Emerging Resistance of Neglected Tropical Diseases: A Scoping Review of the Literature

 , ,
, ,
Abstract
1. Introduction
2. Methods
2.1. Protocol Registration
2.2. Eligibility Criteria
2.3. Search Strategy
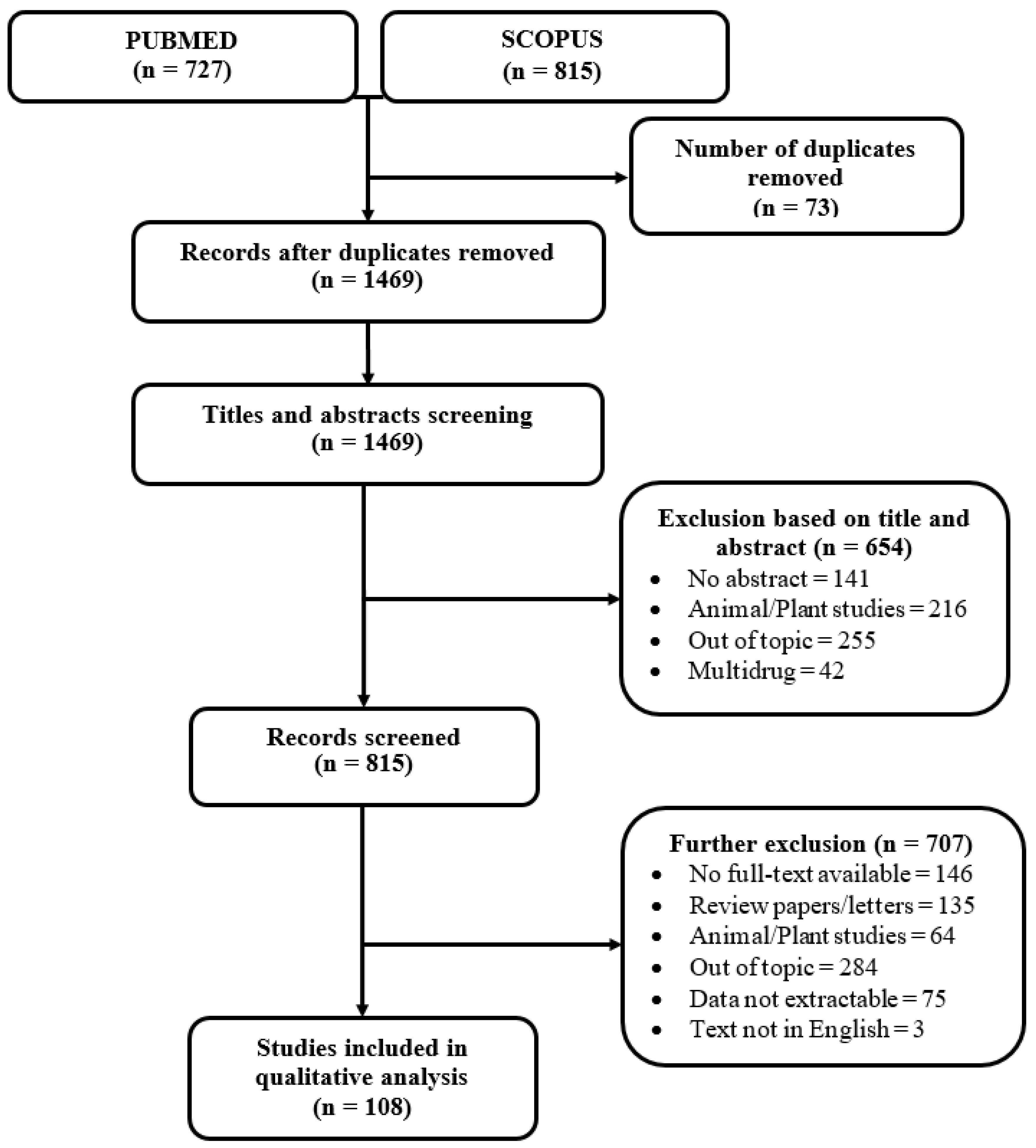
2.4. Study Selection
2.5. Assessment of the Methodological Quality
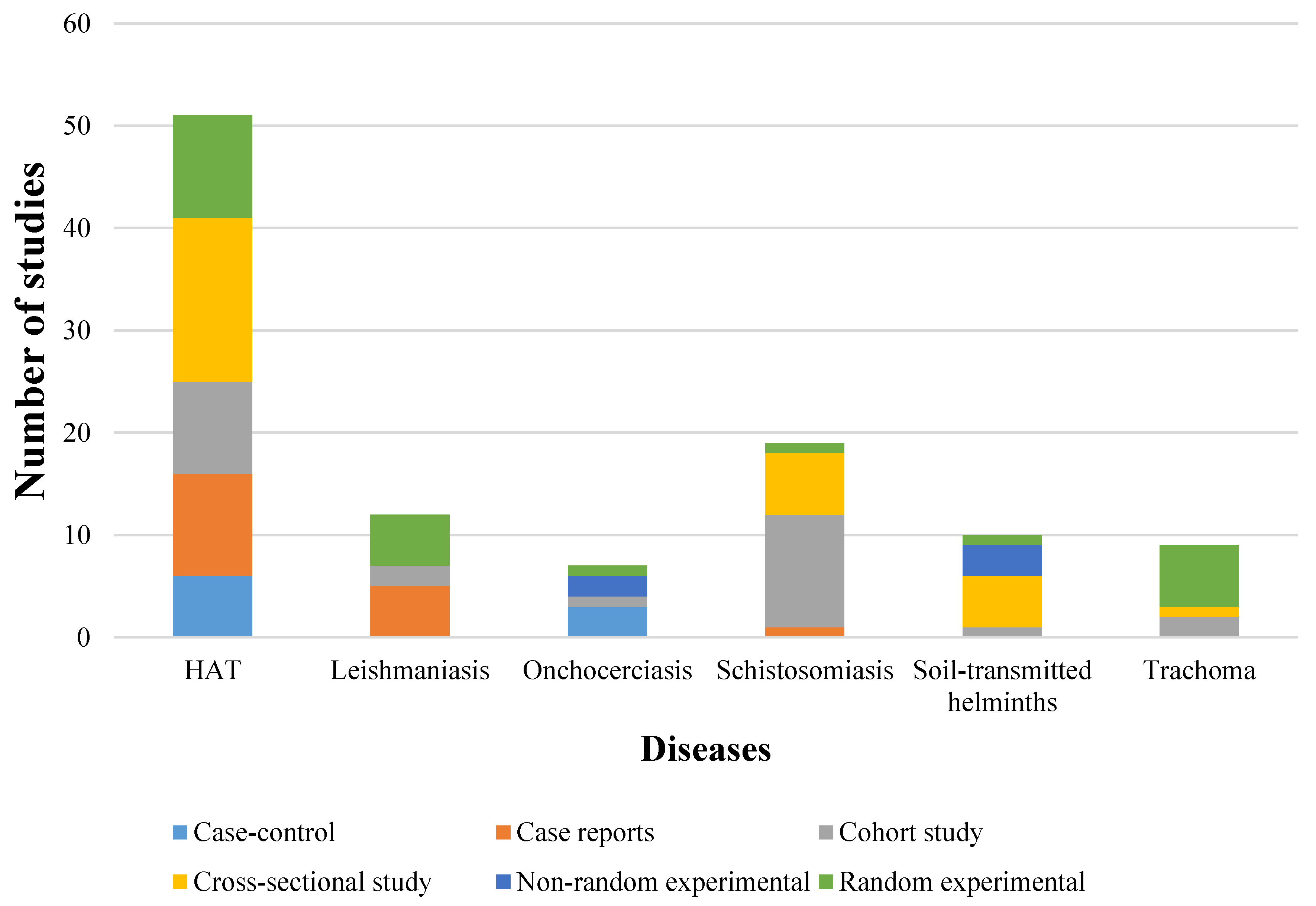
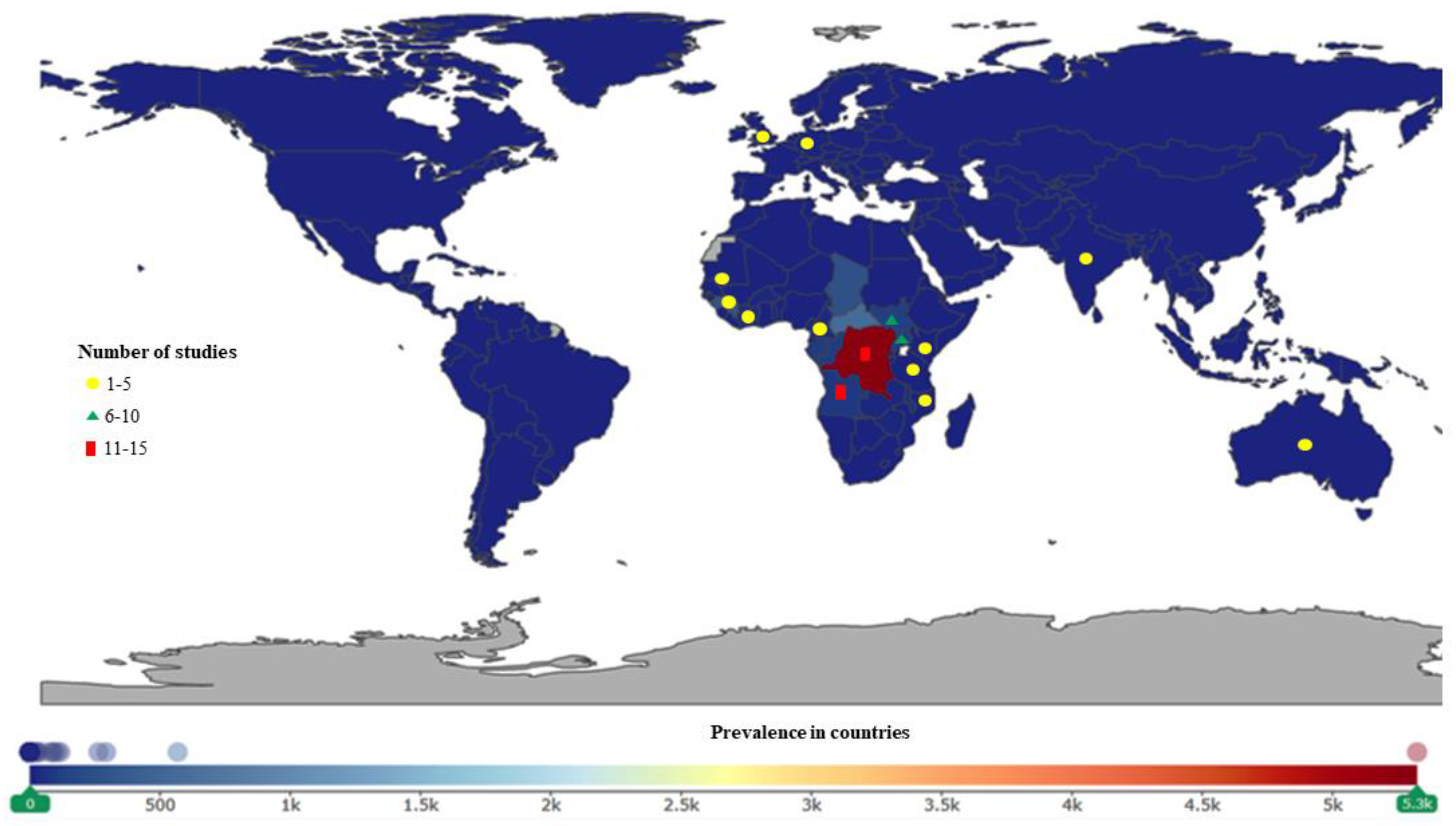
