Design and Validation of an Instrument to Evaluate the Learning Acquired by Nursing Students from a Brief Tobacco Intervention (BTI-St©)

 ,
,  ,
,  and
and
Abstract
:1. Introduction
Background
2. Materials and Methods
Ethical Considerations
3. Results
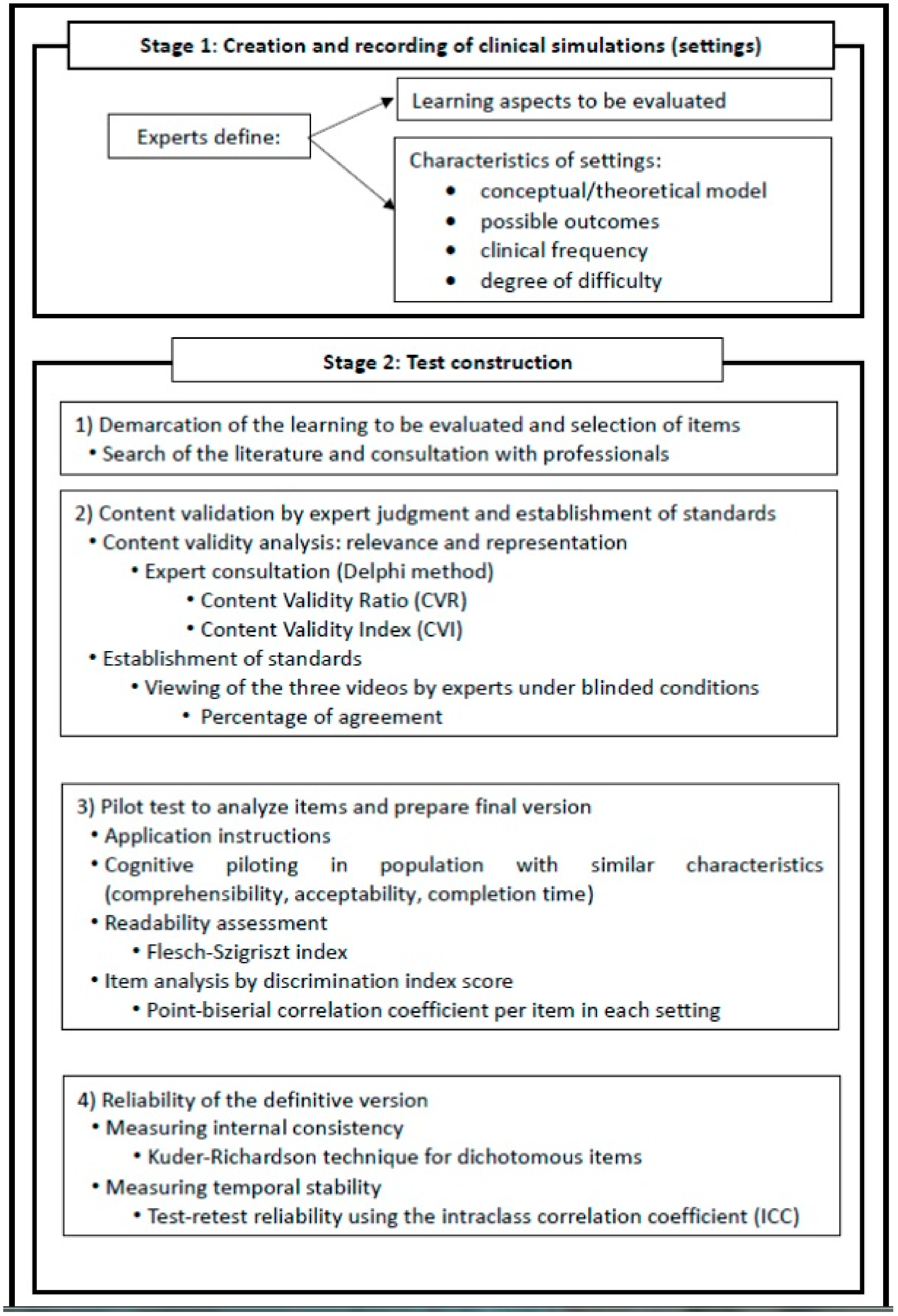
3.1. Stage 1
3.2. Stage 2
3.2.1. Phase 1: Demarcation of Evaluated Learning and Item Redaction
3.2.2. Phase 2: Content Validation by Expert Judgment and Establishment of Standards
3.2.3. Phase 3: Pilot Test to Analyze Items and Prepare Final Version
3.2.4. Phase 4: Reliability of the Definitive Version
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Oberg, M.; Jaakkola, M.S.; Woodward, A.; Peruga, A.; Prüss-Ustün, A. Worldwide burden of disease from exposure to second-hand smoke: A retrospective analysis of data from 192 countries. Lancet 2011, 377, 139–146. [Google Scholar] [CrossRef]
- Eriksen, M.; Mackay, J.; Schluger, N.; Islami, F.; Drope, J. The Tobacco Atlas, 5th ed.; American Cancer Society: Atlanta, GA, USA, 2015. [Google Scholar]
- WHO. Global Status Report on Noncommunicable Diseases 2010; WHO: Geneva, Switzerland, 2011. [Google Scholar]
- WHO. WHO Report on the Global Tobacco Epidemic: Monitoring Tobacco Use and Prevention Policices; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- WHO. MPOWER: A Policy Package To Reverse The Tobacco Epidemic; WHO: Geneva, Switzerland, 2008; ISBN 978-92-4-159663-3. [Google Scholar]
- Carr, A.B.; Ebbert, J. Interventions for tobacco cessation in the dental setting. Cochrane Database Syst. Rev. 2012, CD005084. [Google Scholar] [CrossRef] [PubMed]
- Rice, V.H.; Hartmann-Boyce, J.; Stead, L.F. Nursing interventions for smoking cessation. Cochrane Database Syst. Rev. 2013, 8, CD001188. [Google Scholar] [CrossRef] [PubMed]
- Silagy, C. Physician advice for smoking cessation. Cochrane Database Syst Rev 2000, CD000165. [Google Scholar] [CrossRef]
- West, R.; Raw, M.; McNeill, A.; Stead, L.; Aveyard, P.; Bitton, J.; Stapleton, J.; McRobbie, H.; Pokhrel, S.; Lester-George, A.; et al. Health-care interventions to promote and assist tobacco cessation: A review of efficacy, effectiveness and affordability for use in national guideline development. Addiction 2015, 110, 1388–1403. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Nicolas, A.; Trapero-Bertran, M.; Munoz, C. Cost-benefit of medical advice for quitting smoking in the Region of Murcia. Aten. Primaria 2017, 49, 407–416. [Google Scholar] [PubMed]
- Bartsch, A.-L.; Harter, M.; Niedrich, J.; Brutt, A.L.; Buchholz, A. A Systematic Literature Review of Self-Reported Smoking Cessation Counseling by Primary Care Physicians. PLoS ONE 2016, 11, e0168482. [Google Scholar] [CrossRef]
