The Association between Socioeconomic Status, Smoking, and Chronic Disease in Inner Mongolia in Northern China

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. NHSS Methods in Inner Mongolia
2.2. Ethics Approval and Consent to Participate
2.3. Variable Definitions
2.4. Data Analyses
3. Results
3.1. Smoking Prevalence according to Sex and Socio-Demographic Characteristics
3.2. Socioeconomic Status and Smoking Prevalence According to Sex
3.3. Chronic Disease Prevalence According to Sex, Socioeconomic Status, and Socio-Demographic Characteristics
3.4. Predictors of Chronic Conditions by Socioeconomic Status Interaction with Smoking
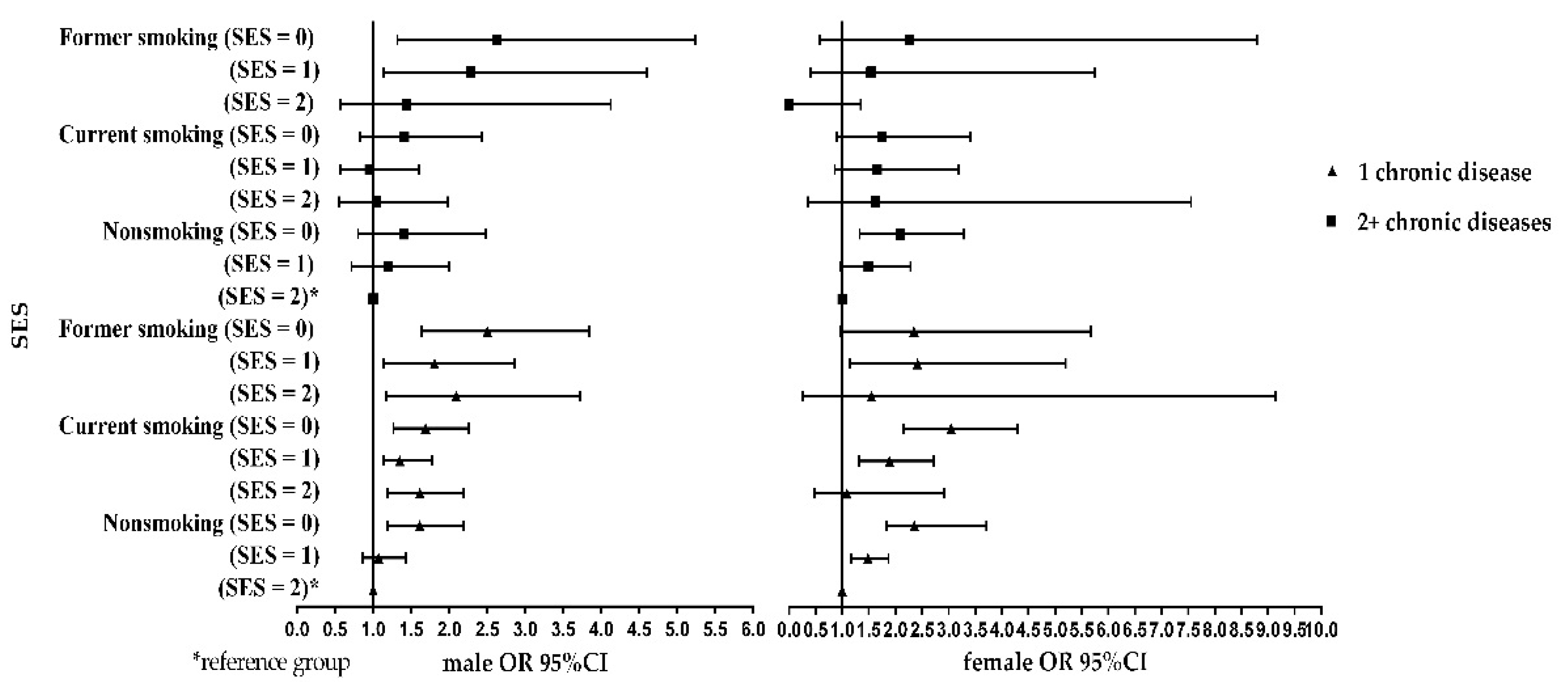
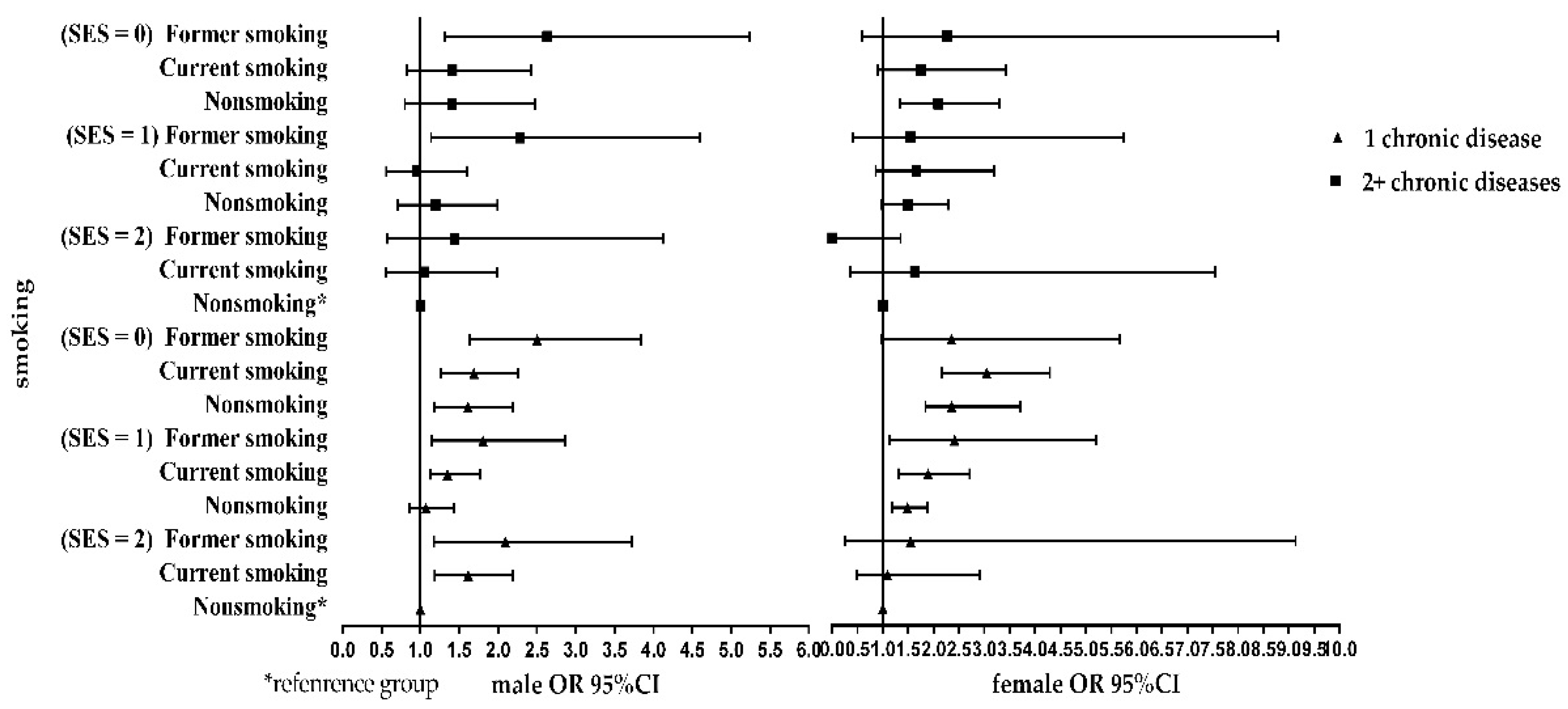
3.5. Simple Effect of Chronic Disease Risk at Different Socioeconomic Status or Smoking Status
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Newacheck, P.W.; Hung, Y.Y.; Park, M.J.; Brindis, C.D.; Irwin, C.J. Disparities in adolescent health and health care: Does socioeconomic status matter? Health Serv. Res. 2003, 38, 1235–1252. [Google Scholar] [CrossRef] [PubMed]
- Frank, J.W.; Cohen, R.; Yen, I.; Balfour, J.; Smith, M. Socioeconomic gradients in health status over 29 years of follow-up after midlife: The Alameda county study. Soc. Sci. Med. 2003, 57, 2305–2323. [Google Scholar] [CrossRef] [PubMed]
- Murray, C.J.; Lopez, A.D. Alternative projections of mortality and disability by cause 1990–2020: Global Burden of Disease Study. Lancet 1997, 349, 1498–1504. [Google Scholar] [CrossRef]
- Guang, Y.Z. The analysis of risk factor for smoking behavior in Guangdong Province of China. Chin. J. Health Stat. 2013, 4, 561–562. [Google Scholar]
- Yun, W.J.; Rhee, J.A.; Kim, S.A.; Kweon, S.S.; Lee, Y.H.; Ryu, S.Y.; Park, S.W.; Kim, D.H.; Shin, M.H. Household and area income levels are associated with smoking status in the Korean adult population. BMC Public Health 2015, 15, 39. [Google Scholar] [CrossRef] [PubMed]
- Hosseinpoor, A.R.; Parker, L.A.; D’Espaignet, E.T.; Chatterji, S. Socioeconomic Inequality in Smoking in Low-Income and Middle-Income Countries: Results from the World Health Survey. PLoS ONE 2012, 7, e42843. [Google Scholar] [CrossRef] [PubMed]
- Mathur, C.; Stigler, M.H.; Perry, C.L.; Arora, M.; Reddy, K.S. Differences in prevalence of tobacco use among Indian urban youth: The role of socioeconomic status. Nicotine Tob. Res. 2008, 10, 109–116. [Google Scholar] [CrossRef]
- Bauld, L.; Judge, K.; Platt, S. Assessing the impact of smoking cessation services on reducing health inequalities in England: Observational study. Tob. Control 2007, 16, 400. [Google Scholar] [CrossRef]
