Adult E-Cigarettes Use Associated with a Self-Reported Diagnosis of COPD



Abstract
1. Introduction
2. Materials and Methods
2.1. Measures of Independent Variables
2.2. Measure of Dependent Variable
2.3. Statistical Analysis
3. Results
3.1. Study Sample Characteristics
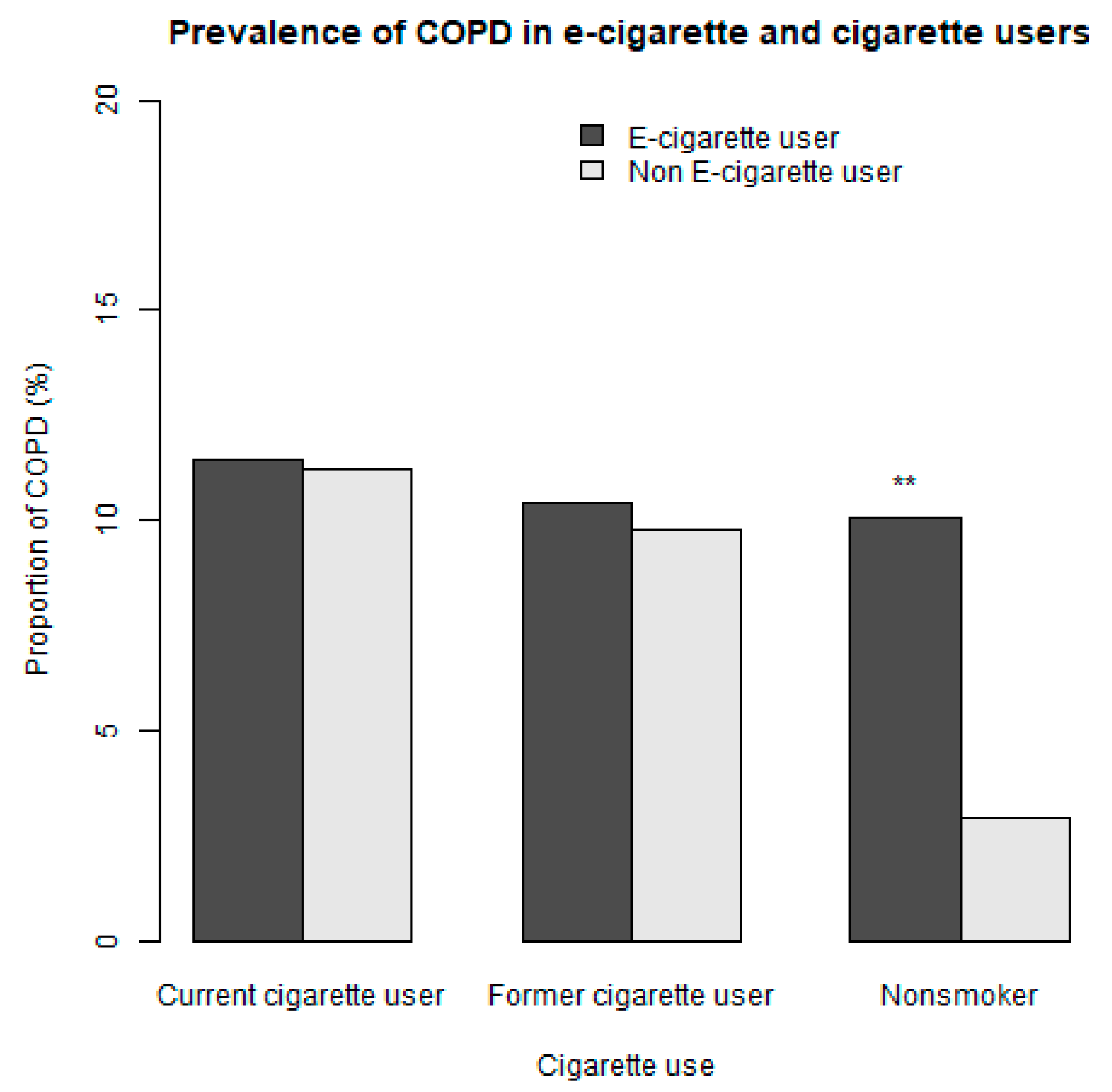
3.2. Association between E-Cigarette Use and Reporting COPD
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- E-Cigarette Use among Youth and Young Adults: A Report of the Surgeon General. Available online: https://www.ncbi.nlm.nih.gov/books/NBK538680/ (accessed on 20 September 2019).
