Professional and Volunteer Refugee Aid Workers–Depressive Symptoms and Their Predictors, Experienced Traumatic Events, PTSD, Burdens, Engagement Motivators and Support Needs

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure and Setting
2.3. Measures
2.3.1. Sociodemographic, Migration-Specific and Aid Work related Variables
2.3.2. Traumatic Events and PTSD
2.3.3. Depressive Symptoms
2.3.4. Attitude Structure of Volunteers
2.4. Statistical Analysis
3. Results
3.1. Sociodemographics
3.2. Information on Refugee Work of the Study Sample
3.3. Motivation
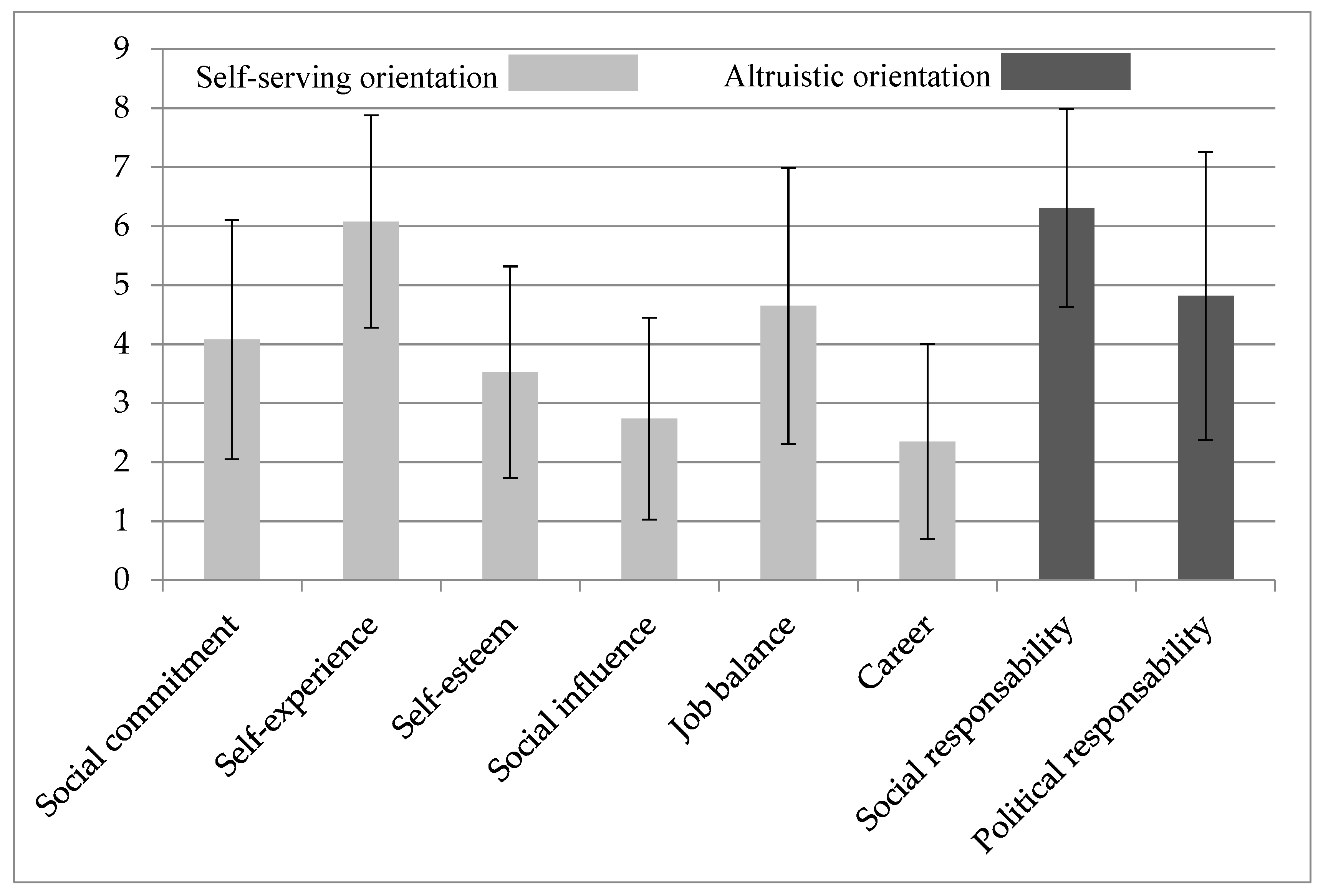
3.4. Specific Engagement Motivators of VAD
3.5. Burdens
3.6. Needs
3.7. Depressive Symptoms
3.8. Traumatic Events and PTSD
3.9. Predictors of Severity of Depressive Symptoms
4. Discussion
Strengths, Limitations and Implications for Policy and Practice
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- United Nations High Commissioner for Refugees (UNHCR). Global Trends—Forced Displacement in 2018. Available online: https://www.unhcr.org/5d08d7ee7.pdf (accessed on 15 October 2019).
