Spatial-Temporal Effects of PM2.5 on Health Burden: Evidence from China



Abstract
1. Introduction
2. Research Design
2.1. Data
2.2. Variable
2.2.1. Dependent Variable: Health Burden
2.2.2. Independent Variable: PM2.5 Exposure
2.2.3. Control Variable
2.3. Method
2.3.1. Spatial Autocorrelation Test
2.3.2. Spatial Econometric Model
2.3.3. Model Test
3. Spatial Distribution and Spatial Autocorrelation Analysis
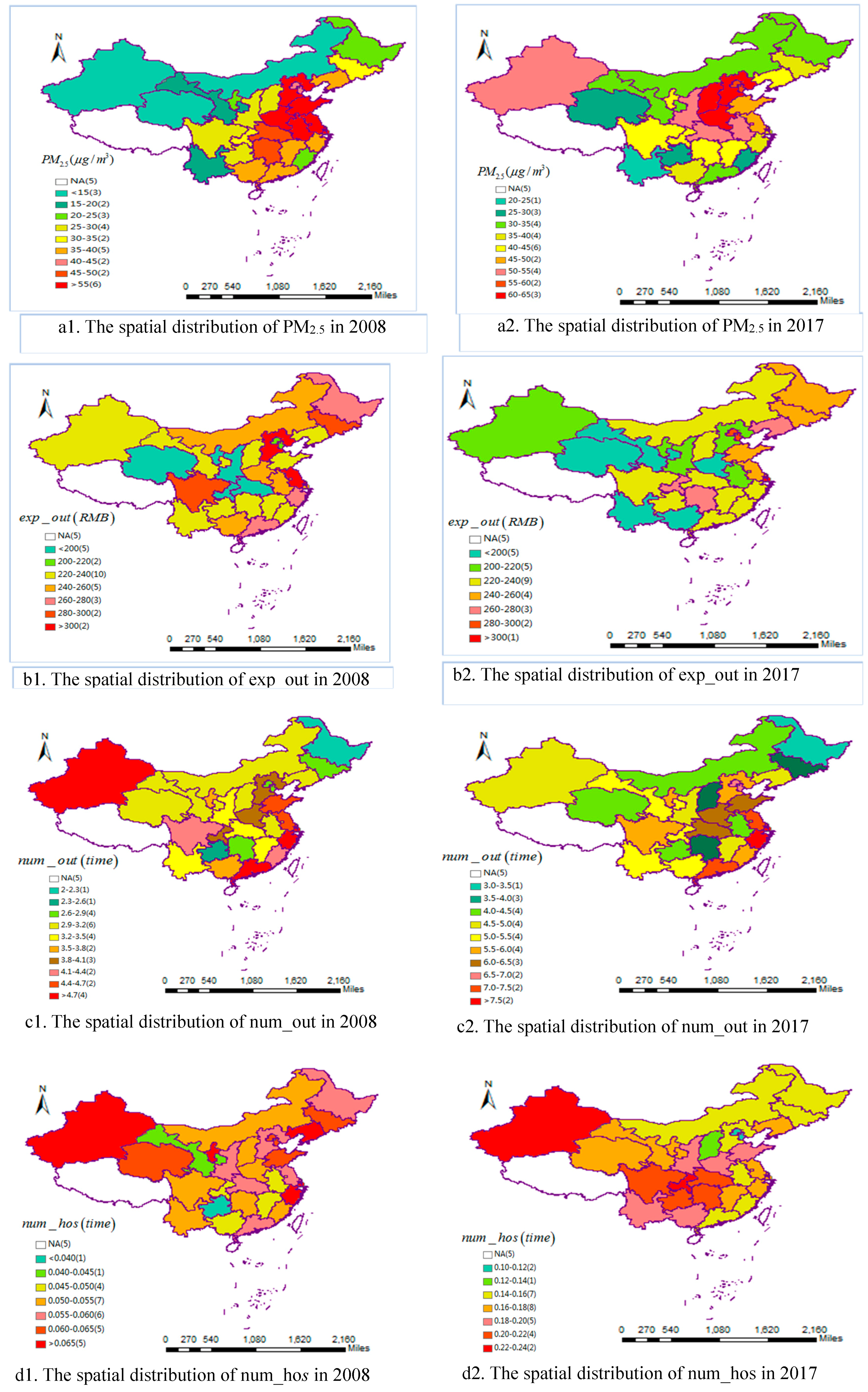
3.1. Spatial Distribution
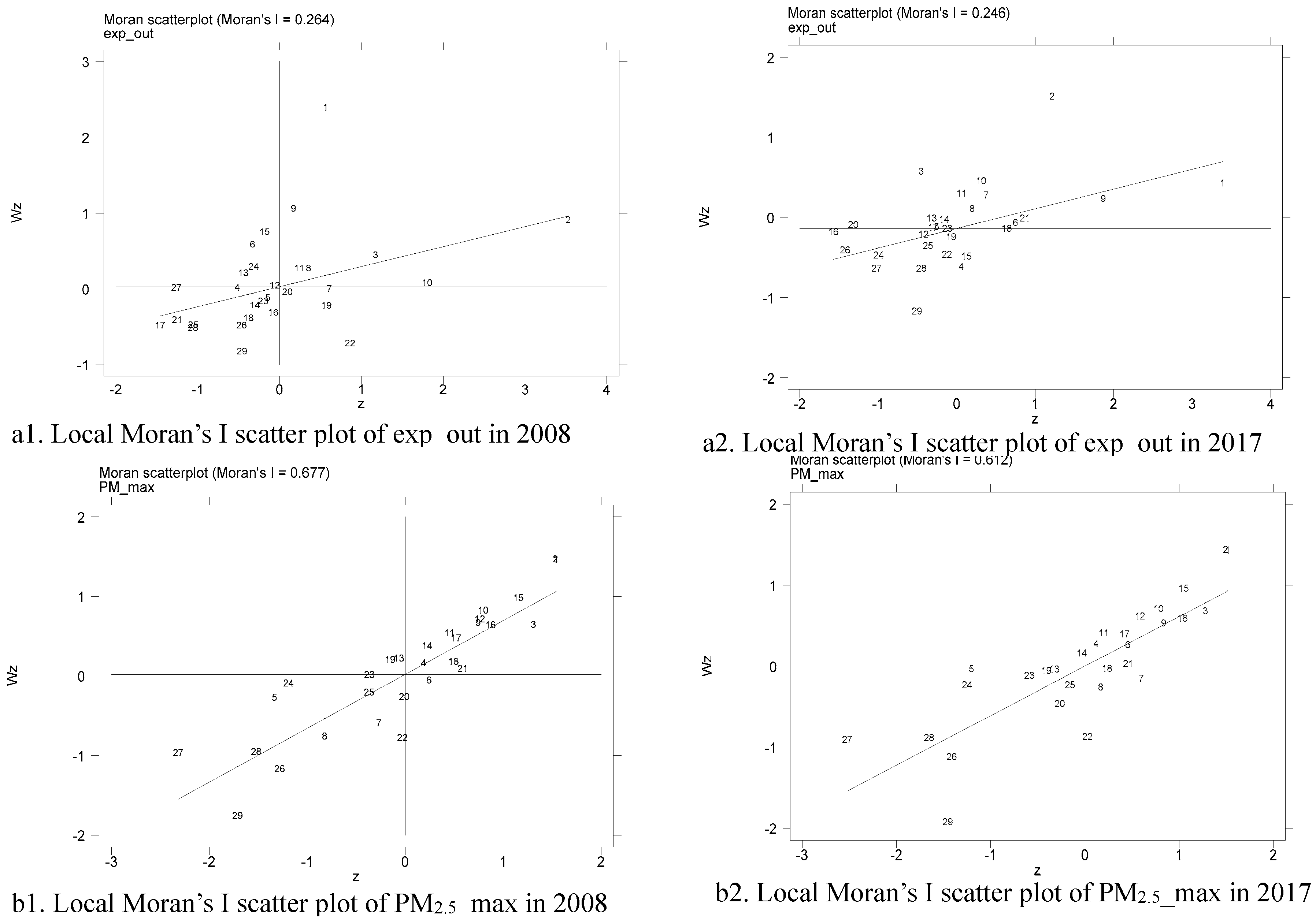
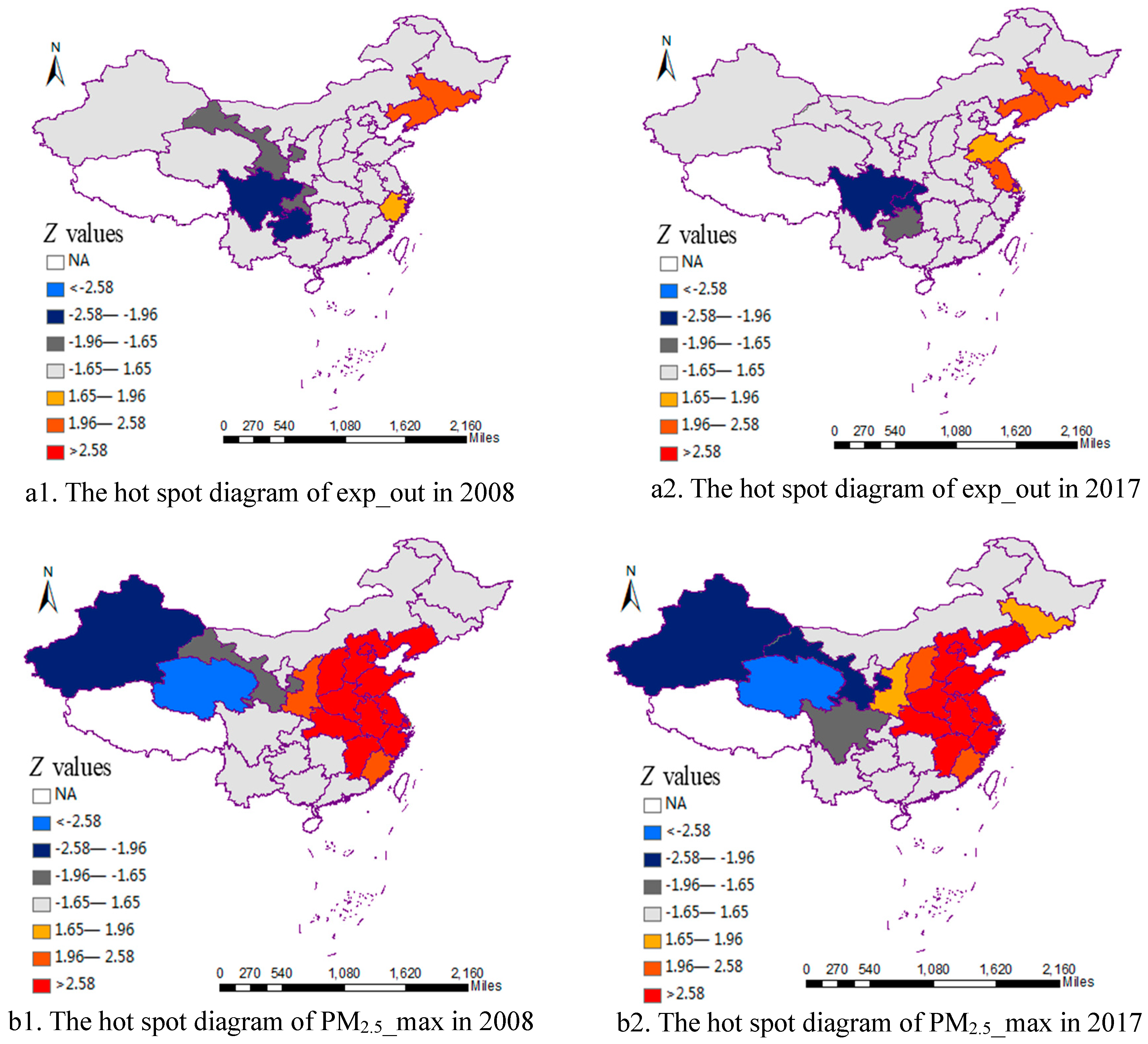
3.2. Spatial Autocorrelation Analysis
4. Empirical Analysis and Discussion
4.1. Impact of PM2.5 Exposureon Outpatient Expense
4.2. Impact of PM2.5 Exposure on Outpatient Visits
4.3. Robustness Tests
4.3.1. Alternative Independent Variable Estimation
4.3.2. Alternative Dependent Variable Estimation
4.3.3. Endogenous Test
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Region | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Beijing | 50.81 | 48.21 | 47.35 | 48.59 | 43.02 | 48.06 | 41.55 | 50.00 | 44.06 | 48.46 | 45.00 |
| Tianjin | 81.93 | 74.84 | 74.95 | 78.14 | 70.81 | 71.88 | 62.03 | 81.79 | 71.47 | 74.82 | 70.79 |
| Hebei | 62.95 | 60.32 | 54.69 | 57.14 | 52.64 | 53.13 | 49.84 | 61.00 | 53.52 | 55.35 | 55.99 |
| Shanxi | 33.98 | 33.93 | 26.71 | 27.76 | 26.56 | 27.11 | 24.82 | 30.08 | 25.37 | 25.92 | 24.97 |
| Inner Mongolia | 11.07 | 12.28 | 11.92 | 11.77 | 12.04 | 10.52 | 10.12 | 21.05 | 10.88 | 13.52 | 12.49 |
| Liaoning | 33.02 | 34.49 | 37.19 | 38.34 | 35.85 | 33.13 | 28.49 | 35.81 | 34.47 | 47.66 | 34.61 |
| Jilin | 28.82 | 29.79 | 32.65 | 34.62 | 32.59 | 29.42 | 26.24 | 33.24 | 32.12 | 47.53 | 34.47 |
| Heilongjiang | 19.23 | 18.36 | 20.39 | 21.83 | 21.59 | 18.42 | 16.83 | 22.09 | 22.49 | 32.68 | 26.69 |
| Shanghai | 52.07 | 56.95 | 56.78 | 58.01 | 51.61 | 49.96 | 44.70 | 54.15 | 47.31 | 61.08 | 50.85 |
| Jiangsu | 61.23 | 61.74 | 59.58 | 60.00 | 59.97 | 58.06 | 50.20 | 60.65 | 57.22 | 65.39 | 58.31 |
| Zhejiang | 33.38 | 37.86 | 38.35 | 34.29 | 33.81 | 31.62 | 31.70 | 34.90 | 34.27 | 33.21 | 28.58 |
| Anhui | 49.57 | 58.11 | 55.19 | 52.24 | 53.38 | 49.67 | 45.46 | 53.13 | 53.81 | 57.02 | 46.15 |
| Fujian | 23.73 | 24.65 | 23.23 | 21.74 | 20.68 | 19.96 | 19.56 | 20.37 | 21.29 | 19.91 | 20.00 |
| Jiangxi | 37.63 | 41.04 | 39.74 | 37.46 | 36.72 | 33.67 | 34.56 | 34.93 | 37.99 | 34.86 | 31.36 |
| Shandong | 64.44 | 69.31 | 60.95 | 58.24 | 64.12 | 57.36 | 55.35 | 64.77 | 57.81 | 61.65 | 62.53 |
| Henan | 60.31 | 65.44 | 50.66 | 50.87 | 54.51 | 52.10 | 48.74 | 61.33 | 51.56 | 52.56 | 48.91 |
| Hubei | 45.82 | 49.18 | 46.88 | 45.58 | 49.40 | 45.47 | 40.35 | 46.29 | 48.14 | 47.29 | 37.68 |