- Dai, H.; Leventhal, A.M. Prevalence of E-Cigarette Use Among Adults in the United States, 2014–2018. JAMA 2019. [Google Scholar] [CrossRef] [PubMed]
- Cullen, K.A.; Ambrose, B.K.; Gentzke, A.S.; Apelberg, B.J.; Jamal, A.; King, B.A. Notes from the Field: Use of Electronic Cigarettes and Any Tobacco Product Among Middle and High School Students–United States, 2011–2018. MMWR Morb. Mortal. Wkly. Rep. 2018, 67, 1276–1277. [Google Scholar] [CrossRef] [PubMed]
- Dinakar, C.; O’Connor, G.T. The Health Effects of Electronic Cigarettes. N. Engl. J. Med. 2016, 375, 1372–1381. [Google Scholar] [CrossRef] [PubMed]
- Cheng, T. Chemical evaluation of electronic cigarettes. Tob. Control 2014, 23, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Goniewicz, M.L.; Knysak, J.; Gawron, M.; Kosmider, L.; Sobczak, A.; Kurek, J.; Prokopowicz, A.; Jablonska-Czapla, M.; Rosik-Dulewska, C.; Havel, C.; et al. Levels of selected carcinogens and toxicants in vapour from electronic cigarettes. Tob. Control 2014, 23, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Goniewicz, M.L.; Smith, D.M.; Edwards, K.C.; Blount, B.C.; Caldwell, K.L.; Feng, J.; van Bemmel, D. Comparison of nicotine and toxicant exposure in users of electronic cigarettes and combustible cigarettes. JAMA Netw. Open 2018, 1, e185937. [Google Scholar] [CrossRef] [PubMed]
- Layden, J.E.; Ghinai, I.; Pray, I.; Kimball, A.; Layer, M.; Tenforde, M.; Navon, L.; Hoots, B.; Salvatore, P.P.; Elderbrook, M.; et al. Pulmonary Illness Related to E-Cigarette Use in Illinois and Wisconsin–Preliminary Report. N. Engl. J. Med. 2019. [Google Scholar] [CrossRef]
- Morjaria, J.B.; Mondati, E.; Polosa, R. E-cigarettes in patients with COPD: Current perspectives. Int. J. Chron. Obstruct Pulmon. Dis. 2017, 12, 3203–3210. [Google Scholar] [CrossRef]
- Coleman, B.N.; Rostron, B.; Johnson, S.E.; Ambrose, B.K.; Pearson, J.; Stanton, C.A.; Wang, B.; Delnevo, C.; Bansal-Travers, M.; Kimmel, H.L.; et al. Electronic cigarette use among US adults in the Population Assessment of Tobacco and Health (PATH) Study, 2013–2014. Tob. Control 2017, 26, e117–e126. [Google Scholar] [CrossRef]
- Foulds, J.; Veldheer, S.; Berg, A. Electronic cigarettes (e-cigs): Views of aficionados and clinical/public health perspectives. Int. J. Clin. Pract. 2011, 65, 1037–1042. [Google Scholar] [CrossRef]
- Etter, J.F. Electronic cigarettes: A survey of users. BMC Public Health 2010, 10, 231. [Google Scholar] [CrossRef] [PubMed]
- Walker, N.; Parag, V.; Verbiest, M.; Laking, G.; Laugesen, M.; Bullen, C. Nicotine patches used in combination with e-cigarettes (with and without nicotine) for smoking cessation: A pragmatic, randomised trial. Lancet Respir. Med. 2019. [Google Scholar] [CrossRef]
