Mediating Effect of Cognitive Social Capital on the Relationship Between Physical Disability and Depression in Elderly People of Rural Pakistan


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Measurement Variables
2.2.1. Depression
2.2.2. Physical Disability
2.2.3. Cognitive Social Capital
2.3. Analytical Techniques
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Vink, D.; Aartsen, M.J.; Schoevers, R.A. Risk factors for anxiety and depression in the elderly: A review. J. Affect. Disord. 2008, 106, 29–44. [Google Scholar] [CrossRef] [PubMed]
- Volkert, J.; Schulz, H.; Härter, M.; Wlodarczyk, O.; Andreas, S. The prevalence of mental disorders in older people in Western countries—A meta-analysis. Ageing Res. Rev. 2013, 12, 339–353. [Google Scholar] [CrossRef] [PubMed]
- De Silva, M.J.; McKenzie, K.; Harpham, T.; Huttly, S. Social capital and mental illness: A systematic review. J. Epidemiol. Community Health 2005, 59, 619–627. [Google Scholar] [CrossRef] [PubMed]
- Bassett, E.; Moore, S. Mental Health and Social Capital: Social Capital as a Promising Initiative to Improving the Mental Health of Communities. In Current Topics in Public Health; IntechOpen: London, UK, 2013. [Google Scholar]
- Wilson, K.C.M.; Taylor, S.; Copeland, J.R.M.; Chen, R.; McCracken, C.F.M. Socio-economic deprivation and the prevalence and prediction of depression in older community residents The MRC-ALPHA study. Br. J. Psychiatry 1999, 176, 549–553. [Google Scholar] [CrossRef] [PubMed]
- Murata, C.; Kondo, K.; Hirai, H.; Ichida, Y.; Ojima, T. Association between depression and socio-economic status among community-dwelling elderly in Japan: The Aichi Gerontological Evaluation Study (AGES). Health Place 2008, 14, 406–414. [Google Scholar] [CrossRef]
- Ashiq, U.; Amir, Z.A. The Rising Old Age Problem in Pakistan. J. Res. Soc. Pak. 2017, 54, 325–333. [Google Scholar]
- Javed, S.; Mustafa, N. Prevalence of Depression in various demographic variables among elderly. Open Access Sci. Rep. 2013, 2, 1–4. [Google Scholar]
- Zubair, B.U.; Mansoor, S. Prevalence of Depression and Associated Socio Demographic Factors in Elderly Rural Poplution. J. Pak. Psychiatr. Soc. 2015, 12, 19–22. [Google Scholar]
- Han, K.-M.; Han, C.; Shin, C.; Jee, H.-J.; An, H.; Yoon, H.-K.; Ko, Y.-H.; Kim, S.-H. Social capital, socioeconomic status, and depression in community-living elderly. J. Psychiatr. Res. 2018, 98, 133–140. [Google Scholar] [CrossRef]
- Xie, H.; Peng, W.; Yang, Y.; Zhang, D.; Sun, Y.; Wu, M.; Zhang, J.; Jia, J.; Su, Y. Social Support as a Mediator of Physical Disability and Depressive Symptoms in Chinese Elderly. Arch. Psychiatr. Nurs. 2018, 32, 256–262. [Google Scholar] [CrossRef]
- An, S.; Jang, Y. The role of social capital in the relationship between physical constraint and mental distress in older adults: A latent interaction model. Aging Ment. Health 2018, 22, 245–249. [Google Scholar] [CrossRef] [PubMed]