- Sarna, L.; Bialous, S.A.; Wells, M.; Kotlerman, J.; Wewers, M.E.; Froelicher, E.S. Frequency of nurses’ smoking cessation interventions: Report from a national survey. J. Clin. Nurs. 2009, 18, 2066–2077. [Google Scholar] [CrossRef] [PubMed]
- Duaso, M.J.; Bakhshi, S.; Mujika, A.; Purssell, E.; While, A.E. Nurses’ smoking habits and their professional smoking cessation practices. A systematic review and meta-analysis. Int. J. Nurs. Stud. 2017, 67, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Carson, K.V.; Verbiest, M.E.A.; Crone, M.R.; Brinn, M.P.; Esterman, A.J.; Assendelft, W.J.J.; Smith, B.J. Training health professionals in smoking cessation. Cochrane Database Syst. Rev. 2012, CD000214. [Google Scholar] [CrossRef]
- WHO. Guidelines for Implementation of Article 12 of the WHO Framework Convention on Tobacco Control; WHO: Geneva, Switzerland, 2010. [Google Scholar]
- Hagimoto, A.; Nakamura, M.; Masui, S.; Bai, Y.; Oshima, A. Effects of trained health professionals’ behavioral counseling skills on smoking cessation outcomes. Ann. Behav. Med. 2018, 52, 752–761. [Google Scholar] [CrossRef] [PubMed]
- Ockene, J.K.; Hayes, R.B.; Churchill, L.C.; Crawford, S.L.; Jolicoeur, D.G.; Murray, D.M.; Shoben, A.B.; David, S.P.; Ferguson, K.J.; Huggett, K.N.; et al. Teaching Medical Students to Help Patients Quit Smoking: Outcomes of a 10-School Randomized Controlled Trial. J. Gen. Intern. Med. 2016, 31, 172–181. [Google Scholar] [CrossRef] [PubMed]
- The Clinical Practice Guideline Treating Tobacco Use and Dependence 2008 Update Panel and Staff. A clinical practice guideline for treating tobacco use and dependence: 2008 update: A US Public Health Service report. Am. J. Prev. Med. 2008, 35, 158–176. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Toolkit for Delivering the 5A’s and 5R’s Brief Tobacco Interventions in Primary Care; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Kerr, S.; Whyte, R.; Watson, H.; Tolson, D.; McFdyen, A. Smoking Cessation in Later Life: An Evaluation of the Impact of Smoking Cessation Training on the Knowledge, Attitudes and Practice of Members of the Primary Care Team Who Work with Older People. Internet J. Health 2007, 5, 1–10. [Google Scholar]
- Newhouse, R.P.; Himmelfarb, C.D.; Liang, Y. Psychometric testing of the smoking cessation counseling scale. J. Nurs. Scholarsh. Off. Publ. Sigma Theta Tau Int. Honor Soc. Nurs. 2011, 43, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Romito, L.; Schrader, S.; Zahl, D. Using experiential learning and OSCEs to teach and assess tobacco dependence education with first-year dental students. J. Dent. Educ. 2014, 78, 703–713. [Google Scholar]
