“Beyond Safer Injecting”—Health and Social Needs and Acceptance of Support among Clients of a Supervised Injecting Facility

 ,
,
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Sample
3.2. Aggregate Health and Social Indicators
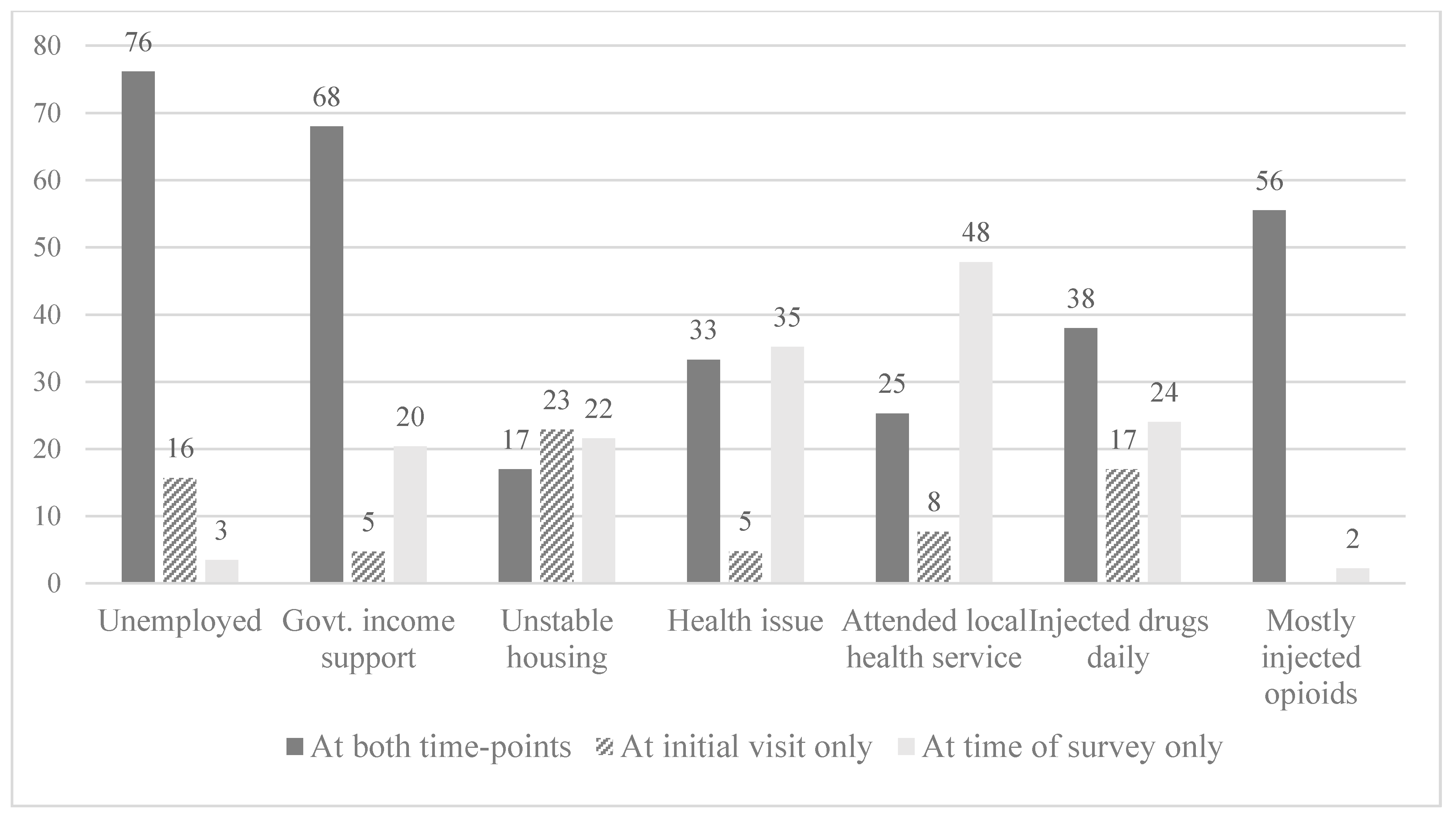
3.3. Transitions between Lower- and Higher-Risk Health and Social Indicators
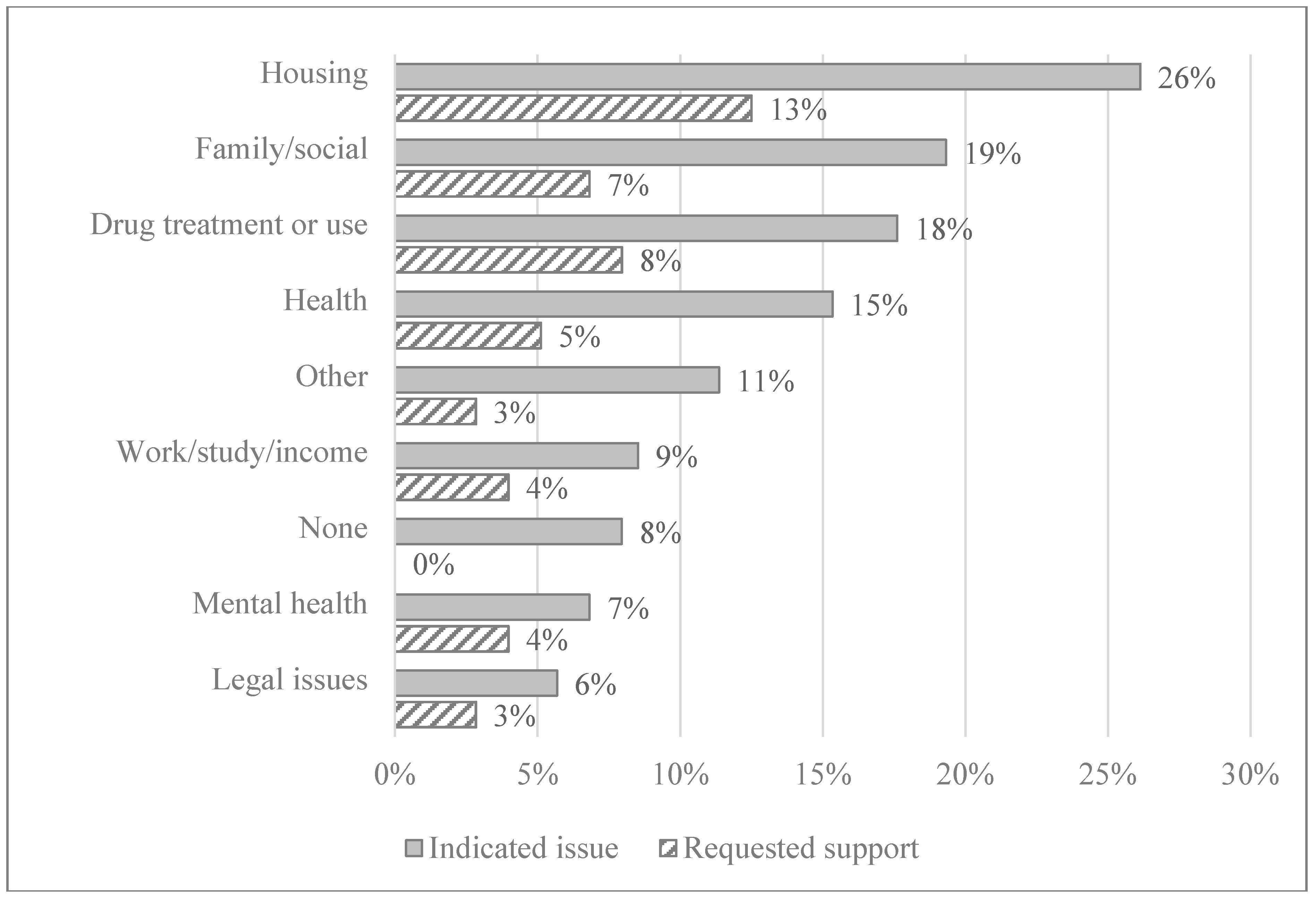
3.4. Current Issues and Extent of Support Requested
3.5. Factors Associated with Willingness to Discuss Issues with Staff
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hedrich, D.; Hartnoll, R. Harm Reduction Interventions. In Textbook of Addiction Treatment: International Perspectives; Springer Nature: Basel, Switzerland, 2015; pp. 1291–1313. [Google Scholar]
- Marlatt, G.A. Harm reduction: Come as you are. Addict. Behav. 1996, 21, 779–788. [Google Scholar] [CrossRef]
- Rhodes, T. The ‘risk environment’: A framework for understanding and reducing drug-related harm. Int. J. Drug Policy 2002, 13, 85–94. [Google Scholar] [CrossRef]
- Hedrich, D.; Kerr, T.; Dubois-Arber, F. Drug Consumption Facilities in Europe and Beyond; The European Monitoring Centre for Drugs and Drug Addiction (EMCDDA): Lisbon, Portugal, 2010. [Google Scholar]
- Belackova, V.; Salmon, A.M.; Day, C.; Ritter, A.; Shanahan, M.; Hedrich, D.; Jauncey, M.E. Drug Consumption Rooms: A systematic review of evaluation methodologies. Drug Alcohol Rev. 2019, 38, 406–422. [Google Scholar] [CrossRef] [PubMed]
- Bravo, M.J.; Royuela, L.; De la Fuente, L.; Brugal, M.T.; Barrio, G.; Domingo-Salvany, A.; Itínere Project Group. Use of supervised injection facilities and injection risk behaviours among young drug injectors. Addiction 2009, 104, 614–619. [Google Scholar] [CrossRef] [PubMed]
- Scherbaum, N.; Specka, M.; Bombeck, J.; Marrziniak, B. Drug consumption facility as part of a primary health care centre for problem drug users. Which clients are attracted? Int. J. Drug Policy 2009, 20, 447–449. [Google Scholar] [CrossRef] [PubMed]
