Association of Bedtime with both Suicidal Ideation and Suicide Planning among Korean Adolescents

 , , ,
, , ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Data and Study Participants
2.2. Variables
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Preventing Suicide, Mental and Behavioural Disorders; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Centers for Disease Conrtol and Prevention. Leading Cause of Death by Age Group, United States—2014; CDC: Atlanta, GA, USA, 2014. [Google Scholar]
- Korea National Statistical Office. The Report of the Korean Adolescent in 2017; Statistic Korea: Daejeon, Korea, 2017. [Google Scholar]
- Organization for Economic Cooperation and Development. The Report of the Suicide Rates in 2018; OECD: Paris, France, 2018. [Google Scholar]
- Korea National Statistical Office. Death and Cause of Death in Korea: 2013; Statistic Korea: Daejeon, Korea, 2014. [Google Scholar]
- Moore, R.; Mao, Y.; Zhang, J.; Clarke, K. Economic Burden of Illness in Canada, 1998; Health Canada: Ottawa, ON, Canada, 2002; pp. 37–43. [Google Scholar]
- Kim, J.; Hahm, M.I.; Park, E.C.; Park, J.H.; Park, J.H.; Kim, S.E.; Kim, S.G. Economic burden of cancer in South Korea for the year 2005. J. Prev. Med. Public Health 2009, 42, 190–198. [Google Scholar] [CrossRef] [PubMed]
- Jang, S.I.; Lee, K.S.; Park, E.C. Relationship between current sleep duration and past suicidal ideation or attempt among Korean adolescents. J. Prev. Med. Public Health 2013, 46, 329–335. [Google Scholar] [CrossRef] [PubMed]
- Mann, J.J.; Brent, D.A.; Arango, V. The neurobiology and genetics of suicide and attempted suicide: A focus on the serotonergic system. Neuropsychopharmacology 2001, 24, 467–477. [Google Scholar] [CrossRef]
- Kim, J.H.; Park, E.C.; Cho, W.H.; Park, J.Y.; Choi, W.J.; Chang, H.S. Association between total sleep duration and suicidal ideation among the Korean general adult population. Sleep 2013, 36, 1563–1572. [Google Scholar] [CrossRef] [PubMed]
- Atay, I.M.; Eren, I.; Gundogar, D. The prevalence of death ideation and attempted suicide and the associated risk factors in Isparta, Turkey. Turk. J. Psychiatry 2012, 23, 1–10. [Google Scholar]
