Validation of a Short-Form Version of the Danish Need for Recovery Scale against the Full Scale

 , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Outcomes and Data Collection
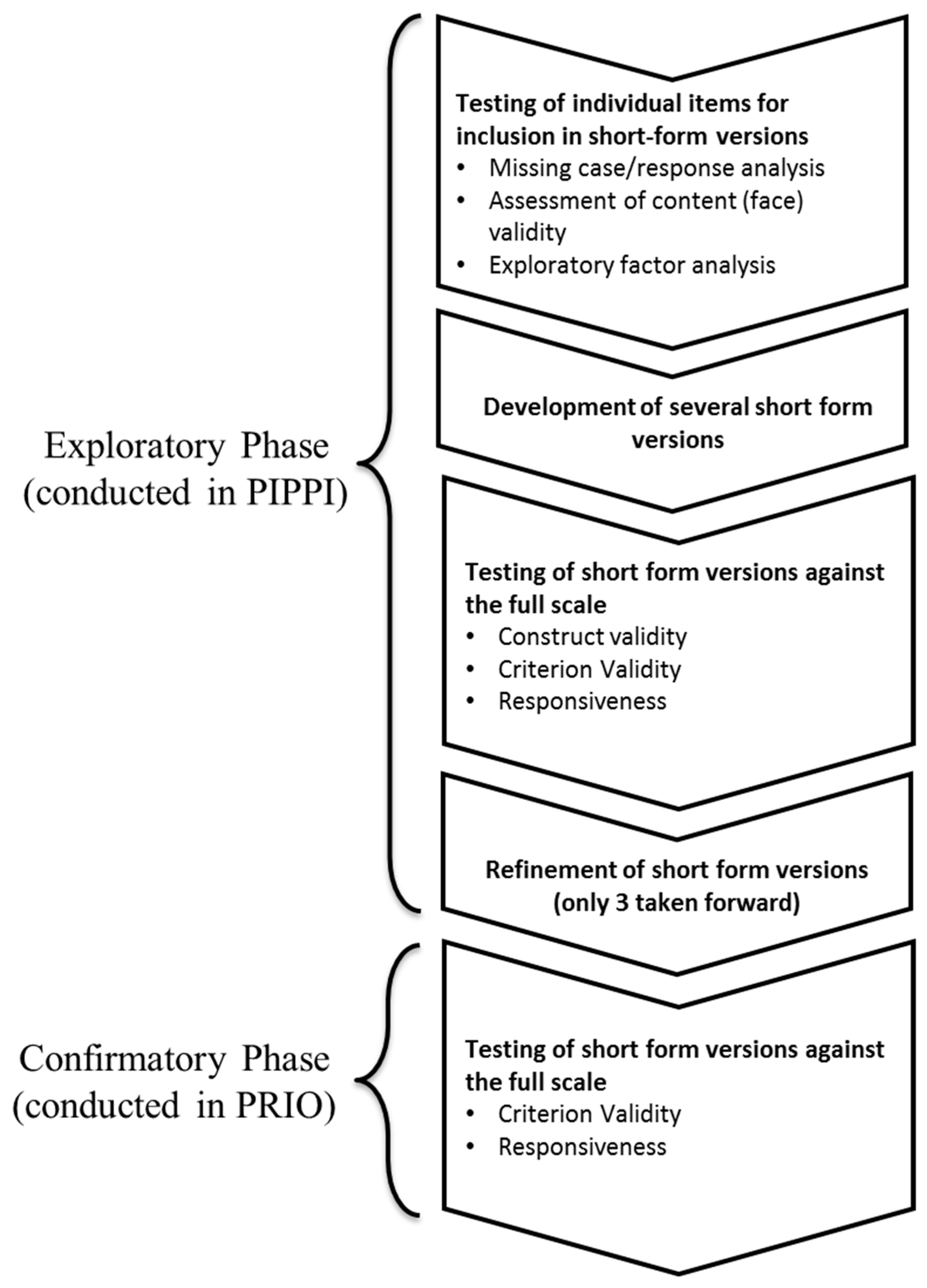
2.3. Validation Process and Statistical Analyses
2.4. Exploratory Phase
2.5. Confirmatory Phase
3. Results
3.1. Exploratory Analyses
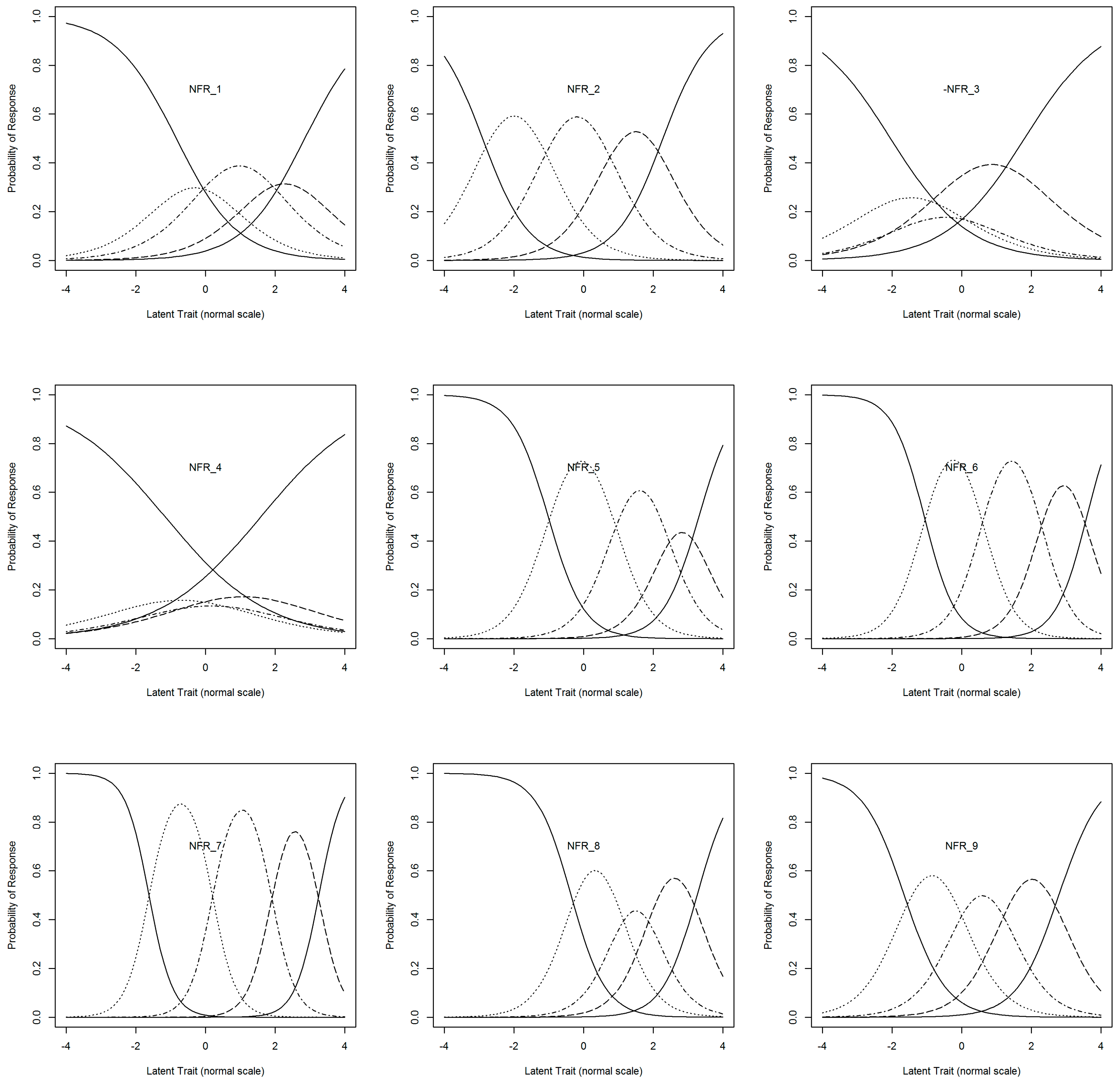
3.1.1. Content Validity and Item-Accessibility
- Factor 1: Recovery of mental resources—items 1, 4, 5, 6, and 8. These items refer to constructs, such as ‘trouble relaxing’, ‘trouble concentrating’, ‘hard to show interest in others’, and ‘a need for being left alone after work’. These phrases can predominantly be linked to increased mental stress and fatigue, apathy, and irritability; all being symptoms of drained mental resources.
- Factor 2: Recovery of physical resources—items 2 and 9. These items use words, such as ‘exhausted’ or indicate ‘tiredness’ too great to initiate other activities. Both of these items could be interpreted as referring to the depletion of physical resources.