- Kimber, J.; MacDonald, M.; van Beek, I.; Kaldor, J.; Weatherburn, D.; Lapsley, H.; Mattick, R.P. The Sydney Medically Supervised Injecting Centre: Client characteristics and predictors of frequent attendance during the first 12 months of operation. J. Drug Issues 2003, 33, 639–648. [Google Scholar] [CrossRef]
- Tyndall, M.W.; Kerr, T.; Zhang, R.; King, E.; Montaner, J.G.; Wood, E. Attendance, drug use patterns, and referrals made from North America’s first supervised injection facility. Drug Alcohol Depend. 2006, 83, 193–198. [Google Scholar] [CrossRef]
- Wood, E.; Tyndall, M.W.; Zhang, R.; Montaner, J.S.G.; Kerr, T. Rate of detoxification service use and its impact among a cohort of supervised injecting facility users. Addiction 2007, 102, 916–919. [Google Scholar] [CrossRef] [PubMed]
- Kimber, J.; Mattick, R.P.; Kaldor, J.; Van Beek, I.; Gilmour, S.; Rance, J.A. Process and predictors of drug treatment referral and referral uptake at the Sydney Medically Supervised Injecting Centre. Drug Alcohol Rev. 2008, 27, 602–612. [Google Scholar] [CrossRef]
- Toth, E.C.; Tegner, J.; Lauridsen, S.; Kappel, N. A cross-sectional national survey assessing self-reported drug intake behavior, contact with the primary sector and drug treatment among service users of Danish drug consumption rooms. Harm Reduct. J. 2016, 13, 27. [Google Scholar] [CrossRef]
- Salmon, A.M.; Belackova, V.; Schwanz, R.S.; Jauncey, M.; Hiley, S. Homelessness among clients of Sydney’s supervised injecting facility. Drugs Alcohol Today 2017, 17, 258–268. [Google Scholar] [CrossRef]
- Larney, S.; Hickman, M.; Guy, R.; Grebely, J.; Dore, G.; Gray, R.; Day, C.; Kimber, J.; Degenhardt, L. Estimating the number of people who inject drugs in Australia. BMC Public Health 2017, 17, 757. [Google Scholar] [CrossRef] [PubMed]