| Hunan | 41.63 | 46.79 | 45.02 | 43.05 | 40.58 | 37.99 | 39.47 | 37.93 | 40.88 | 36.55 | 31.43 |
| Guangdong | 31.33 | 34.20 | 35.28 | 34.32 | 30.74 | 29.13 | 28.60 | 28.93 | 33.49 | 26.75 | 25.49 |
| Guangxi | 35.25 | 38.76 | 38.20 | 37.71 | 33.92 | 34.51 | 36.17 | 35.08 | 36.97 | 29.95 | 28.67 |
| Chongqing | 39.01 | 36.18 | 32.13 | 32.30 | 35.43 | 30.37 | 30.77 | 30.94 | 28.98 | 25.90 | 23.28 |
| Sichuan | 37.16 | 29.48 | 29.71 | 28.39 | 34.60 | 30.00 | 29.68 | 31.11 | 28.53 | 23.14 | 22.85 |
| Guizhou | 29.93 | 29.19 | 29.71 | 29.98 | 28.55 | 28.81 | 28.77 | 26.41 | 28.93 | 23.14 | 20.74 |
| Yunnan | 16.27 | 16.09 | 16.37 | 16.61 | 16.57 | 17.62 | 15.75 | 18.07 | 17.26 | 14.77 | 14.25 |
| Shaanxi | 32.31 | 32.74 | 25.68 | 27.36 | 28.21 | 28.07 | 26.32 | 31.82 | 25.76 | 26.28 | 24.23 |
| Gansu | 21.39 | 22.11 | 19.39 | 18.22 | 18.44 | 17.71 | 16.32 | 21.05 | 18.34 | 15.15 | 15.38 |
| Qinghai | 9.71 | 9.93 | 10.04 | 9.10 | 10.92 | 8.70 | 8.16 | 10.65 | 9.70 | 6.94 | 7.85 |
| Ningxia | 24.02 | 20.85 | 20.51 | 19.92 | 21.03 | 17.34 | 16.91 | 21.94 | 19.60 | 17.32 | 17.30 |
| Xinjiang | 9.04 | 7.78 | 9.06 | 8.39 | 8.69 | 7.70 | 7.75 | 9.77 | 8.72 | 10.43 | 11.50 |
| Region | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Beijing | 102.10 | 90.80 | 88.70 | 89.70 | 85.60 | 92.00 | 78.60 | 97.00 | 84.30 | 93.50 | 88.90 |
| Tianjin | 96.10 | 89.00 | 88.50 | 90.80 | 83.80 | 87.00 | 75.00 | 96.20 | 86.10 | 84.60 | 84.10 |
| Hebei | 90.24 | 86.91 | 80.84 | 84.26 | 78.54 | 80.29 | 74.94 | 88.25 | 81.16 | 81.97 | 84.65 |
| Shanxi | 62.63 | 60.25 | 51.49 | 53.26 | 51.29 | 51.77 | 49.26 | 55.43 | 50.45 | 50.35 | 51.29 |
| Inner Mongolia | 26.68 | 27.57 | 27.87 | 27.56 | 27.60 | 25.08 | 24.53 | 30.06 | 26.62 | 32.67 | 29.68 |
| Liaoning | 48.08 | 49.34 | 52.65 | 54.36 | 51.15 | 48.95 | 42.80 | 51.18 | 49.37 | 63.48 | 50.55 |
| Jilin | 38.97 | 40.83 | 42.83 | 46.27 | 43.71 | 39.90 | 36.43 | 44.84 | 43.83 | 67.19 | 47.13 |
| Heilongjiang | 34.24 | 33.18 | 34.22 | 38.81 | 37.29 | 33.05 | 30.92 | 38.75 | 38.95 | 56.52 | 43.22 |
| Shanghai | 60.10 | 65.80 | 64.40 | 65.20 | 56.60 | 57.50 | 52.70 | 62.70 | 57.90 | 73.90 | 59.50 |
| Jiangsu | 67.92 | 68.58 | 65.76 | 65.92 | 66.45 | 64.05 | 55.94 | 67.04 | 63.93 | 72.25 | 64.88 |
| Zhejiang | 51.66 | 56.85 | 57.27 | 53.29 | 51.46 | 49.53 | 50.04 | 54.35 | 52.73 | 52.25 | 47.15 |
| Anhui | 59.15 | 68.31 | 64.88 | 62.39 | 63.00 | 58.51 | 54.29 | 63.08 | 65.01 | 66.88 | 55.85 |
| Fujian | 47.62 | 48.24 | 46.49 | 44.93 | 43.87 | 43.22 | 42.37 | 43.88 | 45.06 | 43.87 | 43.70 |
| Jiangxi | 50.33 | 54.01 | 52.22 | 50.61 | 49.77 | 45.95 | 47.21 | 47.91 | 51.87 | 48.44 | 44.33 |
| Shandong | 80.28 | 84.74 | 75.99 | 72.74 | 79.43 | 72.10 | 71.08 | 80.45 | 73.63 | 77.12 | 79.54 |