3.1.2. Factor Analysis
3.1.3. Development of the Short-Form Versions
3.1.4. Construct Validity
3.1.5. Criterion Validity and Responsiveness
3.2. Confirmatory Analyses
4. Discussion
4.1. Summary of Findings
4.2. Strengths and Limitations of the Study
4.3. Comparisons with Other Studies
4.4. Meaning and Implications of the Study
4.5. Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- OECD. Live Longer, Work Longer, Ageing and Employment Policies; OECD Publishing: Paris, France, 2006. [Google Scholar]
- De Vet, H.C.W.; Terwee, C.B.; Mokkink, L.B.; Knol, D.L. Measurement in Medicine; Cambridge University Press: Cambridge, UK, 2011. [Google Scholar]
- Velentgas, P.; Dreyer, N.; Wu, A. Outcome Definition and Measurement. In Developing a Protocol for Observational Comparative Effectiveness Research A User’s Guide; Velentgas, P., Dreyer, N., Nourjah, P., Smith, S., Torchia, M., Eds.; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2013; pp. 71–92. [Google Scholar]
- Galesic, M.; Bosnjak, M. Effects of questionnaire length on participation and indicators of response quality in a web survey. Public Opin. Q. 2009, 73, 349–360. [Google Scholar] [CrossRef]
- Sahlqvist, S.; Song, Y.; Bull, F.; Adams, E.; Preston, J.; Ogilvie, D. Effect of questionnaire length, personalisation and reminder type on response rate to a complex postal survey: Randomised controlled trial. BMC Med. Res. Methodol. 2011, 11. [Google Scholar] [CrossRef] [PubMed]
- Jepson, C.; Asch, D.A.; Hershey, J.C.; Ubel, P.A. In a mailed physician survey, questionnaire length had a threshold effect on response rate. J. Clin. Epidemiol. 2005, 58, 103–105. [Google Scholar] [CrossRef] [PubMed]
- Rolstad, S.; Adler, J.; Rydén, A. Response burden and questionnaire length: Is shorter better? A review and meta-analysis. Value Health 2011, 14, 1101–1108. [Google Scholar] [CrossRef] [PubMed]
- De Croon, E.M.; Sluiter, J.K.; Frings-Dresen, M.H.W. Psychometric properties of the Need for Recovery after work scale: Test-retest reliability and sensitivity to detect change. Occup. Environ. Med. 2006, 63, 202–206. [Google Scholar] [CrossRef] [PubMed]
- Van Veldhoven, M.; Meijman, T. Het Meten Van Psychosociale Arbeids-Belasting Met een Vragenlijst: De Vragenlijst Beleving en Beoordeling van de Arbeid (VBBA); Nederlands Instituut voor Arbeidsomstandigheden (NIA): Amsterdam, The Netherlands, 1994; pp. 229–230. [Google Scholar]
- Van Veldhoven, M.; Broersen, S. Measurement quality and validity of the “need for recovery scale”. J. Occup. Env. Med. 2003, 60, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Van Veldhoven, M.J.P.M. Psychosociale Arbeidsbelasting en Werkstress; University of Groningen: Groningen, The Netherlands, 1996. [Google Scholar]
- De Croon, E.M.; Sluiter, J.K.; Frings-Dresen, M.H.W. Need for recovery after work predicts sickness absence: A 2-year prospective cohort study in truck drivers. J. Psychosom. Res. 2003, 55, 331–339. [Google Scholar] [CrossRef]
- Moriguchi, C.S.; Alem, M.E.R.; Veldhoven, M.; van Coury, H.J.C.G. Cultural adaptation and psychometric properties of Brazilian Need for Recovery Scale. Rev. Saude Publica 2010, 44, 131–139. [Google Scholar] [CrossRef]
- Moriguchi, C.S.; Alem, M.E.R.; Coury, H.J.C.G. Evaluation of workload among industrial workers with the Need for Recovery Scale. Rev. Bras. Fisioter. 2011, 15, 154–159. [Google Scholar] [CrossRef]
- Pace, F.; Lo Cascio, V.; Civilleri, A.; Guzzo, G.; Foddai, E.; Van Veldhoven, M. The need for recovery scale: Adaptation to the Italian context. Rev. Eur. Psychol. Appl. 2013, 63, 243–249. [Google Scholar] [CrossRef]
- Lin, Y.C.; Chen, Y.C.; Hsieh, H.I.; Chen, P.C. Risk for work-related fatigue among the employees on semiconductor manufacturing lines. Asia Pac. J. Public Health 2015, 27, 1805–1818. [Google Scholar] [CrossRef] [PubMed]