- Topp, L.; Day, C.; Iversen, J.; Wand, H.; Maher, L. Fifteen years of HIV surveillance among people who inject drugs: The Australian Needle and Syringe Program Survey 1995–2009. AIDS 2011, 25, 835–842. [Google Scholar] [CrossRef] [PubMed]
- Rosen, D.; Hunsaker, A.; Albert, A.; Cornelius, J.R.; Reynolds, C.F., III. Characteristics and consequences of heroin use among older adults in the United States: A review of the literature, treatment implications, and recommendations for further research. Addict. Behav. 2011, 36, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Degenhardt, L.; Degenhardt, L.; Kinner, S.A.; Degenhardt, L.; Kinner, S.A.; Roxburgh, A.; Degenhardt, L.; Kinner, S.A.; Roxburgh, A.; Black, E. Drug use and risk among regular injecting drug users in Australia: Does age make a difference? Drug Alcohol Rev. 2008, 27, 357–360. [Google Scholar] [CrossRef] [PubMed]
- Horyniak, D.; Dietze, P.; Degenhardt, L.; Higgs, P.; McIlwraith, F.; Alati, R.; Bruno, R.; Lenton, S.; Burns, L. The relationship between age and risky injecting behaviours among a sample of Australian people who inject drugs. Drug Alcohol Depend. 2013, 132, 541–546. [Google Scholar] [CrossRef] [PubMed]
- Anderson, T.L.; Levy, J.A. Marginality among older injectors in today’s illicit drug culture: Assessing the impact of ageing. Addiction 2003, 98, 761–770. [Google Scholar] [CrossRef]
- Roe, B.; Beynon, C.; Pickering, L.; Duffy, P. Experiences of drug use and ageing: Health, quality of life, relationship and service implications. J. Adv. Nurs. 2010, 66, 1968–1979. [Google Scholar] [CrossRef]
- Van Beek, I.; Kimber, J.; Dakin, A.; Gilmour, S. The Sydney Medically Supervised Injecting Centre: Reducing harm associated with heroin overdose. Crit. Public Health 2004, 14, 391–406. [Google Scholar] [CrossRef]
- DeBeck, K.; Cheng, T.; Montaner, J.S.; Beyrer, C.; Elliott, R.; Sherman, S.; Wood, E.; Baral, S. HIV and the criminalisation of drug use among people who inject drugs: A systematic review. Lancet HIV 2017, 4, e357–e374. [Google Scholar] [CrossRef]
