9/11 Residential Exposures: The Impact of World Trade Center Dust on Respiratory Outcomes of Lower Manhattan Residents

 ,
,
Abstract
1. Introduction
2. Methods
2.1. Environmental and Household Exposures
2.2. Health Outcomes
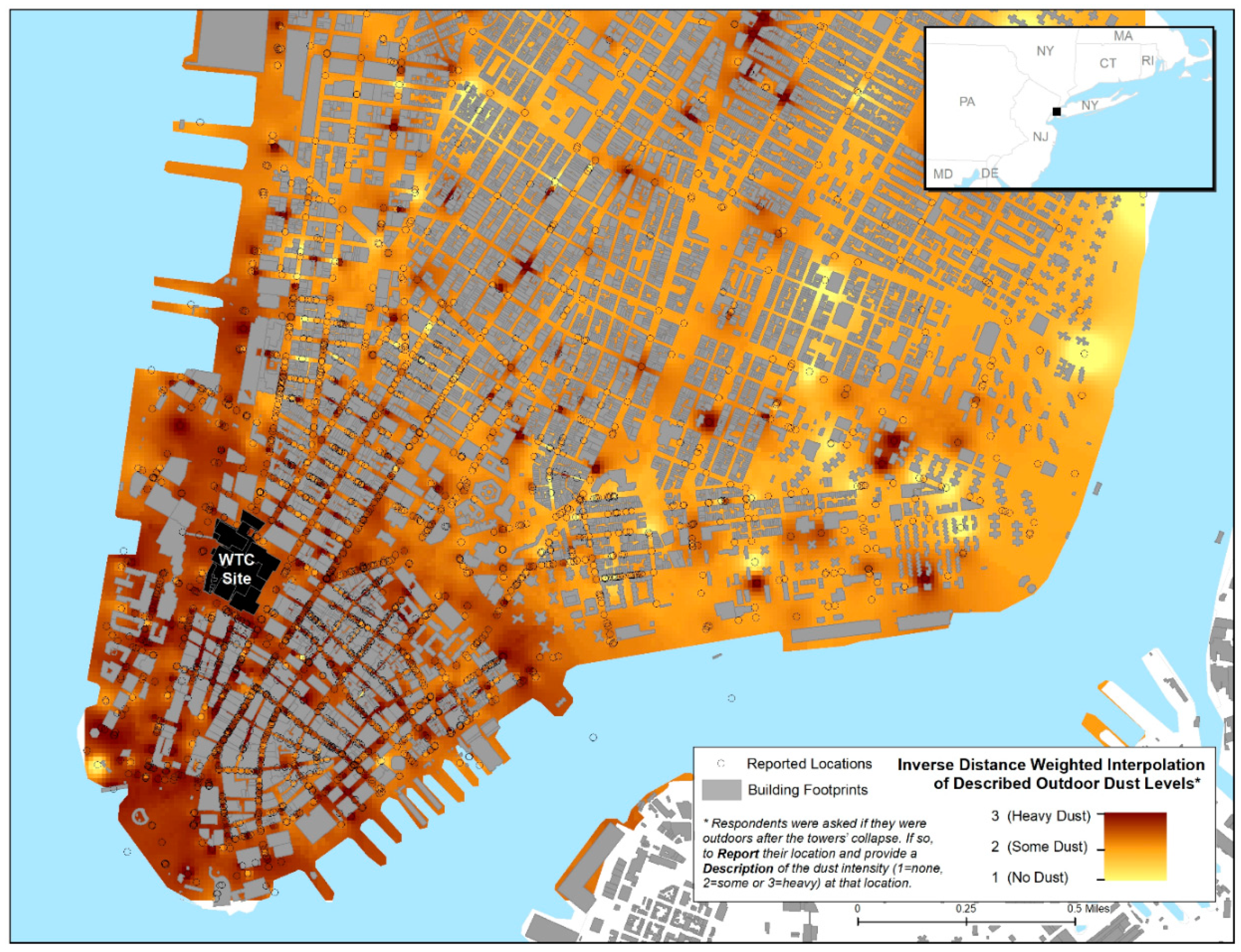
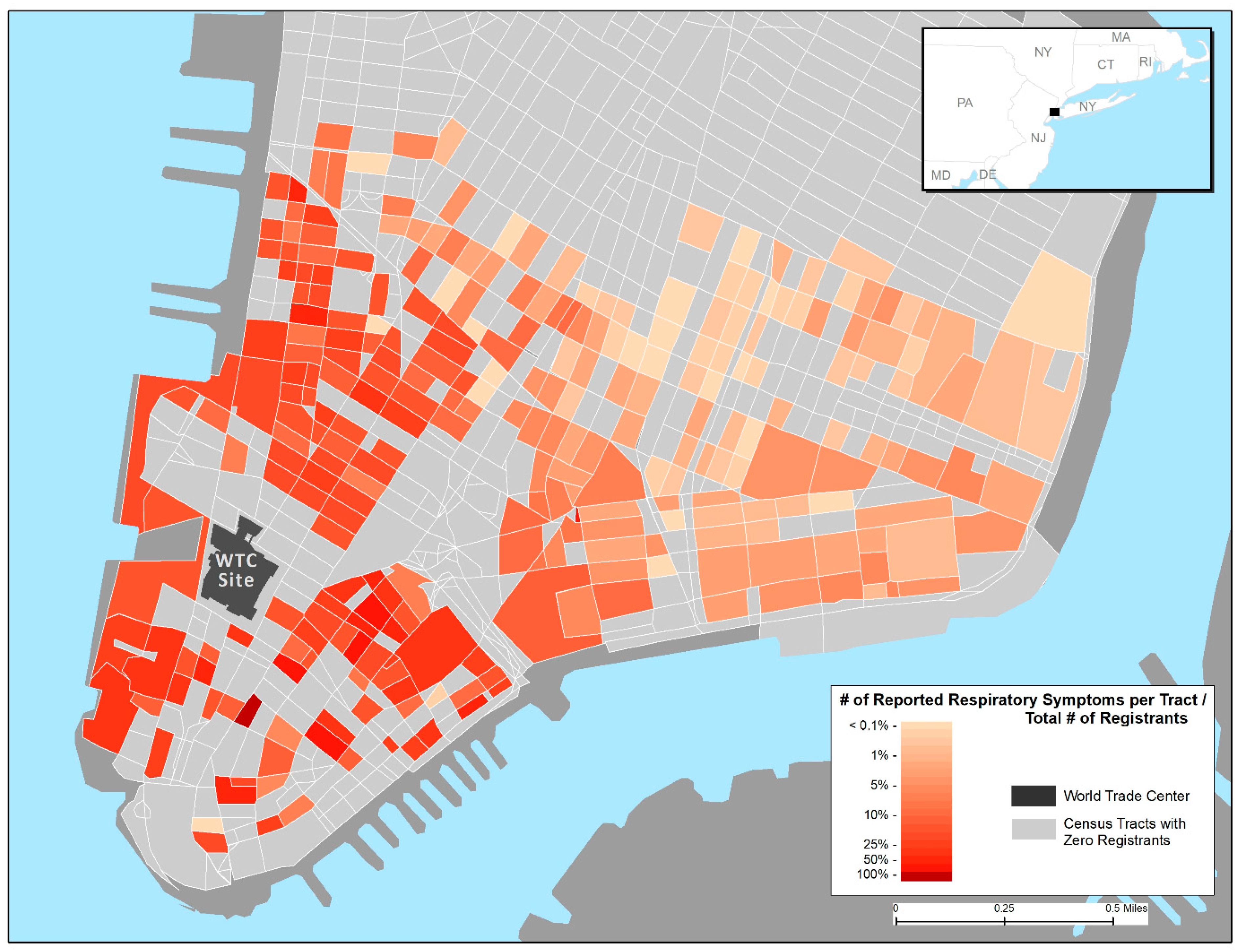
2.3. Geospatial Analyses
2.4. Statistical Analyses
- (a)
- Five demographic variables (age at 9/11, race, sex, education, and income);
- (b)
- Resident priority group, indicating degree of registrant recruitment by area (partially a surrogate for location relative to the WTC site);
- (c)
- Dust cloud exposure category (intense, some, none);
- (d)
- Ever having smoked (at least 100 cigarettes in a lifetime);
- (e)
- Five variables of exposures in the home (broken windows, debris in the home, fine dust, heavy dust, and damage in the home);
- (f)
- Four variables containing data on behavior regarding replacement of various major items in the home (having replaced air-conditioning, carpeting, drapes, and furniture); and
- (g)
- Four variables for the presence of cleaning practices, which are conditioned on the presence of dust in the home.