- Jha, P.; Peto, R.; Zatonski, W.; Boreham, J.; Jarvis, M.J.; Lopez, A.D. Social inequalities in male mortality, and in male mortality from smoking: Indirect estimation from national death rates in England and Wales, Poland, and North America. Lancet 2006, 368, 367–370. [Google Scholar] [CrossRef]
- Lam, C. The socioeconomics of hypertension. Hypertension 2011, 58, 140–141. [Google Scholar] [CrossRef]
- Fu, C.; Chen, Y.; Wang, F.; Wang, X.; Song, J.; Jiang, Q. High prevalence of hyperglycaemia and the impact of high household income in transforming rural China. BMC Public Health 2011, 11, 862. [Google Scholar] [CrossRef] [PubMed]
- Niu, S.R.; Yang, G.H.; Chen, Z.M.; Wang, J.L.; Wang, G.H.; He, X.Z.; Schoepff, H.; Boreham, J.; Pan, H.C.; Peto, R. Emerging tobacco hazards in China: 2. Early mortality results from a prospective study. BMJ Clin. Res. 1998, 317, 1423–1424. [Google Scholar] [CrossRef]
- Khan, F.S.; Lotia-Farrukh, I.; Khan, A.J.; Siddiqui, S.T.; Sajun, S.Z.; Malik, A.A.; Burfat, A.; Arshad, M.H.; Codlin, A.J.; Reininger, B.M. The burden of non-communicable disease in transition communities in an Asian megacity: Baseline findings from a cohort study in Karachi, Pakistan. PLoS ONE 2013, 8, 276. [Google Scholar] [CrossRef] [PubMed]
- Kengne, A.P.; Junerose, M.Z.; Amoah, A.G.; Mbanya, J.C. Cardiovascular diseases and diabetes as economic and developmental challenges in Africa. Prog. Cardiovasc. Dis. 2013, 56, 302–313. [Google Scholar] [CrossRef] [PubMed]
- Tang, S.L.; Ehiri, J.; Long, Q. China’s biggest, most neglected health challenge: Non-communicable diseases. Chin. J. Health Policy 2013, 2, 7. [Google Scholar] [CrossRef] [PubMed]
- Alwan, A.; Alwan, A. Global status report on noncommunicable diseases 2010. Women 2011, 47, 2562–2563. [Google Scholar] [CrossRef]
- Sharma, A.; Lewis, S.; Szatkowski, L. Insights into social disparities in smoking prevalence using Mosaic, a novel measure of socioeconomic status: An analysis using a large primary care dataset. BMC Public Health 2010, 10, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Flint, A.J.; Novotny, T.E. Poverty status and cigarette smoking prevalence and cessation in the United States, 1983–1993: The independent risk of being poor. Tob. Control 1997, 6, 14–18. [Google Scholar] [CrossRef]
- Yang, T.; Barnett, R.; Rockett, I.R.H.; Yang, X.Y.; Dan, W.; Zheng, W.; Lu, L. The impact of regional economic reliance on the tobacco industry on current smoking in China. Health Place 2015, 33, 159–171. [Google Scholar] [CrossRef]