- Rosenstein, R. Fight drug abuse, don’t subsidize it. New York Times, 27 August 2018. [Google Scholar]
- Ball, A. HIV, injecting drug use and harm reduction: A public health response. Addiction 2007, 102, 684–690. [Google Scholar] [CrossRef]
- Aubin, S. Safe injection sites and needle exchange programs: An important part of ensuring health to injection drug users. Interdiscip. J. Health Sci. 2010, 1. [Google Scholar] [CrossRef]
- Islam, M.; Day, C.; Conigrave, K. Harm reduction healthcare: From an alternative to the mainstream platform? Int. J. Drug Policy 2010, 21, 131–133. [Google Scholar] [CrossRef]
- Darke, S. Heroin overdose. Addiction 2016, 111, 2060–2063. [Google Scholar] [CrossRef]
- Roxburgh, A.; Darke, S.; Salmon, A.M.; Dobbins, T.; Jauncey, M. Frequency and severity of non-fatal opioid overdoses among clients attending the Sydney Medically Supervised Injecting Centre. Drug Alcohol Depend. 2017, 176, 126–132. [Google Scholar] [CrossRef]
- Lenton, S.; Single, E. The definition of harm reduction. Drug Alcohol Rev. 1998, 17, 213–219. [Google Scholar] [CrossRef]
- Marlatt, G.A.; Witkiewitz, K. Update on harm-reduction policy and intervention research. Annu. Rev. Clin. Psychol. 2010, 6, 591–606. [Google Scholar] [CrossRef]
- Wood, E.; Tyndall, M.W.; Zhang, R.; Stoltz, J.-A.; Lai, C.; Montaner, J.S.; Kerr, T. Attendance at supervised injecting facilities and use of detoxification services. N. Engl. J. Med. 2006, 354, 2512–2514. [Google Scholar] [CrossRef]
- DeBeck, K.; Kerr, T.; Bird, L.; Zhang, R.; Marsh, D.; Tyndall, M.; Montaner, J.; Wood, E. Injection drug use cessation and use of North America’s first medically supervised safer injecting facility. Drug Alcohol Depend. 2011, 113, 172–176. [Google Scholar] [CrossRef]
- Health Canada. Supervised Consumption Sites Explained; Government of Canada: Vancouver, BC, Canada, 2018.