- Mazor, K.M.; Jolicoeur, D.; Hayes, R.B.; Geller, A.C.; Churchill, L.; Ockene, J.K. Assessing Medical Students’ Tobacco Dependence Treatment Skills Using a Detailed Behavioral Checklist. Teach. Learn. Med. 2015, 27, 292–298. [Google Scholar] [CrossRef]
- Hambleton, R.K.; Swaminathan, H.; Algina, J.; Coulson, D.B. Criterion-Referenced Testing and Measurement: A Review of Technical Issues and Developments. Rev. Educ. Res. 1978, 48, 1–47. [Google Scholar] [CrossRef]
- Pohpham, W. Criterion-Referenced Measurement; Prentice-Hall: Englewood Cliffs, NJ, USA, 1978. [Google Scholar]
- Hambleton, R.K.; Rogers, H.J. Advances in criterion-referenced measurement. In Advances in Educational and Psychological Testing: Theory and Applications; Evaluation in education and human services series; Kluwer Academic/Plenum Publishers: New York, NY, USA, 1991; pp. 3–43. ISBN 0-7923-9070-9. [Google Scholar]
- Barrio-Cantalejo, I.M.; Simón-Lorda, P.; Melguizo, M.; Escalona, I.; Marijuán, M.I.; Hernando, P. Validation of the INFLESZ scale to evaluate readability of texts aimed at the patient. An. Sist. Sanit. Navar. 2008, 31, 135–152. [Google Scholar]
- Hulsman, R.L.; Mollema, E.D.; Oort, F.J.; Hoos, A.M.; de Haes, J.C.J.M. Using standardized video cases for assessment of medical communication skills: Reliability of an objective structured video examination by computer. Patient Educ. Couns. 2006, 60, 24–31. [Google Scholar] [CrossRef]
- Koole, S.; Dornan, T.; Aper, L.; De Wever, B.; Scherpbier, A.; Valcke, M.; Cohen-Schotanus, J.; Derese, A. Using video-cases to assess student reflection: Development and validation of an instrument. BMC Med. Educ. 2012, 12, 22. [Google Scholar] [CrossRef] [PubMed]
- Coyne, E.; Frommolt, V.; Rands, H.; Kain, V.; Mitchell, M. Simulation videos presented in a blended learning platform to improve Australian nursing students’ knowledge of family assessment. Nurse Educ. Today 2018, 66, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Corelli, R.L.; Kroon, L.A.; Chung, E.P.; Sakamoto, L.M.; Gundersen, B.; Fenlon, C.M.; Hudmon, K.S. Statewide evaluation of a tobacco cessation curriculum for pharmacy students. Prev. Med. 2005, 40, 888–895. [Google Scholar] [CrossRef] [PubMed]
- Delucchi, K.L.; Tajima, B.; Guydish, J. Development of the Smoking Knowledge, Attitudes, and Practices (S-KAP) Instrument. J. Drug Issues 2009, 39, 347–364. [Google Scholar] [CrossRef] [PubMed]
- Wadland, W.C.; WinklerPrins, V.J.; Noel, M.M.; Thompson, M.E.; Ríos-Bedoya, C.F. Student performance on smoking cessation counseling with standardized patients. Fam. Med. 2011, 43, 422–428. [Google Scholar] [PubMed]
- Pedrosa, I.; Suárez-Álvarez, J.; García-Cueto, E. Content validity evidences: Theoretical advances and estimation methods. Acción Psicológica 2014, 10, 3–18. [Google Scholar] [CrossRef]