- Gupta, N.; Wåhlin-Jacobsen, C.D.; Abildgaard, J.S.; Henriksen, L.N.; Nielsen, K.; Holtermann, A. Effectiveness of a participatory physical and psychosocial intervention to balance the demands and resources of industrial workers: A cluster-randomized controlled trial. Scand. J. Work Environ. Health 2018, 44, 58–68. [Google Scholar] [CrossRef] [PubMed]
- Garde, A.H.; Albertsen, K.; Nabe-Nielsen, K.; Carneiro, I.G.; Skotte, J.; Hansen, S.M.; Lund, H.; Hvid, H.; Hansen, Å.M. Implementation of self-rostering (the PRIO project): Effects on working hours, recovery, and health. Scand. J. Work Environ. Health 2012, 38, 314–326. [Google Scholar] [CrossRef] [PubMed]
- Ahlstrom, L.; Grimby-Ekman, A.; Hagberg, M.; Dellve, L. The Work Ability Index and single-item question: Associations with sick leave, symptoms and health—A prospective study of women on long-term sick leave. Scand. J. Work Environ. Health 2010, 36, 404–412. [Google Scholar] [CrossRef] [PubMed]
- Jääskeläinen, A.; Kausto, J.; Seitsamo, J.; Ojajärvi, A.; Nygård, C.H.; Arjas, E.; Leino-Arjas, P. Work ability index and perceived work ability as predictors of disability pension: A prospective study among Finnish municipal employees. Scand. J. Work Environ. Health 2016, 42, 490–499. [Google Scholar] [CrossRef] [PubMed]
- Karstad, K.; Jorgensen, A.F.B.; Greiner, B.A.; Burdorf, A.; Sogaard, K.; Rugulies, R.; Holtermann, A. Danish Observational Study of Eldercare work and musculoskeletal disorders (DOSES): A prospective study at 20 nursing homes in Denmark. BMJ Open 2018, 8. [Google Scholar] [CrossRef] [PubMed]
- Jørgensen, M.B.; Korshøj, M.; Lagersted-Olsen, J.; Villumsen, M.; Mortensen, O.S.; Skotte, J.; Søgaard, K.; Madeleine, P.; Thomsen, B.L.; Holtermann, A. Physical activities at work and risk of musculoskeletal pain and its consequences: Protocol for a study with objective field measures among blue-collar workers. BMC Musculoskelet. Disord. 2013, 14. [Google Scholar] [CrossRef]
- Gupta, N.; Wåhlin-Jacobsen, C.D.; Henriksen, L.N.; Abildgaard, J.S.; Nielsen, K.; Holtermann, A. A participatory physical and psychosocial intervention for balancing the demands and resources among industrial workers (PIPPI): Study protocol of a cluster-randomized controlled trial Environmental and occupational health. BMC Public Health 2015, 15, 1–12. [Google Scholar] [CrossRef]
- Borg, V.; Kristensen, T.S.; Burr, H. Work environment and changes in self-rated health: A five year follow-up study. Stress Med. 2000, 16, 37–47. [Google Scholar] [CrossRef]
- Topp, C.W.; Østergaard, S.D.; Søndergaard, S.; Bech, P. The WHO-5 well-being index: A systematic review of the literature. Psychother. Psychosom. 2015, 84, 167–176. [Google Scholar] [CrossRef]
- Tuomi, K.; Ilmarinen, J.; Jahkola, A.; Katajarinne, L.; Tulkki, A. Work Ability Index, 2nd ed.; Oxford University Press: Oxford, UK, 1998. [Google Scholar]
- Noble, B.J.; Borg, G.A.V.; Jacobs, I.; Ceci, R.; Kaiser, P. A category-ratio perceived exertion scale: Relationship to blood and muscle lactates and heart rate. Med. Sci. Sports Exerc. 1983, 15, 523–528. [Google Scholar] [CrossRef] [PubMed]
- Goetz, C.; Coste, J.; Lemetayer, F.; Rat, A.C.; Montel, S.; Recchia, S.; Debouverie, M.; Pouchot, J.; Spitz, E.; Guillemin, F. Item reduction based on rigorous methodological guidelines is necessary to maintain validity when shortening composite measurement scales. J. Clin. Epidemiol. 2013, 66, 710–718. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. A Language and Environment for Statistical Computing 2018; R Foundation for Statistical Computing: Vienna, Austria, 2018. [Google Scholar]
- Bernaards, C.; Jennrich, R. R Package ‘GPArotation’: GPA Factor Rotation 2015. Available online: https://CRAN.R-project.org/package=GPArotation (accessed on 2 July 2019).
