Influence of Smoking Status on Risk of Incident Heart Failure: A Systematic Review and Meta-Analysis of Prospective Cohort Studies


Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategies
2.2. Study Selection
2.3. Data Extraction
2.4. Quality Assessment
2.5. Statistical Methodology
3. Results
3.1. Literature Search
3.2. Description of Included Studies
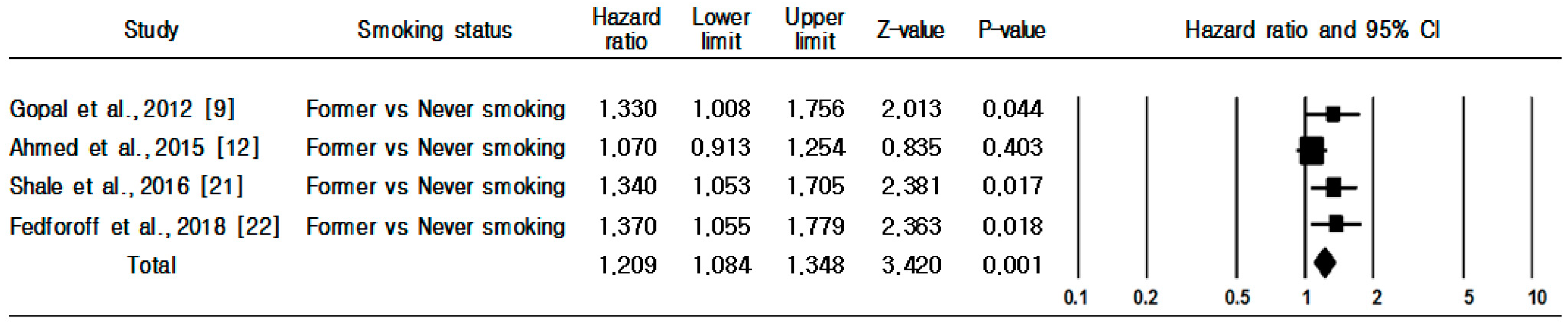
3.3. Smoking Status and Incident Risk of HF
3.4. Subgroup and Sensitivity Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Conrad, N.; Judge, A.; Tran, J.; Mohseni, H.; Hedgecott, D.; Crespillo, A.P.; Allison, M.; Hemingway, H.; Cleland, J.G.; McMurray, J.J.V.; et al. Temporal trends and patterns in heart failure incidence: A population-based study of 4 million individuals. Lancet 2018, 391, 572–580. [Google Scholar] [CrossRef]
- Savarese, G.; Lund, L.H. Global public health burden of heart failure. Card. Fail. Rev. 2017, 3, 7–11. [Google Scholar] [CrossRef]
- Avery, C.L.; Loehr, L.R.; Baggett, C.; Chang, P.P.; Kucharska-Newton, A.M.; Matsushita, K.; Rosamond, W.D.; Heiss, G. The population burden of heart failure attributable to modifiable risk factors. J. Am. Coll. Cardiol. 2012, 60, 1640–1646. [Google Scholar] [CrossRef] [PubMed]
- Dunlay, S.M.; Weston, S.A.; Jacobsen, S.J.; Roger, V.L. Risk factors for heart failure: A population-based case-control study. Am. J. Med. 2009, 122, 1023–1028. [Google Scholar] [CrossRef] [PubMed]
- Khatibzadeh, S.; Farzadfar, F.; Oliver, J.; Ezzati, M.; Moran, A. Worldwide risk factors for heart failure: A systematic review and pooled analysis. Int. J. Cardiol. 2013, 168, 1186–1194. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Negishi, K.; Otahal, P.; Marwick, T.H. Clinical prediction of incident heart failure risk: A systematic review and meta-analysis. Open Heart 2015, 2, e000222. [Google Scholar] [CrossRef] [PubMed]
- Fleg, J.L. Healthy lifestyle and risk of heart failure: An ounce of prevention well worth the effort. Circ. Heart Fail. 2016, 9, e003155. [Google Scholar] [CrossRef] [PubMed]
- Kamimura, D.; Cain, L.R.; Mentz, R.J.; White, W.B.; Blaha, M.J.; DeFilippis, A.P.; Fox, E.R.; Rodriguez, C.J.; Keith, R.J.; Benjamin, E.J.; et al. Cigarette smoking and incident heart failure: Insights from the Jackson Heart Study. Circulation 2018, 137, 2572–2582. [Google Scholar] [CrossRef] [PubMed]
- Gopal, D.M.; Kalogeropoulos, A.P.; Georgiopoulou, V.; Smith, A.L.; Bauer, D.C.; Newman, A.B.; Kim, L.; Bibbins-Domingo, K.; Tindle, H.; Harris, T.B.; et al. Cigarette smoking exposure and heart failure risk in older adults: The health, aging, and body composition study. Am. Heart J. 2012, 164, 236–242. [Google Scholar] [CrossRef]
- Mons, U.; Muezzinler, A.; Gellert, C.; Schottker, B.; Abnet, C.C.; Bobak, M.; De Groot, L.; Freedman, N.D.; Jansen, E.; Kee, F.; et al. Impact of smoking and smoking cessation on cardiovascular events and mortality among older adults: Meta-analysis of individual participant data from prospective cohort studies of the CHANCES consortium. BMJ 2015, 350, h1551. [Google Scholar] [CrossRef]
