Validation of the CIMI-Ethiopia Program and Seasonal Variation in Maternal Nutrient Intake in Enset (False Banana) Growing Areas of Southern Ethiopia

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Area
2.2. Study Design
2.3. Study Population
2.4. Sample Size Calculation
2.5. Sampling
2.6. Data Collection
2.7. Statistical Analysis
3. Results
3.1. Sociodemographic Characteristics of Participants
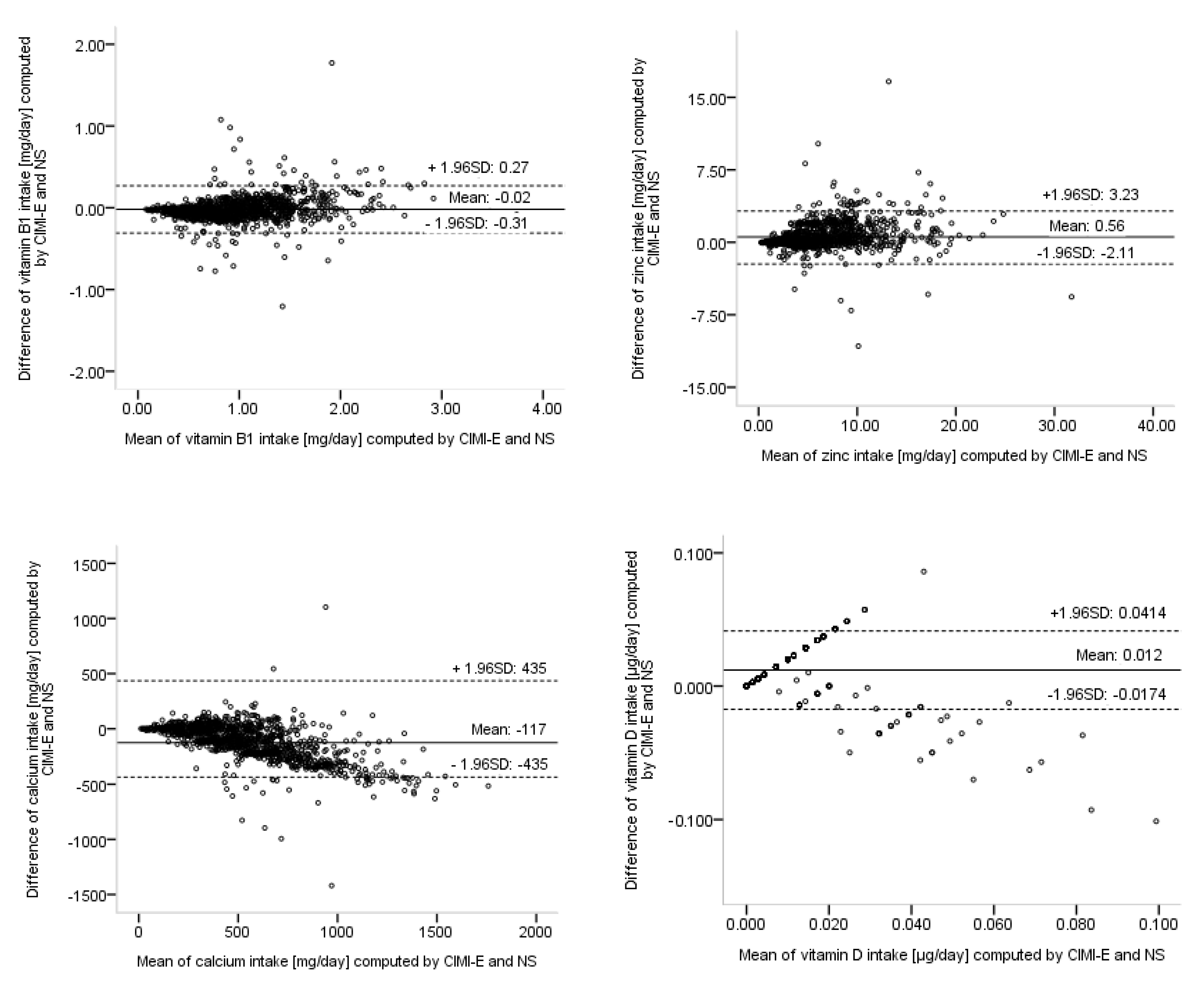
3.2. Validation of CIMI-Ethiopia
3.3. Seasonal Variation in Nutrinet Intake
4. Discussion
4.1. Validation of CIMI-Ethiopia
4.2. Seasonal Variation in Nutrient Intake
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Tulchinsky, T.H. Micronutrient Deficiency Conditions: Global Health Issues. BMC Public Health Rev. 2010, 32, 243–255. [Google Scholar] [CrossRef]
- WHO; WFP; UNICEF. Preventing and Controlling Micronutrient Deficiencies in Populations Affected by an Emergency: Multiple Vitamin and Mineral Supplements for Pregnant and Lactating Women, and for Children Aged 6 to 59 Months; WHO: Geneva, Switzerland, 2007; pp. 1–2. [Google Scholar]
- Gani, G.; Beenish, G.; Bashir, O.; Bhat, T.A.; Naseer, B.; Qadri, T.; Jan, N. Hidden hunger and its prevention by food processing: A review. IJUIM 2018, 2, 1–10. [Google Scholar]
- Brandt, S.A.; Spring, A.; Hiebsch, C.; Yntiso, G.; Tabogie, E.; Diro, M.; Wolde-Michael, G.; Tesfaye, S.; McCabe, J.T.; Shigeta, M. The “Tree Against Hunger” Enset-Based Agricultural Systems in Ethiopia; American Association for the Advancement of Science: Washington, DC, USA, 1997; Available online: http://users.clas.ufl.edu/aspring/publications/enset (accessed on 25 July 2019).
- Gebremedhin, S.; Enquselassie, F.; Umeta, M. Prevalence of prenatal zinc deficiency and its association with socio-demographic, dietary and health care related factors in Rural Sidama, Southern Ethiopia: A cross-sectional study. BMC Public Health 2011, 11, 898. [Google Scholar] [CrossRef] [PubMed]
- Gebreselassie, S.G.; Gase, F.E.; Deressa, M.U. Prevalence and Correlates of Prenatal Vitamin A Deficiency in Rural Sidama, Southern Ethiopia. J. Health Popul. Nutr. 2013, 31, 185–194. [Google Scholar] [CrossRef] [PubMed]
