Risk Communication and Factors Influencing Private Well Testing Behavior: A Systematic Scoping Review

Abstract
1. Introduction
2. Materials and Methods
2.1. Text Selection
2.2. Data Extraction and Synthesis
3. Results
3.1. Overview of Studies
3.2. Empirical Studies of Risk Communication Effectiveness
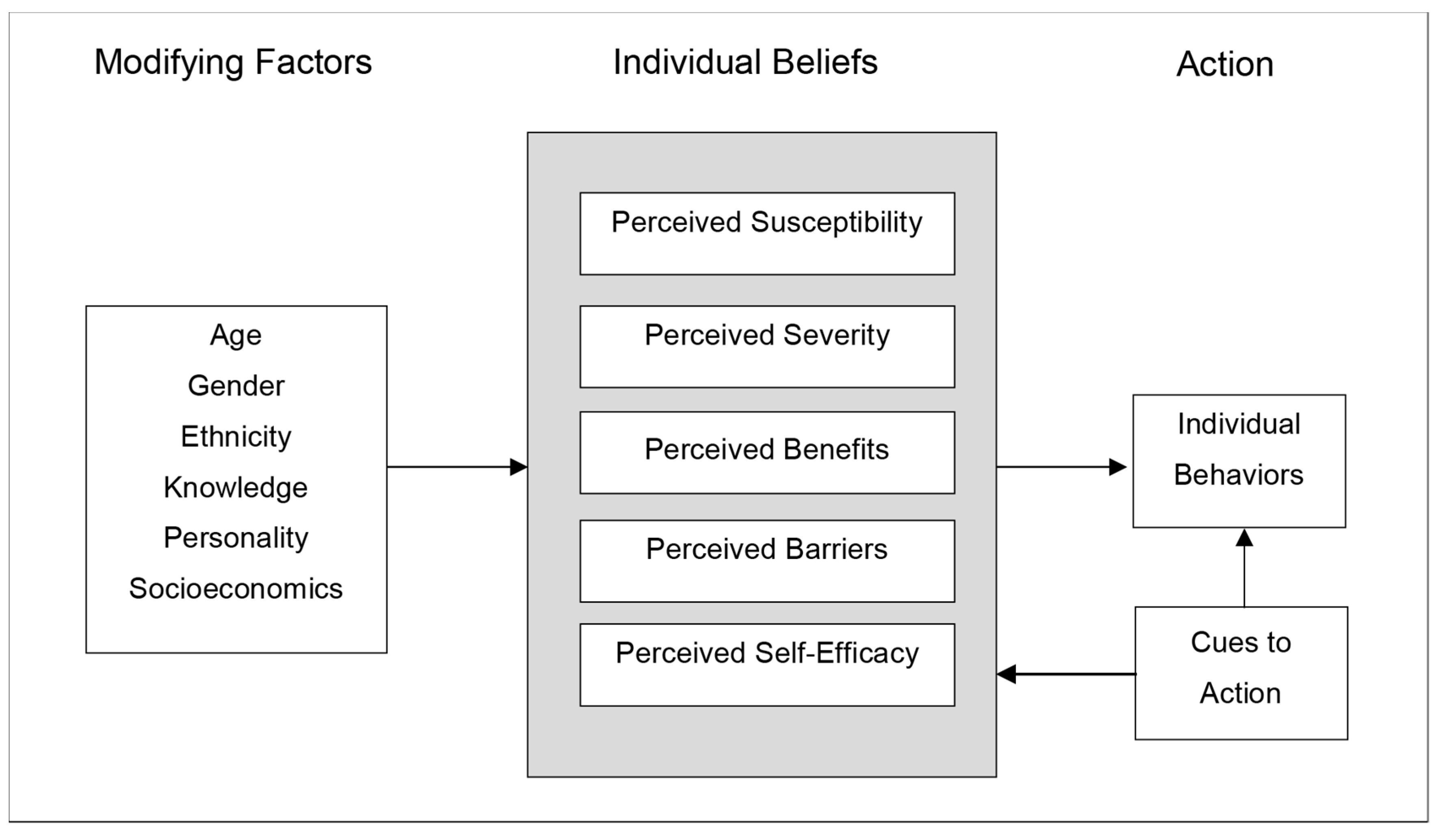
3.3. Factors Influencing Well Testing Behavior
3.3.1. Modifying Factors Associated with Well Testing Behavior
3.3.2. Individual Beliefs Associated with Well Testing Behavior
(i) Perceived Susceptibility
(ii) Perceived Severity
(iii) Perceived Benefits
(IV) Perceived Barriers
(V) Perceived Self-Efficacy
3.3.3. Cues to Action Associated with Well Testing Behavior
3.4. Risk of Bias
4. Discussion
4.1. Summary of Evidence
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Dieter, C.A.; Maupin, M.A.; Caldwell, R.R.; Harris, M.A.; Ivahnenko, T.I.; Lovelace, J.K.; Barber, N.L.; Linsey, K.S. Estimated Use of Water in the United States in 2015; U.S. Geological Survey Circular 1441; U.S. Geological Survey: Reston, VA, USA, 2018; p. 65.