- Thompson, W.W.; Zack, M.M.; Krahn, G.L.; Andresen, E.M.; Barile, J.P. Health-Related Quality of Life Among Older Adults with and Without Functional Limitations. Am. J. Public Health 2012, 102, 496–502. [Google Scholar] [CrossRef] [PubMed]
- Jang, Y.; Haley, W.E.; Small, B.J.; Mortimer, J.A. The Role of Mastery and Social Resources in the Associations Between Disability and Depression in Later Life for a comprehensive review on late-life disability and de-pression. Gerontologist 2002, 42, 807–813. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, J.K.; Walker, K.L.; Chang, E.C.; Lyness, J.M. Illness burden and symptoms of anxiety in older adults: Optimism and pessimism as moderators. Int. Psychogeriatr. 2012, 24, 1674–1683. [Google Scholar] [CrossRef] [PubMed]
- Paukert, A.L.; Pettit, J.W.; Kunik, M.E.; Wilson, N.; Novy, D.M.; Rhoades, H.M.; Greisinger, A.J.; Wehmanen, O.A.; Stanley, M.A. The roles of social support and self-efficacy in physical health’s impact on depressive and anxiety symptoms in older adults. J. Clin. Psychol. Med. Settings 2010, 17, 387–400. [Google Scholar] [CrossRef]
- Bozo, Ö.; Toksabay, N.E.; Kürüm, O. Activities of Daily Living, Depression, and Social Support Among Elderly Turkish People. J. Psychol. Interdiscip. Appl. 2009, 143, 193–206. [Google Scholar] [CrossRef]
- Sartorius, N. Social capital and mental health. Curr. Opin. Psychiatry 2003, 16 (Suppl. 2), 280–283. [Google Scholar] [CrossRef]
- Morgan, C.; Bhugra, D. Principles of Social Psychiatry; John Wiley & Sons: New York, NY, USA, 2010. [Google Scholar]
- Uphoff, E.P.; Pickett, K.E.; Cabieses, B.; Small, N.; Wright, J. A systematic review of the relationships between social capital and socioeconomic inequalities in health: A contribution to understanding the psychosocial pathway of health inequalities. Int. J. Equity Health 2013, 12, 54. [Google Scholar] [CrossRef]
- Bassett, E.; Moore, S. Social capital and depressive symptoms: The association of psychosocial and network dimensions of social capital with depressive symptoms in Montreal, Canada. Soc. Sci. Med. 2013, 86, 96–102. [Google Scholar] [CrossRef]
- Han, S.; Lee, H.S. Social capital and depression: Does household context matter? Asia Pac. J. Public Health 2015, 27, NP2008–NP2018. [Google Scholar] [CrossRef]
- Wilmot, N.A.; Dauner, K.N. Examination of the influence of social capital on depression in fragile families. J. Epidemiol. Community Health 2017, 71, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Aihara, Y.; Minai, J.; Kikuchi, Y.; Aoyama, A.; Shimanouchi, S. Cognition of Social Capital in Older Japanese Men and Women. J. Aging Health 2009, 21, 1083–1097. [Google Scholar] [CrossRef] [PubMed]
- Lu, N.; Jiang, N.; Lou, V.W.Q.; Zeng, Y.; Liu, M. Does Gender Moderate the Relationship Between Social Capital and Life Satisfaction? Evidence From Urban China. Res. Aging 2018, 40, 740–761. [Google Scholar] [CrossRef] [PubMed]
- Imamura, H.; Hamano, T.; Michikawa, T.; Takeda-Imai, F.; Nakamura, T.; Takebayashi, T.; Nishiwaki, Y. Relationships of Community and Individual Level Social Capital with Activities of Daily Living and Death by Gender. Int. J. Environ. Res. Public Health 2016, 13, 860. [Google Scholar] [CrossRef]