| Henan | 78.56 | 83.93 | 67.74 | 68.16 | 72.04 | 69.85 | 65.70 | 80.07 | 70.34 | 70.09 | 67.53 |
| Hubei | 57.63 | 61.85 | 58.80 | 57.47 | 62.58 | 57.44 | 51.22 | 59.29 | 61.58 | 60.62 | 49.24 |
| Hunan | 53.39 | 58.99 | 58.15 | 55.76 | 53.34 | 50.07 | 51.76 | 50.86 | 55.29 | 49.62 | 43.48 |
| Guangdong | 41.08 | 44.34 | 44.86 | 44.23 | 40.25 | 38.04 | 37.79 | 37.96 | 43.83 | 35.56 | 34.21 |
| Guangxi | 44.74 | 48.71 | 47.54 | 47.47 | 42.94 | 43.33 | 45.32 | 44.45 | 45.89 | 38.84 | 37.56 |
| Chongqing | 72.50 | 72.20 | 60.50 | 58.40 | 63.60 | 57.40 | 57.70 | 59.10 | 55.60 | 51.70 | 44.70 |
| Sichuan | 57.32 | 47.46 | 47.19 | 45.56 | 53.48 | 47.53 | 46.91 | 49.98 | 46.19 | 39.77 | 39.54 |
| Guizhou | 40.97 | 40.32 | 41.16 | 41.81 | 40.14 | 40.36 | 40.77 | 37.42 | 40.62 | 34.52 | 31.49 |
| Yunnan | 29.53 | 29.73 | 29.51 | 29.99 | 30.51 | 31.43 | 29.32 | 32.10 | 31.05 | 28.14 | 27.66 |
| Shaanxi | 50.02 | 50.38 | 41.12 | 42.99 | 43.96 | 44.20 | 41.20 | 49.68 | 42.09 | 42.64 | 40.87 |
| Gansu | 30.59 | 32.34 | 28.46 | 26.22 | 26.31 | 25.83 | 23.49 | 30.06 | 26.76 | 22.36 | 23.14 |
| Qinghai | 17.73 | 18.75 | 18.75 | 16.73 | 19.24 | 15.79 | 15.28 | 19.31 | 17.66 | 13.54 | 15.66 |
| Ningxia | 29.60 | 26.06 | 25.86 | 24.82 | 26.06 | 22.06 | 21.98 | 27.32 | 24.58 | 22.68 | 23.08 |
| Xinjiang | 25.44 | 22.86 | 23.91 | 23.31 | 23.66 | 21.28 | 21.36 | 25.56 | 23.67 | 26.52 | 29.57 |
References
- Sarkodie, S.A.; Strezov, V.; Jiang, Y.J.; Evans, T. Proximate Determinants of Particulate Matter (PM2.5) Emission, Mortality and Life Expectancy in Europe, Central Asia, Australia, Canada and the US. Sci. Total Environ. 2019, 683, 489–497. [Google Scholar] [CrossRef] [PubMed]
- Cohen, G.; Gerber, Y. Air Pollution and Successful Aging: Recent Evidence and New Perspectives. Curr. Environ. Health Rep. 2017, 4, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Apte, J.S.; Brauer, M.; Cohen, A.J.; Ezzati, M.; Pope, C.A. Ambient PM2.5 Reduces Global and Regional Life Expectancy. Environ. Sci. Technol. Lett. 2018, 5, 546–551. [Google Scholar] [CrossRef]
- Liu, X.; Xu, Y.J.; Ge, Y.; Zhang, W.K.; Herrera, F. A Group Decision Making Approach Considering Self-Confidence Behaviors and Its Application in Environmental Pollution Emergency Management. Int. J. Environ. Res. Public Health 2019, 16, 385. [Google Scholar] [CrossRef]
- Zhang, W.K.; Du, J.; Tian, X.L. Finding a Promising Venture Capital Project with TODIM under Probabilistic Hesitant Fuzzy Circumstance. Technol. Econ. Dev. Econ. 2018, 24, 2026–2044. [Google Scholar] [CrossRef]
- Li, Y.; Chiu, Y.H.; Wang, L.H.; Liu, Y.C.; Chiu, C.R. A Comparative Study of Different Energy Efficiency of OECD and Non-OECD Countries. Trop. Conserv. Sci. 2019, 12, 1940082919837441. [Google Scholar] [CrossRef]
