The Process of Constructing a Health Tourism Destination Index

Abstract
1. Introduction
2. Background Conceptions
2.1. Demarcation of Health Tourism
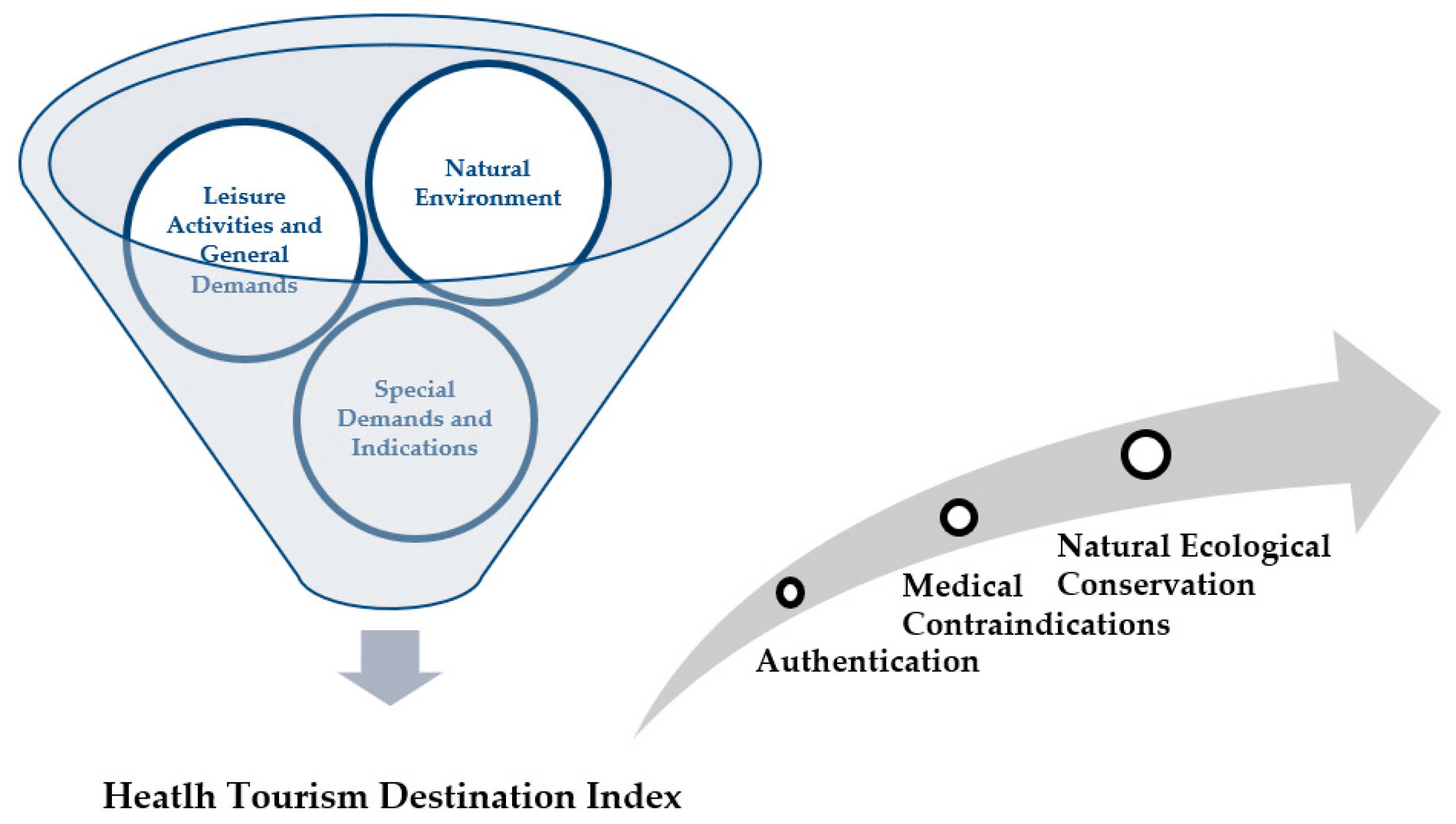
2.2. Measurement of the Health Tourism Destination Index
2.3. Activities in Health Tourism Destinations
2.3.1. Indicators of Leisure Activities and General Demand
2.3.2. Indicators of Special Demands and Indications
3. Methodology
4. Results and Discussion
5. Conclusions and Future Suggestions
5.1. Establishing the Reliability of the Health Tourism Destination Index
5.2. Strengthening Regional Advantages Using the Health Tourism Destination Index
Author Contributions
Acknowledgments
Conflicts of Interest
References
- The State Council. Healthy China 2030 Action (2019–2030). Available online: http://english.www.gov.cn/news/topnews/201908/09/content_WS5d4cc9e7c6d0c6695ff7e705.html (accessed on 1 November 2019).