- TNS Infratest Political Research. Voluntary Refugee Helpers in Germany. GESIS Datenarchiv 2017. [Google Scholar] [CrossRef]
- European Union, Eurostat. Asylum and First Time Asylum Applicants—Annual Aggregated Data (Rounded). Available online: http://appsso.eurostat.ec.europa.eu/nui/show.do?dataset=migr_asyappctza&lang=en (accessed on 20 September 2019).
- Federal Office for Migration and Refugees. Migrationreport 2015. Available online: https://www.bamf.de/SharedDocs/Anlagen/DE/Publikationen/Migrationsberichte/migrationsbericht-2015.pdf?__blob=publicationFile (accessed on 20 September 2019).
- Federal Office for Migration and Refugees. The Federal Office in Figures 2016: Asylum, Migration and Integration 2017. Available online: https://www.bamf.de/SharedDocs/Anlagen/DE/Publikationen/Broschueren/bundesamt-in-zahlen-2016.pdf?__blob=publicationFile (accessed on 20 September 2019).
- Federal Ministry for Family Affairs, Seniors, Women and Youth. Engagement in Refugee Aid. Available online: https://www.bmfsfj.de/blob/122010/d35ec9bf4a940ea49283485db4625aaf/engagement-in-der-fluechlingshilfe-data.pdf (accessed on 20 September 2019).
- Serhat Karakayali, J.O.K. EFA-Study 2: Structures and Motives of Voluntary Refugee Work in Germany, 2nd Research Report: Results of an Explorative Survey of November/December 2015; Berlin Institutes for Empirical Integration and Migration Research (BIM), Humboldt-Universität zu Berlin: Berlin, Germany, 2016. [Google Scholar]
- Krumpal, I. Determinants of social desirability bias in sensitive surveys: A literature review. Qual. Quant. 2013, 47, 2025–2047. [Google Scholar] [CrossRef]
- Jobst, E.; Gall, C.; Eiche, C.; Birkholz, T.; Prottengeier, J. Do good, stay well. Well-being and work satisfaction among German refugee helpers: A national cross-sectional study. PLoS ONE 2018, 13, e0209697. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, C.; King, R.; Chenoweth, L. Social work, stress and burnout: A review. J. Ment. Health 2002, 11, 255–266. [Google Scholar] [CrossRef]
- Blomberg, H.; Kallio, J.; Kroll, C.; Saarinen, A. Job Stress among Social Workers: Determinants and Attitude Effects in the Nordic Countries. Br. J. Soc. Work 2014, 45, 2089–2105. [Google Scholar] [CrossRef]
- Wirth, T.; Mette, J.; Prill, J.; Harth, V.; Nienhaus, A. Working conditions, mental health and coping of staff in social work with refugees and homeless individuals: A scoping review. Health Soc. Care Community 2019. [Google Scholar] [CrossRef]
- Guhan, R.; Liebling-Kalifani, H. The Experiences of Staff Working with Refugees and Asylum Seekers in the United Kingdom: A Grounded Theory Exploration. J. Immigr. Refug. Stud. 2011, 9, 205–228. [Google Scholar] [CrossRef]
- Kosny, A.A.; Eakin, J.M. The hazards of helping: Work, mission and risk in non-profit social service organizations. Health Risk Soc. 2008, 10, 149–166. [Google Scholar] [CrossRef]
- Figley, C.R. Compassion Fatigue as Secondary Traumatic Stress Disorder: An Overview. Available online: https://www.researchgate.net/publication/245720535_Compassion_fatigue_as_secondary_traumatic_stress_disorder_An_overview (accessed on 12 November 2019).