- Government of Canada Be Well Aware—Information for Private Well Owners. Available online: https://www.canada.ca/en/health-canada/services/publications/healthy-living/water-talk-information-private-well-owners.html#targetText=About%203%20million%20people%20in,well%20for%20their%20drinking%20water (accessed on 30 August 2019).
- Centers for Disease Control and Prevention Overview of Water-related Diseases and Contaminants in Private Wells. Available online: https://www.cdc.gov/healthywater/drinking/private/wells/diseases.html (accessed on 30 August 2019).
- Centers for Disease Control and Prevention Well Siting & Potential Contaminants. Available online: https://www.cdc.gov/healthywater/drinking/private/wells/location.html (accessed on 30 August 2019).
- DeSimone, L.A.; Hamilton, P.A.; Gilliom, R.J. Quality of Water from Domestic Wells in Principal Aquifers of the United States, 1991–2004—Overview of Major Findings; U.S. Geological Survey Circular 1332; U.S. Geological Survey: Reston, VA, USA, 2009.
- Postma, J.; Butterfield, P.W.; Odom-Maryon, T.; Hill, W.; Butterfield, P.G. Rural children’s exposure to well water contaminants: Implications in light of the American Academy of Pediatrics’ recent policy statement. J. Am. Acad. Nurse Pract. 2011, 23, 258–265. [Google Scholar] [CrossRef]
- Villanueva, C.M.; Kogevinas, M.; Cordier, S.; Templeton, M.R.; Vermeulen, R.; Nuckols, J.R.; Nieuwenhuijsen, M.J.; Levallois, P. Assessing exposure and health consequences of chemicals in drinking water: Current state of knowledge and research needs. Environ. Health Perspect. 2014, 122, 213–221. [Google Scholar] [CrossRef]
- Malecki, K.M.C.; Schultz, A.A.; Severtson, D.J.; Anderson, H.A.; VanDerslice, J.A. Private-well stewardship among a general population based sample of private well-owners. Sci. Total Environ. 2017, 601–602, 1533–1543. [Google Scholar] [CrossRef]
- Kreutzwiser, R.; De Loë, R.; Imgrund, K.; Conboy, M.J.; Simpson, H.; Plummer, R. Understanding stewardship behaviour: Factors facilitating and constraining private water well stewardship. J. Environ. Manag. 2011, 92, 1104–1114. [Google Scholar] [CrossRef]
- Fizer, C.; de Bruin, W.B.; Stillo, F.; Gibson, J.M. Barriers to managing private wells and septic systems in underserved communities: Mental models of homeowner decision making. J. Environ. Health 2018, 81, 8–15. [Google Scholar]
- Lewandowski, A.M.; Montgomery, B.R.; Rosen, C.J.; Moncrief, J.F. Groundwater nitrate contamination costs: A survey of private well owners. J. Soil Water Conserv. 2008, 63, 153–161. [Google Scholar] [CrossRef]
- Chappells, H.; Campbell, N.; Drage, J.; Fernandez, C.V.; Parker, L.; Dummer, T.J.B. Understanding the translation of scientific knowledge about arsenic risk exposure among private well water users in Nova Scotia. Sci. Total Environ. 2015, 505, 1259–1273. [Google Scholar] [CrossRef]
- Clemens, S.; Swistock, B.R.; Sharpe, W.E. The Master Well Owner Network: Volunteers Educating Pennsylvania Well Owners. J. Ext. 2007, 45, 1–7. [Google Scholar]
- Swistock, B.R.; Clemens, S.; Sharpe, W.E.; Rummel, S. Water quality and management of private drinking water wells in Pennsylvania. J. Environ. Health 2013, 75, 60–66. [Google Scholar]
- Benham, B. What’s in Your Water? Development and Evaluation of the Virginia Household Water Quality Program and Virginia Master Well Owner Network. J. Human Sci. Ext. 2016, 4, 123–138. [Google Scholar]
- Lang, S.; Fewtrell, L.; Bartram, J. Risk Communication. In Water Quality Guidelines, Standards and Health: Assessment of Risk and Risk Management for Water-Related Infectious Disease; IWA Publishing on Behalf of the World Health Organization: London, UK, 2001; pp. 317–332. [Google Scholar]
- Rackelhoff-Dangel, C.; Petersen, D. Risk Communication in Action: The Risk Communication Workbook; U.S. Environmental Protection Agency, Office of Research and Development: Cincinnati, OH, USA, 2007.