- Hajek, P.; Phillips-Waller, A.; Przulj, D.; Pesola, F.; Myers Smith, K.; Bisal, N.; Li, J.; Parrott, S.; Sasieni, P.; Dawkins, L.; et al. A Randomized Trial of E-Cigarettes versus Nicotine-Replacement Therapy. N. Engl. J. Med. 2019, 380, 629–637. [Google Scholar] [CrossRef] [PubMed]
- Bullen, C.; Howe, C.; Laugesen, M.; McRobbie, H.; Parag, V.; Williman, J.; Walker, N. Electronic cigarettes for smoking cessation: A randomised controlled trial. Lancet 2013, 382, 1629–1637. [Google Scholar] [CrossRef]
- Outbreak of Lung Injury Associated with E-Cigarette Use, or Vaping. Available online: https://www.cdc.gov/tobacco/basic_information/e-cigarettes/severe-lung-disease.html (accessed on 19 September 2019).
- Baldassarri, S.R.; Chupp, G.L.; Leone, F.T.; Warren, G.W.; Toll, B.A. Practice Patterns and Perceptions of Chest Health Care Providers on Electronic Cigarette Use: An In-Depth Discussion and Report of Survey Results. J. Smok. Cessat. 2018, 13, 72–77. [Google Scholar] [CrossRef]
- Schraufnagel, D.E.; Blasi, F.; Drummond, M.B.; Lam, D.C.; Latif, E.; Rosen, M.J.; Sansores, R.; Van Zyl-Smit, R. Electronic cigarettes. A position statement of the forum of international respiratory societies. Am. J. Respir. Crit. Care Med. 2014, 190, 611–618. [Google Scholar] [CrossRef]
- Perez, M.F.; Atuegwu, N.C.; Oncken, C.M.; Mead, E.L.; Mortensen, E.M. Association of Electronic Cigarette Use and Asthma in Never Smokers. Ann. Am. Thorac. Soc. 2019. [Google Scholar] [CrossRef]
- Cho, J.H.; Paik, S.Y. Association between Electronic Cigarette Use and Asthma among High School Students in South Korea. PLoS ONE 2016, 11, e0151022. [Google Scholar] [CrossRef]
- Choi, K.; Bernat, D. E-Cigarette Use among Florida Youth with and Without Asthma. Am. J. Prev. Med. 2016, 51, 446–453. [Google Scholar] [CrossRef]
- Schweitzer, R.J.; Wills, T.A.; Tam, E.; Pagano, I.; Choi, K. E-cigarette use and asthma in a multiethnic sample of adolescents. Prev. Med. 2017, 105, 226–231. [Google Scholar] [CrossRef]
- Vogelmeier, C.F.; Criner, G.J.; Martinez, F.J.; Anzueto, A.; Barnes, P.J.; Bourbeau, J.; Celli, B.R.; Chen, R.; Decramer, M.; Fabbri, L.M.; et al. Global Strategy for the Diagnosis, Management and Prevention of Chronic Obstructive Lung Disease 2017 Report: GOLD Executive Summary. Respirology 2017, 22, 575–601. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, J.; Pravosud, V.; Mannino, D.M.; Siegel, K.; Choate, R.; Sullivan, T. National and State Estimates of COPD Morbidity and Mortality–United States, 2014–2015. Chronic Obstr. Pulm. Dis. 2018, 5, 324–333. [Google Scholar] [CrossRef] [PubMed]