- Kim, Y.J. Secondary Traumatic Stress and Burnout of North Korean Refugees Service Providers. Psychiatry Investig. 2017, 14, 118–125. [Google Scholar] [CrossRef]
- Bride, B.E. Prevalence of secondary traumatic stress among social workers. Soc. Work 2007, 52, 63–70. [Google Scholar] [CrossRef]
- Georgiadou, E.; Zbidat, A.; Schmitt, G.M.; Erim, Y. Prevalence of Mental Distress Among Syrian Refugees With Residence Permission in Germany: A Registry-Based Study. Front. Psychiatry 2018, 9, 393. [Google Scholar] [CrossRef] [PubMed]
- Pell, M. Secondary Traumatisation of Helpers in Dealing with Traumatised Refugees. Master’s Thesis, University of Vienna, Vienna, Austria, 2013. [Google Scholar]
- Lindert, J.; von Ehrenstein, O.S.; Wehrwein, A.; Brähler, E.; Schafer, I. Anxiety, Depression and Posttraumatic Stress Disorder in Refugees—A Systematic Review. Psychother. Psychosom. Med. Psychol. 2018, 68, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Alpak, G.; Unal, A.; Bulbul, F.; Sagaltici, E.; Bez, Y.; Altindag, A.; Dalkilic, A.; Savas, H.A. Post-traumatic stress disorder among Syrian refugees in Turkey: A cross-sectional study. Int. J. Psychiatry Clin. Pract. 2015, 19, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Gammouh, O.S.; Al-Smadi, A.M.; Tawalbeh, L.I.; Khoury, L.S. Chronic diseases, lack of medications, and depression among Syrian refugees in Jordan, 2013–2014. Prev. Chronic Dis. 2015, 12, E10. [Google Scholar] [CrossRef] [PubMed]
- Slewa-Younan, S.; Uribe Guajardo, M.G.; Heriseanu, A.; Hasan, T. A Systematic Review of Post-traumatic Stress Disorder and Depression Amongst Iraqi Refugees Located in Western Countries. J. Immigr. Minority Health 2015, 17, 1231–1239. [Google Scholar] [CrossRef]
- Goldstein, R.B.; Smith, S.M.; Chou, S.P.; Saha, T.D.; Jung, J.; Zhang, H.; Pickering, R.P.; Ruan, W.J.; Huang, B.; Grant, B.F. The epidemiology of DSM-5 posttraumatic stress disorder in the United States: Results from the National Epidemiologic Survey on Alcohol and Related Conditions-III. Soc. Psychiatry Psychiatr. Epidemiol. 2016, 51, 1137–1148. [Google Scholar] [CrossRef]
- Strohmeier, H.; Scholte, W.F.; Ager, A. Factors associated with common mental health problems of humanitarian workers in South Sudan. PLoS ONE 2018, 13, e0205333. [Google Scholar] [CrossRef]
- Lusk, M.; Terrazas, S. Secondary Trauma Among Caregivers Who Work With Mexican and Central American Refugees. Hisp. J. Behav. Sci. 2015, 37, 257–273. [Google Scholar] [CrossRef]
- Birck, A. Secondary traumatization and burnout in professionals working with torture survivors. Traumatology 2001, 7, 85–90. [Google Scholar] [CrossRef]
- Collins, S.; Long, A. Working with the psychological effects of trauma: Consequences for mental health-care workers - a literature review. J. Psychiatr. Ment. Health Nurs. 2003, 10, 417–424. [Google Scholar] [CrossRef]
- Pross, C. Burnout, vicarious traumatization and its prevention. Torture Q. J. Rehabil. Torture Vict. Prev. Torture 2006, 16, 1–9. [Google Scholar]
- Grimm, T.; Georgiadou, E.; Silbermann, A.; Junker, K.; Nisslbeck, W.; Erim, Y. Distress, Main Burdens, Engagement Motivators and Needs of Fulltime and Volunteer Refugee Aid Workers. Psychother. Psychosom. Med. Psychol. 2017, 67, 345–351. [Google Scholar] [CrossRef] [PubMed]
- Federal Statistical Office. Population with Migration Background: Results of the Microcensus 2016. Available online: www.destatis.de/DE/Publikationen/Thematisch/Bevoelkerung/MigrationIntegration/Migrationshintergrund2010220167004.pdf?__blob=publicationFile (accessed on 20 September 2019).