- Abebe, Y.; Bogale, A.; Hambidge, K.M.; Stoecker, B.J.; Arbide, I.; Teshome, A.; Krebs, N.F.; Westcott, J.E.; Bailey, K.B. Inadequate intakes of dietary zinc among pregnant women from subsistence households in Sidama, Southern Ethiopia. Public Health Nutr. 2008, 11, 379–386. [Google Scholar] [CrossRef]
- Borrell, J.S.; Biswas, M.K.; Goodwin, M.; Blomme, G.; Schwarzacher, T.; Heslop-Harrison, J.S.; Wendawek, A.M.; Berhanu, A.; Kallow, S.; Janssens, S.; et al. Enset in Ethiopia: A poorly characterized but resilient starch staple. Ann. Bot. 2019, 123, 747–766. [Google Scholar] [CrossRef]
- Daba, T.; Shigeta, M. Enset (Ensete Ventricosum) Production in Ethiopia: Its Nutritional and Socio-Cultural Values. Agric. Food Sci. Res. 2016, 3, 66–74. [Google Scholar] [CrossRef]
- Karssa, T.; Papini, A. Effect of Clonal Variation on Quality of Kocho, Traditional Fermented Food from Enset (Ensete Ventricosum), Musaceae. Int. J. Food Sci. Nutr. Eng. 2018, 8, 79–85. [Google Scholar] [CrossRef]
- Bezuneh, T.; Feleke, A. The production and utilization of the genus ensete in Ethiopia. Econ. Bot. 1966, 20, 65–70. Available online: http://www.jstor.org/stable/4252703 (accessed on 25 July 2019). [CrossRef]
- Abebe, Y.; Stoecker, B.J.; Hinds, M.J.; Gates, G.E. Nutritive value and sensory acceptability of corn- and kocho- based foods supplemented with legumes for infant feeding in Southern Ethiopia. Afr. J. Food Agric. Nutr. Dev. 2006, 6, 1–19. [Google Scholar]
- Shim, J.; Oh, K.; Kim, H.C. Dietary assessment methods in epidemiologic studies. Epidemiol. Health 2014, 36, e2014009. [Google Scholar] [CrossRef] [PubMed]
- Jati, I.R.A.P.; Widmer, C.; Purwestri, R.C.; Wirawan, N.N.; Gola, U.; Lambert, C.; Biesalski, H.K. Design and validation of a program to identify inadequate intake of iron, zinc, and vitamin A. Nutrition 2014, 30, 1310–1317. [Google Scholar] [CrossRef]
- Wald, J.P.; Asare, E.; Nakua, E.K.; Lambert, C.; Biesalski, H.K.; Gola, U.; Nohr, D. Dietary assessment using the CIMI approach: A case study from three districts of the Ashanti region in Ghana. In Proceedings of the 3rd International Conference on Global Food Security, Cape Town, South Africa, 3–6 December 2017. [Google Scholar]