3. Results
3.1. Geospatial Representation of Exposures and Symptoms
3.2. Home Damage and Cleaning Practices
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lioy, P.J.; Weisel, C.P.; Millette, J.R.; Eisenreich, S.; Vallero, D.; Offenberg, J.; Buckley, B.; Turpin, B.; Zhong, M.; Cohen, M.D.; et al. Characterization of the dust/smoke aerosol that settled east of the World Trade Center (WTC) in lower Manhattan after the collapse of the WTC 11 September 2001. Environ. Health Perspect. 2002, 110, 703–714. [Google Scholar] [CrossRef] [PubMed]
- Lioy, P.J.; Georgopoulos, P. The anatomy of the exposures that occurred around the World Trade Center site: 9/11 and beyond. Ann. N. Y. Acad. Sci. 2006, 1076, 54–79. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Prevention, Potential exposures to airborne and settled surface dust in residential areas of lower Manhattan following the collapse of the World Trade Center—New York City, November 4–December 11, 2001. MMWR Morb. Mortal Wkly. Rep. 2003, 52, 131–136. [Google Scholar]
- Lorber, M.; Gibb, H.; Grant, L.; Pinto, J.; Pleil, J.; Cleverly, D. Assessment of inhalation exposures and potential health risks to the general population that resulted from the collapse of the World Trade Center towers. Risk Anal. 2007, 27, 1203–1221. [Google Scholar] [CrossRef] [PubMed]
- Offenberg, J.H.; Eisenreich, S.J.; Gigliotti, C.L.; Chen, L.C.; Xiong, J.Q.; Quan, C.; Lou, X.; Zhong, M.; Gorczynski, J.; Yiin, L.M.; et al. Persistent organic pollutants in dusts that settled indoors in lower Manhattan after September 11, 2001. J. Expo. Anal. Environ. Epidemiol. 2004, 14, 164–172. [Google Scholar] [CrossRef] [PubMed]
- Yiin, L.M.; Millette, J.R.; Vette, A.; Ilacqua, V.; Quan, C.; Gorczynski, J.; Kendall, M.; Chen, L.C.; Weisel, C.P.; Buckley, B.; et al. Comparisons of the dust/smoke particulate that settled inside the surrounding buildings and outside on the streets of southern New York City after the collapse of the World Trade Center, September 11, 2001. J. Air Waste Manag. Assoc. 2004, 54, 515–528. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Community needs assessment of lower Manhattan residents following the World Trade Center attacks—Manhattan, New York City, 2001. MMWR Morb. Mortal Wkly. Rep. 2002, 51, 10–13. [Google Scholar]
- Lin, S.; Jones, R.; Reibman, J.; Bowers, J.; Fitzgerald, E.F.; Hwang, S.A. Reported respiratory symptoms and adverse home conditions after 9/11 among residents living near the World Trade Center. J. Asthma 2007, 44, 325–332. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.; Jones, R.; Reibman, J.; Morse, D.; Hwang, S.A. Lower respiratory symptoms among residents living near the World Trade Center, two and four years after 9/11. Int. J. Occup. Environ. Health 2010, 16, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.; Reibman, J.; Bowers, J.A.; Hwang, S.A.; Hoerning, A.; Gomez, M.I.; Fitzgerald, E.F. Upper respiratory symptoms and other health effects among residents living near the World Trade Center site after September 11, 2001. Am. J. Epidemiol. 2005, 162, 499–507. [Google Scholar] [CrossRef] [PubMed]