- Tagay, S.; Erim, Y.; Möllering, A.; Stoelk, B.; Mewes, R.; Senf, W. The Essen Trauma-Inventory (ETI)—A screening instrument of identification of traumatic events and posttraumatic disorders. Psychother. Psychosom. Med. Psychol. 2007, 1, 75–89. [Google Scholar] [CrossRef][Green Version]
- Löwe, B.; Kroenke, K.; Herzog, W.; Grafe, K. Measuring depression outcome with a brief self-report instrument: Sensitivity to change of the Patient Health Questionnaire (PHQ-9). J. Affect. Disord. 2004, 81, 61–66. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Segal, D.L. Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR). In The Corsini Encyclopedia of Psychology; University of Colorado: Colorado Springs, CO, USA, 2010. [Google Scholar] [CrossRef]
- Gilbody, S.; Richards, D.; Brealey, S.; Hewitt, C. Screening for depression in medical settings with the Patient Health Questionnaire (PHQ): A diagnostic meta-analysis. J. Gen. Intern. Med. 2007, 22, 1596–1602. [Google Scholar] [CrossRef] [PubMed]
- Bierhoff, H.-W.; Schülken, T.; Hoof, M. Scales of the attitude structure of volunteers (SEEH). Z. Pers. 2007, 6, 12–27. [Google Scholar] [CrossRef]
- Federal Statistical Office. Educational Level. Available online: https://www.destatis.de/DE/Themen/Gesellschaft-Umwelt/Bildung-Forschung-Kultur/Bildungsstand/_inhalt.html (accessed on 20 September 2019).
- Federal Statistical Office. Population with Migration Background: Results of the Microcensus 2017. Available online: https://www.destatis.de/DE/Themen/Gesellschaft-Umwelt/Bevoelkerung/Migration-Integration/Publikationen/Downloads-Migration/migrationshintergrund-2010220177004.pdf?__blob=publicationFile&v=4 (accessed on 20 September 2019).
- Müller, D.; Hameister, N.; Lux, K. Initiation and motives for volunteering. In Volunteering in Germany: The German Volunteer Survey 2014; Simonson, J., Vogel, C., Tesch-Römer, C., Eds.; Springer Fachmedien Wiesbaden: Wiesbaden, Germany, 2017; pp. 413–435. [Google Scholar] [CrossRef]
- Robinson, K. Voices from the Front Line: Social Work with Refugees and Asylum Seekers in Australia and the UK. Br. J. Soc. Work 2013, 44, 1602–1620. [Google Scholar] [CrossRef]
- Busch, M.; Maske, U.; Ryl, L.; Schlack, R.; Hapke, U. Prevalence of Depressive Symptoms and Diagnosed Depression in Adults in Germany; Robert Koch-Institut, Epidemiologie und Gesundheitsberichterstattung: Berlin, Germany, 2013; Volume 56. [Google Scholar]
- Bretschneider, J.; Kuhnert, R.; Hapke, U. Depressive symptoms in adults in Germany. J. Health Monit. 2017, 2. [Google Scholar] [CrossRef]
- Cardozo, B.L.; Crawford, C.G.; Eriksson, C.; Zhu, J.; Sabin, M.; Ager, A.; Foy, D.; Snider, L.; Scholte, W.; Kaiser, R.; et al. Psychological distress, depression, anxiety, and burnout among international humanitarian aid workers: A longitudinal study. PLoS ONE 2012, 7, e44948. [Google Scholar] [CrossRef]