- Wald, J.P.; Asare, E.; Nakua, E.K.; Nohr, D.; Lambert, C.; Riedel, S.; Gola, U.; Biesalski, H.K. Validation of a computer-based analysis tool for real-time dietary assessment within a Ghanaian region. NFS J. 2019, 16, 15–25. [Google Scholar] [CrossRef]
- Lambert, C.; Eleraky, L.; Mbwana, H.; Kinabo, J.; Biesalski, H.K.; Riedel, S.; Widmer, C.; Gola, U.; Stuetz, W. Validation of a food group based nutrition software to assess nutrient intake in Tanzania. In Proceedings of the Tropentag Conference, Ghent, Belgium, 17–19 September 2018. [Google Scholar]
- Desalegn, B.; Borko, T.; Lambert, C.; Widmer, C.; Gola, U.; Riedel, S.; Negese, T.; Biesalski, H.K. Nutrient Intake of 12–59-Months-Old Children and Women in Ethiopia, and Development of Calculator for Inadequate Micronutrient Intake (CIMI) App for Ethiopian Population. Curr. Dev. Nutr. 2019, 3. [Google Scholar] [CrossRef]
- Desalegn, B.B.; Lambert, C.; Riedel, S.; Negese, T.; Biesalski, H.K. Ethiopian Orthodox Fasting and Lactating Mothers: Longitudinal Study on Dietary Pattern and Nutritional Status in Rural Tigray, Ethiopia. Int. J. Environ. Res. Public Health 2018, 15, 1767. [Google Scholar] [CrossRef]
- Ethiopian Public Health Institute [EPHI]. Ethiopia National Food Consumption Survey. 2013. Available online: https://www.ephi.gov.et/images/pictures/National%20Food%20Consumption%20Survey%20 (accessed on 10 December 2018).
- Erhard, J. NutriSurvey for Windows. 2007. Available online: https://www.nutrisurvey.de (accessed on 2 January 2017).
- World Health Organization (WHO); Food and Agriculture Organization (FAO). Vitamin and Mineral Requirements in Human Nutrition, 2nd ed.; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- WHO. Protein and Amino Acid Requirements in Human Nutrition; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- FAO; WHO; UNU. Human Energy Requirements. 2004. Available online: https://www.who.int/nutrition/publications/nutrientrequirements/9251052123/en/ (accessed on 2 January 2017).
- CSA. Population Projection of Ethiopia for All Regions at Wereda Level from 2014–2017; Federal Democratic Republic of Ethiopia Central Statistical Agency: Addis Ababa, Ethiopia. Available online: www.csa.gov.et (accessed on 5 December 2018).