- Wickham, H.; François, R.; Henry, L.; Müller, K. R Package “dplyr”: A Grammar of Data Manipulation 2019. Available online: https://dplyr.tidyverse.org/ (accessed on 2 July 2019).
- Wickham, H.; Chang, W.; Henry, L.; Pedersen, T.L.; Wilke, C.; Woo, K. R Package “ggplot2”: Create Elegant Data Visualisations Using the Grammar of Graphics 2018. Available online: https://ggplot2.tidyverse.org/ (accessed on 2 July 2019).
- Revelle, W. R Package “psych”: Procedures for Psychological, Psychometric, and Personality Research 2019. Available online: https://personality-project.org/r/psych/ (accessed on 2 July 2019).
- Temel, G.; Erdogan, S. Determining the sample size in agreement studies. Marmara Med. J. 2017, 30, 101–112. [Google Scholar] [CrossRef]
- Cohen, J. A Power Primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Ilmarinen, J.; Tuomi, K.; Klockars, M. Changes in the Work Ability Index Over an 11-Year Period. Scand. J. Work Environ. Health 1997, 23, 49–57. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Item Number | Danish 9-Item NFR Scale | English Translation |
|---|---|---|
| Item 1 | Jeg har svært ved at slappe af efter en arbejdsdag | I find it hard to relax after a working day |
| Item 2 | I slutningen af min arbejdsdag er jeg udmattet | At the end of my work day I am exhausted |
| Item 3 | Jeg føler mig frisk efter aftensmad | I feel fresh after dinner |
| Item 4 | Jeg slapper ikke ordentlig af, hvis jeg kun har en dag uden arbejde | I do not normally relax, if I have only had one day without work |
| Item 5 | Jeg har problemer med at koncentrere mig i timerne efter, at jeg er kommet hjem fra arbejde | I have trouble concentrating in the hours after I come home from work |
| Item 6 | Jeg har svært ved at udvise interesse for andre mennesker, lige når jeg er kommet hjem fra arbejde | I find it hard to show interest in other people, when I have just come home from work |
| Item 7 | Det tager mig over en time, før jeg er restitueret /er kommet mig fuldstændigt efter en arbejdsdag | It takes me over an hour before I am fully recovered/fully improved after a work day |
| Item 8 | Når jeg kommer hjem efter arbejde, skal folk lade mig være i et stykke tid | When I get home after work, people have to leave me alone for a while |
| Item 9 | Efter en arbejdsdag er jeg for træt til at begynde andre aktiviteter | After a working day I am too tired to begin other activities |
| Response Categories | Response Categories | |
| 1. Aldrig 2. Sjældent 3. Engang i mellem 4. For det meste 5. Altid | 1. Never 2. Rarely 3. Sometimes 4. Generally 5. Always | |
| English Translation | Scoring Values |
|---|---|
| How many days in the last four weeks has muscle or joint pain inhibited you? (e.g., affected you daily routine or activities) | 0–28 days |
| How physically demanding do you normally perceive your working situation? [27] | 0–10 numerical ratings scale. 0 being not demanding; 10 being maximally demanding |
| How do you rate your overall health? [24] | 5 point likert scale 1 being very poor; 5 being excellent |
| How do you rate your current work ability in relation to the psychological/cognitive demands of your work? [26] | 5 point likert scale 1 being very poor; 5 being excellent |