- Goodwin, R.D.; Gotlib, I.H. Gender differences in depression: The role of personality factors. Psychiatry Res. 2004, 126, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Siegrist, J.; Dragano, N. Psychosocial stress and disease risks in working life. Bundesgesundheitsblatt Gesundh. 2008, 51, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Jurado, D.; Alarcon, R.D.; Martinez-Ortega, J.M.; Mendieta-Marichal, Y.; Gutierrez-Rojas, L.; Gurpegui, M. Factors associated with psychological distress or common mental disorders in migrant populations across the world. Rev. De Psiquiatr. Y Salud Ment. 2017, 10, 45–58. [Google Scholar] [CrossRef] [PubMed]
- Hauffa, R.; Rief, W.; Brahler, E.; Martin, A.; Mewes, R.; Glaesmer, H. Lifetime traumatic experiences and posttraumatic stress disorder in the German population: Results of a representative population survey. J. Nerv. Ment. Dis. 2011, 199, 934–939. [Google Scholar] [CrossRef]
- Bustamante, L.H.U.; Cerqueira, R.O.; Leclerc, E.; Brietzke, E. Stress, trauma, and posttraumatic stress disorder in migrants: A comprehensive review. Braz. J. Psychiatry 2018, 40, 220–225. [Google Scholar] [CrossRef]
- Tagay, S.; Zararsiz, R.; Erim, Y.; Düllmann, S.; Schlegl, S.; Brähler, E.; Senf, W. Traumatic events and post-traumatic stress disorder in Turkish-speaking primary care patients. Psychother Psych. Med. 2008, 58, 155–161. [Google Scholar] [CrossRef]
- Maercker, A.; Forstmeier, S.; Wagner, B.; Glaesmer, H.; Brähler, E. Post-traumatic stress disorder in Germany. Results of a nationwide epidemiological study. Nervenarzt 2008, 79, 577–586. [Google Scholar] [CrossRef]
- Khantzian, E.J. The Self-Medication Hypothesis of Substance Use Disorders: A Reconsideration and Recent Applications. Harv. Rev. Psychiatry 1997, 4, 231–244. [Google Scholar] [CrossRef]
- Weiss, R.D.; Griffin, M.L.; Mirin, S.M. Drug Abuse as Self-Medication for Depression: An Empirical Study. Am. J. Drug Alcohol Abus. 1992, 18, 121–129. [Google Scholar] [CrossRef]
- International Organization for Migration (IOM). World Migration Report 2018. Available online: https://www.iom.int/sites/default/files/country/docs/china/r5_world_migration_report_2018_en.pdf (accessed on 20 September 2019).




{kind=link}
{kind=link}
{kind=link}
| Sociodemographic Variables | Total (N = 135) | VAD (n = 45) | PAD (n = 90) | p-Values | |
|---|---|---|---|---|---|
| Age | mean (SD) range | 44.1 (14.5) 19–80 | 48.2 (19.0) 19–80 | 42.2 (11.3) 23–71 | p = 0.060 a |
| N (%) | n (%) | n (%) | |||
| Gender | Male Female | 47 (34.6) 88 (65.4) | 14 (30.2) 31 (69.8) | 33 (36.7) 57 (63.3) | p = 0.523 b |
| Marital status | Single Married Divorced In a relationship | 32 (24.1) 56 (42.1) 19 (14.3) 26 (19.5) | 10 (22.7) 20 (45.5) 6 (13.6) 8 (18.2) | 22 (24.7) 36 (40.4) 13 (14.6) 18 (20.2) | p = 0.941 b |
| Education | Middle school or less High-school diploma University degree | 16 (11.9) 20 (14.8) 99 (73.3) | 8 (17.8) 12 (26.7) 25 (55.6) | 8 (8.9) 8 (8.9) 74 (82.2) | p = 0.004 b |