- Xu, Y.; Xu, S.; Wu, Q.; Wang, L.; Liu, H.; Zhao, Y.; Lyu, Q. Smoking and secondhand smoking in Zhejiang province, China. Zhonghua Liu Xing Bing Xue Za Zhi 2014, 35, 1343–1348. [Google Scholar]
- Whitlock, G.; Macmahon, S.; Vander, H.S.; Davis, P.; Jackson, R.; Norton, R. Socioeconomic distribution of smoking in a population of 10,529 New Zealanders. N. Z. Med. J. 1997, 110, 327–330. [Google Scholar] [CrossRef] [PubMed]
- Osler, M.; Holstein, B.; Avlund, K.; Damsgaard, M.T.; Rasmussen, N.K. Socioeconomic position and smoking behaviour in Danish adults. Scand. J. Public Health 2001, 29, 32. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Yuan, Z.; Maddock, J.E.; Zou, J.; Zheng, Z.; Zhou, W.; Zheng, H. Chronic disease prevalence and influencing factors among rural residents in Jiangxi, China. Int. Health 2014, 6, 106–111. [Google Scholar] [CrossRef]
- International, C. Closing the gap in a generation: Health equity through action on the social determinants of health. An international conference based on the work of the Commission on Social Determinants of Health, London, UK, 6–7 November 2008. Glob. Health Promot. 2009, 16 (Suppl. 1), 7–8. [Google Scholar] [CrossRef]
- Mocumbi, A.O. Focus on non-communicable diseases: An important agenda for the African continent. Cardiovasc. Diagn. Ther. 2013, 3, 193–195. [Google Scholar] [CrossRef] [PubMed]
- Daar, A.S.; Singer, P.A.; Persad, D.L.; Pramming, S.K.; Matthews, D.R.; Beaglehole, R.; Bernstein, A.; Borysiewicz, L.K.; Colagiuri, S.; Ganguly, N. Grand challenges in chronic non-communicable diseases. Nature 2007, 450, 494–496. [Google Scholar] [CrossRef] [PubMed]
- Hanson, M.; Gluckman, P.; Nutbeam, D.; Hearn, J. Priority actions for the non-communicable disease crisis. Lancet 2011, 378, 566. [Google Scholar] [CrossRef]
- Sen, A. Why health equity? Health Econ. 2002, 11, 659–666. [Google Scholar] [CrossRef]
- Huang, X.; Gu, X.F.; Wang, Y.P. Research on the prevalence status of chronic disease in the rural poor residents. Mod. Prev. Med. 2009, 36, 4465–4467. [Google Scholar]
- Schäfer, I.; Hansen, H.; Schön, G.; Höfels, S.; Altiner, A.; Dahlhaus, A.; Gensichen, J.; Riedelheller, S.; Weyerer, S.; Blank, W.A. The influence of age, gender and socio-economic status on multimorbidity patterns in primary care. First results from the multicare cohort study. BMC Health Serv. Res. 2012, 12, 1–15. [Google Scholar] [CrossRef]
- Mercer, S.W.; Watt, G.C. The inverse care law: Clinical primary care encounters in deprived and affluent areas of Scotland. Ann. Fam. Med. 2007, 5, 503–510. [Google Scholar] [CrossRef] [PubMed]