- Glanz, K.; Rimer, B.; Viswanath, K. Health Behavior: Theory, Research and Practice, 5th ed.; Jossey-Bass: San Francisco, CA, USA, 2015. [Google Scholar]
- Morgan, M.G.; Fischhoff, B.; Bostrum, A.; Atman, C.J. Risk Communication: A Mental Models Approach, 1st ed.; Cambridge University Press: Cambridge, UK, 2002; ISBN 0-521-80223-7. [Google Scholar]
- Gerrard, M.; Gibbons, F.X.; Reis-Bergan, M. The effect of risk communication on risk perceptions: The significance of individual differences. J. Natl. Cancer Inst. Monogr. 1999, 1999, 94–100. [Google Scholar] [CrossRef] [PubMed]
- De Bruin, W.B.; Bostrom, A. Assessing what to address in science communication. Proc. Natl. Acad. Sci. USA 2013, 110, 14062–14068. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, N.D. Perceived probability, perceived severity, and health-protective behavior. Health Psychol. 2000, 19, 65–74. [Google Scholar] [CrossRef]
- Rosenstock, I.M. Historical Origins of the Health Belief Model. Health Educ. Monogr. 1978, 2, 328–335. [Google Scholar] [CrossRef]
- Jones, C.L.; Jensen, J.D.; Scherr, C.L.; Brown, N.R.; Christy, K.; Weaver, J. The Health Belief Model as an Explanatory Framework in Communication Research. Health Commun. 2015, 30, 566–576. [Google Scholar] [CrossRef]
- Straub, C.L.; Leahy, J.E. Application of a modified Health Belief Model to the pro-environmental behavior of private well water testing. J. Am. Water Resour. Assoc. 2014, 50, 1515–1526. [Google Scholar] [CrossRef]
- Janz, N.K.; Becker, M.H. The Health Belief Model: A Decade Later. Health Educ. Q. 1984, 11, 1–47. [Google Scholar] [CrossRef]
- Sohl, S.J.; Moyer, A. Tailored Interventions to Promote Mammography Screening: A Meta-Analytic Review. Prev. Med. 2007, 45, 252–261. [Google Scholar] [CrossRef]
- Morris, L.; Wilson, S.; Kelly, W. Methods of conducting effective outreach to private well owners—A literature review and model approach. J. Water Health 2016, 14, 167–182. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Phys. Ther. 2009, 89, 873–880. [Google Scholar]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- United Nations. World Economic Situation and Prospects Report; United Nations: New York, NY, USA, 2019. [Google Scholar]
- Hölzel, L.; Härter, M.; Reese, C.; Kriston, L. Risk factors for chronic depression—A systematic review. J. Affect. Disord. 2011, 129, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Lewis, J.J.; Pattanayak, S.K. Who Adopts Improved Fuels and Cookstoves? A Systematic Review. Environ. Health Perspect. 2012, 120, 637–645. [Google Scholar] [CrossRef] [PubMed]
- Flodgren, G.; Eccles, M.P.; Shepperd, S.; Scott, A.; Parmelli, E.; Beyer, F.R. An overview of reviews evaluating the effectiveness of financial incentives in changing healthcare professional behaviours and patient outcomes. Cochrane Database Syst. Rev. 2011. [Google Scholar] [CrossRef]
- Imgrund, K.; Kreutzwiser, R.; De Loë, R. Influences on the water testing behaviors of private well owners. J. Water Health 2011, 9, 241–252. [Google Scholar] [CrossRef]
- Paul, M.P.; Rigrod, P.; Wingate, S.; Borsuk, M.E. A Community-Driven Intervention in Tuftonboro, New Hampshire, Succeeds in Altering Water Testing Behavior. J. Environ. Health 2015, 78, 30–39. [Google Scholar]
- Jones, A.Q.; Dewey, C.E.; Doré, K.; Majowicz, S.E.; McEwen, S.A.; David, W.T.; Eric, M.; Carr, D.J.; Henson, S.J. Public perceptions of drinking water: A postal survey of residents with private water supplies. BMC Public Health 2006, 6, 94. [Google Scholar] [CrossRef]
- Jones, A.Q.; Dewey, C.E.; Doré, K.; Majowicz, S.E.; McEwen, S.A.; Waltner-Toews, D.; Henson, S.J.; Mathews, E. Public perception of drinking water from private water supplies: Focus group analyses. BMC Public Health 2005, 5, 129. [Google Scholar] [CrossRef]