- Reyes-Portillo, J.A.; Lake, A.M.; Kleinman, M.; Gould, M.S. The Relation between descriptive norms, suicide ideation, and suicide attempts among adolescents. Suicide Life Threat. Behav. 2019, 49, 535–546. [Google Scholar] [CrossRef] [PubMed]
- Goodwin, R.D.; Marusic, A. Association between short sleep and suicidal ideation and suicide attempt among adults in the general population. Sleep 2008, 31, 1097–1101. [Google Scholar] [PubMed]
- Wojnar, M.; Ilgen, M.A.; Wojnar, J.; McCammon, R.J.; Valenstein, M.; Brower, K.J. Sleep problems and suicidality in the National Comorbidity Survey Replication. J. Psychiatr. Res. 2009, 43, 526–531. [Google Scholar] [CrossRef] [PubMed]
- Lensch, T.; Clements-Nolle, K.; Oman, R.F.; Lu, M.; Dominguez, A. Prospective impact of individual, family and community youth assets on adolescent suicide ideation. J. Epidemiol. Community Health 2019, 73, 219. [Google Scholar] [CrossRef]
- Kim, J.L.; Kim, J.M.; Choi, Y.; Lee, T.H.; Park, E.C. Effect of socioeconomic status on the linkage between suicidal ideation and suicide attempts. Suicide Life Threat. Behav. 2016, 46, 588–597. [Google Scholar] [CrossRef]
- Nock, M.K.; Borges, G.; Bromet, E.J.; Cha, C.B.; Kessler, R.C.; Lee, S. Suicide and suicidal behavior. Epidemiol. Rev. 2008, 30, 133–154. [Google Scholar] [CrossRef] [PubMed]
- OECD Special Focus. Measuring Leisure in OECD Countries, Society at a Glance 2009; OECD Development: Paris, France, 2009. [Google Scholar]
- Gradisar, M.; Gardner, G.; Dohnt, H. Recent worldwide sleep patterns and problems during adolescence: A review and meta-analysis of age, region, and sleep. Sleep Med. 2011, 12, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.A.; Park, H.S. Relation between sleep duration, overweight, and metabolic syndrome in Korean adolescents. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.; Ha, J. The association between nonstandard employment and suicidal ideation: Data from the first~fourth Korea National Health and Nutrition Examination Surveys. Korean J. Occup. Environ. Med. 2011, 23, 89–97. [Google Scholar] [CrossRef]
- Korea Centers for Disease Control and Prevention. The Report of the Korea Youth Risk Behavior Web-Based Survey in 2017; KCDC: Cheongju, Korea, 2017. [Google Scholar]