- Reibman, J.; Lin, S.; Hwang, S.A.; Gulati, M.; Bowers, J.A.; Rogers, L.; Berger, K.I.; Hoerning, A.; Gomez, M.; Fitzgerald, E.F. The World Trade Center residents’ respiratory health study: New-onset respiratory symptoms and pulmonary function. Environ. Health Perspect. 2005, 113, 406–411. [Google Scholar] [CrossRef] [PubMed]
- Brackbill, R.M.; Hadler, J.L.; DiGrande, L.; Ekenga, C.C.; Farfel, M.R.; Friedman, S.; Perlman, S.E.; Stellman, S.D.; Walker, D.J.; Wu, D.; et al. Asthma and posttraumatic stress symptoms 5 to 6 years following exposure to the World Trade Center terrorist attack. JAMA 2009, 302, 502–516. [Google Scholar] [CrossRef] [PubMed]
- Maslow, C.B.; Friedman, S.M.; Pillai, P.S.; Reibman, J.; Berger, K.I.; Goldring, R.; Stellman, S.D.; Farfel, M. Chronic and acute exposures to the world trade center disaster and lower respiratory symptoms: Area residents and workers. Am. J. Public Health 2012, 102, 1186–1194. [Google Scholar] [CrossRef] [PubMed]
- Farfel, M.; DiGrande, L.; Brackbill, R.; Prann, A.; Cone, J.; Friedman, S.; Walker, D.J.; Pezeshki, G.; Thomas, P.; Galea, S.; et al. An overview of 9/11 experiences and respiratory and mental health conditions among World Trade Center Health Registry enrollees. J. Urban Health 2008, 85, 880–909. [Google Scholar] [CrossRef] [PubMed]
- Environmental Protection Agency. Interim Final WTC Residential Confirmation Study. In 2003. Available online: http://www.epa.gov/wtc/reports/confirmation_cleaning_study.pdf (accessed on 18 December 2014).
- Environmental Protection Agency. World Trade Center Residential Dust Cleanup Program. Final Report. In 2005. Available online: http://permanent.access.gpo.gov/gpo41622/residential-dust-cleanup-final-report.pdf (accessed on 28 January 2016).
- Antao, V.C.; Pallos, L.L.; Shim, Y.K.; Sapp, J.H., 2nd; Brackbill, R.M.; Cone, J.E.; Stellman, S.D.; Farfel, M.R. Respiratory protective equipment, mask use, and respiratory outcomes among World Trade Center rescue and recovery workers. Am. J. Ind. Med. 2011, 54, 897–905. [Google Scholar] [CrossRef] [PubMed]
- De la Hoz, R.E.; Shohet, M.R.; Chasan, R.; Bienenfeld, L.A.; Afilaka, A.A.; Levin, S.M.; Herbert, R. Occupational toxicant inhalation injury: The World Trade Center (WTC) experience. Int. Arch. Occup. Environ. Health 2008, 81, 479–485. [Google Scholar] [CrossRef] [PubMed]
- Herbert, R.; Moline, J.; Skloot, G.; Metzger, K.; Baron, S.; Luft, B.; Markowitz, S.; Udasin, I.; Harrison, D.; Stein, D.; et al. The World Trade Center disaster and the health of workers: Five-year assessment of a unique medical screening program. Environ. Health Perspect. 2006, 114, 1853–1858. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | N | % |
|---|---|---|
| Age on 9/11/2001 (yrs, mean ± SD) | 45.1 ± 15.1 | - |
| Sex (male) | 2688 | 41.7 |
| Race | ||
| White | 4281 | 66.4 |
| Black | 325 | 5 |
| Hispanic | 579 | 9 |
| Asian | 1061 | 16.5 |
| Other/Unknown | 201 | 3.1 |
| Education * | ||
| <High school | 504 | 7.9 |
| High school | 738 | 11.5 |
| Some college | 893 | 14 |