- Kruse, G.R.; Rigotti, N.A.; Raw, M.; McNeill, A.; Murray, R.; Piné-Abata, H.; Bitton, A.; McEwen, A. Content and Methods used to Train Tobacco Cessation Treatment Providers: An International Survey. J. Smok. Cessat. 2017, 12, 213–220. [Google Scholar] [CrossRef]
- Kerr, S.; Whyte, R.; Watson, H.; Tolson, D.; McFadyen, A.K. A Mixed-Methods Evaluation of the Effectiveness of Tailored Smoking Cessation Training for Healthcare Practitioners Who Work with Older People. Worldviews Evid. Based Nurs. 2011, 8, 177–186. [Google Scholar] [CrossRef]
- Ockene, J.; Quirk, M.; Goldberg, R.; Kristeller, J.; Donnelly, G.; Kalan, K.; Gould, B.; Greene, H.; Harrison-Atlas, R.; Pease, J.; et al. A residents’ training program for the development of smoking intervention skills. Arch. Intern. Med. 1988, 148, 1039–1045. [Google Scholar] [CrossRef]
- Molina, A.J.; Fernández, T.; Fernández, D.; Delgado, M.; de Abajo, S.; Martín, V. Knowledge, attitudes and beliefs about tobacco use after an educative intervention in health sciences’ students. Nurse Educ. Today 2012, 32, 862–867. [Google Scholar] [CrossRef]
- Sreeramareddy, C.; Suri, S.; Menezes, R.; Kumar, H.; Rahman, M.; Islam, M.R.; Pereira, X.V.; Shah, M.; Sathian, B.; Shetty, U.; et al. Self-reported tobacco smoking practices among medical students and their perceptions towards training about tobacco smoking in medical curricula: A cross-sectional, questionnaire survey in Malaysia, India, Pakistan, Nepal, and Bangladesh. Subst. Abuse Treat. Prev. Policy 2010, 5, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Lucas, N.C.C.; Walker, N.; Bullen, C. Using a videotaped objective structured clinical examination to assess Knowledge in Smoking cessation amongst medical Students (the K.I.S.S. Study). Med. Teach. 2016, 38, 1256–1261. [Google Scholar] [CrossRef] [PubMed]
- Alhaj Ali, A.; Musallam, E. Debriefing Quality Evaluation in Nursing Simulation-Based Education: An Integrative Review. Clin. Simul. Nurs. 2018, 16, 15–24. [Google Scholar] [CrossRef]

{kind=link}
| Setting 1 | Setting 2 | Setting 3 | |
|---|---|---|---|
| (BTI)-St Items | Corrected Item—Total Correlation | Corrected Item—Total Correlation | Corrected Item—Total Correlation |
| Item 5 Classifying the person as a smoker | 0.46 | 0.34 | 0.35 |
| Item 6 Recording this information in their clinical history | 0.48 | 0.40 | 0.69 |
| Item 7 Clearly offering advice | 0.40 | 0.35 | 0.64 |
| Item 8 Assertively offering advice | 0.55 | 0.45 | 0.64 |
| Item 9 Offering advice in a personalized manner | 0.52 | 0.46 | 0.63 |
| Item 10 Assessing whether they would like to be a non-smoker | 0.48 | 0.32 | 0.31 |