| Employment status | Full-time Part-time Unemployed (housewife, pensioner) School/University Studies | 70 (51.9) 33 (24.4) 19 (14.1) 13 (9.6) | 5 (11.1) 11 (24.4) 18 (40.1) 11 (24.4) | 65 (72.2) 22 (24.4) 1 (1.1) 2 (2.2) | p < 0.001 b |
| Religion | Roman-Catholic Protestant Muslim Other None | 37 (27.6) 53 (39.6) 7 (5.2) 8 (6.0) 29 (21.6) | 12 (27.3) 22 (48.9) 0 (0.0) 4 (9.1) 6 (13.6) | 25 (27.8) 31 (34.4) 7 (7.8) 4 (4.4) 23 (25.6) | p = 0.083 c |
| Migration background | Yes No | 39 (28.9) 96 (71.1) | 6 (13.3) 39 (86.7) | 33 (36.7) 57 (63.3) | p = 0.005 b |
| Refugee Work | Total (N = 135) | VAD (n = 45) | PAD (n = 90) | p-Values | |
|---|---|---|---|---|---|
| N (%) | n (%) | n (%) | |||
| Field of activity in refugee work | School a Daily support/care b Counseling c Interpreter Accomodation d Job centre/City council Medical supplies Therapeutic support e No data | 21 (15.6) 23 (17.0) 31 (23.0) 9 (6.7) 13 (9.6) 10 (7.4) 4 (3.0) 4 (3.0) 20 (14.8) | 1 (2.2) 20 (44.4) 7 (15.6) 3 (6.7) 2 (4.4) 0 (0) 2 (4.4) 1 (2.2) 9 (20.0) | 20 (22.2) 3 (3.3) 24 (26.7) 6 (6.7) 11 (12.2) 10 (11.2) 2 (2.2) 3 (3.3) 11 (12.2) | p = 0.131 |
| Weekly working hours f | mean (SD) range | 19.4 (17.1) 0–60 | 6.6 (9.7) 1–40 | 26.9 (16.0) 0–60 | p < 0.001 |
| Duration of refugee work g | mean (SD) range | 45.9 (82.8) 0.5–360 | 32.7 (54.7) 1–216 | 54.8 (96.9) 0.5–360 | p = 0.208 |
| Support Needs | Total (N = 135) | VAD (n = 45) | PAD (n = 90) | p-Values a |
|---|---|---|---|---|
| M (SD) | M (SD) | M (SD) | ||
| I want to learn how to take good care of myself in view of the stress in working with refugees. | 2.12 (1.07) | 2.16 (1.11) | 2.09 (1.07) | p = 0.787 |
| I would like to be able to help the refugees if they are obviously mentally distressed. | 1.48 (0.75) | 1.25 (0.44) | 1.60 (0.85) | p = 0.016 |
| I would like to recognize if a refugee has mental problems. | 1.30 (0.62) | 1.16 (0.53) | 1.38 (0.65) | p = 0.015 |
| I need information about possible trauma-related mental problems after traumatic experiences. | 1.60 (0.89) | 1.55 (0.86) | 1.62 (1.67) | p = 0.551 |
| I need information on dealing with possible complaints of trauma. | 1.63 (0.85) | 1.55 (0.82) | 1.67 (2.14) | p = 0.827 |
| I would like to learn more about the cultural background of refugees. | 2.00 (1.03) | 1.73 (0.82) | 2.14 (1.11) | p = 0.042 |
| I need psychosocial support because of the burdens of work with refugees. | 3.31 (1.23) | 3.63 (1.14) | 3.16 (1.25) | p = 0.037 |
| I need information about asylum law | 2.98 (1.27) | 3.12 (1.22) | 2.91 (1.30) | p = 0.371 |
| Personally and/or as Witness Experienced Traumatic Events | Total (N = 135) | VAD (n = 45) | PAD (n = 90) |
|---|---|---|---|
| N (%) | n (%) | n (%) | |
| War effort/Military conflict | 10 (7.4) | 2 (4.4) | 8 (9.0) |
| Prisoner/hostage | 7 (5.2) | 2 (4.4) | 5 (5.6) |
| Torture | 2 (1.5) | 1 (2.2) | 1 (1.1) |
| Physical violence (stranger) | 37 (27.4) | 10 (22.2) | 27 (30.3) |
| Physical violence (acquaintance) | 22 (16.3) | 7 (15.6) | 15 (16.7) |
| Death of loved one (e.g., homicide) | 45 (33.3) | 11 (24.4) | 34 (37.8) |