- Kim, J.H.; Park, E.C.; Lee, S.G.; Yoo, K.B. Associations between time in bed and suicidal thoughts, plans and attempts in Korean adolescents. BMJ Open 2015, 5, e008766. [Google Scholar] [CrossRef] [PubMed]
- Vandenbulck, J. Television viewing, computer game playing, and internet use and self-reported time to bed and time out of bed in secondary-school children. Sleep 2004, 27, 101–104. [Google Scholar] [CrossRef] [PubMed]
- Gupta, N.; Garg, S.; Arora, K. Pattern of mobile phone usage and its effects on psychological health, sleep, and academic performance in students of a medical university. Nat. J. Physiol. Pharm. Pharmacol. 2016, 6, 132. [Google Scholar] [CrossRef]
- Cheung, L.M.; Wong, W.S. The effects of insomnia and internet addiction on depression in Hong Kong Chinese adolescents: An exploratory cross-sectional analysis. J. Sleep Res. 2011, 20, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Aboujaoude, E. Problematic Internet use: An overview. World Psychiatry 2010, 9, 85–90. [Google Scholar] [CrossRef]
- Kim, K.; Ryu, E.; Chon, M.Y.; Yeun, E.J.; Choi, S.Y.; Seo, J.S.; Nam, B.W. Internet addiction in Korean adolescents and its relation to depression and suicidal ideation: A questionnaire survey. Int. J. Nurs. Stud. 2006, 43, 185–192. [Google Scholar] [CrossRef]
- Oshima, N.; Nishida, A.; Shimodera, S.; Tochigi, M.; Ando, S.; Yamasaki, S.; Okazaki, Y.; Sasaki, T. The suicidal feeling, self-injury, and mobile phone use after lights out in adolescents. J. Pediatric Psychol. 2012, 37, 1023–1030. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.J.; Park, J.; Kim, S.; Cho, S.J.; Kim, S.J. Academic performance among adolescents with behaviorally induced insufficient sleep syndrome. J. Clin. Sleep Med. 2015, 11, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.J.; Cho, S.J.; Cho, I.H.; Kim, S.J. Insufficient sleep and suicidality in adolescents. Sleep 2012, 35, 455–460. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Oh, J.H.; Kim, S.M.; Um, Y.H.; Seo, H.J.; Jeong, J.H.; Hong, S.C.; Kim, T.W. Effect of delaying school start time on sleep quality, emotions, and performance in Korean adolescents. Sleep Med. Res. 2019, 10, 1–7. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Male | Female | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Suicidal Ideation | Suicide Planning | Suicidal Ideation | Suicide Planning | ||||||