- Gaddis, A.; Kennedy, M.C.; Nosova, E.; Milloy, M.-J.; Hayashi, K.; Wood, E.; Kerr, T. Use of on-site detoxification services co-located with a supervised injection facility. J. Subst. Abus. Treat. 2017, 82, 1–6. [Google Scholar] [CrossRef]
- British Columbia Centre on Substa (BCCS). Supervised Consumption Services: Operational Guidance; British Columbia Centre on Substance Use, Ministry of Health: Vancouver, BC, Canada, 2018. [Google Scholar]
- Rachlis, B.S.; Kerr, T.; Montaner, J.S.; Wood, E. Harm reduction in hospitals: Is it time? Harm Reduct. J. 2009, 6, 19. [Google Scholar] [CrossRef]
- Crawford, S. Shouting through bullet-proof glass: Some reflections on pharmacotherapy provision in one Australian clinic. Int. J. Drug Policy 2013, 24, e14–e17. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | Survey Participants n = 182 % (n/N) | Non-Participants n = 318 % (n/N) |
|---|---|---|
| Gender | ||
| Female | 29 (53) | 24 (77) |
| Male | 69 (126) | 74 (235) |
| Transgender | 1 (3) | 2 (5) |
| Not stated | 0 (0) | <1 (2) |
| Age, in years—median (mean; SD) | 42 (43.0; 9.0) | 43 (42.6; 6.9) |
| Aboriginality | ||
| Neither Aboriginal nor Torres Strait Islander | 78 (141) | 73 (232) |
| Aboriginal and/or Torres Strait Islander | 17 (31) | 16 (50) |
| Did not specify | 2 (3) | 1 (3) |
| Missing | 4 (7) | 10 (31) |
| Other characteristics (assessed at initial visit) | ||
| Stable accommodation | 60 (92/153) | 67 (86/172) |
| Employed | 20 (35/174) | 22 (63/288) |
| Ever in drug treatment | 61 (111/182) | 59 (188/318) |
| Ever in prison | 45 (77/94) | 41 (117/284) |
| Ever overdosed | 38 (64/169) | 39 (108/278) |
| Health issue | 36 (52/143) | 29 (67/229) |
| Injected drugs daily * | 55 (94/171) | 45 (124/277) |
| Client of local primary health care service ** | 33 (60/182) | 23 (74/318) |
| Drug used most (assessed in the 8 months before survey) a | ||
| Heroin | 54 | 52 |
| Oxycodone | 5 | 5 |
| Buprenorphine ** | 8 | 3 |
| Methadone | 6 | 8 |
| Morphine | 6 | 6 |
| Cocaine | 4 | 2 |
| Methamphetamine | 31 | 40 |
| Service use—median (mean; SD) | ||
| Number of visits since initial visit *** | 313 (796.2; 1308.6) | 97 (406.2; 811.6) |
| Number of visits during survey period *** | 5 (9.0; 10.4) | 2 (2.9; 3.9) |
| Number of referrals in the past 12 months *** | 1 (2.0; 2.7) | 0 (0.6; 1.4) |
| Number of years since initial visit ** | 10.5 (9.4; 8.5) | 8.3 (8.2; 7.6) |
| Age in years when first injected | 18 (19.3; 6.9) | 18 (19.6; 7.0) |
| Health and Social Indicators | N | At the Time of the Survey % | At Initial Visit % | t-Test |
|---|---|---|---|---|
| Unstable housing | 153 | 39 | 40 | −0.242 |
| Unemployed | 172 | 92 | 80 | −3.795 ** |
| Government income support | 172 | 88 | 73 | 0.000 *** |
| Currently has a physical health issue | 105 | 69 | 38 | −5.608 ** |
| Currently has a mental health issue | 176 | 64 | 18 | 0.000 *** |
| Attendance at a nearby primary healthcare service | 182 | 73 | 33 | −8.596 ** |
| Injected daily in the past month | 171 | 62 | 55 | −1.438 |
| Injected mostly opioid | 182 | 58 | 56 | −2.017 * |
| Engaged in drug treatment | 181 | 93 | 61 | −8.778 ** |
| Has been to prison | 171 | 73 | 45 | −9.936 ** |
| Has had an overdose | 167 | 61 | 38 | 5.187 ** |
