Food/Nutrient | Recommended Intake | Actual Mean Intake (SE) | |
|---|---|---|---|
| Men (n = 792) | Women (n = 1005) | ||
| Fruits (g/day) * | 250.0 | 105.0 (3.97) | 147.0 (3.53) |
| Vegetables (g/day) * | 250.0 | 169.0 (3.69) | 182.0 (3.09) |
| Fibre (g/day) | 30.00 | 21.30 (0.29) | 18.80 (0.22) |
| Salt (g/day) | 6.00 | 8.84 (0.10) | 6.78 (0.063) |
| Total fat (%E) | 40.00 | 34.0 (0.21) | 34.40 (0.20) |
| Saturated fat (%E) | 9.00 | 13.0 (0.11) | 13.10 (0.10) |
| MUFA (%E) * | 20.00 | 12.80 (0.09) | 12.90 (0.09) |
| PUFA (%E) | 10.00 | 5.5 (0.067) | 5.7 (0.06) |
| Cholesterol (mg/day) * | 300 | 320 (5.15) | 263 (3.9) |
| Men (Mean, 95% UI) | Women (Mean, 95% UI) | Total (Mean, 95% UI) | |
|---|---|---|---|
| Fruits and vegetables | 1905 (1262–2152) | 1073 (811–1420) | 3013 (2080–3566) |
| Fiber | 718 (512–1275) | 1285 (656–1577) | 2025 (1197–2792) |
| Fats | 623 (471–792) | 245 (224–487) | 969 (709–1274) |
| Salt | 666 (335–1175) | 180 (63–237) | 1057 (391–1423) |
| All dietary guidelines combined | 3626 (2994–4175) | 2553 (2030–2980) | 6405 (5086–7086) |
| Causes of Death | Men (Mean, 95% UI) | Women (Mean, 95% UI) | Total (Mean, 95% UI) |
|---|---|---|---|
| Cardiovascular Diseases | |||
| Coronary heart disease | 2532 (1913–2775) | 1623 (1266–2028) | 4077 (4529–6462) |
| Stroke | 551 (407–777) | 609 (302–822) | 1219 (729–1548) |
| Heart failure | 72 (37–139) | 30 (9–36) | 147 (46–175) |
| Aortic aneurysm | 27 (12–47) | 4 (2–6) | 49 (14–54) |
| Pulmonary embolism | 6 (2–11) | 1 (0–3) | 10 (2–14) |
| Rheumatic Heart disease | 1 (0–3) | 0 (0–1) | 2 (1–4) |
| Hypertensive disease | 120 (59–200) | 54 (18–65) | 233 (77–267) |
| Actual mortality | 12,206 | 11,093 | 23,299 |
| Cancer | |||
| Colo-rectal | 76 (10–241) | 90 (32–178) | 261 (96–363) |
| Lung | 240 (103–381) | 142 (45–174) | 407 (141–564) |
| Actual mortality | 3251 | 3141 | 6392 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saha, S.; Nordstrom, J.; Gerdtham, U.-G.; Mattisson, I.; Nilsson, P.M.; Scarborough, P. Prevention of Cardiovascular Disease and Cancer Mortality by Achieving Healthy Dietary Goals for the Swedish Population: A Macro-Simulation Modelling Study. Int. J. Environ. Res. Public Health 2019, 16, 890. https://doi.org/10.3390/ijerph16050890
Saha S, Nordstrom J, Gerdtham U-G, Mattisson I, Nilsson PM, Scarborough P. Prevention of Cardiovascular Disease and Cancer Mortality by Achieving Healthy Dietary Goals for the Swedish Population: A Macro-Simulation Modelling Study. International Journal of Environmental Research and Public Health. 2019; 16(5):890. https://doi.org/10.3390/ijerph16050890
Chicago/Turabian StyleSaha, Sanjib, Jonas Nordstrom, Ulf-G Gerdtham, Irene Mattisson, Peter M Nilsson, and Peter Scarborough. 2019. "Prevention of Cardiovascular Disease and Cancer Mortality by Achieving Healthy Dietary Goals for the Swedish Population: A Macro-Simulation Modelling Study" International Journal of Environmental Research and Public Health 16, no. 5: 890. https://doi.org/10.3390/ijerph16050890
APA StyleSaha, S., Nordstrom, J., Gerdtham, U.-G., Mattisson, I., Nilsson, P. M., & Scarborough, P. (2019). Prevention of Cardiovascular Disease and Cancer Mortality by Achieving Healthy Dietary Goals for the Swedish Population: A Macro-Simulation Modelling Study. International Journal of Environmental Research and Public Health, 16(5), 890. https://doi.org/10.3390/ijerph16050890