- Gu, H.J.; Cao, Y.X.; Ehan, E.; Sunil, K.J. Human Health Damages Related to Air Pollution in China. Environ. Sci. Pollut. Res. 2019, 26, 13115–13125. [Google Scholar] [CrossRef]
- Lin, Y.L.; Zou, J.L.; Yang, W.; Li, C.Q. A Review of Recent Advances in Research on PM2.5 in China. Int. J. Environ. Res. Public Health 2018, 15, 438. [Google Scholar] [CrossRef]
- Munir, S.; Habeebullah, T.M. Vehicular Emissions on Main Roads in Makkah, Saudi Arabiaa Dispersion Modelling Study. Arabian J. Geosci. 2018, 11, 531. [Google Scholar] [CrossRef]
- Zhang, S.; Li, Y.; Hao, Y.; Zhang, Y.P. Does Public Opinion Affect Air Quality? Evidence based on the Monthly Data of 109 Prefecture-Level Cities in China. Energy Policy 2018, 116, 299–311. [Google Scholar] [CrossRef]
- Gao, J.H.; Woodward, A.; Vardoulakis, S. Haze, Public Health and Mitigation Measures in China: A Review of the Current Evidence for Further Policy Response. Sci. Total Environ. 2017, 578, 148–157. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Li, J.; Zhu, G.; Yuan, Q. Spatio-Temporal Relationship and Evolvement of Socioeconomic Factors and PM2.5 in China During 1998–2016. Int. J. Environ. Res. Public Health 2019, 16, 1149. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zheng, C.; Ma, Z.; Quan, W. Acute and Cumulative Effects of Haze Fine Particles on Mortality and the Seasonal Characteristics in Beijing, China, 2005–2013: A Time-Stratified Case-Crossover Study. Int. J. Environ. Res. Public Health 2019, 16, 2383. [Google Scholar] [CrossRef] [PubMed]
- The State of China’s Ecological Environment in 2018. Available online: http://www.mee.gov.cn/home/jrtt1/201905/t20190529_704841.shtml (accessed on 17 August 2019).
- Li, Y.; Chiu, Y.H.; Lu, L.C. New Energy Development and Pollution Emissions in China. Int. J. Environ. Res. Public Health 2019, 16, 1764. [Google Scholar] [CrossRef]
- Chen, H.M.; Liu, J.; Li, Y.; Chiu, Y.H.; Lin, T.Y. A Two-stage Dynamic Undesirable Data Envelopment Analysis Model Focused on Media Reports and the Impact on Energy and Health Efficiency. Int. J. Environ. Res. Public Health 2019, 16, 1535. [Google Scholar] [CrossRef]
- Li, Y.; Chiu, Y.H.; Lu, L.C. Energy, CO2, AQI and Economic Performance in 31 Cities in China: A Slacks-Based Dynamic Data Envelopment Analysis. Carbon Manag. 2019, 10, 269–286. [Google Scholar] [CrossRef]
- Li, Y.; Chiu, Y.H.; Lin, T.Y. Research on New and Traditional Energy Sources in OECD Countries. Int. J. Environ. Res. Public Health 2019, 16, 1122. [Google Scholar] [CrossRef]
- National Bureau of Statistics of China. Available online: http://data.stats.gov.cn/easyquery.htm?cn = C01 (accessed on 19 August 2019).