| Adjusted OR | 95% CI | Adjusted OR | 95% CI | Adjusted OR | 95% CI | Adjusted OR | 95% CI | ||
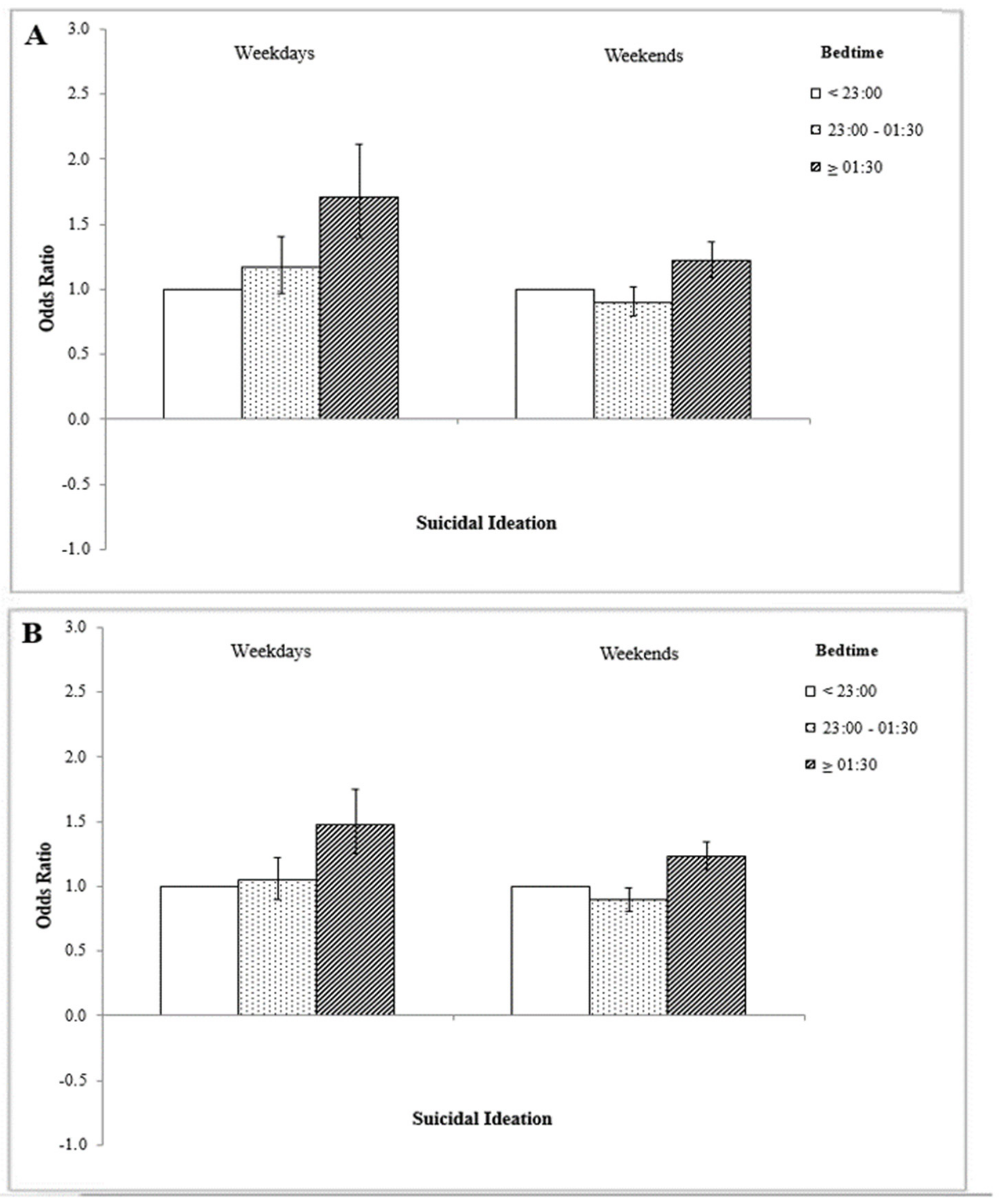
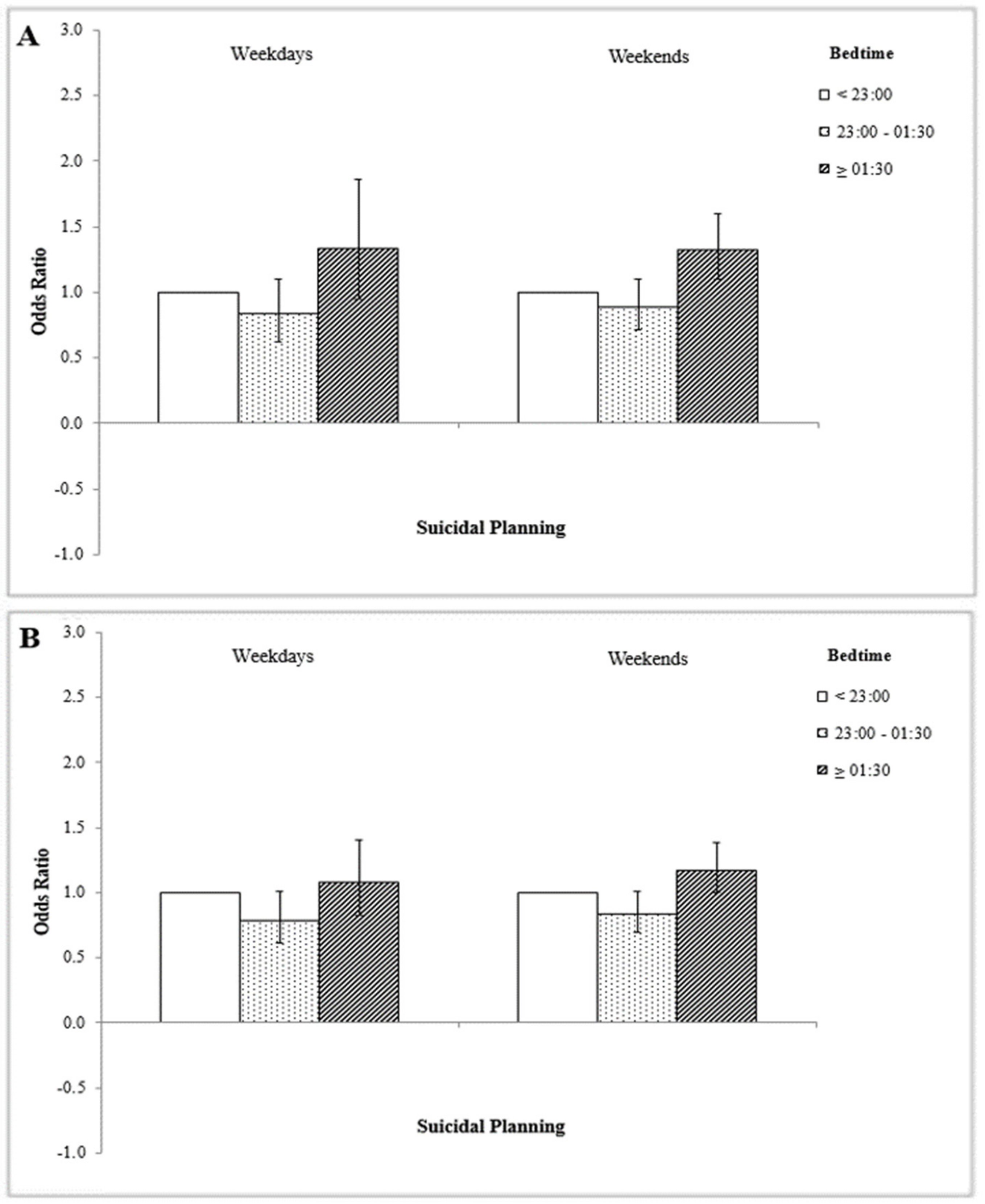
| Bedtime | <23:00 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| 23:00–01:30 | 0.97 | (0.86–1.10) | 0.90 | (0.74–1.10) | 0.98 | (0.89–1.08) | 0.96 | (0.81–1.15) | |
| ≥01:30 | 1.29 | (1.16–1.45) | 1.41 | (1.16–1.70) | 1.32 | (1.20–1.44) | 1.21 | (1.03–1.43) | |
| Age | 12–15 | 1.29 | (1.15–1.44) | 1.66 | (1.40–1.97) | 1.69 | (1.55–1.85) | 2.17 | (1.85–2.55) |
| 16–18 | 1.00 | 1.00 | 1.00 | 1.00 | |||||
| Allowance | Low | 1.09 | (0.94–1.26) | 1.01 | (0.80–1.28) | 1.09 | (0.98–1.22) | 1.11 | (0.91–1.35) |
| Lower Middle | 0.98 | (0.86–1.13) | 0.84 | (0.67–1.05) | 0.94 | (0.84–1.05) | 0.93 | (0.77–1.13) | |
| Upper Middle | 0.95 | (0.82–1.09) | 0.94 | (0.75–1.17) | 0.96 | (0.86–1.07) | 0.86 | (0.71–1.04) | |
| High | 1.00 | 1.00 | 1.00 | 1.00 | |||||
| Economic Status | Low | 1.43 | (1.25–1.63) | 1.19 | (0.96–1.48) | 1.34 | (1.19–1.50) | 1.38 | (1.15–1.65) |
| Middle | 0.83 | (0.75–0.92) | 0.73 | (0.61–0.88) | 0.89 | (0.82–0.97) | 0.83 | (0.72–0.97) | |
| High | 1.00 | 1.00 | 1.00 | 1.00 | |||||
| Grade | High | 0.79 | (0.71–0.89) | 0.75 | (0.62–0.91) | 0.80 | (0.73–0.87) | 0.78 | (0.67–0.91) |
| Middle | 0.84 | (0.75–0.95) | 0.87 | (0.72–1.06) | 0.80 | (0.73–0.88) | 0.77 | (0.65–0.91) | |
| Low | 1.00 | 1.00 | 1.00 | 1.00 | |||||
| Smoking Status | Never | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Ever | 1.47 | (1.32–1.65) | 1.41 | (1.16–1.71) | 1.65 | (1.43–1.89) | 1.94 | (1.59–2.36) | |
| Alcohol Status | Never | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Ever | 1.44 | (1.29–1.60) | 1.63 | (1.36–1.97) | 1.64 | (1.51–1.78) | 1.82 | (1.57–2.11) | |
| Physical Activity | Low | 0.97 | (0.88–1.06) | 0.91 | (0.77–1.07) | 0.77 | (0.70–0.84) | 0.68 | (0.59–0.79) |
| High | 1.00 | 1.00 | 1.00 | 1.00 | |||||
| Self-Reported Health Status | High | 0.24 | (0.20–0.28) | 0.25 | (0.20–0.32) | 0.24 | (0.21–0.27) | 0.22 | (0.19–0.27) |
| Middle | 0.52 | (0.44–0.62) | 0.52 | (0.40–0.68) | 0.49 | (0.44–0.55) | 0.51 | (0.42–0.61) | |
| Low | 1.00 | 1.00 | 1.00 | 1.00 | |||||