| Item 11 Assessing whether the person thinks they can quit smoking | 0.31 | 0.32 | 0.30 |
| Item 12 Providing motivation based on the importance of quitting for the person | 0.59 | 0.67 | |
| Item 13 Reporting the risks of smoking for the person | 0.60 | 0.50 | |
| Item 14 Asking the person to identify the benefits of quitting that they consider important | 0.55 | 0.65 | |
| Item 15 Asking the person to identify the barriers/obstacles to quitting | 0.63 | 0.57 | |
| Item 16 Indicating a date to quit smoking (preferably within 2 weeks) | 0.53 | ||
| Item 17 Indicating the need to communicate the quitting attempt to family, workmates, and friends and to ask them for help | 0.58 | ||
| Item 18 Indicating the need to anticipate difficulties (situations that can hamper quitting) | 0.58 | ||
| Item 19 Recommending the person to make his/her house a tobacco-free environment | 0.59 | ||
| Item 20 Describing the availability of pharmacological treatments if appropriate | 0.43 | ||
| Item 21 Offering complementary materials (brochures, quit line, etc.) | 0.51 | ||
| Item 22 Agreeing on a follow-up contact | 0.44 | ||
| Item 23 Referring the person to specialized resources for quitting (if available) | 0.60 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramos-Morcillo, A.J.; Leal-Costa, C.; García-Moral, A.T.; del-Pino-Casado, R.; Ruzafa-Martínez, M. Design and Validation of an Instrument to Evaluate the Learning Acquired by Nursing Students from a Brief Tobacco Intervention (BTI-St©). Int. J. Environ. Res. Public Health 2019, 16, 3944. https://doi.org/10.3390/ijerph16203944
Ramos-Morcillo AJ, Leal-Costa C, García-Moral AT, del-Pino-Casado R, Ruzafa-Martínez M. Design and Validation of an Instrument to Evaluate the Learning Acquired by Nursing Students from a Brief Tobacco Intervention (BTI-St©). International Journal of Environmental Research and Public Health. 2019; 16(20):3944. https://doi.org/10.3390/ijerph16203944
Chicago/Turabian StyleRamos-Morcillo, Antonio Jesús, César Leal-Costa, Ana Teresa García-Moral, Rafael del-Pino-Casado, and María Ruzafa-Martínez. 2019. "Design and Validation of an Instrument to Evaluate the Learning Acquired by Nursing Students from a Brief Tobacco Intervention (BTI-St©)" International Journal of Environmental Research and Public Health 16, no. 20: 3944. https://doi.org/10.3390/ijerph16203944
APA StyleRamos-Morcillo, A. J., Leal-Costa, C., García-Moral, A. T., del-Pino-Casado, R., & Ruzafa-Martínez, M. (2019). Design and Validation of an Instrument to Evaluate the Learning Acquired by Nursing Students from a Brief Tobacco Intervention (BTI-St©). International Journal of Environmental Research and Public Health, 16(20), 3944. https://doi.org/10.3390/ijerph16203944