- Ramsey, S.D.; Hobbs, F.D. Chronic obstructive pulmonary disease, risk factors, and outcome trials: Comparisons with cardiovascular disease. Proc. Am. Thorac. Soc. 2006, 3, 635–640. [Google Scholar] [CrossRef] [PubMed]
- Buist, A.S.; McBurnie, M.A.; Vollmer, W.M.; Gillespie, S.; Burney, P.; Mannino, D.M.; Menezes, A.M.; Sullivan, S.D.; Lee, T.A.; Weiss, K.B.; et al. International variation in the prevalence of COPD (the BOLD Study): A population-based prevalence study. Lancet 2007, 370, 741–750. [Google Scholar] [CrossRef]
- Larcombe, A.N.; Janka, M.A.; Mullins, B.J.; Berry, L.J.; Bredin, A.; Franklin, P.J. The effects of electronic cigarette aerosol exposure on inflammation and lung function in mice. Am. J. Physiol. Lung Cell Mol. Physiol. 2017, 313, L67–L79. [Google Scholar] [CrossRef]
- Lerner, C.A.; Sundar, I.K.; Yao, H.; Gerloff, J.; Ossip, D.J.; McIntosh, S.; Robinson, R.; Rahman, I. Vapors produced by electronic cigarettes and e-juices with flavorings induce toxicity, oxidative stress, and inflammatory response in lung epithelial cells and in mouse lung. PLoS ONE 2015, 10, e0116732. [Google Scholar] [CrossRef]
- Garcia-Arcos, I.; Geraghty, P.; Baumlin, N.; Campos, M.; Dabo, A.J.; Jundi, B.; Cummins, N.; Eden, E.; Grosche, A.; Salathe, M.; et al. Chronic electronic cigarette exposure in mice induces features of COPD in a nicotine-dependent manner. Thorax 2016, 71, 1119–1129. [Google Scholar] [CrossRef]
- Lim, H.B.; Kim, S.H. Inhallation of e-Cigarette Cartridge Solution Aggravates Allergen-induced Airway Inflammation and Hyper-responsiveness in Mice. Toxicol Res. 2014, 30, 13–18. [Google Scholar] [CrossRef]
- Barnes, P.J. Immunology of asthma and chronic obstructive pulmonary disease. Nat. Rev. Immunol. 2008, 8, 183–192. [Google Scholar] [CrossRef]
- Wills, T.A.; Pagano, I.; Williams, R.; Tam, E. E-cigarette use and respiratory disorder in an adult sample. Drug Alcohol Depend. 2018, 194, 363–370. [Google Scholar] [CrossRef]
- Polosa, R.; Cibella, F.; Caponnetto, P.; Maglia, M.; Prosperini, U.; Russo, C.; Tashkin, D. Health impact of E-cigarettes: A prospective 3.5-year study of regular daily users who have never smoked. Sci. Rep. 2017, 7, 13825. [Google Scholar] [PubMed]
- Hyland, A.; Ambrose, B.K.; Conway, K.P.; Borek, N.; Lambert, E.; Carusi, C.; Taylor, K.; Crosse, S.; Fong, G.T.; Cummings, K.M.; et al. Design and methods of the Population Assessment of Tobacco and Health (PATH) Study. Tob. Control 2017, 26, 371–378. [Google Scholar] [CrossRef] [PubMed]
- Population Assessment of Tobacco and Health (PATH) Study Series. Available online: https://www.icpsr.umich.edu/icpsrweb/NAHDAP/series/606 (accessed on 18 September 2019).
- CDC. NHIS–Adult Tobacco Use–Glossary. Available online: https://www.cdc.gov/nchs/nhis/tobacco /tobacco_glossary.htm (accessed on 1 October 2019).