- Liotta, G.; Inzerilli, M.C.; Palombi, L.; Madaro, O.; Orlando, S.; Scarcella, P.; Betti, D.; Marazzi, M.C. Social Interventions to Prevent Heat-Related Mortality in the Older Adult in Rome, Italy: A Quasi-Experimental Study. Int. J. Environ. Res. Public Health 2018, 15, 715. [Google Scholar] [CrossRef]
- Goth, U.S.; Småland, E. The Role of Civic Engagement for Men’s Health and Well Being in Norway—A Contribution to Public Health. Int. J. Environ. Res. Public Health 2014, 11, 6375–6387. [Google Scholar] [CrossRef]
- Agampodi, T.C.; Agampodi, S.B.; Glozier, N.; Siribaddana, S. Measurement of social capital in relation to health in low and middle income countries (LMIC): A systematic review. Soc. Sci. Med. 2015, 128, 95–104. [Google Scholar] [CrossRef]
- Kawachi, I.; Berkman, L.F. [Overview/theory] Social Ties and Mental Health. J. Urban Health Bull. N. Y. Acad. Med. 2001, 78, 458–467. [Google Scholar] [CrossRef]
- Kim, S.-S.; Chung, Y.; Perry, M.J.; Kawachi, I.; Subramanian, S.V. Association between Interpersonal Trust, Reciprocity, and Depression in South Korea: A Prospective Analysis. PLoS ONE 2012, 7, e30602. [Google Scholar] [CrossRef]
- Fujiwara, T.; Kawachi, I. A prospective study of individual-level social capital and major depression in the United States. J. Epidemiol. Community Health 2008, 62, 627–633. [Google Scholar] [CrossRef]
- Vanderhorst, R.K.; McLaren, S. Social relationships as predictors of depression and suicidal ideation in older adults. Aging Ment. Health 2005, 9, 517–525. [Google Scholar] [CrossRef] [PubMed]
- Nyqvist, F.; Gustavsson, J.; Gustafson, Y. Social Capital and Health in the Oldest Old: The Umeå 85+ Study. Int. J. Ageing Later Life 2006, 1, 91–114. [Google Scholar] [CrossRef]
- Verbrugge, L.M.; Jette, A.M. The disablement process. Soc. Sci. Med. 1994, 38, 1–14. [Google Scholar] [CrossRef]
- Sheikh, J.I.; Yesavage, J.A. Geriatric Depression Scale (GDS) Jerome. Clin. Gerontol. 1986, 5, 165–173. [Google Scholar]
- Taqui, A.M.; Itrat, A.; Qidwai, W.; Qadri, Z. Depression in the elderly: Does family system play a role? A cross-sectional study. BMC Psychiatry 2007, 7, 57. [Google Scholar] [CrossRef] [PubMed]
- Katz, S.; Ford, A.B.; Moskowitz, R.W.; Jackson, B.A.; Jaffe, M.W. Studies of Illness in the Aged The Index of ADL: A Standardized Measure of Biological and Psychosocial Function. JAMA 1963, 185, 914–919. [Google Scholar] [CrossRef] [PubMed]
- Lawton, M.P.; Brody, E.M. Assessment of Older People: Self-Maintaining and Instrumental Activities of Daily Living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis; The Guilford Press: New York, NY, USA, 2013. [Google Scholar]
- Vyncke, V.; De Clercq, B.; Stevens, V.; Costongs, C.; Barbareschi, G.; Jónsson, S.H.; Curvo, S.D.; Kebza, V.; Currie, C.; Maes, L. Does neighbourhood social capital aid in levelling the social gradient in the health and well-being of children and adolescents? A literature review. BMC Public Health 2013, 13, 65. [Google Scholar] [CrossRef]