| How do you rate your current work ability in relation to the physical demands of you work? [26] | 5 point likert scale 1 being very poor; 5 being excellent |
| How do you rate your current work ability? [26] | 0–10 numerical ratings scale. 0 being unable to work; 10 being work ability at it’s best |
| Do you wake up fresh and recovered? [25] | 6 point likert scale 1 being at no time; 6 being all the time |
| Do you feel calm and relaxed? [25] | 6 point likert scale 1 being at no time; 6 being all the time |
| Demographics Information | PIPPI a | PRIO b | ||
|---|---|---|---|---|
| Mean or n | (SD) or (%) | Mean or n | (SD) or (%) | |
| Sex (male) | 242 | 71% | 74 | 9.7% |
| Age (years) | 44 | SD 10 | 43 | SD 11 |
| BMI (kg/m2) | 26.6 | SD 4.4 | 25 | SD 3.9 |
| Smoking | ||||
| Daily | 80 | 23% | N/A | |
| Never | 27 | 8% | 360 | 48% |
| Former | 97 | 28% | 237 | 31% |
| Current | 140 | 41% | 160 | 21% |
| Self-reported health | ||||
| Very good | 29 | 8% | 49 | 6% |
| Good | 122 | 36% | 317 | 42% |
| Fairly good | 166 | 48% | 329 | 44% |
| Poor | 26 | 8% | 60 | 8% |
| Very poor | 1 | 0.3% | 2 | 0.3% |
| NFR index | 51 | SD 8.8 | 55 | SD 12.6 |
| Construct Validity Items | Mean | SD or n (%) |
|---|---|---|
| Overall work ability | 8 | SD 1.4 |
| Work ability in the physical domain | ||
| Very poor | 72 | 21% |
| Poor | 157 | 46% |
| Fairly good | 100 | 29% |
| Good | 15 | 4% |
| Very good | 0 | 0% |
| Work ability in the psychological domain | ||
| Very poor | 56 | 16% |
| Poor | 155 | 45% |
| Fairly good | 47 | 14% |
| Good | 24 | 7% |
| Very good | 1 | 0.3% |
| Feeling recovered on awaking | ||
| At no time | 8 | 2% |
| Rarely | 103 | 30% |
| Some of the time | 153 | 45% |
| Most of the time | 60 | 17% |
| All of the time | 20 | 6% |
| Feeling calm and relaxed | ||
| At no time | 14 | 4% |
| Rarely | 144 | 42% |
| Some of the time | 95 | 28% |
| Often | 59 | 17% |
| Most of the time | 23 | 7 % |
| All of the time | 9 | 3% |
| Physical exertion at work | 6 | SD 2.3 |
| Days of inhibiting pain | ||
| 0–10 | 287 | 85% |
| 11–20 | 27 | 8% |
| >20 | 24 | 7% |
| NFR Item | PIPPI n = 11 | PRIO n = 40 |
|---|---|---|
| Item 1 | 1 | 6 |
| Item 2 | 1 | 2 |
| Item 3 | 2 | 14 |
| Item 4 | 6 | 14 |
| Item 5 | 0 | 5 |
| Item 6 | 1 | 6 |
| Item 7 | 1 | 9 |
| Item 8 | 1 | 3 |
| Item 9 | 0 | 3 |
| Related Construct | Danish Need for Recovery (NFR) Scale | ||||||
|---|---|---|---|---|---|---|---|
| Primary Aim | Secondary Aim | ||||||
| Items 1–9 (Original) | Items 1, 2, 5–9 | Items 2, 6, 7 | Items 2, 6 | Item 7 | Items 1, 2 & 9 | Items 2, 9 | |
| Days of inhibiting pain k | 0.28 (0.20, 0.35) | 0.30 (0.23, 0.37) | 0.31 (0.24, 0.38) | 0.31 (0.24, 0.38) | 0.27 (0.18, 0.35) | 0.32 (0.24, 0.39) | 0.33 (0.24, 0.40) |
| Perceived exertion p | 0.17 (0.06, 0.28) | 0.18 (0.08, 0.29) | 0.21 (0.10, 0.31) | 0.22 (0.11, 0.31) | 0.17 (0.07, 0.27) | 0.26 (0.14, 0.36) | 0.26 (0.15, 0.35) |
| Perceived health p | −0.32 (−0.41, −0.21) | −0.36 (−0.44, −0.26) | −0.32 (−0.41, −0.22) | −0.31 (−0.41, −0.21) | −0.28 (−0.37, −0.19) | −0.35 (−0.44, −0.26) | −0.36 (−0.45, −0.26) |