- Uijen, A.A.; Eh, V.D.L. Multimorbidity in primary care: Prevalence and trend over the last 20 years. Eur. J. Gen. Pract. 2008, 14 (Suppl. 1), 28–32. [Google Scholar] [CrossRef]
- Alaba, O.; Chola, L. The social determinants of multimorbidity in South Africa. Int. J. Equity Health 2013, 12, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Chandola, T.; Ferrie, J.; Sacker, A.; Marmot, M. Social inequalities in self reported health in early old age: Follow-up of prospective cohort study. BMJ 2007, 334, 990. [Google Scholar] [CrossRef] [PubMed]
- Arokiasamy, P.; Uttamacharya, U.; Jain, K.; Biritwum, R.B.; Yawson, A.E.; Wu, F.; Guo, Y.; Maximova, T.; Espinoza, B.M.; Rodríguez, A.S. The impact of multimorbidity on adult physical and mental health in low- and middle-income countries: What does the study on global ageing and adult health (SAGE) reveal? BMC Med. 2015, 13, 1–16. [Google Scholar] [CrossRef]
- Smith, W.C.; Anderson, E.; Salinas, D.; Horvatek, R.; Baker, D.P. A meta-analysis of education effects on chronic disease: The causal dynamics of the Population Education Transition Curve. Soc. Sci. Med. 2015, 127, 29–40. [Google Scholar] [CrossRef] [PubMed]
- Malan, Z.; Mash, R.; Everett-Murphy, K. Qualitative evaluation of primary care providers experiences of a training programme to offer brief behaviour change counselling on risk factors for non-communicable diseases in South Africa. BMC Fam. Pract. 2015, 16, 1–10. [Google Scholar] [CrossRef]
- Rehm, J.; Room, R.; Monteiro, M.; Gmel, G.; Graham, K.; Rehn, N.; Sempos, C.T.; Jernigan, D. Alcohol as a risk factor for global burden of disease. Eur. Addict. Res. 2003, 9, 157–164. [Google Scholar] [CrossRef]
- Bryant, J.; Bonevski, B.; Paul, C.; McElduff, P.; Attia, J. A systematic review and meta-analysis of the effectiveness of behavioural smoking cessation interventions in selected disadvantaged groups. Addiction 2011, 106, 1568–1585. [Google Scholar] [CrossRef]
- Hiscock, R.; Bauld, L.; Amos, A.; Fidler, J.A.; Munafò, M. Socioeconomic status and smoking: A review. Ann. N. Y. Acad. Sci. 2012, 1248, 107–123. [Google Scholar] [CrossRef]
- Radi, S.; Ostry, A.; Lamontagne, A.D. Job stress and other working conditions: relationships with smoking behaviors in a representative sample of working Australians. Am. J. Ind. Med. 2010, 50, 584–596. [Google Scholar] [CrossRef]