- Rosenbaum, P.R.; Rubin, D.B. The Central Role of the Propensity Score in Observational Studies for Causal Effects. Biometrika 1983, 70, 41–55. [Google Scholar] [CrossRef]
- Lenis, D.; Nguyen, T.Q.; Dong, N.; Stuart, E.A. It’s all about balance: Propensity score matching in the context of complex survey data. Biostatistics 2017, 20, 147–163. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2013. [Google Scholar]
- Lappas, A.S.; Tzortzi, A.S.; Konstantinidi, E.M.; Teloniatis, S.I.; Tzavara, C.K.; Gennimata, S.A.; Koulouris, N.G.; Behrakis, P.K. Short-term respiratory effects of e-cigarettes in healthy individuals and smokers with asthma. Respirology 2018, 23, 291–297. [Google Scholar] [CrossRef]
- McConnell, R.; Barrington-Trimis, J.L.; Wang, K.; Urman, R.; Hong, H.; Unger, J.; Samet, J.; Leventhal, A.; Berhane, K. Electronic Cigarette Use and Respiratory Symptoms in Adolescents. Am. J. Respir. Crit. Care Med. 2017, 195, 1043–1049. [Google Scholar] [CrossRef]
- Bowler, R.P.; Hansel, N.N.; Jacobson, S.; Graham Barr, R.; Make, B.J.; Han, M.K.; O’Neal, W.K.; Oelsner, E.C.; Casaburi, R.; Barjaktarevic, I.; et al. Electronic Cigarette Use in US Adults at Risk for or with COPD: Analysis from Two Observational Cohorts. J. Gen. Intern Med. 2017, 32, 1315–1322. [Google Scholar] [CrossRef]
- Department of Health. New York State Department of Health Announces Update on Investigation into Vaping-Associated Pulmonary Illnesses. Available online: https://www.health.ny.gov/press/releases/2019/2019-09-05_vaping.htm (accessed on 14 September 2019).
- Farsalinos, K.E.; Romagna, G.; Tsiapras, D.; Kyrzopoulos, S.; Voudris, V. Characteristics, perceived side effects and benefits of electronic cigarette use: A worldwide survey of more than 19,000 consumers. Int. J. Environ. Res. Public Health 2014, 11, 4356–4373. [Google Scholar] [CrossRef]
- Polosa, R.; Morjaria, J.B.; Caponnetto, P.; Prosperini, U.; Russo, C.; Pennisi, A.; Bruno, C.M. Evidence for harm reduction in COPD smokers who switch to electronic cigarettes. Respir Res. 2016, 17, 166. [Google Scholar] [CrossRef]
- Polosa, R.; Morjaria, J.B.; Prosperini, U.; Russo, C.; Pennisi, A.; Puleo, R.; Caruso, M.; Caponnetto, P. Health effects in COPD smokers who switch to electronic cigarettes: A retrospective-prospective 3-year follow-up. Int. J. Chron. Obstruct Pulmon. Dis. 2018, 13, 2533–2542. [Google Scholar] [CrossRef]
- Kasza, K.A.; Ambrose, B.K.; Conway, K.P.; Borek, N.; Taylor, K.; Goniewicz, M.L.; Cummings, K.M.; Sharma, E.; Pearson, J.L.; Green, V.R.; et al. Tobacco-Product Use by Adults and Youths in the United States in 2013 and 2014. N. Engl. J. Med. 2017, 376, 342–353. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, S.P.; Kim, Y.I.; Harrington, K.F.; Hokanson, J.E.; Lutz, S.M.; Cho, M.H.; DeMeo, D.L.; Wells, J.M.; Make, B.J.; Rennard, S.I.; et al. Smoking duration alone provides stronger risk estimates of chronic obstructive pulmonary disease than pack-years. Thorax 2018, 73, 414–421. [Google Scholar] [CrossRef] [PubMed]
- Akinbami, L.J.; Moorman, J.E.; Liu, X.; National Center for Health Statistics (U.S.). Asthma Prevalence, Health Care Use, and Mortality: United States, 2005–2009; Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics: Hyattsville, MD, USA, 2011.