| College + | 4265 | 66.6 |
| Income level | ||
| Less than 25K | 1322 | 20.9 |
| 25 to <50K | 1181 | 18.6 |
| 50 to <75K | 836 | 13.2 |
| 75 to <100K | 1801 | 28.4 |
| 100K or more | 1197 | 18.9 |
| Ever smoking * | 2903 | 45.4 |
| Dust cloud exposure on 9/11 * | ||
| None | 3446 | 56.3 |
| Some | 1196 | 19.5 |
| Intense | 1479 | 24.2 |
| Characteristics | N * | % |
|---|---|---|
| Fine coating of dust | 3974/6241 | 63.7 |
| Heavy coating of dust | 1067/6251 | 17.1 |
| Broken windows | 368/6256 | 5.9 |
| Damage to home or furnishings | 927/6250 | 14.8 |
| Presence of debris | 759/6256 | 12.1 |
| Cleaned ventilation ducts | 1061/5931 | 17.9 |
| Cleaned with damp cloth, sponge, or mop | 3307/5919 | 55.9 |
| Used a vacuum to clean | 2687/5934 | 45.3 |
| Dusted or swept without water | 1263/5407 | 23.4 |
| Replaced carpet or rugs | 1201/6090 | 19.7 |
| Replaced furniture | 1304/6090 | 21.4 |
| Replaced drapes, blinds, or curtains | 1232/6090 | 20.2 |
| Replaced air conditioners | 1896/6090 | 31.1 |
| Exposure/Cleaning Practices | Adjusted Odds Ratio (95% Confidence Interval) * | |||
|---|---|---|---|---|
| Dusted or Swept without Water | Cleaned with Damp Cloth, Sponge, or Mop | Used a Vacuum to Clean | Cleaned Ventilation Ducts | |
| Fine coating of dust | 0.99 (0.82, 1.20) | 1.85 (1.59, 2.14) | 0.63 (0.53, 0.74) | 0.38 (0.27, 0.52) |
| Heavy coating of dust | 1.03 (0.82, 1.29) | 1.08 (0.88, 1.33) | 0.64 (0.52, 0.79) | 0.59 (0.42, 0.83) |
| Broken windows | 1.24 (0.86, 1.79) | 0.69 (0.48, 0.99) | 0.97 (0.67, 1.39) | 0.95 (0.57, 1.59) |
| Damage to home or furnishings | 0.92 (0.73, 1.14) | 0.90 (0.72, 1.12) | 1.25 (1.01, 1.54) | 1.34 (1.01, 1.79) |
| Presence of debris | 1.31 (1.06, 1.61) | 1.07 (0.87, 1.33) | 1.20 (0.98, 1.48) | 1.16 (0.87, 1.53) |
| Dusted or swept without water | - | 1.50 (1.26, 1.79) | 1.76 (1.50, 2.07) | 1.76 (1.43, 2.18) |
| Cleaned with damp cloth, sponge, or mop | 1.47 (1.23, 1.74) | - | 4.59 (3.95, 5.34) | 3.92 (2.94, 5.23) |
| Used a vacuum to clean | 1.73 (1.48, 2.03) | 4.71 (4.04, 5.50) | - | 1.95 (1.56, 2.43) |
| Cleaned ventilation ducts | 1.74 (1.41, 2.15) | 5.28 (3.72, 7.50) | 2.08 (1.65, 2.62) | - |
| Symptom/Disease | N * | % |
|---|---|---|
| Shortness of breath | 983/6126 | 16.1 |
| Wheezing | 668/6234 | 10.7 |
| Chronic cough | 439/6415 | 6.8 |
| Upper respiratory symptoms | 3761/6,190 | 60.8 |
| Asthma/RADS † | 434/5466 | 7.9 |
| Chronic obstructive pulmonary disease | 320/5931 | 5.4 |
| Exposure/Cleaning Practices | Adjusted Odds Ratios (95% Confidence Interval) * for Each Respiratory Condition | |||||
|---|---|---|---|---|---|---|
| Shortness of Breath | Wheezing | Chronic Cough | URS ** | Asthma/RADS † | COPD ‡ | |
| Light coating of dust | 1.25 (0.98–1.59) | 1.10 (0.84, 1.45) | 1.06 (0.77, 1.47) | 1.11 (0.93, 1.31) | 1.01 (0.74, 1.39) | 1.19 (0.84, 1.70) |
| Broken Windows | 0.95 (0.60, 1.50) | 1.46 (0.91, 2.36) | 0.88 (0.68, 1.62) | 0.98 (0.66, 1.44) | 1.16 (0.63, 2.12) | 1.01 (0.51, 1.99) |
| Heavy coating of dust | 1.65 (1.24, 2.18) | 1.43 (1.03, 1.97) | 1.59 (1.09, 2.28) | 1.08 (0.87, 1.35) | 1.21 (0.82, 1.79) | 1.35 (0.89, 2.05) |