- Siahpush, M.; Borland, R.; Scollo, M. Smoking and financial stress. Tob. Control 2003, 12, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Aryal, U.R.; Bhatta, D.N. Perceived benefits and health risks of cigarette smoking among young adults: Insights from a cross-sectional study. Tob. Induc. Dis. 2014, 13, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Millar, W.J. Age of smoking initiation: Implications for quitting. Health Rep. 1998, 9, 39–48. [Google Scholar] [CrossRef]
- Yan, L.I.; Ungeer, J.; Gong, J. Stressful Life Events and Smoking in Adolescents of Wuhan. Chin. Ment. Health J. 2003, 17, 113–116. [Google Scholar]
- Cosci, F.; Zagà, V.; Bertoli, G.; Campiotti, A. Significant others, knowledge, and belief on smoking as factors associated with tobacco use in italian adolescents. ISRN Addict. 2012, 2013. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Wei, Y.L.; Qi-Jun, D.U. Smoking Survey among Adolescent in Chendgu. Mod. Prev. Med. 2005, 9, 57. [Google Scholar]
- Mckee, S.A.; Krishnan-Sarin, S.; Shi, J.; Mase, T.; O’Malley, S.S. Modeling the effect of alcohol on smoking lapse behavior. Psychopharmacology 2006, 189, 201–210. [Google Scholar] [CrossRef]
- Lee, E.K.; Kim, O.S.; Hong, J.Y. Characteristics and Factors Associated with Problem Drinking in Male Workers. Asian Nurs. Res. 2015, 27, 132–137. [Google Scholar] [CrossRef]
- Levinson, A.H.; Valverde, P.; Garrett, K.; Kimminau, M.; Burns, E.K.; Albright, K.; Flynn, D. Community-based navigators for tobacco cessation treatment: A proof-of-concept pilot study among low-income smokers. BMC Public Health 2015, 15, 627. [Google Scholar] [CrossRef]
- Cosgrove, K.P.; Wang, S.; Kim, S.J.; Mcgovern, E.; Nabulsi, N.; Gao, H.; Labaree, D.; Tagare, H.D.; Sullivan, J.M.; Morris, E.D. Sex differences in the brain’s dopamine signature of cigarette smoking. J. Neurosci. Off. J. Soc. Neurosci. 2014, 34, 16851–16855. [Google Scholar] [CrossRef] [PubMed]
- Smith, P.H.; Kasza, K.A.; Hyland, A.; Fong, G.T.; Borland, R.; Brady, K.; Carpenter, M.J.; Hartwell, K.; Cummings, K.M.; McKee, S.A. Gender differences in medication use and cigarette smoking cessation: Results from the International Tobacco Control Four Country Survey. Nicotine Tob. Res. 2015, 17, 463–472. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.C.; Zhang, J.Y.; Yan, L.X.; Zi-Long, L.U.; Cai, X.N.; Chu, J.; Guo, X.L. Survey on the Status of Smoking in Adult Population in Shandong Province of China during 2011. Mod. Prev. Med. 2014, 41, 2202. [Google Scholar]



{kind=link}
{kind=link}
| Variable | Male (n = 6721) | Female (n = 6814) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Non-Smoking | Former Smoking | Current Smoking | χ2 | p-Value | Non-Smoking | Former Smoking | Current Smoking | χ2 | p-Value | |