{kind=link}
{kind=link}
| Variable | Controls a | E-Cigarette Users a | Sample Balance | Population Balance c | ||
|---|---|---|---|---|---|---|
| p-Value | SMD b | p-Value | SMD b | |||
| Number of Individuals | 2727 | 2727 | ||||
| BMI | 27.5 (6.7) | 27.7 (6.8) | 0.38 | 0.02 | 0.74 | 0.01 |
| Years of conventional cigarette use | 14.2 (14.4) | 13.9 (13.7) | 0.37 | 0.02 | 0.80 | 0.01 |
| Age Group | 0.85 | 0.04 | 0.86 | 0.04 | ||
| 18 to 24 years old | 793 (29.1) | 830 (30.4) | ||||
| 25 to 34 years old | 685 (25.1) | 685 (25.1) | ||||
| 35 to 44 years old | 475 (17.4) | 478 (17.5) | ||||
| 45 to 54 years old | 419 (15.4) | 394 (14.4) | ||||
| 55 to 65 years old | 265 (9.7) | 256 (9.4) | ||||
| 65 years old or older | 90 (3.3) | 84 (3.1) | ||||
| Male | 1493 (54.7) | 1451 (53.2) | 0.27 | 0.03 | 0.15 | 0.04 |
| Hispanic | 396 (14.5) | 396 (14.5) | 1.00 | <0.001 | 0.92 | 0.003 |
| Race | 0.78 | 0.02 | 0.12 | 0.06 | ||
| White | 2171 (79.6) | 2155 (79.0) | ||||
| Black | 257 (9.4) | 272 (10.0) | ||||
| Other | 299 (11.0) | 300 (11.0) | ||||
| Grade of Highest Education | 0.37 | 0.06 | 0.29 | 0.07 | ||
| Less than High School | 312 (11.4) | 306 (11.2) | ||||
| GED | 289 (10.6) | 271 (9.9) | ||||
| High school graduate | 633 (23.2) | 664 (24.3) | ||||
| Some college (no degree) or associates degree | 1096 (40.2) | 1131 (41.5) | ||||
| Bachelor’s degree or higher | 397 (14.6) | 355 (13.0) | ||||
| Census Region | 0.84 | 0.03 | 0.75 | 0.04 | ||
| Northeast | 301 (11.0) | 310 (11.4) | ||||
| Midwest | 718 (26.3) | 692 (25.4) | ||||
| South | 1059 (38.8) | 1081 (39.6) | ||||
| West | 649 (23.8) | 644 (23.6) | ||||
| Second Hand Exposure During Childhood | 1747 (64.1) | 1767 (64.8) | 0.59 | 0.02 | 0.72 | 0.01 |
| History of Asthma | 356 (13.1) | 371 (13.6) | 0.58 | 0.02 | 0.78 | 0.01 |
| Poverty level | 0.69 | 0.02 | 0.48 | 0.04 | ||
| 100% of poverty guideline | 985 (36.1) | 987 (36.2) | ||||
| 100-199% of poverty guideline | 674 (24.7) | 698 (25.6) | ||||
| ≥200% of poverty guideline | 1068 (39.2) | 1042 (38.2) | ||||
| History of Blunt Use | 1097 (40.2) | 1107 (40.6) | 0.80 | 0.01 | 0.29 | 0.03 |
| Current Secondhand Smoke Exposure in Household | 1366 (50.1) | 1351 (49.5) | 0.71 | 0.01 | 0.82 | 0.01 |
| Never Used Cigars d | 1193 (43.7) | 1197 (43.9) | 0.94 | 0.003 | 0.40 | 0.03 |
| Never Used Cigarillos | 968 (35.5) | 969 (35.5) | 1.00 | 0.001 | 0.97 | 0.001 |
| Never Used Pipe | 1762 (64.6) | 1773 (65.0) | 0.78 | 0.01 | 0.40 | 0.03 |
| Never Used Hookah | 1442 (52.9) | 1412 (51.8) | 0.43 | 0.02 | 0.48 | 0.03 |
| Never Used Oral Tobacco | 1729 (63.4) | 1703 (62.4) | 0.48 | 0.02 | 0.81 | 0.01 |