- Lelieveld, J.; Evans, J.S.; Fnais, M.; Giannadaki, D.; Pozzer, A. The Contribution of Outdoor Air Pollution Sources to Premature Mortality on a Global Scale. Nature 2015, 525, 367–371. [Google Scholar] [CrossRef]
- Wu, Y.; Lu, B.; Zhu, X.L. Seasonal Variations, Source Apportionment, and Health Risk Assessment of Heavy Metals in PM2.5 in Ningbo, China. Aerosol Air Qual. Res. 2019, 19, 2083–2092. [Google Scholar] [CrossRef]
- Polezer, G.; Tadano, Y.S.; Siqueira, H.V. Assessing the Impact of PM2.5 on Respiratory Disease using Artificial Neural Networks. Environ. Pollut. 2018, 235, 394–403. [Google Scholar] [CrossRef]
- Andrea, R.V.L.; Yezid, R.R.N.; Camilo, B.B.L. Short-Term Effects of Air Pollution on Respiratory and Circulatory Morbidity in Colombia 2011–2014: A Multi-City, Time-Series Analysis. Int. J. Environ. Res. Public Health 2018, 15, 1610. [Google Scholar]
- Weber, S.A.; Insaf, T.Z.; Hall, E.S. Assessing the Impact of Fine Particulate Matter (PM2.5) on Respiratory-Cardiovascular Chronic Diseases in the New York City Metropolitan Area Using Hierarchical Bayesian Model Estimates. Environ. Res. 2016, 151, 399–409. [Google Scholar] [CrossRef] [PubMed]
- Cao, Q.L.; Rui, G.Q.; Liang, Y. Study on PM2.5 Pollution and the Mortality Due to Lung Cancer in China Based on Geographic Weighted Regression Model. BMC Public Health 2018, 18, 925. [Google Scholar] [CrossRef] [PubMed]
- De, M.A.; Amoatey, P.; Khaniabadi, Y.O. Mortality and Morbidity for Cardiopulmonary Diseases Attributed to PM2.5 Exposure in the Metropolis of Rome, Italy. Eur. J. Intern. Med. 2018, 57, 49–57. [Google Scholar]
- Badyda, A.J.; Grellier, J.D.P. Ambient PM2.5 Exposure and Mortality Due to Lung Cancer and Cardiopulmonary Diseases in Polish Cities. Adv. Exp. Med. Biol. 2017, 944, 9–17. [Google Scholar]
- Dabass, A.; Talbott, E.O.; Venkat, A.; Rager, J.; Marsh, G.M. Association of Exposure to Particulate Matter (PM2.5) Air Pollution and Biomarkers of Cardiovascular Disease Risk in Adult NHANES participants (2001–2008). Int. J. Hyg. Environ. Health 2016, 219, 301–310. [Google Scholar] [CrossRef]
- Chen, X.Z.; Zhang, W.K.; Yang, K.; Wang, L.L.; Liu, J.; Wang, L.; Hu, J.K.; Zhang, B.; Chen, Z.X.; Chen, J.P.; et al. Correlation between Serum CA724 and Gastric Cancer: Multiple Analyses based on Chinese Population. Mol. Biol. Rep. 2012, 39, 9031–9039. [Google Scholar] [CrossRef]
- De Grubb, M.C.M.; Kilbourne, B.; Kilbourne, K. Socioeconomic, Environmental, and Geographic Factors and US Lung Cancer Mortality, 1999–2009. Fam. Med. Community Health 2017, 5, 3–12. [Google Scholar] [CrossRef]
- Chen, J.C.; Wang, X.H.; Wellenius, G.A. Ambient Air Pollution and Neurotoxicity on Brain Structure: Evidence from Women’s Health Initiative Memory Study. Ann. Neurol. 2015, 78, 466–476. [Google Scholar] [CrossRef]
- Calderon, G.L.; Calderon, G.A.; Torres, J.R. Air Pollution and Your Brain: What do You Need to Know Right Now. Prim. Health Care Res. Dev. 2015, 16, 329–345. [Google Scholar] [CrossRef]
- Shin, J.; Han, S.H.; Choi, J. Exposure to Ambient Air Pollution and Cognitive Impairment in Community-Dwelling Older Adults: The Korean Frailty and Aging Cohort Study. Int. J. Environ. Res. Public Health 2019, 16, 3767. [Google Scholar] [CrossRef] [PubMed]
- Li, R.L.; Ho, Y.C.; Luo, C.W.; Lee, S.S.; Kuan, Y.H. Influence of PM2.5 Exposure Level on the Association between Alzheimer’s Disease and Allergic Rhinitis: A National Population-Based Cohort Study. Int. J. Environ. Res. Public Health 2019, 16, 3357. [Google Scholar] [CrossRef] [PubMed]
- Tran, B.L.; Chang, C.C.; Hsu, C.S.; Chen, C.C.; Tseng, W.C.; Hsu, S.H. Threshold Effects of PM2.5 Exposure on Particle-Related Mortality in China. Int. J. Environ. Res. Public Health 2019, 16, 3549. [Google Scholar] [CrossRef] [PubMed]
- Xia, Y.; Guan, D.B.; Jiang, X.J. Assessment of Socioeconomic Costs to China’s Air Pollution. Atmos. Environ. 2016, 139, 147–156. [Google Scholar] [CrossRef]
- Yang, Y.; Luo, L.W.; Song, C. Spatiotemporal Assessment of PM2.5-Related Economic Losses from Health Impacts during 2014–2016 in China. Int. J. Environ. Res. Public Health 2018, 15, 1278. [Google Scholar] [CrossRef] [PubMed]
- Miao, W.J.; Huang, X.; Song, Y. An Economic Assessment of the Health Effects and Crop Yield Losses Caused by Air Pollution in Mainland China. J. Environ. Sci. 2017, 56, 102–113. [Google Scholar] [CrossRef]
- Liu, Y.W.; Xie, S.G.; Yu, Q. Short-Term Effects of Ambient Air Pollution on Pediatric Outpatient Visits for Respiratory Diseases in Yichang City, China. Environ. Pollut. 2017, 227, 116–124. [Google Scholar] [CrossRef]
- Zeng, X.G.; Ruan, F.F.; Peng, Y.Y. Health Effects’ Spatial Distribution Analysis of PM2.5 Pollution in China Based on Spatial Grid Scale. China Environ. Sci. 2019, 39, 2624–2632. [Google Scholar]
- Sun, W.; Sun, J.Y. Daily PM2.5 Concentration Prediction based on Principal Component Analysis and LSSVM Optimized by Cuckoo Search Algorithm. J. Environ. Manag. 2017, 188, 144–152. [Google Scholar] [CrossRef]
- Tobler, W.R. A Computer Movie Simulating Urban Growth in the Detroit Region. Econ. Geogr. 1970, 46, 234–240. [Google Scholar] [CrossRef]
- Anselin, L.; Griffith, D.A. Do Spatial Effects Really Matter in Regression Analysis? Pap. Reg. Sci. 1988, 65, 1–34. [Google Scholar]
- Chen, X.Y.; Shao, S.; Tian, Z.H.; Xie, Z.; Yin, P. Impacts of Air Pollution and its Spatial Spillover Effect on Public Health Bbased on China’s Big Data Sample. J. Clean. Prod. 2017, 142, 915–925. [Google Scholar] [CrossRef]
- Shao, S.; Liu, A.J.; Yu, C.J.; Yang, H.J.; Li, H.; Li, B. Spatial Time-Frequency Distribution of Cross Term-Based Direction-of-Arrival Estimation for Weak Non-Stationary Signal. Eurasip J. Wirel. Commun. Netw. 2019, 2019, 1–12. [Google Scholar] [CrossRef]
- Cheng, Z.H.; Li, L.S.; Liu, J. Identifying the Spatial Effects and Driving Factors of Urban PM2.5 Pollution in China. Ecol. Indic. 2017, 82, 61–75. [Google Scholar] [CrossRef]
- Feng, Y.; Cheng, J.H.; Shen, J. Spatial Effects of Air Pollution on Public Health in China. Environ. Resour. Econ. 2019, 73, 229–250. [Google Scholar] [CrossRef]
- Li, G.Q.; He, R.W. PM2.5 Pollution and Health Spending: Temporal Lag Effects and Spatial Spillover Effects. J. Saf. Environ. 2019, 19, 326–336. (In Chinese) [Google Scholar]
- Columbia University Center for Socio-Economic Data and Applications. Available online: https://sedac.ciesin.columbia.edu/ (accessed on 20 July 2019).
- Chinese Health Statistics Yearbook 2008–2017. Available online: http://data.cnki.net/yearbook/Single/N2019030282/ (accessed on 23 July 2019).
- Chinese Health Statistics Yearbook 2008–2017. Available online: http://www.stats.gov.cn/tjsj/ndsj/ (accessed on 23 July 2019).