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | |||||
| SES score | 89.806 | <0.001 ^ | 102.084 | <0.001 ^ | ||||||
| 2 | 747 (49.73) | 78 (5.19) | 677 (45.07) | 1158 (95.00) | 12 (0.98) | 49 (4.02) | ||||
| 1 | 1138 (40.10) | 149 (5.25) | 1551 (54.65) | 2445 (87.48) | 45 (1.61) | 305 (10.91) | ||||
| 0 | 684 (35.76) | 169 (8.83) | 1060 (55.41) | 1597 (83.09) | 30 (1.56) | 295 (15.35) | ||||
| Variable | Male | Female | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 0 | 1 | 2+ | χ2 | p-Value | 0 | 1 | 2+ | χ2 | p-Value | |
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | |||||
| SES score | 38.158 | <0.001 ^ | 199.854 | <0.001 ^ | ||||||
| 2 | 1348 (81.06) | 264 (15.87) | 51 (3.07) | 1287 (87.02) | 152 (10.28) | 40 (2.70) | ||||
| 1 | 2442 (80.20) | 477 (15.67) | 126 (4.14) | 2455 (76.96) | 567 (17.77) | 168 (5.27) | ||||
| 0 | 1489 (74.08) | 412 (20.50) | 109 (5.42) | 1427 (66.78) | 556 (26.02) | 154 (7.21) | ||||
| Age | 998.204 | <0.001 ^ | 1474.931 | <0.001 ^ | ||||||
| <45 | 2807 (94.07) | 165 (5.53) | 12 (0.40) | 2858 (95.71) | 121 (4.05) | 7 (0.23) | ||||
| 45~59 | 1618 (73.71) | 487 (22.19) | 90 (4.10) | 1581 (70.45) | 544 (24.24) | 119 (5.30) | ||||
| 60~ | 857 (55.58) | 501 (32.49) | 184 (11.93) | 737 (46.53) | 611 (38.57) | 236 (14.90) | ||||
| Ethnicity | 8.638 | 0.071 | 27.531 | <0.001 ^ | ||||||
| Han | 4214 (78.50) | 918 (17.10) | 236 (4.40) | 3977 (74.77) | 1045 (19.65) | 297 (5.58) | ||||
| Mongolian | 823 (80.53) | 165 (16.14) | 34 (3.33) | 897 (82.07) | 157 (14.36) | 39 (3.57) | ||||
| Others | 231 (73.33) | 68 (21.59) | 16 (5.08) | 289 (75.06) | 72 (18.70) | 24 (6.23) | ||||
| Employment status | 543.707 | <0.001 ^ | 568.705 | <0.001 ^ | ||||||
| Unemployed | 477 (69.03) | 150 (21.71) | 64 (9.26) | 888 (64.44) | 362 (26.27) | 128 (9.29) | ||||
| Retired | 396 (51.10) | 273 (35.23) | 106 (13.68) | 441 (51.70) | 296 (34.70) | 116 (13.60) | ||||
| Employed | 4404 (83.90) | 729 (13.89) | 116 (2.21) | 3836 (83.94) | 616 (13.48) | 118 (2.58) | ||||
| Marital status | 257.328 | <0.001 ^ | 437.693 | <0.001 ^ | ||||||
| Single | 899 (97.19) | 24 (2.59) | 2 (0.22) | 614 (96.69) | 14 (2.20) | 7 (1.10) | ||||
| Widowed or divorced | 222 (64.72) | 86 (25.07) | 35 (10.20) | 318 (49.00) | 232 (35.75) | 99 (15.25) | ||||
| Married | 4156 (76.28) | 1043 (19.14) | 249 (4.57) | 4235 (76.71) | 1030 (18.66) | 256 (4.64) | ||||
| Urban/Rural | 10.144 | 0.006 & | 13.912 | <0.001 ^ | ||||||
| Urban | 1656 (76.60) | 394 (18.22) | 112 (5.18) | 1740 (75.69) | 406 (17.66) | 153 (6.66) | ||||
| Rural | 3626 (79.53) | 759 (16.65) | 174 (3.82) | 3436 (76.10) | 870 (19.27) | 209 (4.63) | ||||