| Problematic Mobile Phone Use | Yes | 1.52 | (1.38–1.69) | 1.05 | (0.89–1.24) | 1.86 | (1.69–2.05) | 1.45 | (1.21–1.74) |
| No | 1.00 | 1.00 | 1.00 | 1.00 | |||||
| Variables | Suicidal Ideation | |||||
|---|---|---|---|---|---|---|
| <23:00 | 23:00–01:30 | ≥01:30 | ||||
| Adjusted OR | Adjusted OR | 95% CI | Adjusted OR | 95% CI | ||
| Male | ||||||
| Problematic Mobile Phone Use | Yes | 1.00 | 1.03 | (0.89–1.19) | 1.31 | (1.15–1.49) |
| No | 1.00 | 0.84 | (0.67–1.06) | 1.25 | (1.00–1.56) | |
| Grade | High | 1.00 | 1.00 | (0.82–1.22) | 1.33 | (1.10–1.61) |
| Middle | 1.00 | 0.99 | (0.78–1.26) | 1.26 | (1.01–1.57) | |
| Low | 1.00 | 0.94 | (0.77–1.16) | 1.30 | (1.06–1.58) | |
| Self-Reported Health Status | High | 1.00 | 0.95 | (0.82–1.11) | 1.34 | (1.15–1.56) |
| Middle | 1.00 | 0.92 | (0.73–1.15) | 1.21 | (0.97–1.50) | |
| Low | 1.00 | 1.29 | (0.89–1.86) | 1.31 | (0.93–1.86) | |
| Physical Activity | Low | 1.00 | 0.92 | (0.78–1.08) | 1.26 | (1.07–1.48) |
| High | 1.00 | 1.03 | (0.87–1.22) | 1.32 | (1.11–1.56) | |
| Female | ||||||
| Problematic Mobile Phone Use | Yes | 1.00 | 0.98 | (0.89–1.09) | 1.27 | (1.15–1.40) |
| No | 1.00 | 0.99 | (0.79–1.24) | 1.57 | (1.27–1.94) | |
| Grade | High | 1.00 | 0.93 | (0.80–1.10) | 1.32 | (1.13–1.53) |
| Middle | 1.00 | 0.93 | (0.77–1.12) | 1.31 | (1.08–1.57) | |
| Low | 1.00 | 1.07 | (0.91–1.26) | 1.32 | (1.13–1.53) | |
| Self-Reported Health Status | High | 1.00 | 0.97 | (0.85–1.10) | 1.28 | (1.13–1.45) |
| Middle | 1.00 | 0.92 | (0.77–1.10) | 1.29 | (1.10–1.51) | |
| Low | 1.00 | 1.26 | (0.92–1.71) | 1.54 | (1.20–1.99) | |
| Physical Activity | Low | 1.00 | 0.97 | (0.86–1.09) | 1.32 | (1.19–1.48) |
| High | 1.00 | 1.01 | (0.85–1.20) | 1.29 | (1.08–1.52) | |
| Variables | Suicide Planning | |||||
|---|---|---|---|---|---|---|
| <23:00 | 23:00–01:30 | ≥01:30 | ||||
| Adjusted OR | Adjusted OR | 95% CI | Adjusted OR | 95% CI | ||
| Male | ||||||
| Problematic Mobile Phone Use | Yes | 1.00 | 0.88 | (0.69–1.14) | 1.42 | (1.13–1.78) |
| No | 1.00 | 0.92 | (0.65–1.29) | 1.39 | (0.99–1.94) | |
| Grade | High | 1.00 | 0.93 | (0.66–1.31) | 1.62 | (1.18–2.22) |
| Middle | 1.00 | 0.83 | (0.55–1.27) | 1.53 | (1.06–2.21) | |
| Low | 1.00 | 0.94 | (0.67–1.33) | 1.18 | (0.86–1.62) | |
| Self-Reported Health Status | High | 1.00 | 0.83 | (0.64–1.08) | 1.41 | (1.10–1.82) |