- Quinlan, R.J.; Quinlan, M.B.; Dira, S.; Caudell, M.; Sooge, A.; Assoma, A.A. Vulnerability and Resilience of Sidama Enset and Maize Farms in Southwestern Ethiopia. J. Ethnobiol. 2015, 35, 314–336. [Google Scholar] [CrossRef]
- Zewdie, E.; Sivakumar, S. Determinants of Off Farm Participation of Rural Farm Households in Shebedino District of Sidama. Int. J. Dev. Res. 2017, 7, 15157–15165. [Google Scholar]
- Bosha, T.; Lambert, C.; Riedel, S.; Melesse, A.; Biesalski, H.K. Dietary Diversity and Anthropometric Status of Mother–Child Pairs from Enset (False Banana) Staple Areas: A Panel Evidence from Southern Ethiopia. Int. J. Environ. Res. Public Health 2019, 16, 2170. [Google Scholar] [CrossRef]
- Hulley, S.B.; Cummings, S.R.; Browner, W.S.; Grady, D.G.; Newman, T.B. Designing Clinical Research. In A Wolters Kluwer Business, 4th ed.; Williams, L., Wilkins, Eds.; Two Commerce Square 2001 Market Street: Philadelphia, PA, USA, 2013; p. 79. [Google Scholar]
- Liabsuetrakul, T.; Kuning, M.; Sukchan, P.; Chongsuvivatwong, V.; Sornsrivichai, V.; Songwathana, P. Inadequacy of nutrients intake among pregnant women in the Deep South of Thailand. BMC Public Health 2010, 10, 1. [Google Scholar] [CrossRef]
- Serra-Majem, L.; Ribas, L.; Garcia, A.; Perez-Rodrigo, C.; Aranceta, J. Nutrient adequacy and Mediterranean Diet in Spanish school children and adolescents. Eur. J. Clin. Nutr. 2003, 57, S35–S39. [Google Scholar] [CrossRef]
- Hirvonen, K.; Taffesse, A.S.; Hassen, I.W. Seasonality and household diets in Ethiopia. Public Health Nutr. 2016, 19, 1723–1730. [Google Scholar] [CrossRef] [PubMed]
- Sibhatu, K.T.; Qaim, M. Rural food security, subsistence agriculture, and seasonality. PLoS ONE 2017, 12, e0186406. [Google Scholar] [CrossRef]
- Gebreegziabher, T.; Stoecker, B.J. Vitamin D insufficiency in a sunshine-sufficient area: Southern Ethiopia. Food Nutr. Bull. 2013, 34, 429–433. [Google Scholar] [CrossRef] [PubMed]
- Wakayo, T.; Belachew, T.; Vatanparast, H.; Whiting, S.J. Vitamin D Deficiency and Its Predictorsina Country with Thirteen Months of Sunshine: The Case of School Children in Central Ethiopia. PLoS ONE 2015, 10, e0120963. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, F.; Yabuta, Y.; Bito, T.; Teng, F. Vitamin B12-containing plant food sources for vegetarians. Nutrients 2014, 6, 1861–1873. [Google Scholar] [CrossRef] [PubMed]
- Green, R. Vitamin B12 deficiency from the perspective of a practicing hematologist. Am. Soc. Hematol. 2019, 129, 2603–2611. [Google Scholar] [CrossRef]
- Umeta, M.; West, C.E.; Fufa, H. Content of zinc, iron, calcium and their absorption inhibitors in foods commonly consumed in Ethiopia. J. Food Compost. Anal. 2005, 18, 803–817. [Google Scholar] [CrossRef]