- Iyengar, S.S.; Lepper, M.R. When choice is demotivating: Can one desire too much of a good thing? J. Pers. Soc. Psychol. 2000, 79, 995–1006. [Google Scholar] [CrossRef]
- Flanagan, S.V.; Spayd, S.E.; Procopio, N.A.; Marvinney, R.G.; Smith, A.E.; Chillrud, S.N.; Braman, S.; Zheng, Y. Arsenic in private well water part 3 of 3: Socioeconomic vulnerability to exposure in Maine and New Jersey. Sci. Total Environ. 2016, 562, 1019–1030. [Google Scholar] [CrossRef]
- Flanagan, S.V.; Marvinney, R.G.; Zheng, Y. Influences on domestic well water testing behavior in a Central Maine area with frequent groundwater arsenic occurrence. Sci. Total Environ. 2015, 505, 1274–1281. [Google Scholar] [CrossRef] [PubMed]
- Flanagan, S.V.; Spayd, S.E.; Procopio, N.A.; Chillrud, S.N.; Braman, S.; Zheng, Y. Arsenic in private well water part 1 of 3: Impact of the New Jersey Private Well Testing Act on household testing and mitigation behavior. Sci. Total Environ. 2016, 562, 999–1009. [Google Scholar] [CrossRef] [PubMed]
- Flanagan, S.V.; Spayd, S.E.; Procopio, N.A.; Chillrud, S.N.; Braman, S.; Zheng, Y. Arsenic in Private Well Water part 2 of 3: Who benefits the most from traditional testing promotion? Sci. Total Environ. 2016, 562, 1010–1018. [Google Scholar] [CrossRef] [PubMed]
- Rogan, W.J.; Brady, M.T. Drinking Water From Private Wells and Risks to Children. Pediatrics 2009, 123, 1599–1605. [Google Scholar] [CrossRef] [PubMed]
- Hexemer, A.M.; Pintar, K.; Bird, T.M.; Zentner, S.E.; Garcia, H.P.; Pollari, F. An investigation of bacteriological and chemical water quality and the barriers to private well water sampling in a Southwestern Ontario community. J. Water Health 2008, 6, 521–525. [Google Scholar] [CrossRef] [PubMed]
- Hoppe, B.O.; Harding, A.K.; Staab, J.; Counter, M. Private Well Testing in Oregon from Real Estate Transactions: An Innovative Approach toward a State-Based Surveillance System. Public Health Rep. 2011, 126, 107–115. [Google Scholar] [PubMed]
- Renaud, J.; Gagnon, F.; Michaud, C.; Boivin, S. Evaluation of the effectiveness of arsenic screening promotion in private wells: A quasi-experimental study. Health Promot. Int. 2011, 26, 465–475. [Google Scholar] [CrossRef]
- Carpenter, C.J. A Meta-Analysis of the Effectiveness of Health Belief Model Variables in Predicting Behavior. Health Commun. 2010, 25, 661–669. [Google Scholar] [CrossRef]
- Munene, A.; Hall, D.C. Factors influencing perceptions of private water quality in North America: A systematic review. Syst. Rev. 2019, 8, 111. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| “risk communication” OR “risk information” OR communication * OR promotion * OR education * OR outreach * OR “public relations” OR awareness OR campaign | |
| AND | “private well” OR “private wells” OR “well owners” OR “private well owners” OR “water wells” |
| AND | test OR tests OR testing |
| Inclusion Criteria | Exclusion Criteria | |
|---|---|---|
| 1. Language | English | Other |
| 2. Study Location | Developed country | Developing country |
| 3. (a) Intervention | Risk communication intended to encourage well testing behavior | Other |
| OR | OR | |
| (b) Factor | Factor that may influence well testing behavior | |
| 4. Publication Type | Peer-reviewed journal | Other |
| Author(s), Publication Year | Study Location(s) | Study Design | Total Sample Size * | Article Categorization | |
|---|---|---|---|---|---|
| Empirical Risk Communication Assessment | Factors Influencing Decisions to Test | ||||
| Chappells et al., 2015 | Nova Scotia, Canada | Observational (mail survey, interview analyses) | 420 | X | |