- Thun, M.J.; Carter, B.D.; Feskanich, D.; Freedman, N.D.; Prentice, R.; Lopez, A.D.; Hartge, P.; Gapstur, S.M. 50-year trends in smoking-related mortality in the United States. N. Engl. Med. 2013, 368, 351–364. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.A.; Patel, K.; Nyaku, M.A.; Kheirbek, R.E.; Bittner, V.; Fonarow, G.C.; Filippatos, G.S.; Morgan, C.J.; Aban, I.B.; Mujib, M.; et al. Risk of heart failure and death after prolonged smoking cessation: Role of amount and duration of prior smoking. Circ. Heart Fail. 2015, 8, 694–701. [Google Scholar] [CrossRef] [PubMed]
- Conard, M.W.; Haddock, K.; Poston, W.S.C.; Spertus, J.A. The impact of smoking status on the health status of heart failure patients. Congest. Heart Fail. 2009, 15, 82–86. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Schlesinger, S.; Norat, T.; Riboli, E. Tobacco smoking and the risk of heart failure: A systematic review and meta-analysis of prospective studies. Eur. J. Prev. Cardiol. 2019, 26, 279–288. [Google Scholar] [CrossRef] [PubMed]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting, Meta-analysis of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 25 April 2016).
- Higgins, J.P.; Green, S. Cochrane Collaboration. Cochrane Handbook for Systematic Reviews of Interventions; Wiley-Blackwell: Hoboken, NJ, USA, 2008; p. 418. [Google Scholar]
- He, J.; Ogden, L.G.; Bazzano, L.A.; Vupputuri, S.; Loria, C.; Whelton, P.K. Risk factors for congestive heart failure in US men and women. Arch. Intern. Med. 2001, 161, 996–1002. [Google Scholar] [CrossRef] [PubMed]
- Ingelsson, E.; Arnlov, J.; Lind, L.; Sundstrom, J. Metabolic syndrome and risk fro heart failure in middle aged mend. Heart 2006, 92, 1409–1413. [Google Scholar] [CrossRef] [PubMed]
- Nadruz, W.; Goncalves, A.; Claggett, B.; Roca, G.Q.; Shah, A.M.; Cheng, S.; Heiss, G.; Ballantyne, C.M.; Solomon, S.D. Influence of cigarette smoking on cardiac biomarkers: The Atherosclerosis Risk in Communities (ARIC) Study. Eur. J. Heart Fail. 2016, 8, 629–637. [Google Scholar] [CrossRef] [PubMed]
- Sahle, B.W.; Owen, A.J.; Krum, H.; Reid, C.M. Incidence of heart failure in 6083 elderly hypertensive patients: The Second Australian National Blood Pressure Study (ANBP2). Eur. J. Heart Fail. 2016, 18, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Feodoroff, M.; Harjutsalo, V.; Forsblom, C.; Groop, P.H. Dose-dependent effect of smoking on risk of coronary heart disease, heart failure and stroke in individuals with type 1 diabetes. Dibetologia 2018, 61, 2580–2589. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Sutton, A.J.; Duval, S.J.; Tweedie, R.L.; Abrams, K.R.; Jones, D.R. Empirical assessment of effect of publication bias on meta-analyses. BMJ 2000, 320, 1574–1577. [Google Scholar] [CrossRef] [PubMed]
- Messner, B.; Bernhard, D. Smoking and cardiovascular disease: Mechanisms of endothelial dysfunction and early atherogenesis. Arter. Thromb. Vasc. Biol. 2014, 34, 509–515. [Google Scholar] [CrossRef] [PubMed]