- Xie, Y.B.; Chen, J.; Li, W. An Assessment of PM2.5 Related Health Risks and Impaired Values of Beijing Residents in a Consecutive High-Level Exposure During Heavy Haze Days. Environ. Sci. 2014, 35, 1–8. [Google Scholar]
- Mu, Q.; Zhang, S.Q. An Evaluation of the Economic Loss Due to the Heavy Haze during January 2013 in China. China Environ. Sci. 2013, 33, 2087–2094. (In Chinese) [Google Scholar]
- Wei, G.R.; Shi, X.M. Evaluation the Extent of Health Damage Caused by PM2.5 Particulate in Xi’an City. Environ. Sci. 2018, 39, 3014–3021. (In Chinese) [Google Scholar]
- Yang, D.R.; Wang, H.X.; Lan, L.; Tao, Y.; Mi, S.Q. Evaluation of Economic Losses Due to Human Health Damage from Air Pollution before and after Energy Reform in Lanzhou. Environ. Eng. 2013, 31, 112–116. (In Chinese) [Google Scholar]
- Dong, Y.; Xu, G.Z.; Wang, A.H.; Lu, B.B. Evaluation of PM2.5 Air Pollution Impacts on the Public Health and Related Economic Loss in a City from 2014–2016. China Prev. Med. 2018, 19, 579–582. [Google Scholar]
- Cao, C.H.; Han, L.Y. The Assessment on the Social Health Costs Caused by Fog and Haze. Stat. Res. 2015, 32, 19–23. [Google Scholar]
- Shao, S.; Li, X.; Cao, J.H.; Yang, L.L. China’s Economic Policy Choices for Governing Smog Pollution Based on Spatial Spillover Effects. Econ. Res. 2016, 51, 73–88. [Google Scholar]
- Moran, P. Notes on Continuous Stochastic Phenomena. Biometrika 1950, 37, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Elhorst, J.P. Spatial Econometrics: From Cross-Sectional Data to Spatial Panels; Springer: Heidelberg, Germany, 2014. [Google Scholar]
- Anselin, L.; Arribas, B.D. Spatial Fixed Effects and Spatial Dependence in A Single Cross-Section. Pap. Reg. Sci. 2013, 37, 17–23. [Google Scholar] [CrossRef]
- Belotti, F.; Hughes, G.; Mortari, A.P. Spatial Panel-Data Models Using Stata. Stata J. 2017, 17, 139–180. [Google Scholar] [CrossRef]
- Qiu, Y.L.; Wang, Z.Q. The Forty Years Development of Medical Insurance System in China: Process, Experience and Prospect. J. Cent. China Norm. Univ. (Human. Soc. Sci.) 2019, 58, 23–30. (In Chinese) [Google Scholar]
- Getis, A.; Ord, J. The Analysis of Spatial Association by Use of Distance Statistics. Geogr. Anal. 1992, 24, 189–206. [Google Scholar] [CrossRef]
- Gan, W.Q.; Davies, H.W.; Koehoorn, M.; Brauer, M. Association of Long-Term Exposure to Community Noise and Traffic-Related Air Pollution with Coronary Heart Disease Mortality. Am. J. Epidemiol. 2012, 175, 898–906. [Google Scholar] [CrossRef]
- Heinrich, J.; Thiering, E.; Rzehak, P.; Krämer, U.; Hochadel, M.; Rauchfuss, K.M.; Gehring, U.; Wichmann, H. Long-Term Exposure to NO2 and PM10 and All-Cause and Cause−Specific Mortality in a Prospective Cohort of Women. Occup. Environ. Med. 2013, 70, 179–186. [Google Scholar] [CrossRef]
- Lanzinger, S.; Rosenbauer, J.; Sugiri, D. Impact of Long–Term Air Pollution Exposure on Metabolic Control in Children and Adolescents with Type 1 Diabetes: Results from the DPV Registry. Diabetologia 2018, 61, 1354–1361. [Google Scholar] [CrossRef] [PubMed]
- Kelejian, H.H.; Prucha, I.R.; Yuzefovich, Y. Instrumental Variable Estimation of a Spatial Autoregressive Model with Autoregressive Disturbances: Large and Small Sample Results. Spat. Spatiotemporal Econom. 2004, 18, 163–198. [Google Scholar]
- Yu, Y.Z.; Liu, D.Y. The Effect of the Space Outflow of China’s Regional Innovation and the Effect of the Outflow of Value Chanins: A Study, from the Perspective of the Innovative Value Chain, on the Model of the Panel of Multidimentsional Space. Manag. World 2013, 7, 6–20, 70, 187. (In Chinese) [Google Scholar]



| Type | Variable | Symbol | Definition |
|---|---|---|---|
| Dependent variable | Outpatient expense | exp_out | The ratio of the total outpatient expense to the total number of outpatient visits in the form of the natural logarithm |
| Outpatient visits | num_out | The ratio of the total number of outpatient visits to the total population in the form of the natural logarithm | |
| The number of hospitalization | num_hos | The ratio of the total number of hospitalization to the total population | |
| Independent variable | Maximum PM2.5 concentrations | PM2.5_max | The maximum values of PM2.5 concentrations in the form of natural logarithm |
| Maximum PM2.5 concentrations lag by one stage | PM2.5_max(−1) | The maximum values of the last year’s PM2.5 concentrations in the form of the natural logarithm | |
| Average PM2.5 concentrations | PM2.5_avg | The average values of PM2.5 concentrations in the form of the natural logarithm | |
| Average PM2.5 concentrations lag by one stage | PM2.5_avg(−1) | The average values of the last year’s PM2.5 concentrations in the form of natural logarithm | |
| Control variable | Per capita GDP | PGDP | The ratio of gross domestic product to the total population in the form of the natural logarithm |
| The ratio of urban population | urban | The ratio of the urban population to the total population | |
| The number of medical institutions | num_inst | The ratio of the total number of medical institutions to the total population in the form of the natural logarithm | |
| The number of hospital beds | num_bed | The ratio of the total number of hospital beds to the total population in the form of the natural logarithm | |