- Hofmeyr, G.J.; Betrán, A.P.; Singata-madliki, M.; Cormick, G.; Munjanja, S.P.; Fawcus, S.; Mose, S.; Hall, D.; Ciganda, A.; Seuc, A.H. Prepregnancy and early pregnancy calcium supplementation among women at high risk of pre-eclampsia: A multicentre, double-blind, randomised, placebo-controlled trial. Lancet 2019, 393, 330–339. [Google Scholar] [CrossRef]
- Balk, E.M.; Adam, G.P.; Langberg, V.N.; Earley, A.; Clark, P.; Ebeling, P.R. Global dietary calcium intake among adults: A systematic review. Osteoporos. Int. 2017, 28, 3315–3324. [Google Scholar] [CrossRef]
- Chotboon, C.; Soontrapa, S.; Buppasiri, P.; Muktabhant, B.; Kongwattanakul, K.; Thinkhamrop, J. Adequacy of calcium intake during pregnancy in a tertiary care center. Int. J. Women’s Health 2018, 10, 523–527. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Category | Number | Percent |
|---|---|---|---|
| Age of mothers, years | 18–24 | 52 | 9.0 |
| 25–34 | 512 | 88.7 | |
| ≥35 | 13 | 2.3 | |
| Lactating, postharvest dry season | Yes | 433 | 75.0 |
| No | 144 | 25.0 | |
| Lactating, lean wet season | Yes | 338 | 58.6 |
| No | 239 | 41.4 | |
| Marital status | Co-habiting in marriage | 563 | 97.6 |
| Other | 14 | 2.4 | |
| Ethnicity | Sidama | 560 | 97.1 |
| Others | 17 | 2.9 | |
| Religion | Protestants | 528 | 91.5 |
| Others | 49 | 8.5 | |
| Educational level | Illiterate | 239 | 41.4 |
| Some education | 338 | 58.6 | |
| Occupation | Housewives | 506 | 87.7 |
| Others | 71 | 12.3 | |
| Family size | 3–5 members | 349 | 60.5 |
| ≥6 members | 228 | 39.5 |
| Nutrient | Devi-ces | Postharvest Dry Season | Lean Wet Season | ||||
|---|---|---|---|---|---|---|---|
| Mean (SD) | Median (25th, 75th Perc.) | N (%) of <2/3 RNI | Mean (SD) | Median (25th, 75th Perc.) | N (%) of <2/3 RNI | ||
| Iron (mg) | CIMI-E | 30.1 (14.3) | 27.1 (20.2, 36.6) | 218 (37.8) | 26.9 (11.4) | 25.7 (19.8, 31.1) | 291 (50.4) |
| NS | 32.9 (15.1) | 29.5 (22.4, 39.7) | 185 (32.1) | 29.9 (11.6) | 28.7 (21.9, 35.2) | 252 (43.7) | |
| Zinc (mg) | CIMI-E | 7.1 (4.6) | 6.2 (3.6, 9.6) | 446 (77.3) | 5.8 (3.8) | 5.1 (3.0, 8.2) | 465 (80.6) |
| NS | 6.5 (4.3) | 5.6 (3.5, 8.4) | 473 (82.0) | 5.3 (3.4) | 4.8 (2.8, 6.9) | 480 (83.2) | |
| Calcium (mg) | CIMI-E | 464 (249) | 432 (282, 606) | 556 (96.4) | 502 (233) | 477 (342, 645) | 560 (97.1) |
| NS | 547 (333) | 481 (298, 733) | 521 (90.3) | 652 (340) | 625 (400, 840) | 489 (84.7) | |
| Magnesium (mg) | CIMI-E | 371 (216) | 330 (215, 483) | 132 (22.9) | 329 (179) | 293 (199, 438) | 163 (28.2) |
| NS | 397 (227) | 353 (232, 510) | 115 (19.9) | 340 (179) | 314 (203, 451) | 146 (25.3) | |
| Niacin (mg) | CIMI-E | 10.3 (4.7) | 9.8 (6.9, 12.8) | 338 (58.6) | 10.1 (4.6) | 9.5 (6.6, 13.0) | 337 (58.4) |