- Mancini, A.D.; Bonanno, G.A. Marital closeness, functional disability, and adjustment in late life. Psychol. Aging 2006, 21, 600–610. [Google Scholar] [CrossRef]
- Verbrugge, L.M.; Patrick, D.L. Seven chronic conditions: Their impact on US adults’ activity levels and use of medical services. Am. J. Public Health 1995, 85, 173–182. [Google Scholar] [CrossRef]
- Eide, A.H.; Roysamb, E. The relationship between level of disability, psychological problems, social activity, and social networks. Rehabil. Psychol. 2002, 47, 165–183. [Google Scholar] [CrossRef]
- Cao, W.; Li, L.; Zhou, X.; Zhou, C. Aging & Mental Health Social capital and depression: Evidence from urban elderly in China. Aging Ment. Health 2014, 19, 418–429. [Google Scholar] [PubMed]
- Ehsan, A.M.; De Silva, M.J. Social capital and common mental disorder: A systematic review. J. Epidemiol. Community Health 2015, 69, 1021–1028. [Google Scholar] [CrossRef] [PubMed]
- Forsman, A.; Nyqvist, F.; Schierenbeck, I.; Gustafson, Y.; Wahlbeck, K. Structural and cognitive social capital and depression among older adults in two Nordic regions. Aging Ment. Health 2012, 16, 771–779. [Google Scholar] [CrossRef]
- Forsman, A.K.; Nyqvist, F.; Wahlbeck, K. Cognitive components of social capital and mental health status among older adults: A population-based cross-sectional study. Scand. J. Public Health 2011, 39, 757–765. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Socio-Demographic Variables | No. | Percentage (%) | Depression | F | p |
|---|---|---|---|---|---|
| Gender Male Female | 106 40 | 72.6 27.3 | 8.10 ± 3.43 7.77 ± 3.48 | 0.264 | 0.608 |
| Age (Years) 60–69 70–79 80–89 ≥90 | 49 47 28 22 | 33.5 32.1 19.1 15.0 | 7.46 ± 3.06 8.51 ± 3.85 7.64 ± 3.45 8.63 ± 3.23 | 1.086 | 0.357 |
| Level of education Illiterate Primary (5 Years) Middle (8 Years) ≥High school | 69 26 26 25 | 47.2 17.8 17.8 17.1 | 7.23 ± 3.50 9.57 ± 2.91 8.30 ± 3.10 8.24 ± 3.63 | 3.218 | 0.025 |
| Marital status Single Married Divorced/Widowed | 34 75 38 | 23.2 51.3 26.0 | 8.76 ± 3.46 7.20 ± 3.29 8.92 ± 3.40 | 4.384 | 0.014 |
| Family system Joint family Nuclear family | 92 54 | 63.0 36.9 | 7.58 ± 3.29 8.74 ± 3.58 | 3.904 | 0.050 |
| Living status Living with a spouse Living with Others (Son or relatives) | 68 78 | 46.5 53.4 | 8.80 ± 3.51 7.32 ± 3.24 | 7.085 | 0.009 |
| Average monthly income (PKR) ≤15,000 15,001–30,000 >30,000 | 63 58 25 | 43.1 39.7 17.1 | 7.87 ± 3.52 8.72 ± 3.29 6.72 ± 3.27 | 3.184 | 0.046 |
| No. of chronic diseases 1 2 3 | 62 59 25 | 42.4 40.4 17.1 | 7.00 ± 3.46 8.64 ± 3.27 9.04 ± 3.22 | 5.064 | 0.008 |
| Variables | Range | Mean | SD | Interpersonal Trust | Reciprocity | Depressive Symptoms |
|---|---|---|---|---|---|---|
| Physical disability | 14~56 | 23.58 | 8.91 | −0.012 | −0.218 ** | 0.249 ** |
| Interpersonal trust | 1~3 | 1.50 | 0.61 | - | 0.011 | −0.196 * |
| Reciprocity | 1~3 | 1.69 | 0.83 | - | - | −0.251 ** |
| Depressive symptoms | 1~14 | 8.01 | 3.44 | - | - | - |