| Smoking status | 102.811 | <0.001 ^ | 20.759 | <0.001 ^ | ||||||
| Current smoking | 2609 (79.35) | 570 (17.34) | 109 (3.32) | 458 (70.57) | 157 (24.19) | 34 (5.24) | ||||
| Former smoking | 237 (59.85) | 117 (29.55) | 42 (10.61) | 56 (64.37) | 25 (28.74) | 6 (6.90) | ||||
| Non-smoking | 2059(80.12) | 397 (15.45) | 114 (4.44) | 3991 (76.72) | 941 (18.09) | 270 (5.19) | ||||
| Alcohol use | 16.452 | <0.001 ^ | 5.398 | 0.067 | ||||||
| Yes | 2314 (79.33) | 512 (17.55) | 91 (3.12) | 261 (80.06) | 56 (17.18) | 9 (2.76) | ||||
| No | 2968 (78.02) | 641 (16.85) | 195 (5.13) | 4914 (75.75) | 1220 (18.81) | 353 (5.44) | ||||
| BMI | 124.722 | <0.001 ^ | 273.888 | <0.001 ^ | ||||||
| <24 | 3245 (82.89) | 540 (13.79) | 130 (3.32) | 3553 (81.92) | 623 (14.36) | 161 (3.71) | ||||
| 24~28 | 1614 (74.52) | 441 (20.36) | 111 (5.12) | 1320 (68.11) | 472 (24.36) | 146 (7.53) | ||||
| ≥28 | 408 (65.81) | 169 (27.26) | 43 (6.94) | 286 (55.21) | 180 (34.75) | 52 (10.04) | ||||
| Education level | 14.583 | <0.001 ^ | 167.937 | <0.001 ^ | ||||||
| Middle school and below | 3621 (77.36) | 843 (18.01) | 217 (4.64) | 3602 (71.92) | 1095 (21.87) | 311 (6.21) | ||||
| High school and above | 1658 (81.39) | 310 (15.22) | 69 (3.39) | 1567 (87.15) | 180 (10.01) | 51 (2.84) | ||||
| Household annual income | 24.907 | <0.001 ^ | 90.369 | <0.001 ^ | ||||||
| Low | 1800 (75.47) | 458 (19.20) | 127 (5.32) | 1709 (69.53) | 584 (23.76) | 165 (6.71) | ||||
| Middle | 2817 (80.05) | 575 (16.34) | 127 (3.61) | 2810 (79.04) | 581 (16.34) | 164 (4.61) | ||||
| High | 665 (81.40) | 120 (14.69) | 32 (3.92) | 657 (82.02) | 111 (13.86) | 33 (4.12) | ||||
| Variable | Male | Female | ||
|---|---|---|---|---|
| 1 | 2+ | 1 | 2+ | |
| OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| Univariate model $ | ||||
| (SES = 2) Nonsmoking | 1 | 1 | 1 | 1 |
| (SES = 1) Nonsmoking | 1.185 (0.972−1.557) | 1.332 (0.822−2.169) | 1.883 (1.513−2.344) * | 2.052 (1.381−3.453) * |
| (SES = 0) Nonsmoking | 1.825 (1.371−2.431) * | 1.756 (1.449−2.944) * | 3.273 (2.619−4.098) * | 3.344 (2.238−4.995) * |
| (SES = 2) Current smoking | 1.500 (1.119−2.211) * | 0.806 (0.438−1.488) | 1.026 (0.398−2.646) | 1.501 (0.348−6.475) |
| (SES = 1) Current smoking | 1.281 (0.991−1.656) | 0.819 (0.499−1.346) | 2.355 (1.677−3.349) * | 2.222 (1.199−4.125) * |
| (SES = 0) Current smoking | 1.704 (1.387−2.223) * | 1.436 (0.881−2.341) | 4.107 (2.995−5.631) * | 2.669 (1.436−4.962) * |
| (SES = 2) Former smoking | 3.267 (1.915−5.574) * | 2.460 (0.955−6.691) | 2.874 (0.767−14.767) | 0.000 (0.000−3.210) |