| Current conventional cigarette use | 1880 (68.9) | 1899 (69.6) | 0.60 | 0.02 | 0.08 | 0.05 |
| Former conventional cigarette use | 395 (14.5) | 368 (13.5) | 0.31 | 0.03 | 0.11 | 0.05 |
| History of High Blood Pressure | 519 (19.0) | 527 (19.3) | 0.81 | 0.01 | 0.32 | 0.03 |
| History of High Cholesterol | 376 (13.8) | 369 (13.5) | 0.81 | 0.01 | 0.98 | 0.001 |
| History of Congestive Heart Failure | 35 (1.3) | 42 (1.5) | 0.75 | 0.02 | 0.67 | 0.01 |
| History of Stroke | 47 (1.7) | 43 (1.6) | 0.52 | 0.01 | 0.92 | 0.003 |
| History of Heart Attack | 40 (1.5) | 47 (1.7) | 0.75 | 0.02 | 0.85 | 0.01 |
| History of Heroin, Inhalants or Hallucinogens | 482 (17.7) | 462 (16.9) | 0.50 | 0.02 | 0.58 | 0.02 |
| History of Diabetes | 257 (9.4) | 261 (9.6) | 0.89 | 0.01 | 0.98 | 0.001 |
| Category | Entire Cohort | Nonsmokers a | Subjects ≥35 b | Subjects ≥45 b | Subjects ≥55 b |
|---|---|---|---|---|---|
| Not users | Reference | Reference | Reference | Reference | Reference |
| E-cigarette user | 1.47 (1.21–1.79) | 2.94 (1.73–4.99) | 1.57(1.27–1.95) | 1.57 (1.20–2.06) | 1.62 (1.14–2.31) |
| Age groups b | |||||
| 18 to 24 | Reference | Reference | |||
| 25 to 34 | 1.03 (0.70–1.52) | 1.29 (0.68–2.42) | |||
| 35 to 44 | 1.79 (1.21–2.63) | 1.97 (0.87–4.45) | Reference | - | - |
| 45 to 54 | 2.37(1.67–3.37) | 1.96 (1.03–3.71) | 1.33 (0.96–1.85) | Reference | - |
| 55 to 65 | 3.15 (2.18–4.54) | 4.06 (2.07–7.97) | 1.79 (1.25–2.58) | 1.35 (1.03–1.77) | Reference |
| >65 | 3.79 (2.55–5.65) | 5.96 (3.31–10.74) | 2.15 (1.38–3.37) | 1.64 (1.18–2.26) | 1.25 (0.91–1.72) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perez, M.F.; Atuegwu, N.C.; Mead, E.L.; Oncken, C.; Mortensen, E.M. Adult E-Cigarettes Use Associated with a Self-Reported Diagnosis of COPD. Int. J. Environ. Res. Public Health 2019, 16, 3938. https://doi.org/10.3390/ijerph16203938
Perez MF, Atuegwu NC, Mead EL, Oncken C, Mortensen EM. Adult E-Cigarettes Use Associated with a Self-Reported Diagnosis of COPD. International Journal of Environmental Research and Public Health. 2019; 16(20):3938. https://doi.org/10.3390/ijerph16203938
Chicago/Turabian StylePerez, Mario F., Nkiruka C. Atuegwu, Erin L. Mead, Cheryl Oncken, and Eric M. Mortensen. 2019. "Adult E-Cigarettes Use Associated with a Self-Reported Diagnosis of COPD" International Journal of Environmental Research and Public Health 16, no. 20: 3938. https://doi.org/10.3390/ijerph16203938
APA StylePerez, M. F., Atuegwu, N. C., Mead, E. L., Oncken, C., & Mortensen, E. M. (2019). Adult E-Cigarettes Use Associated with a Self-Reported Diagnosis of COPD. International Journal of Environmental Research and Public Health, 16(20), 3938. https://doi.org/10.3390/ijerph16203938