- Yong, Z. To create a national sports and health city and promote national fitness. Sport 2017, 18, 3. [Google Scholar]
- WHO (World health Organization). Health Promotion. Available online: http://www.who.int/topics/ health_promotion/en/ (accessed on 1 November 2018).
- Wu, Z.; Guo, Q. Research on the development strategy of health tourism industry. Chin. J. Health Policy 2014, 7, 7–11. [Google Scholar]
- Kaplan, R.; Kaplan, S. The Experience of Nature: A Psychological Perspective; Cambridge University Press: New York, NY, USA, 1989. [Google Scholar]
- Nobuyuki, K. Introduction to Kurort; Shoshi Sai: Tokyo, Japan, 2012. [Google Scholar]
- Andergassen, R.; Candela, G.; Figini, P. An economic model for tourism destinations: Product sophistication and price coordination. Tour. Manag. 2013, 37, 86–98. [Google Scholar] [CrossRef]
- Zhang, S.; Wei, Z.; Liu, W.; Yao, L.; Suo, W.; Xing, J.; Huang, B.; Jin, D.; Wang, J. Indicators for Environment Health Risk Assessment in the Jiangsu Province of China. Int. J. Environ. Res. Public. Health 2015, 12, 11012–11024. [Google Scholar] [CrossRef]
- Alegre, J.; Garau, J. Tourist satisfaction and dissatisfaction. Ann. Tour. Res. 2010, 37, 52–73. [Google Scholar] [CrossRef]
- Žabkar, V.; Brenčič, M.M.; Dmitrović, T. Modelling perceived quality, visitor satisfaction and behavioural intentions at the destination level. Tour. Manag. 2010, 31, 537–546. [Google Scholar] [CrossRef]
- Zhang, H.; Gu, C.-L.; Gu, L.-W.; Zhang, Y. The evaluation of tourism destination competitiveness by TOPSIS & information entropy—A case in the Yangtze River Delta of China. Tour. Manag. 2011, 32, 443–451. [Google Scholar]
- Richards, G. Tourism attraction systems: Exploring cultural behavior. Ann. Tour. Res. 2002, 29, 1048–1064. [Google Scholar] [CrossRef]
- Sparks, B.; Bowen, J.; Klag, S. Restaurants and the tourist market. Int. J. Contemp. Hosp. Manag. 2003, 15, 6–13. [Google Scholar] [CrossRef]
- Cavlek, N. Tour operators and destination safety. Ann. Tour. Res. 2002, 29, 478–496. [Google Scholar] [CrossRef]
- Dwyer, L.; Mellor, R.; Livaic, Z.; Edwards, D.; Kim, C. Attributes of destination competitiveness: A factor analysis. Tour. Anal. 2004, 9, 91–101. [Google Scholar] [CrossRef]
- Crouch, G.I.; Ritchie, J.B. Application of the analytic hierarchy process to tourism choice and decision making: A review and illustration applied to destination competitiveness. Tour. Anal. 2005, 10, 17–25. [Google Scholar] [CrossRef]
- Mueller, H.; Kaufmann, E.L. Wellness Tourism: Market Analysis of a Special Health Tourism Segment and Implications for the Hotel Industry. J. Vacat. Mark. 2001, 7, 5–17. [Google Scholar] [CrossRef]
- Japanese Institute of Tourism Research. Handbook of Health Tourism; Japanese Institute of Tourism Research: Tokay, Japanese, 2010. [Google Scholar]
- Fetscherin, M.; Stephano, R.M. The medical tourism index: Scale develoment and validation. Tour. Manag. 2016, 52, 539–556. [Google Scholar] [CrossRef]
- Stavrovskaia, I.G.; Sirota, T.V.; Saakian, I.R. Optimization of energy-dependent processes in mitochondria from rat liver and brain after inhalation of negative air ions. Biofizika 1997, 43, 766–771. [Google Scholar]
- Chen, C. Study on the development strategy of state health tourism: Based on the perspectives of government, tourists, and residents. J. Huaihai Inst. Technol. 2018, 16, 99–102. [Google Scholar]
- Schlemmer, P.; Blank, C.; Schnitzer, M. Does physical activity during alpine vacations increase tourists’ well-being? Int. J. Environ. Res. Public Health 2019, 16, 1707. [Google Scholar] [CrossRef]
- Li, C. The Impacts of the Climate Change on Hiking Behaviors. Leis. Sport J. 2008, 7, 45–53. [Google Scholar]
- Environmental Protection Administration Executive Yuan. The Definition of Air Pollution Indicators. Available online: https://taqm.epa.gov.tw/taqm/en/b0201.aspx (accessed on 4 November 2019).