- Barua, R.S.; Ambrose, J.A.; Eales-Reynolds, L.J.; DeVoe, M.C.; Zervas, J.G.; Saha, D.C. Dysfunctional endothelial nitric oxide biosynthesis in healthy smokers with impaired endothelium-dependent vasodilatation. Circulation 2001, 104, 1905–1910. [Google Scholar] [CrossRef] [PubMed]
- Cross, C.E.; Halliwell, B.; Borish, E.T.; Pryor, W.A.; Ames, B.N.; Saul, R.L.; McCord, J.M.; Harman, D. Oxygen radicals and human disease. Ann. Intern. Med. 1987, 107, 526–545. [Google Scholar] [CrossRef] [PubMed]
- FitzGerald, G.A.; Oates, J.A.; Nowak, J. Cigarette smoking and hemostatic function. Am. Heart J. 1988, 115, 267–271. [Google Scholar] [CrossRef]
- Mendall, M.A.; Patel, P.; Asante, M.; Ballam, L.; Morris, J.; Strachan, D.P.; Camm, A.J.; Northfield, T.C. Relation of serum cytokine concentrations to cardiovascular risk factors and coronary heart disease. Heart 1997, 78, 273–277. [Google Scholar] [CrossRef] [PubMed]
- Dochi, M.; Sakata, K.; Oishi, M.; Tanaka, K.; Kobayashi, E.; Suwazono, Y. Smoking as an independent risk factor for hypertension: A 14-year longitudinal study in male Japanese workers. Tohoku J. Exp. Med. 2009, 217, 37–43. [Google Scholar] [CrossRef]
- Zhu, W.; Yuan, P.; Shen, Y.; Wan, R.; Hong, K. Association of smoking with the risk of incident atrial fibrillation: A meta-analysis of prospective studies. Int. J. Cardiol. 2016, 218, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Linneberg, A.; Jacobsen, R.K.; Skaaby, T.; Taylor, A.E.; Fluharty, M.E.; Jeppesen, J.L.; Bjorngaard, J.H.; Åsvold, B.O.; Gabrielsen, M.E.; Campbell, A.; et al. Effect of smoking on blood pressure and resting heart rate: A Mendelian randomization meta-analysis in the CARTA Consortium. Circ. Cardiovasc. Genet. 2015, 8, 832–841. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Sen, A.; O’Hartaigh, B.; Janszky, I.; Romundstad, P.R.; Tonstad, S.; Vatten, L.J. Resting heart rate and the risk of cardiovascular disease, total cancer, and all-cause mortality—A systematic review and dose- response meta-analysis of prospective studies. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 504–517. [Google Scholar] [CrossRef] [PubMed]
- Critchley, J.A.; Capewell, S. Mortality risk reduction associated with smoking cessation in patients with coronary heart disease: A systematic review. JAMA 2003, 290, 86–89. [Google Scholar] [CrossRef] [PubMed]
- Mannan, H.R.; Stevenson, C.E.; Peeters, A.; Walls, H.L.; McNeil, J.J. Age at quitting smoking as a predictor of risk of cardiovascular disease incidence independent of smoking status, time since quitting and pack-years. BMC Res. Notes. 2011, 4, 39. [Google Scholar] [CrossRef]
- Jordan, H.; Hidajat, M.; Payne, N.; Adams, J.; White, M.; Ben-Shlomo, Y. What are older smokers’ attitudes to quitting and how are they managed in primary care? An analysis of the cross- sectional English Smoking Toolkit Study. BMJ Open 2017, 7, 018150. [Google Scholar] [CrossRef] [PubMed]
- Shahoumian, T.A.; Phillips, B.R.; Backus, L.I. Cigarette smoking, reduction and quit attempts: Prevalence among Veterans with coronary heart disease. Prev. Chronic Dis. 2016, 13, 150282. [Google Scholar] [CrossRef]