| Dependent Variable: Depression | Unstandardized Coefficient | Standardized Coefficient |
|---|---|---|
| B (SE) | β | |
| level of Education (Ref. = Illiterate) Primary (5 Years) Middle (8 Years) ≥High school | 1.819 (0.695) 0.988 (0.675) 1.615 (0.703) | 0.203 ** 0.110 0.177 * |
| Marital status (Ref. = Single) Married Divorced/Widowed | −0.606 (0.623) 0.507 (0.705) | −0.088 0.065 |
| Family system | 0.951 (0.510) | 0.134 |
| Living status | −1.082 (0.504) | −0.157 * |
| Average monthly income (PKR) (Ref. ≤15,000) 15,001–30,000 >30,000 | 0.871 (0.545) −0.677 (0.707) | 0.124 −0.074 |
| No. of chronic diseases (Ref. = 1) 2 3 | 1.222 (0.545) 1.698 (0.701) | 0.175 * 0.187 * |
| Physical disability | 0.087 (0.028) | 0.225 ** |
| Interpersonal trust | −0.924 (0.396) | −0.165 * |
| Reciprocity | −1.087 (0.296) | −0.264 ** |
| R2 F | 0.380 5.738 ** |
| Variables | B (SE) | LLCI | ULCI |
|---|---|---|---|
| Outcome: Depressive symptoms | |||
| Physical disability | 0.097 ** (0.029) | 0.037 | 0.156 |
| Average monthly income (PKR) (Ref. ≤15,000) | |||
| 15,001–30,000 | 0.972 (0.584) | −0.182 | 2.127 |
| >30,000 | −1.224 (0.758) | −2.723 | 0.274 |
| Living status | −1.484 ** (0.533) | −2.538 | −0.431 |
| R2 F | 0.155 6.510* | ||
| Outcome: Depressive symptoms | |||
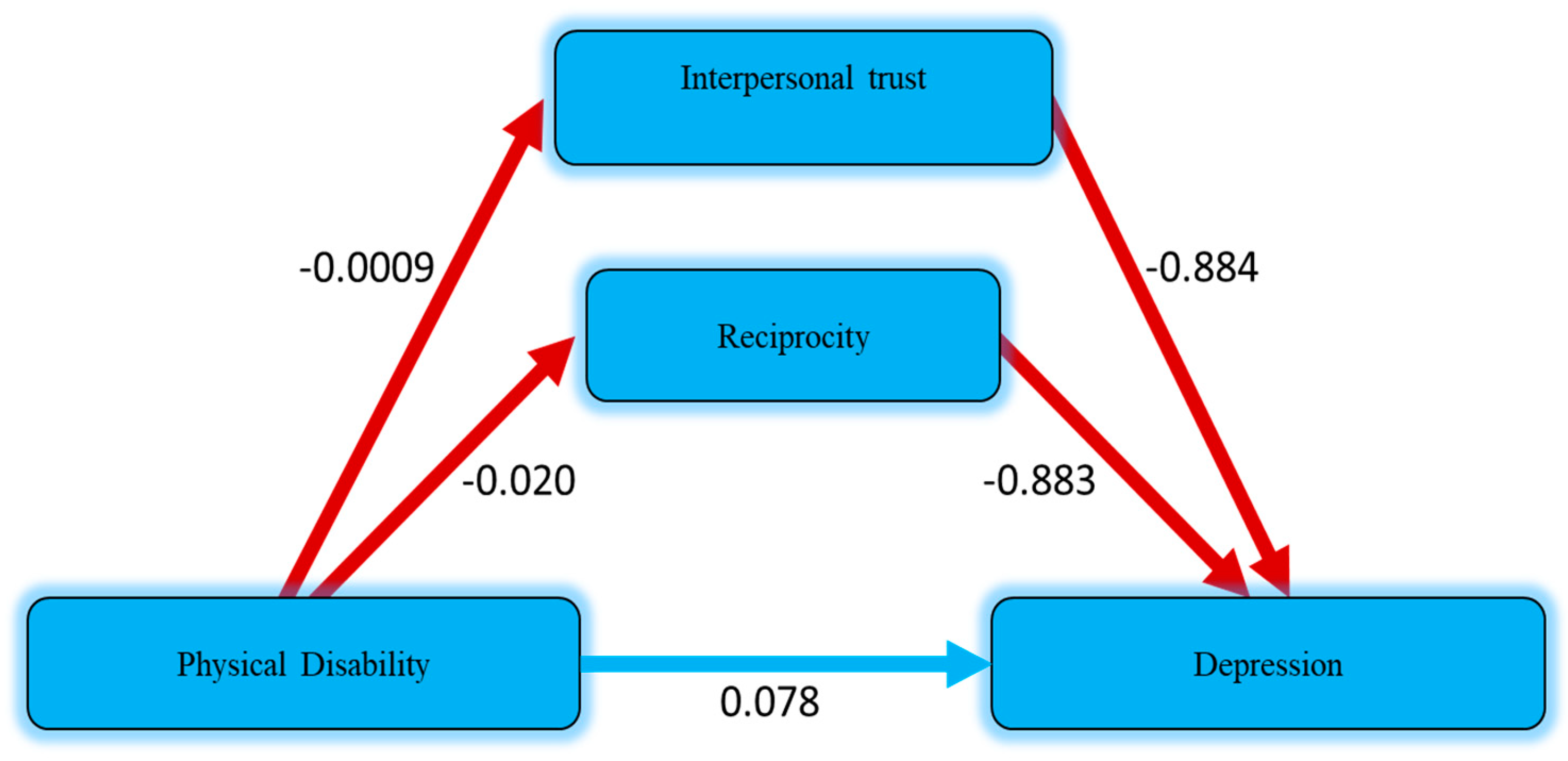
| Interpersonal trust | −0.884 * (0.425) | −1.726 | −0.042 |
| Reciprocity | −0.883 ** (0.315) | −1.507 | −0.259 |
| Physical disability | 0.078 ** (0.029) | 0.019 | 0.136 |
| Average monthly income (PKR) (Ref. ≤15,000) | |||
| 15,001–30,000 | 1.020 (0.565) | −0.097 | 2.137 |
| >30,000 | −1.051 (0.739) | −2.513 | 0.411 |
| Living status | −1.438 ** (0.517) | −2.461 | −0.415 |
| R2 F | 0.224 6.715 * | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tariq, A.; Beihai, T.; Ali, S.; Abbas, N.; Ilyas, A. Mediating Effect of Cognitive Social Capital on the Relationship Between Physical Disability and Depression in Elderly People of Rural Pakistan. Int. J. Environ. Res. Public Health 2019, 16, 4232. https://doi.org/10.3390/ijerph16214232
Tariq A, Beihai T, Ali S, Abbas N, Ilyas A. Mediating Effect of Cognitive Social Capital on the Relationship Between Physical Disability and Depression in Elderly People of Rural Pakistan. International Journal of Environmental Research and Public Health. 2019; 16(21):4232. https://doi.org/10.3390/ijerph16214232
Chicago/Turabian StyleTariq, Azam, Tian Beihai, Sajjad Ali, Nadeem Abbas, and Aasir Ilyas. 2019. "Mediating Effect of Cognitive Social Capital on the Relationship Between Physical Disability and Depression in Elderly People of Rural Pakistan" International Journal of Environmental Research and Public Health 16, no. 21: 4232. https://doi.org/10.3390/ijerph16214232
APA StyleTariq, A., Beihai, T., Ali, S., Abbas, N., & Ilyas, A. (2019). Mediating Effect of Cognitive Social Capital on the Relationship Between Physical Disability and Depression in Elderly People of Rural Pakistan. International Journal of Environmental Research and Public Health, 16(21), 4232. https://doi.org/10.3390/ijerph16214232