| NS | 12.4 (5.1) | 11.9 (8.8,15.3) | 236 (40.9) | 12.1 (4.7) | 11.3 (8.5, 15.1) | 248 (43.0) | |
| Vitamin A (μg) | CIMI-E | 789 (772) | 608 (141, 1361) | 274 (47.5) | 1092 (842) | 930 (363, 1574) | 160 (27.7) |
| NS | 1108 (1136) | 680 (218, 1951) | 255 (44.2) | 1509 (1143) | 1338 (513, 2174) | 137 (23.7) | |
| PA (mg) | CIMI-E | 2.4 (1.5) | 2.2 (1.3, 3.3) | 505 (87.5) | 2.0 (1.3) | 1.9 (1.1, 2.8) | 527 (91.3) |
| NS | 2.5 (1.7) | 2.1 (1.3, 3.3) | 494 (85.6) | 2.0 (1.3) | 1.8 (1.1, 2.6) | 531 (92.0) | |
| Vitamin B12 (μg) | CIMI-E | 0.019 (0.158) | 0.000 (0.000, 0.000) | 575 (99.7) | 0.001 (0.012) | 0.000 (0.000, 0.000) | 577 (100) |
| NS | 0.021 (0.194) | 0.000 (0.000, 0.000) | 574 (99.5) | 0.001 (0.012) | 0.000 (0.000, 0.000) | 577 (100) | |
| Vitamin B1 (mg) | CIMI-E | 1.0 (0.5) | 0.9 (0.6, 1.3) | 270 (46.8) | 0.9 (0.5) | 0.8 (0.5, 1.2) | 297 (51.5) |
| NS | 1.0 (0.5) | 0.9 (0.7, 1.3) | 249 (43.2) | 0.9 (0.4) | 0.9 (0.6, 1.2) | 274 (47.5) | |
| Vitamin B6 (mg) | CIMI-E | 1.2 (0.7) | 1.1 (0.7, 1.6) | 310 (53.7) | 1.1 (0.6) | 1.0 (0.7, 1.5) | 325 (56.3) |
| NS | 1.4 (0.9) | 1.2 (0.8, 1.8) | 277 (48.0) | 1.3 (0.7) | 1.2 (0.8, 1.7) | 271 (47.0) | |
| Vitamin D (μg) | CIMI-E | 0.015 (0.011) | 0.014 (0.006, 0.020) | 577 (100) | 0.015 (0.014) | 0.014 (0.000, 0.023) | 577 (100) |
| NS | 0.003 (0.013) | 0.000 (0.000, 0.000) | 577 (100) | 0.002 (0.012) | 0.000 (0.000, 0.000) | 577 (100) | |
| Protein (g) | CIMI-E | 35.9 (20.6) | 33.1 (19.7, 46.6) | 299 (51.8) | 31.1 (18.2) | 28.0 (16.8, 42.7) | 339 (58.8) |
| NS | 36.8 (20.0) | 33.7 (21.9, 47.0) | 290 (50.3) | 32.7 (17.8) | 30.0 (19.2, 43.3) | 312 (54.1) | |
| Energy (kcal) | CIMI-E | 1531 (588) | 1454 (1100, 1881) | 380 (65.9) | 1405 (507) | 1335 (1068, 1706) | 402 (69.7) |
| NS | 1596 (587) | 1530 (1148, 1946) | 354 (61.4) | 1495 (508) | 1422 (1149, 1819) | 370 (64.1) | |
| Nutrient | Mean Difference | SD | % Difference * | r |
|---|---|---|---|---|
| Iron (mg) | −2.87 | 4.90 | 9.23 b | 0.93 ** |
| Zinc (mg) | 0.56 | 1.36 | 9.45 b | 0.95 ** |
| Calcium (mg) | −116.53 | 161.87 | 19.43 c | 0.90 ** |
| Magnesium (mg) | −18.75 | 57.77 | 5.09 b | 0.96 ** |
| Niacin (mg) | −2.05 | 1.43 | 16.75 c | 0.96 ** |
| Vitamin A (μg) | −367.65 | 526.25 | 28.10 c | 0.91 ** |
| Pantothenic acid (mg) | −0.005 | 0.58 | 0.22 a | 0.92 ** |
| Vitamin B12 (μg) | −0.001 | 0.048 | 10.00 b | 0.95 ** |
| Vitamin B1 (mg) | −0.02 | 0.15 | 2.06 a | 0.95 ** |
| Vitamin B6 (mg) | 0.17 | 0.27 | 12.59 b | 0.95 ** |
| Vitamin D (μg) | 0.012 | 0.015 | NA | 0.21 ** |
| Protein (g) | −1.26 | 5.05 | 3.62 a | 0.97 ** |
| Energy (kcal) | −77.23 | 147.97 | 5.00 b | 0.96 ** |
| Nutrient | Postharvest Dry Season | Lean Wet Season | p-Value | ||
|---|---|---|---|---|---|