- Taiwan Centers for Disease Control. Travelers’ Health of Disease & Conditions. Available online: https://www.cdc.gov.tw/En/Category/ListPage/nbvOxj5T7SmkLuzFbc2Xfw (accessed on 4 November 2019).
- Central Weather Bureau. Air Concentration. Available online: https://www.cwb.gov.tw/V8/C/W/AtmosPollution.html (accessed on 4 November 2019).
- Environmental Protection Administration Executive Yuan. Standard of Drinking Water. Available online: https://oaout.epa.gov.tw/law/LawContent.aspx?id=FL015512 (accessed on 4 November 2019).
- Ministry of Internal Affairs and Communications. Hot Spring Act. Available online: https://elaws.e-gov.go.jp/search/elawsSearch/elaws_search/lsg0500/detail?lawId=323AC0000000125&openerCode=1 (accessed on 1 November 2019).
- Chen, J.B.; Ming, Q.Z.; Lou, S.Y.; Zhou, X.Q. Study on health tourism resources and development strategies in Mountainous Cities: A case study of Chongqing. J. Southwest China Norm. Univ. 2016, 41, 75–80. [Google Scholar]
- Zhang, N.; Tang, Z.; Zhu, D.P. Research on the innovation and development of health tourism in Heilongjiang Province. Foreign Econ. Relat. Trade 2017, 1, 58–60. [Google Scholar]
- Bell, P.A.; Greene, T.C.; Fisher, J.D.; Baum, A. Environmental Psychology, 5th ed.; Wadsworth Publishing: Singapore, 2005. [Google Scholar]
- Zhang, S.R.; Xiang, B.H.; Ju, H.R. Distribution characteristics and development strategy of air anion resources in Longsheng Autonomous County. J. Univ. Chin. Acad. Sci. 2016, 33, 365–372. [Google Scholar]
- Masanori, M. Health Tourism That Combines Travel, Leisure and Health; Square: Tokyo, Japan, 2005. [Google Scholar]
- Li, H.F.; Yang, X.Z.; Liu, H. Basic characteristics and development model of health tourism. J. West. Anhui Univ. 2017, 33, 122–127. [Google Scholar]
- Saaty, T.L. Decision making with the analytic hierarchy process. Int. J. Serv. Sci. 2008, 1, 83–98. [Google Scholar] [CrossRef]
- Chen, L.; Ng, E.; Huang, S.-C.; Fang, W.-T. A Self-Evaluation System of Quality Planning for Tourist Attractions in Taiwan: An Integrated AHP-Delphi Approach from Career Professionals. Sustainability 2017, 9, 1751. [Google Scholar] [CrossRef]
- Siomon, H.A. Administrative Behavior: A Study of Decision-Making Process in Administrative; The Free Press: New York, NY, USA, 1997. [Google Scholar]
- Jin, Y.; Kang, W.; Xue, Q.H. Review and Prospect of Chinese forest tourism research on improving Sub-Health. Tour. Res. 2013, 5, 15–20. [Google Scholar]
- Lipwoski, M.; Krokosz, D.; Lada, A.; Slizik, M. Sense of coherence and connectedness to nature as predictors of motivation for practicing Karate. Int. J. Environ. Res. Public. Health. 2019, 16, 2483. [Google Scholar] [CrossRef]
- Kotarska, K.; Noowak, L.; Szark-Eckardt, M.; Nowak, M. Selected Healthy behaviors and quality of life in people who practice combat sport and martial art. Int. J. Environ. Res. Public Health 2019, 16, 875. [Google Scholar] [CrossRef]
- Li, Q.; Morimoto, K. A forest bathing trip increases human natural killer activity and expression of anti-cancer proteins in female subjects. J. Biol. Regul. Homeost Agents 2008, 22, 45–55. [Google Scholar]



{kind=link}