| Fizer et al., 2018 | North Carolina, USA | Observational (interview analyses) | 18 | X | |
| Flanagan et al., 2015 | Maine, USA | Observational (mail survey) | 525 | X | |
| Flanagan et al., 2016a | New Jersey, USA | Observational (mail survey) | 711 | X | |
| Flanagan et al., 2016b | New Jersey, U.S. | Observational (mail survey) | 670 | X | |
| Flanagan et al., 2016c | Maine, U.S.; New Jersey, USA. | Observational (mail survey) | 1287 | X | |
| Hexemer et al., 2008 | Ontario, Canada | Observational and Quasi-experimental (surveys and free well water tests) | 97 | X | |
| Hoppe et al., 2011 | Oregon, USA | Secondary Data Analysis | N/A ** | X | |
| Imgrund et al., 2011 | Ontario, Canada | Observational (interview analyses) | 22 | X | |
| Jones et al., 2005 | Ontario, Canada | Observational (focus group analyses) | 15 | X | |
| Jones et al., 2006 | Ontario, Canada | Observational (mail survey) | 246 | X | |
| Kreutzwiser et al., 2011 | Ontario, Canada | Observational (mail survey) | 1567 | X | |
| Lewandowski et al., 2008 | Minnesota, USA | Observational (telephone survey and water quality testing) | 483 | X | |
| Malecki et al., 2017 | Wisconsin, USA | Observational (mail survey) | 460 | X | |
| Paul et al., 2015 | New Hampshire, USA | Quasi-experimental | N/A | X | |
| Postma et al., 2011 | Montana, U.S.; Washington, USA | Observational (mail survey and water quality testing) | 188 | X | |
| Renaud et al., 2011 | Quebec, Canada | Quasi-experimental | 539 | X | X |
| Straub et al., 2014 | Connecticut; Rhode Island; Maine; New Hampshire; Vermont, USA | Observational (mail survey) | 714 | X | |
| Author, Year | N | Tested at Least Once for Any Analyte | Tests in Accordance with Local, State, or Provincial Recommendations or More Frequently | Tested for at Least One Analyte in Past 12 Months |
|---|---|---|---|---|
| Chappells, 2015 | 420 | 90% | 12% a | 4% a |
| Fizer, 2018 | 18 | 83% | <6% | <6% |
| Flanagan, 2015 | 419 | 78% | - | 10% |
| Flanagan, 2016a | 532 | 82% b | - | 15% b |
| Flanagan, 2016b | 670 | 82–83% c | - | - |
| Flanagan, 2016c | 972 | ~60–85% d | - | - |
| Hexemer, 2008 | 97 | - | - | 25% e |
| Hoppe, 2011 | N/A | - | - | - |
| Imgrund, 2011 | 22 | - | - | 59% |
| Jones, 2005 | 15 | - | Few f | Few f |
| Jones, 2006 | 239 | 79% | 31% | 23% |
| Kreutzwiser, 2011 | 1386 | 94% | - | 35% a |
| Lewandowski, 2008 | 483 | - | 29% | 10% |
| Malecki, 2017 | 460 | 48% | - | 19% a |
| Paul, 2015 | N/A | - | - | - |
| Postma, 2011 | 186 | 31% | - | - |
| Renaud, 2011 | 539 | - | - | - |
| Straub, 2014 | 714 | - | - | - |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colley, S.K.; Kane, P.K.M.; MacDonald Gibson, J. Risk Communication and Factors Influencing Private Well Testing Behavior: A Systematic Scoping Review. Int. J. Environ. Res. Public Health 2019, 16, 4333. https://doi.org/10.3390/ijerph16224333
Colley SK, Kane PKM, MacDonald Gibson J. Risk Communication and Factors Influencing Private Well Testing Behavior: A Systematic Scoping Review. International Journal of Environmental Research and Public Health. 2019; 16(22):4333. https://doi.org/10.3390/ijerph16224333
Chicago/Turabian StyleColley, Sarah K., Peter K.M. Kane, and Jacqueline MacDonald Gibson. 2019. "Risk Communication and Factors Influencing Private Well Testing Behavior: A Systematic Scoping Review" International Journal of Environmental Research and Public Health 16, no. 22: 4333. https://doi.org/10.3390/ijerph16224333
APA StyleColley, S. K., Kane, P. K. M., & MacDonald Gibson, J. (2019). Risk Communication and Factors Influencing Private Well Testing Behavior: A Systematic Scoping Review. International Journal of Environmental Research and Public Health, 16(22), 4333. https://doi.org/10.3390/ijerph16224333