| The number of doctors | num_doctor | The ratio of the total number of doctors to the total population in the form of the natural logarithm |
| Variable | Obs | Mean | S.D. | Min | Median | Max |
|---|---|---|---|---|---|---|
| exp_out | 290 | 5.230 | 0.297 | 4.385 | 5.242 | 6.248 |
| num_out | 290 | 1.548 | 0.324 | 0.832 | 1.501 | 2.397 |
| num_hos | 290 | 0.125 | 0.043 | 0.039 | 0.126 | 0.224 |
| PM2.5_max | 290 | 3.847 | 0.413 | 2.605 | 3.903 | 4.575 |
| PM2.5_max(−1) | 290 | 3.841 | 0.414 | 2.605 | 3.897 | 4.575 |
| PM2.5_avg | 290 | 3.446 | 0.534 | 1.938 | 3.519 | 4.404 |
| PM2.5_avg(−1) | 290 | 3.422 | 0.549 | 1.938 | 3.488 | 4.404 |
| PGDP | 290 | 1.368 | 0.514 | −0.010 | 1.369 | 2.557 |
| urban | 290 | 0.548 | 0.134 | 0.291 | 0.530 | 0.896 |
| num_inst | 290 | 1.786 | 0.510 | 0.208 | 1.949 | 2.455 |
| num_bed | 290 | 3.773 | 0.236 | 3.140 | 3.802 | 4.227 |
| num_doctor | 290 | 4.293 | 0.198 | 3.689 | 4.310 | 4.978 |
| Name | Model | Selection Criteria | Chi-Square Value | p-Value |
|---|---|---|---|---|
| SAR | 32.32 | 0.0000 | ||
| SEM | 31.37 | 0.0000 | ||
| SDM |
| Year | exp_out | PM2.5_max | ||||
|---|---|---|---|---|---|---|
| W1 | W2 | W3 | W1 | W2 | W3 | |
| 2008 | 0.201 ** | 0.058 ** | 0.079 * | 0.527 *** | 0.238 *** | 0.097 * |
| 2009 | 0.278 *** | 0.167 *** | 0.307 *** | 0.519 *** | 0.243 *** | 0.091 * |
| 2010 | 0.270 *** | 0.168 *** | 0.296 *** | 0.514 *** | 0.233 *** | 0.080 |
| 2011 | 0.256 *** | 0.163 *** | 0.339 *** | 0.504 *** | 0.236 *** | 0.067 |
| 2012 | 0.227 *** | 0.149 *** | 0.310 *** | 0.511 *** | 0.225 *** | 0.038 |
| 2013 | 0.215 *** | 0.136 *** | 0.267 *** | 0.512 *** | 0.256 *** | 0.062 |
| 2014 | 0.197 *** | 0.122 *** | 0.254 *** | 0.542 *** | 0.242 *** | 0.064 |
| 2015 | 0.170 *** | 0.101 *** | 0.234 *** | 0.525 *** | 0.261 *** | 0.112 * |
| 2016 | 0.167 *** | 0.102 *** | 0.245 *** | 0.545 *** | 0.289 *** | 0.081 |
| 2017 | 0.163 ** | 0.091 *** | 0.245 *** | 0.468 *** | 0.239 *** | 0.099 * |
| Variable | Spatial Contiguity Matrix W1 | Spatial Distance Matrix W2 | Spatial Economy Matrix W3 | |||
|---|---|---|---|---|---|---|
| (1) | (2) | (3) | (4) | (5) | (6) | |
| PM2.5_max | 0.1017 *** | 0.1282 *** | 0.1773 *** | |||
| (2.79) | (4.41) | (8.58) | ||||
| PM2.5_max(−1) | 0.0971 *** | 0.1186 *** | 0.1713 *** | |||
| (2.65) | (4.16) | (8.34) | ||||
| PGDP | −0.2317 *** | −0.2323 *** | −0.3029 *** | −0.3097 *** | −0.1916 *** | −0.1975 *** |
| (−4.76) | (−4.76) | (−5.39) | (−5.51) | (−2.70) | (−2.77) | |
| urban | 1.3876 *** | 1.3840 *** | 1.7333 *** | 1.7686 *** | 1.2335 *** | 1.2656 *** |
| (7.32) | (7.30) | (10.04) | (10.22) | (6.86) | (7.03) | |
| num_inst | −0.0710 ** | −0.0717 ** | −0.0469 * | −0.0449 * | −0.0226 | −0.0191 |
| (−2.47) | (−2.49) | (−1.76) | (−1.68) | (−0.78) | (−0.66) | |
| num_bed | 0.4853 *** | 0.4929 *** | 0.3549 *** | 0.3659*** | 0.3868 *** | 0.3915 *** |
| (5.76) | (5.85) | (5.29) | (5.47) | (5.57) | (5.58) | |
| num_doctor | 0.0178 | 0.0118 | 0.1052 | 0.0887 | −0.0487 | −0.0556 |
| (0.23) | (0.15) | (1.26) | (1.06) | (−0.57) | (−0.64) | |
| W*PM2.5_max | 0.1531 *** | 0.4066 ** | 0.0106 | |||
| (2.76) | (2.12) | (0.17) | ||||
| W*PM2.5_max(−1) | 0.1551 *** | 0.4771 ** | 0.0012 | |||
| (2.78) | (2.55) | (0.02) | ||||
| W*PGDP | −0.4213 *** | −0.4178 *** | −1.4444 *** | −1.4888 *** | −0.0383 | −0.0382 |
| (−4.62) | (−4.58) | (−4.70) | (−4.84) | (−0.31) | (−0.31) | |
| W*urban | 2.7245 *** | 2.7882 *** | 5.4106 *** | 5.6841 *** | 0.7962 | 0.8438 * |
| (6.62) | (6.77) | (4.43) | (4.66) | (1.56) | (1.65) | |
| W*num_inst | 0.1294 * | 0.1458 ** | −0.3039 | −0.2645 | −0.3431 *** | −0.3369 *** |
| (1.87) | (2.08) | (−1.23) | (−1.07) | (−4.05) | (−3.95) | |
| W*num_bed | 0.3319 * | 0.3426 ** | 0.2244 | 0.3220 | −0.0646 | −0.0803 |
| (1.91) | (1.96) | (0.47) | (0.68) | (−0.30) | (−0.37) | |
| W*num_doctor | −0.7153 *** | −0.7542 *** | 0.0433 | −0.0844 | −0.0392 | −0.0449 |
| (−3.55) | (−3.71) | (0.08) | (−0.15) | (−0.15) | (−0.17) | |
| ρ | −0.1312 | −0.1230 | −0.7074 *** | −0.7217 *** | −0.2088 * | −0.2034 * |
| −1.49) | (−1.40) | (−2.95) | (−3.01) | (−1.78) | (−1.73) | |
| sigma2_e | 0.0122 *** | 0.0123 *** | 0.0118 *** | 0.0118 *** | 0.0123 *** | 0.0124 *** |
| (11.94) | (11.95) | (12.03) | (12.03) | (12.30) | (12.29) | |
| N | 290 | 290 | 290 | 290 | 290 | 290 |
| Type | Variable | Coefficient | t−Value | p−Value |
|---|---|---|---|---|
| Direct effects | PM2.5_max | 0.0987 ** | 2.55 | 0.011 |
| PM2.5_max(−1) | 0.0942 ** | 2.42 | 0.015 | |
| Spatial Spillover Effects | PM2.5_max | 0.1245 ** | 2.37 | 0.018 |
| PM2.5_max(−1) | 0.1283 ** | 2.42 | 0.016 | |
| Total Effects | PM2.5_max | 0.2232 *** | 7.11 | 0.000 |
| PM2.5_max(−1) | 0.2225 *** | 7.02 | 0.000 |
| Variable | Spatial Contiguity Matrix W1 | Spatial Distance Matrix W2 | Spatial Economy Matrix W3 | |||
|---|---|---|---|---|---|---|
| (1) | (2) | (3) | (4) | (5) | (6) | |
| PM2.5_max | 0.2114 *** | 0.3311 *** | 0.0070 | |||
| (4.10) | (8.56) | (0.24) | ||||
| PM2.5_max(−1) | 0.2154 *** | 0.3169 *** | 0.0178 | |||
| (4.16) | (8.22) | (0.61) | ||||
| PGDP | 0.1840 *** | 0.1874 *** | 0.3900 *** | 0.3944 *** | 0.3556 *** | 0.3569 *** |
| (2.74) | (2.79) | (5.25) | (5.23) | (3.50) | (3.52) | |
| urban | 0.6517 ** | 0.6314 ** | −0.4861 ** | −0.5139 ** | 0.2340 | 0.2304 |
| (2.54) | (2.46) | (−2.13) | (−2.22) | (0.90) | (0.90) | |