{kind=link}
| Dimensions Level 1 | Level 1 Weight * | Sub-Dimensions Level 2 | Level 2 Weight * | Overall Weight * | Sort |
|---|---|---|---|---|---|
| Special Demands and Indications | 38.01 | Medical care | 27.69 | 10.53 | 6 |
| Health promotion | 39.04 | 14.84 | 1 | ||
| Tourism and leisure | 33.26 | 12.64 | 3 | ||
| Natural Environment | 29.75 | Climate | 26.34 | 7.84 | 7 |
| Air | 38.72 | 11.52 | 4 | ||
| Water | 23.49 | 6.99 | 8 | ||
| Light | 11.46 | 3.41 | 10 | ||
| Leisure Activates and General Demands | 32.24 | Sport | 33.38 | 10.76 | 5 |
| Therapeutic activities | 14.93 | 4.81 | 9 | ||
| Animals and Plants | 8.40 | 2.71 | 11 | ||
| Diet | 43.30 | 13.96 | 2 | ||
| Total | 100% | 100% | 100% |
| Dimensions Level 1 | Sub-Dimensions Level 2 | Officers Level 1 Weight | Officers Level 2 Weight | Officers Overall Weight | Sort | Scholars Level 1 Weight | Scholars Level 2 Weight | Scholars Overall Weight | Sort | Professionals Level 1 Weight * | Professionals Level 2 Weight * | Professionals Overall Weight * | Sort | MAD |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Special Demands and Indications | Medical care | 45.87 | 28.89 | 13.25 | 2 | 61.61 | 36.07 | 22.22 | 2 | 20.59 | 21.10 | 4.34 | 9 | 3.11 |
| Health promotion | 22.50 | 10.32 | 4 | 37.93 | 23.37 | 1 | 47.30 | 9.74 | 6 | 1.78 | ||||
| Tourism and leisure | 48.61 | 22.29 | 1 | 26.00 | 16.02 | 3 | 31.59 | 6.50 | 7 | 2.22 | ||||
| Natural Environment | Climate | 25.24 | 31.12 | 7.86 | 6 | 14.09 | 27.76 | 3.91 | 8 | 45.13 | 22.86 | 10.32 | 5 | 1.11 |
| Air | 42.18 | 7.77 | 7 | 42.18 | 5.95 | 6 | 39.56 | 17.85 | 1 | 2.44 | ||||
| Water | 17.63 | 6.73 | 8 | 17.63 | 2.48 | 9 | 27.44 | 12.38 | 4 | 2 | ||||
| Light | 12.43 | 2.88 | 11 | 12.43 | 1.75 | 11 | 10.14 | 4.58 | 8 | 1.33 | ||||
| Leisure Activities and General Demands | Sport | 28.89 | 28.39 | 8.2 | 5 | 24.30 | 20.53 | 4.99 | 7 | 34.28 | 45.21 | 15.5 | 2 | 1.78 |
| Therapeutic activities | 16.47 | 4.76 | 9 | 29.48 | 7.16 | 5 | 7.83 | 2.69 | 10 | 2 | ||||
| Animals and Plants | 13.14 | 3.8 | 10 | 7.73 | 1.88 | 10 | 6.54 | 2.24 | 11 | 0.44 | ||||
| Diet | 42.00 | 12.13 | 3 | 42.27 | 10.27 | 4 | 40.42 | 13.86 | 3 | 0.44 | ||||
| Total | 100% | 100% | 100% | 100% | 100% | 100% | 100% | 100% | 100% |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, C.-W.; Li, C. The Process of Constructing a Health Tourism Destination Index. Int. J. Environ. Res. Public Health 2019, 16, 4579. https://doi.org/10.3390/ijerph16224579
Lee C-W, Li C. The Process of Constructing a Health Tourism Destination Index. International Journal of Environmental Research and Public Health. 2019; 16(22):4579. https://doi.org/10.3390/ijerph16224579
Chicago/Turabian StyleLee, Chia-Wen, and Ching Li. 2019. "The Process of Constructing a Health Tourism Destination Index" International Journal of Environmental Research and Public Health 16, no. 22: 4579. https://doi.org/10.3390/ijerph16224579
APA StyleLee, C.-W., & Li, C. (2019). The Process of Constructing a Health Tourism Destination Index. International Journal of Environmental Research and Public Health, 16(22), 4579. https://doi.org/10.3390/ijerph16224579