| Mental work ability k | −0.30 (−0.38, −0.22) | −0.32 (−0.40, −0.24) | −0.28 (− 0.36, −0.20) | −0.29 (−0.37, −0.21) | 0.26 (0.17, 0.34) | −0.31 (−0.39, −0.23) | −0.26 (−0.34, −0.18) |
| Physical work ability k | −0.22 (−0.30, −0.14) | −0.27 (−0.34, −0.19) | −0.25 (−0.33, −0.17) | −0.25 (−0.32, −0.16) | −0.23 (0.14, 0.32) | −0.28 (−0.35, −0.19) | −0.28 (−0.35, −0.19) |
| Overall work ability k | −0.23 (−0.30, −0.15) | −0.27 (−0.34, −0.19) | −0.24 (−0.31, −0.16) | −0.23 (−0.30, −0.15) | −0.23 (0.14, 0.31) | −0.27 (−0.35, −0.19) | −0.27 (−0.34, −0.18) |
| Feeling rested on waking p | −0.48 (−0.56, −0.38) | −0.48 (−0.57, −0.39) | −0.44 (−0.53, −0.34) | −0.39 (−0.49, −0.27) | −0.45 (−0.54, −0.35) | −0.43 (−0.52, −0.34) | −0.40 (−0.50, −0.29) |
| Feeling calm and relaxed k | −0.40 (−0.47, −0.32) | −0.43 (−0.50, −0.36) | −0.40 (−0.47, −0.32) | −0.40 (−0.47, −0.32) | −0.38 (−0.46, −0.29) | −0.40 (−0.47, −0.31) | −0.37 (−0.45, −0.29) |
| Aim being Addressed | NFR Scale Items Used | Criterion Validity ICC (95% CI) (n = 344) | Responsiveness ICC (95% CI) (n = 245) |
|---|---|---|---|
| Primary Aim | Items 1, 2 & 5–9 | 0.92 (0.90, 0.93) | 0.94 (0.92, 0.95) |
| Items 2, 6 & 7 | 0.85 (0.82, 0.88) | 0.79 (0.74, 0.84) | |
| Items 2 & 6 | 0.82 (0.79, 0.85) | 0.74 (0.68, 0.79) | |
| Item 7 | 0.67 (0.60, 0.72) | 0.51 (0.41, 0.60) | |
| Secondary Aim | Items 1, 2 & 9 | 0.83 (0.80, 0.86) | 0.76 (0.70, 0.81) |
| Items 2 & 9 | 0.66 (0.59, 0.71) | 0.67 (0.60, 0.73) |
| Aim being Addressed | NFR Scale Items Used | Criterion Validity ICC (95% CI) (n = 765) | Responsiveness ICC (95% CI) (n = 475) |
|---|---|---|---|
| Primary Aim | Items 2, 6 & 7 | 0.88 (0.86, 0.90) | 0.80 (0.76, 0.83) |
| Items 2 & 6 | 0.82 (0.80, 0.84) | 0.72 (0.67, 0.76) | |
| Secondary Aim | Items 1, 2 & 9 | 0.86 (0.84, 0.88) | 0.73 (0.69, 0.77) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stevens, M.L.; Crowley, P.; Garde, A.H.; Mortensen, O.S.; Nygård, C.-H.; Holtermann, A. Validation of a Short-Form Version of the Danish Need for Recovery Scale against the Full Scale. Int. J. Environ. Res. Public Health 2019, 16, 2334. https://doi.org/10.3390/ijerph16132334
Stevens ML, Crowley P, Garde AH, Mortensen OS, Nygård C-H, Holtermann A. Validation of a Short-Form Version of the Danish Need for Recovery Scale against the Full Scale. International Journal of Environmental Research and Public Health. 2019; 16(13):2334. https://doi.org/10.3390/ijerph16132334
Chicago/Turabian StyleStevens, Matthew L., Patrick Crowley, Anne H. Garde, Ole S. Mortensen, Clas-Håkan Nygård, and Andreas Holtermann. 2019. "Validation of a Short-Form Version of the Danish Need for Recovery Scale against the Full Scale" International Journal of Environmental Research and Public Health 16, no. 13: 2334. https://doi.org/10.3390/ijerph16132334
APA StyleStevens, M. L., Crowley, P., Garde, A. H., Mortensen, O. S., Nygård, C.-H., & Holtermann, A. (2019). Validation of a Short-Form Version of the Danish Need for Recovery Scale against the Full Scale. International Journal of Environmental Research and Public Health, 16(13), 2334. https://doi.org/10.3390/ijerph16132334