| (SES = 1) Former smoking | 2.828 (1.834−4.359) * | 4.718 (2.489−8.944) * | 3.866 (1.955−7.643) * | 3.261 (0.944−11.268) |
| (SES = 0) Former smoking | 3.752 (2.521−5.584) * | 4.773 (2.544−8.956) * | 4.312 (1.894−9.817) * | 5.255 (1.473−18.749) * |
| Multivariate model $# | ||||
| (SES = 2) Nonsmoking | 1 | 1 | 1 | 1 |
| (SES = 1) Nonsmoking | 1.072 (0.866−1.429) | 1.194 (0.715−1.996) | 1.485 (1.177−1.873) * | 1.493 (0.975−2.287) |
| (SES = 0) Nonsmoking | 1.613 (1.185−2.194) * | 1.410 (0.802−2.481) | 2.355 (1.842−3.713) * | 2.092 (1.329−3.292) * |
| (SES = 2) Current smoking | 1.615 (1.188−2.196) * | 1.047 (0.553−1.985) | 1.089 (0.487−2.913) | 1.628 (0.351−7.554) |
| (SES = 1) Current smoking | 1.352 (1.133−1.771) * | 0.952 (0.564−1.609) | 1.891 (1.316−2.715) * | 1.656 (0.861−3.193) |
| (SES = 0) Current smoking | 1.689 (1.269−2.257) * | 1.413 (0.823−2.428) | 3.044 (2.158−4.292) * | 1.750 (0.896−3.418) |
| (SES = 2) Former smoking | 2.094 (1.176−3.728) * | 1.443 (0.575−4.127) | 1.548 (0.262−9.137) | 0.000 (0.000−1.350) |
| (SES = 1) Former smoking | 1.808 (1.141−2.863) * | 2.287 (1.138−4.596) * | 2.414 (1.143−5.194) * | 1.541 (0.413−5.754) |
| (SES = 0) Former smoking | 2.505 (1.635−3.837) * | 2.631 (1.321−5.243) * | 2.350 (0.973−5.676) | 2.268 (0.585−8.789) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, X.; Zhang, T.; Wu, J.; Yin, S.; Nan, X.; Du, M.; Liu, A.; Wang, P. The Association between Socioeconomic Status, Smoking, and Chronic Disease in Inner Mongolia in Northern China. Int. J. Environ. Res. Public Health 2019, 16, 169. https://doi.org/10.3390/ijerph16020169
Wang X, Zhang T, Wu J, Yin S, Nan X, Du M, Liu A, Wang P. The Association between Socioeconomic Status, Smoking, and Chronic Disease in Inner Mongolia in Northern China. International Journal of Environmental Research and Public Health. 2019; 16(2):169. https://doi.org/10.3390/ijerph16020169
Chicago/Turabian StyleWang, Xuemei, Ting Zhang, Jing Wu, Shaohua Yin, Xi Nan, Maolin Du, Aiping Liu, and Peiyu Wang. 2019. "The Association between Socioeconomic Status, Smoking, and Chronic Disease in Inner Mongolia in Northern China" International Journal of Environmental Research and Public Health 16, no. 2: 169. https://doi.org/10.3390/ijerph16020169
APA StyleWang, X., Zhang, T., Wu, J., Yin, S., Nan, X., Du, M., Liu, A., & Wang, P. (2019). The Association between Socioeconomic Status, Smoking, and Chronic Disease in Inner Mongolia in Northern China. International Journal of Environmental Research and Public Health, 16(2), 169. https://doi.org/10.3390/ijerph16020169