| Serious accident/explosion | 40 (29.6) | 13 (28.9) | 27 (30.7) |
| Serious illness | 88 (65.2) | 27 (60.0) | 61 (68.5) |
| Sexual harassment (stranger) | 3 (2.2) | 0 (0) | 3 (3.4) |
| Sexual harassment (acquaintance) | 4 (3.0) | 3 (6.7) | 1 (1.1) |
| Neglect | 23 (17.0) | 5 (11.1) | 18 (20.0) |
| Childhood sexual abuse (stranger) | 7 (5.2) | 4 (8.9) | 3 (3.4) |
| Childhood sexual abuse (acquaintance) | 7 (5.2) | 3 (6.7) | 4 (4.4) |
| Natural catastrophe | 35 (25.9) | 9 (20.0) | 26 (28.9) |
| Other trauma | 29 (21.5) | 12 (28.6) | 17 (20.7) |
| Predictors | B d | 95% CI e | SE f | β | p-Value |
|---|---|---|---|---|---|
| Sociodemographics | |||||
| Age | −0.041 | −0.087 to 0.006 | 0.023 | −0.160 | p = 0.084 |
| Gender a | 2.438 | 1.053 to 3.823 | 0.698 | 0.315 | p = 0.001 |
| Migration background b | 0.905 | −0.565 to 2.376 | 0.741 | 0.108 | p = 0.225 |
| Refugee work related variables | |||||
| Type of refugee aid worker (VAD or PAD) c | −1.278 | −2.738 to 0.182 | 0.736 | −0.165 | p = 0.086 |
| Weekly working hours (refugee work) | −0.121 | −0.257 to 0.014 | 0.066 | −0.425 | p = 0.078 |
| Duration of refugee work | −0.0061 | −0.029 to 0.018 | 0.011 | −0.081 | p = 0.620 |
| Burdens of refugee work | 0.480 | 0.188 to 0.773 | 0.148 | 0.294 | p = 0.002 |
| Amount of experienced traumatic events (ETI) | 0.698 | 0.335 to 1.062 | 0.183 | 0.357 | p < 0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borho, A.; Georgiadou, E.; Grimm, T.; Morawa, E.; Silbermann, A.; Nißlbeck, W.; Erim, Y. Professional and Volunteer Refugee Aid Workers–Depressive Symptoms and Their Predictors, Experienced Traumatic Events, PTSD, Burdens, Engagement Motivators and Support Needs. Int. J. Environ. Res. Public Health 2019, 16, 4542. https://doi.org/10.3390/ijerph16224542
Borho A, Georgiadou E, Grimm T, Morawa E, Silbermann A, Nißlbeck W, Erim Y. Professional and Volunteer Refugee Aid Workers–Depressive Symptoms and Their Predictors, Experienced Traumatic Events, PTSD, Burdens, Engagement Motivators and Support Needs. International Journal of Environmental Research and Public Health. 2019; 16(22):4542. https://doi.org/10.3390/ijerph16224542
Chicago/Turabian StyleBorho, Andrea, Ekaterini Georgiadou, Theresa Grimm, Eva Morawa, Andrea Silbermann, Winfried Nißlbeck, and Yesim Erim. 2019. "Professional and Volunteer Refugee Aid Workers–Depressive Symptoms and Their Predictors, Experienced Traumatic Events, PTSD, Burdens, Engagement Motivators and Support Needs" International Journal of Environmental Research and Public Health 16, no. 22: 4542. https://doi.org/10.3390/ijerph16224542
APA StyleBorho, A., Georgiadou, E., Grimm, T., Morawa, E., Silbermann, A., Nißlbeck, W., & Erim, Y. (2019). Professional and Volunteer Refugee Aid Workers–Depressive Symptoms and Their Predictors, Experienced Traumatic Events, PTSD, Burdens, Engagement Motivators and Support Needs. International Journal of Environmental Research and Public Health, 16(22), 4542. https://doi.org/10.3390/ijerph16224542