| Interested in Support Now or at Next Visit | Not Interested in Support or Does Not Know | |
|---|---|---|
| % (n/N) | % (n/N) | |
| Take-home naloxone training | ||
| All participants | 48 (51/106) | 52 (55/106) |
| Participants not previously trained | 44 (41/93) | 56 (52/93) |
| Hepatitis C testing and treatment | ||
| All participants | 25 (41/166) | 75 (125/166) |
| Participants not previously tested | 18 (2/11) | 82 (9/11) |
| Drug treatment | 21 (38/181) | 79 (143/181) |
| Physical health support | 21 (29/135) | 79 (106/135) |
| Accommodation | 20 (36/182) | 80 (146/182) |
| Mental health support | 12 (19/165) | 88 (146/165) |
| Support (%) | ||
| Any | 63 | 37 |
| Excluding take-home naloxone training | 52 | 48 |
| Willingness to Discuss with Staff AOR (p Value) | |||
|---|---|---|---|
| Housing Issues | Drug Use and Treatment | Take-Home Naloxone Training | |
| Aboriginal and/or Torres Strait Islander origin 1 | - | - | 4.41 (0.024) |
| Heroin used most at the Sydney SIF | - | 3.90 (0.02) 1 | 3.62 (0.054) 2 |
| Methamphetamine used most the Sydney SIF | - | 2.27 (0.086) | 3.46 (0.069) |
| Buprenorphine used most at the Sydney SIF | 0.068 (0.042) | - | - |
| Oxycodone used in past month at the Sydney SIF | 3.25 (0.068) | - | - |
| Expressed this issue as the most important | 12.74 (p < 0.001) 3 | 3.18 (0.026) 4 | - |
| Currently in unstable accommodation | 5.57 (0.009) | - | - |
| Currently in drug treatment | - | 0.43 (0.044) | - |
| Ever in drug treatment | - | 0.42 (0.087) | - |
| Previously received take-home naloxone training | - | 2.28 (0.057) | - |
| Experienced overdose outside of the Sydney SIF | 3.32 (0.072) | - | 5.12 (0.008) |
| Experienced overdose for the first time since initial visit | - | - | 0.34 (0.081) |
| Number of observations | n = 112 | n = 159 | n = 78 5 |
| LR chi2, df, (p) | 38.33, 5, (p < 0.001) | 25.65, 6, (0.003) | 15.47, 5, (0.0085) |
| Pseudo R2 | 0.345 | 0.1530 | 0.1431 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Belackova, V.; Silins, E.; Salmon, A.M.; Jauncey, M.; Day, C.A. “Beyond Safer Injecting”—Health and Social Needs and Acceptance of Support among Clients of a Supervised Injecting Facility. Int. J. Environ. Res. Public Health 2019, 16, 2032. https://doi.org/10.3390/ijerph16112032
Belackova V, Silins E, Salmon AM, Jauncey M, Day CA. “Beyond Safer Injecting”—Health and Social Needs and Acceptance of Support among Clients of a Supervised Injecting Facility. International Journal of Environmental Research and Public Health. 2019; 16(11):2032. https://doi.org/10.3390/ijerph16112032
Chicago/Turabian StyleBelackova, Vendula, Edmund Silins, Allison M. Salmon, Marianne Jauncey, and Carolyn A. Day. 2019. "“Beyond Safer Injecting”—Health and Social Needs and Acceptance of Support among Clients of a Supervised Injecting Facility" International Journal of Environmental Research and Public Health 16, no. 11: 2032. https://doi.org/10.3390/ijerph16112032
APA StyleBelackova, V., Silins, E., Salmon, A. M., Jauncey, M., & Day, C. A. (2019). “Beyond Safer Injecting”—Health and Social Needs and Acceptance of Support among Clients of a Supervised Injecting Facility. International Journal of Environmental Research and Public Health, 16(11), 2032. https://doi.org/10.3390/ijerph16112032