- Ferrari, A.U.; Radaelli, A.; Centola, M. Invited review: Aging and the cardiovascular system. J. Appl. Physiol. 2003, 95, 2591–2597. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Authors, (Publication Year)/Location | Age (yrs) at Baseline | Cases/Cohort Size | Follow-up Period (yrs) | Exposure Assessment | Smoking Status Identified | Outcome Assessment | Adjustments for Covariates | Quality Assessment Score |
|---|---|---|---|---|---|---|---|---|
| He et al. (2001)/USA [18] | 25–74 | 1382/13,643 | 19 (average) | Interview | Non-smokers/current smokers | Medical records | Age, race, education, alcohol consumption, physical activity, HTN, SBP, DM, BMI, serum cholesterol, VHD, CAD | 9 |
| Ingelsson et al. (2006)/Sweden [19] | 50 | 100/2314 | 20.1 (median) | Interview | Non-smokers/current smokers | Medical records | HTN, DM, BMI, LVH, MI | 8 |
| Gopal et al. (2012)/USA [9] | 70–79 | 231/2125 | 9.4 (median) | Self-reported | Never/former/current smokers | Medical records | Age, SBP, HR, CAD, LVH, albumin, fasting glucose, creatinine | 8 |
| Ahmed et al. (2015)/USA [12] | ≥65 | 931/4482 | 13 | Self-reported | Never/former/current smokers | Medical records | Age, sex, race, education, income, alcohol consumption, ADL, HTN, DM, BMI, CAD, LVH, stroke, AF, PAD, COPD, cancer, left ventricular systolic dysfunction, CRP, ACEIs, serum creatinine, beta-blockers, diuretics | 8 |
| Nadruz et al. (2016)/USA [20] | 45–64 | 1496/9649 | 15 | Interview | Never/passive/former/current smokers | Medical records | Age, sex, race, alcohol consumption, HTN, SBP, HR, DM, BMI, SBP, HR, COPD, estimated GFR | 9 |
| Sahle et al. (2016)/Australia [21] | 84 ± 5 | 373/6083 | 10.8 (median) | Medical records | Never/former/current smokers | Medical records | BP, BMI, CVD, estimated GFR | 7 |
| Feoforoff et al. (2018)/Finland [22] | 27.4–51.3 | 313/4463 | 13.8 (median) | Self-reported | Never/former/current smokers | Medical records | Age, sex, HTN, DM, BMI, HDL-cholesterol, TG, HbA1c | 9 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.; Son, Y.-J. Influence of Smoking Status on Risk of Incident Heart Failure: A Systematic Review and Meta-Analysis of Prospective Cohort Studies. Int. J. Environ. Res. Public Health 2019, 16, 2697. https://doi.org/10.3390/ijerph16152697
Lee H, Son Y-J. Influence of Smoking Status on Risk of Incident Heart Failure: A Systematic Review and Meta-Analysis of Prospective Cohort Studies. International Journal of Environmental Research and Public Health. 2019; 16(15):2697. https://doi.org/10.3390/ijerph16152697
Chicago/Turabian StyleLee, Hyeonju, and Youn-Jung Son. 2019. "Influence of Smoking Status on Risk of Incident Heart Failure: A Systematic Review and Meta-Analysis of Prospective Cohort Studies" International Journal of Environmental Research and Public Health 16, no. 15: 2697. https://doi.org/10.3390/ijerph16152697
APA StyleLee, H., & Son, Y.-J. (2019). Influence of Smoking Status on Risk of Incident Heart Failure: A Systematic Review and Meta-Analysis of Prospective Cohort Studies. International Journal of Environmental Research and Public Health, 16(15), 2697. https://doi.org/10.3390/ijerph16152697