| num_inst | −0.0963 ** | −0.1007 ** | −0.2164 *** | −0.2206 *** | −0.1941 *** | −0.1933 *** |
| (−2.40) | (−2.52) | (−6.12) | (−6.16) | (−4.68) | (−4.68) | |
| num_bed | −0.7171 *** | −0.7150 *** | −0.6721 *** | −0.6841 *** | −0.4667 *** | −0.4541 *** |
| (−6.10) | (−6.09) | (−7.50) | (−7.54) | (−4.70) | (−4.57) | |
| num_doctor | 0.8027 *** | 0.8038 *** | 0.9740 *** | 0.9828 *** | 0.4070 *** | 0.3994 *** |
| (7.65) | (7.65) | (8.75) | (8.71) | (3.34) | (3.28) | |
| W*PM2.5_max | −0.3241 *** | −2.3216 *** | −0.2375 *** | |||
| (−4.33) | (−9.33) | (−2.66) | ||||
| W*PM2.5_max(−1) | −0.3232 *** | −2.1647 *** | −0.2460 *** | |||
| (−4.29) | (−8.76) | (−2.77) | ||||
| W*PGDP | −0.1371 | −0.1416 | 0.6240 | 0.6221 | −0.3989 ** | −0.3803 ** |
| (−1.11) | (−1.15) | (1.53) | (1.50) | (−2.21) | (−2.11) | |
| W*urban | −1.7539 *** | −1.7123 *** | −2.6430 | −2.9903 * | 1.9654 *** | 1.8389 *** |
| (−3.23) | (−3.16) | (−1.62) | (−1.83) | (2.78) | (2.61) | |
| W*num_inst | −0.5490 *** | −0.5367 *** | −0.8454 ** | −0.8419 ** | −0.3412 *** | −0.3607 *** |
| (−5.05) | (−4.90) | (−2.47) | (−2.42) | (−2.83) | (−2.99) | |
| W*num_bed | −0.1504 | −0.1298 | −3.0001 *** | −2.7721 *** | 0.3599 | 0.3428 |
| (−0.59) | (−0.51) | (−4.66) | (−4.27) | (1.17) | (1.12) | |
| W*num_doctor | 0.6217 ** | 0.5846 * | 2.2185 *** | 2.1068 *** | −1.2269 *** | −1.2073 *** |
| (1.96) | (1.83) | (2.89) | (2.69) | (−3.29) | (−3.26) | |
| ρ | 0.2720 *** | 0.2758 *** | 0.1090 | 0.1156 | −0.2840 ** | −0.2862 ** |
| (3.51) | (3.56) | (0.56) | (0.59) | (−2.36) | (−2.38) | |
| sigma2_e | 0.0238 *** | 0.0238 *** | 0.0208 *** | 0.0213 *** | 0.0252 *** | 0.0251 *** |
| (11.95) | (11.93) | (12.08) | (12.09) | (12.13) | (12.14) | |
| N | 290 | 290 | 290 | 290 | 290 | 290 |
| Type | Variable | Coefficient | t-Value | p-Value |
|---|---|---|---|---|
| Direct Effects | PM2.5_max | 0.1944 *** | 3.92 | 0.000 |
| PM2.5_max(−1) | 0.1984 *** | 3.99 | 0.000 | |
| Spatial Spillover Effects | PM2.5_max | −0.3516 *** | −4.09 | 0.000 |
| PM2.5_max(−1) | −0.3497 *** | −4.03 | 0.000 | |
| Total Effects | PM2.5_max | −0.1572 ** | −2.26 | 0.024 |
| PM2.5_max(−1) | −0.1513 ** | −2.16 | 0.031 |
| Variable | exp_out | exp_out | num_hos | num_hos | GMM | GMM |
|---|---|---|---|---|---|---|
| (1) | (2) | (3) | (4) | (5) | (6) | |
| PM2.5_max | 0.0335 *** | |||||
| (8.60) | ||||||
| PM2.5_max(−1) | 0.0329 *** | |||||
| (8.33) | ||||||
| PM2.5_avg | 0.0603 *** | |||||
| (3.16) | ||||||
| PM2.5_avg(−1) | 0.0607 *** | |||||
| (3.35) | ||||||
| PGDP | −0.3068 *** | −0.3404 *** | 0.0141 *** | 0.0143 *** | 1.3684 *** | 1.3684 *** |
| (−5.21) | (−5.81) | (2.73) | (2.76) | (45.35) | (45.35) | |
| urban | 1.7402 *** | 1.8307 *** | −0.0923 *** | −0.0956 *** | 0.5480 *** | 0.5480 *** |
| (9.64) | (10.21) | (−4.61) | (−4.74) | (69.55) | (69.55) | |
| num_inst | −0.0421 | −0.0398 | −0.0112 *** | −0.0119 *** | 1.7864 *** | 1.7864 *** |
| (−1.48) | (−1.42) | (−3.66) | (−3.86) | (59.62) | (59.62) | |
| num_bed | 0.3559 *** | 0.3656 *** | 0.0985 *** | 0.0997 *** | 3.7732 *** | 3.7732 *** |
| (5.36) | (5.23) | (11.01) | (11.07) | (271.75) | (271.75) | |
| num_doctor | 0.1363 | 0.1422 * | 0.0051 | 0.0053 | 4.2932 *** | 4.2932 *** |
| (1.55) | (1.64) | (0.63) | (0.65) | (370.05) | (370.05) | |
| W*PM2.5_max | −0.0484 *** | 3.8471 *** | ||||
| (−8.44) | (158.76) | |||||
| W*PM2.5_max(−1) | −0.0472 *** | 3.8407 *** | ||||
| (−8.11) | (157.95) | |||||
| W*PM2.5_avg | 0.2953 ** | |||||
| (2.18) | ||||||
| W*PM2.5_avg(−1) | 0.4607 *** | |||||
| (3.31) | ||||||
| W*PGDP | −1.3705 *** | −1.6526 *** | −0.0333 *** | −0.0341 *** | ||
| (−4.18) | (−4.94) | (−3.49) | (−3.55) | |||
| W*urban | 5.3744 *** | 5.8229 *** | 0.1284 *** | 0.1368 *** | ||
| (4.27) | (4.68) | (3.09) | (3.28) | |||
| W*num_inst | −0.3455 | −0.3123 | −0.0004 | 0.0010 | ||
| (−1.34) | (−1.23) | (−0.05) | (0.12) | |||
| W*num_bed | −0.3486 | −0.0944 | −0.0570 *** | −0.0556 *** | ||
| (−0.75) | (−0.20) | (−3.04) | (−2.92) | |||
| W*num_doctor | 0.4873 | 0.5663 | −0.0430 ** | −0.0472 ** | ||
| (0.83) | (0.97) | (−2.00) | (−2.17) | |||
| ρ | −0.5548 ** | −0.6443 *** | 0.6150 *** | 0.6131 *** | ||
| (−2.38) | (−2.72) | (11.86) | (11.75) | |||
| sigma2_e | 0.0132 *** | 0.0128 *** | 0.0001 *** | 0.0001 *** | ||
| (12.04) | (12.03) | (11.57) | (11.58) | |||
| N | 290 | 290 | 290 | 290 | 290 | 290 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zeng, M.; Du, J.; Zhang, W. Spatial-Temporal Effects of PM2.5 on Health Burden: Evidence from China. Int. J. Environ. Res. Public Health 2019, 16, 4695. https://doi.org/10.3390/ijerph16234695
Zeng M, Du J, Zhang W. Spatial-Temporal Effects of PM2.5 on Health Burden: Evidence from China. International Journal of Environmental Research and Public Health. 2019; 16(23):4695. https://doi.org/10.3390/ijerph16234695
Chicago/Turabian StyleZeng, Ming, Jiang Du, and Weike Zhang. 2019. "Spatial-Temporal Effects of PM2.5 on Health Burden: Evidence from China" International Journal of Environmental Research and Public Health 16, no. 23: 4695. https://doi.org/10.3390/ijerph16234695
APA StyleZeng, M., Du, J., & Zhang, W. (2019). Spatial-Temporal Effects of PM2.5 on Health Burden: Evidence from China. International Journal of Environmental Research and Public Health, 16(23), 4695. https://doi.org/10.3390/ijerph16234695