| Middle | 1.00 | 0.94 | (0.63–1.40) | 1.10 | (0.76–1.59) | |
| Low | 1.00 | 1.31 | (0.71–2.44) | 2.38 | (1.33–4.26) | |
| Physical Activity | Low | 1.00 | 0.80 | (0.59–1.07) | 1.15 | (0.88–1.50) |
| High | 1.00 | 1.00 | (0.76–1.33) | 1.71 | (1.29–2.28) | |
| Female | ||||||
| Problematic Mobile Phone Use | Yes | 1.00 | 0.98 | (0.81–1.19) | 1.13 | (0.94–1.35) |
| No | 1.00 | 0.89 | (0.60–1.30) | 1.70 | (1.18–2.43) | |
| Grade | High | 1.00 | 0.88 | (0.67–1.16) | 1.19 | (0.91–1.57) |
| Middle | 1.00 | 0.89 | (0.63–1.26) | 1.17 | (0.85–1.62) | |
| Low | 1.00 | 1.10 | (0.82–1.47) | 1.27 | (0.97–1.67) | |
| Self-Reported Health Status | High | 1.00 | 0.92 | (0.73–1.16) | 1.24 | (0.96–1.59) |
| Middle | 1.00 | 1.02 | (0.75–1.38) | 1.24 | (0.94–1.63) | |
| Low | 1.00 | 1.01 | (0.65–1.58) | 1.15 | (0.80–1.65) | |
| Physical Activity | Low | 1.00 | 0.99 | (0.80–1.22) | 1.25 | (1.02–1.53) |
| High | 1.00 | 0.90 | (0.66–1.23) | 1.13 | (0.85–1.52) | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeong, W.; Kim, Y.K.; Lee, H.J.; Jang, J.; Kim, S.; Park, E.-C.; Jang, S.-I. Association of Bedtime with both Suicidal Ideation and Suicide Planning among Korean Adolescents. Int. J. Environ. Res. Public Health 2019, 16, 3817. https://doi.org/10.3390/ijerph16203817
Jeong W, Kim YK, Lee HJ, Jang J, Kim S, Park E-C, Jang S-I. Association of Bedtime with both Suicidal Ideation and Suicide Planning among Korean Adolescents. International Journal of Environmental Research and Public Health. 2019; 16(20):3817. https://doi.org/10.3390/ijerph16203817
Chicago/Turabian StyleJeong, Wonjeong, Yun Kyung Kim, Hyeon Ji Lee, Jieun Jang, Selin Kim, Eun-Cheol Park, and Sung-In Jang. 2019. "Association of Bedtime with both Suicidal Ideation and Suicide Planning among Korean Adolescents" International Journal of Environmental Research and Public Health 16, no. 20: 3817. https://doi.org/10.3390/ijerph16203817
APA StyleJeong, W., Kim, Y. K., Lee, H. J., Jang, J., Kim, S., Park, E.-C., & Jang, S.-I. (2019). Association of Bedtime with both Suicidal Ideation and Suicide Planning among Korean Adolescents. International Journal of Environmental Research and Public Health, 16(20), 3817. https://doi.org/10.3390/ijerph16203817