| Mean (SD) | Median (25th, 75th perc.) | Mean (SD) | Median (25th, 75th perc.) | ||
| Iron (mg) | 32.9 (15.1) | 29.5 (22.4, 39.7) | 29.9 (11.6) | 28.7 (21.9, 35.2) | <0.001 |
| Zinc (mg) | 6.5 (4.3) | 5.6 (3.5, 8.4) | 5.3 (3.4) | 4.8 (2.8, 6.9) | <0.001 |
| Calcium (mg) | 547 (333) | 481 (298, 733) | 652 (340) | 625 (400, 840) | <0.001 |
| Magnesium (mg) | 397 (227) | 353 (232, 510) | 340 (179) | 314 (203, 451) | <0.001 |
| Niacin (mg) | 12.4 (5.1) | 11.9 (8.8,15.3) | 12.1 (4.7) | 11.3 (8.5, 15.1) | 0.394 |
| Vitamin A (μg) | 1108 (1136) | 680 (218, 1951) | 1509 (1143) | 1338 (513, 2174) | <0.001 |
| Pantothenic acid (mg) | 2.5 (1.7) | 2.1 (1.3, 3.3) | 2.0 (1.3) | 1.8 (1.1, 2.6) | <0.001 |
| Vitamin B12 (μg) | 0.021 (0.194) | 0.000 (0.000, 0.000) | 0.001 (0.012) | 0.000 (0.000, 0.000) | 0.007 |
| Vitamin B1 (mg) | 1.0 (0.5) | 0.9 (0.7, 1.3) | 0.9 (0.4) | 0.9 (0.6, 1.2) | 0.001 |
| Vitamin B6 (mg) | 1.4 (0.9) | 1.2 (0.8, 1.8) | 1.3 (0.7) | 1.2 (0.8, 1.7) | 0.076 |
| Vitamin D (μg) | 0.003 (0.013) | 0.000 (0.000, 0.000) | 0.002 (0.012) | 0.000 (0.000, 0.000) | 0.009 |
| Protein (g) | 36.8 (20.0) | 33.7 (21.9, 47.0) | 32.7 (17.8) | 30.0 (19.2, 43.3) | <0.001 |
| Energy (kcal) | 1596 (587) | 1530 (1148, 1946) | 1495 (508) | 1422 (1149, 1819) | 0.020 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bosha, T.; Lambert, C.; Riedel, S.; Gola, U.; Melesse, A.; Biesalski, H.K. Validation of the CIMI-Ethiopia Program and Seasonal Variation in Maternal Nutrient Intake in Enset (False Banana) Growing Areas of Southern Ethiopia. Int. J. Environ. Res. Public Health 2019, 16, 2852. https://doi.org/10.3390/ijerph16162852
Bosha T, Lambert C, Riedel S, Gola U, Melesse A, Biesalski HK. Validation of the CIMI-Ethiopia Program and Seasonal Variation in Maternal Nutrient Intake in Enset (False Banana) Growing Areas of Southern Ethiopia. International Journal of Environmental Research and Public Health. 2019; 16(16):2852. https://doi.org/10.3390/ijerph16162852
Chicago/Turabian StyleBosha, Tafese, Christine Lambert, Simon Riedel, Ute Gola, Aberra Melesse, and Hans K. Biesalski. 2019. "Validation of the CIMI-Ethiopia Program and Seasonal Variation in Maternal Nutrient Intake in Enset (False Banana) Growing Areas of Southern Ethiopia" International Journal of Environmental Research and Public Health 16, no. 16: 2852. https://doi.org/10.3390/ijerph16162852
APA StyleBosha, T., Lambert, C., Riedel, S., Gola, U., Melesse, A., & Biesalski, H. K. (2019). Validation of the CIMI-Ethiopia Program and Seasonal Variation in Maternal Nutrient Intake in Enset (False Banana) Growing Areas of Southern Ethiopia. International Journal of Environmental Research and Public Health, 16(16), 2852. https://doi.org/10.3390/ijerph16162852