| Damage to home or furnishings | 1.33 (1.01, 1.75) | 1.31 (0.96–1.81) | 0.82 (0.56, 1.19) | 1.36 (1.06, 1.74) | 1.11 (0.74, 1.65) | 1.11 (0.73, 1.68) |
| Presence of debris | 1.62 (0.97, 1.64) | 1.19 (0.88, 1.61) | 1.56 (1.12, 2.17) | 1.56 (1.24, 1.95) | 0.92 (0.63, 1.35) | 0.94 (0.63, 1.40) |
| Replaced air conditioner | 1.06 (0.87, 1.28) | 1.08 (0.87, 1.34) | 1.24 (0.96, 1.60) | 1.32 (1.14, 1.54) | 0.91 (0.69, 1.19) | 1.31 (0.99, 1.74) |
| Replaced carpets | 0.90 (0.70, 1.17) | 1.05 (0.78, 1.41) | 1.07 (0.76, 1.50) | 1.03 (0.83, 1.28) | 1.21 (0.85, 1.73) | 1.49 (1.03, 2.16) |
| Replaced drapes | 1.31 (1.03, 1.65) | 0.98 (0.75, 1.29) | 1.02 (0.74, 1.40) | 1.11 (0.90, 1.36) | 0.99 (0.71, 1.39) | 0.96 (0.67, 1.38) |
| Replaced furniture | 1.24 (0.97, 1.59) | 1.13 (0.85, 1.51) | 1.24 (0.89, 1.73) | 1.14 (0.93, 1.40) | 1.40 (0.99, 1.96) | 0.89 (0.62, 1.29) |
| Dusted or swept without water | 1.37 (1.11, 1.69) | 1.49 (1.17, 1.90) | 1.21 (0.91, 1.61) | 1.28 (1.08, 1.53) | 1.35 (1.00, 1.81) | 1.16 (0.85, 1.61) |
| Cleaned with damp cloth, sponge, mop | 1.15 (0.92, 1.43) | 1.01 (0.79, 1.30) | 1.05 (0.78, 1.41) | 1.40 (1.18, 1.64) | 0.91 (0.67, 1.22) | 0.96 (0.69, 1.32) |
| Cleaned ventilation ducts | 1.23 (0.93, 1.64) | 1.48 (1.08, 2.01) | 1.94 (1.38, 2.73) | 1.18 (0.92, 1.53) | 1.23 (0.82, 1.82) | 1.30 (0.86, 1.96) |
| Vacuumed | 0.96 (0.78, 1.19) | 1.06 (0.84, 1.34) | 0.95 (0.71, 1.25) | 1.01 (0.86, 1.19) | 0.99 (0.75, 1.33) | 0.94 (0.69, 1.29) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Antao, V.C.; Pallos, L.L.; Graham, S.L.; Shim, Y.K.; Sapp, J.H.; Lewis, B.; Bullard, S.; Alper, H.E.; Cone, J.E.; Farfel, M.R.; et al. 9/11 Residential Exposures: The Impact of World Trade Center Dust on Respiratory Outcomes of Lower Manhattan Residents. Int. J. Environ. Res. Public Health 2019, 16, 798. https://doi.org/10.3390/ijerph16050798
Antao VC, Pallos LL, Graham SL, Shim YK, Sapp JH, Lewis B, Bullard S, Alper HE, Cone JE, Farfel MR, et al. 9/11 Residential Exposures: The Impact of World Trade Center Dust on Respiratory Outcomes of Lower Manhattan Residents. International Journal of Environmental Research and Public Health. 2019; 16(5):798. https://doi.org/10.3390/ijerph16050798
Chicago/Turabian StyleAntao, Vinicius C., L. Lászlo Pallos, Shannon L. Graham, Youn K. Shim, James H. Sapp, Brian Lewis, Steven Bullard, Howard E. Alper, James E. Cone, Mark R. Farfel, and et al. 2019. "9/11 Residential Exposures: The Impact of World Trade Center Dust on Respiratory Outcomes of Lower Manhattan Residents" International Journal of Environmental Research and Public Health 16, no. 5: 798. https://doi.org/10.3390/ijerph16050798
APA StyleAntao, V. C., Pallos, L. L., Graham, S. L., Shim, Y. K., Sapp, J. H., Lewis, B., Bullard, S., Alper, H. E., Cone, J. E., Farfel, M. R., & Brackbill, R. M. (2019). 9/11 Residential Exposures: The Impact of World Trade Center Dust on Respiratory Outcomes of Lower Manhattan Residents. International Journal of Environmental Research and Public Health, 16(5), 798. https://doi.org/10.3390/ijerph16050798