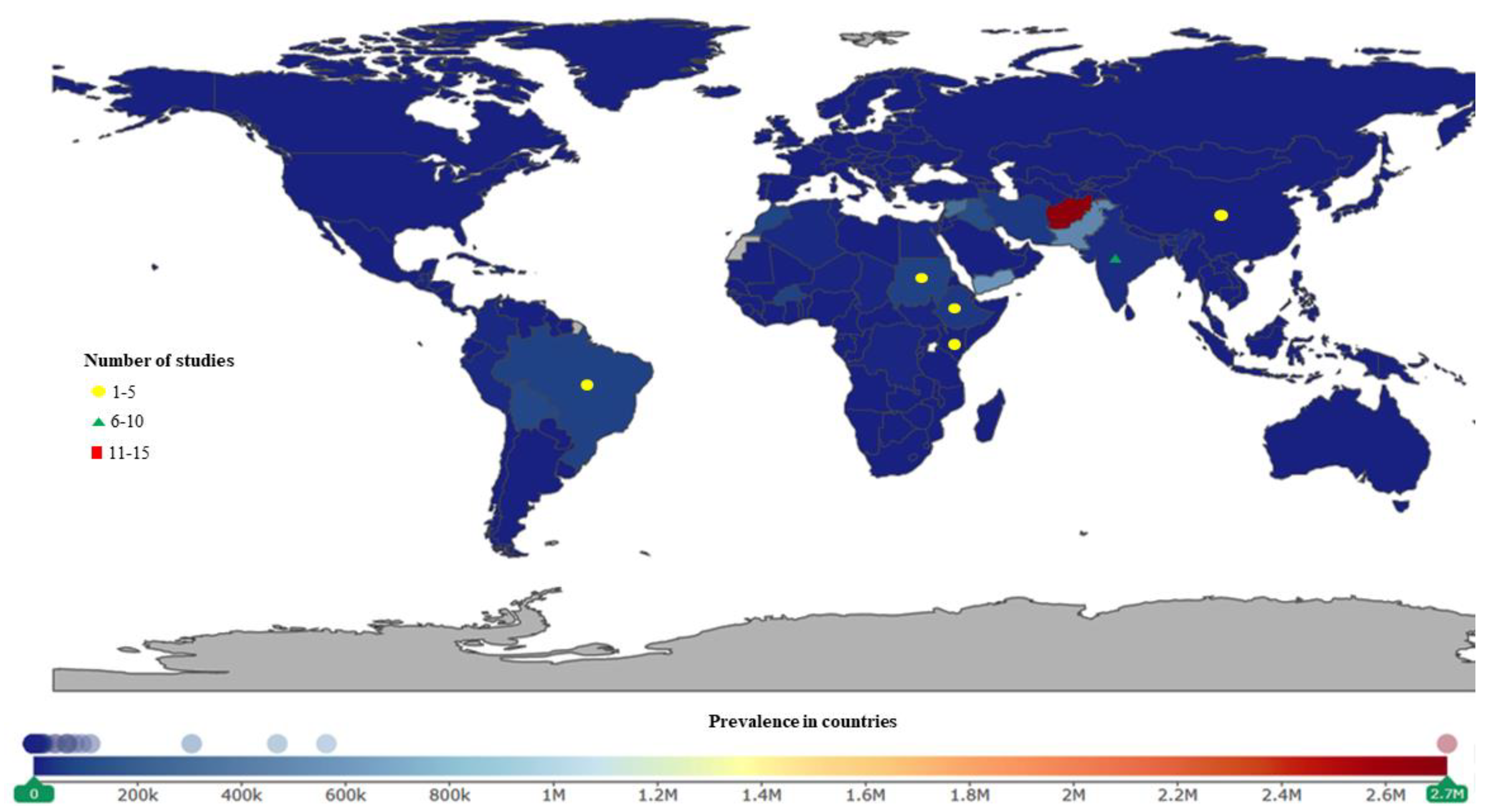
3. Results
Methodological Quality Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kappagoda, S.; Ioannidis, J. Prevention and Control of Neglected Tropical Diseases: Overview of Randomized Trials, Systematic Reviews and Meta-Analyses; Bulletin of the World Health Organization: Geneva, Switzerland, 2014; Volume 92, pp. 356–366C. [Google Scholar]
- Akinsolu, F.T.; de Paiva, V.N.; Souza, S.S.; Varga, O. Patent landscape of neglected tropical diseases: An analysis of worldwide patent families. Glob. Health 2017, 13, 82. [Google Scholar] [CrossRef]
- World Health Organization. Neglected Tropical Diseases; WHO: Geneva, Switzerland, 2017; Available online: http://www.who.int/neglected_diseases/diseases/en/ (accessed on 12 March 2018).
- Hotez, P.J. Ten failings in global neglected tropical diseases control. PLoS Negl. Trop. Dis. 2017, 11, e0005896. [Google Scholar] [CrossRef] [PubMed]
- Kealey, A. Neglected tropical diseases: Infection, modeling, and control. J. Health Care Poor Underserved 2010, 21, 53–69. [Google Scholar] [CrossRef] [PubMed]
- Molyneux, D.H.; Hotez, P.J.; Fenwick, A. “Rapid-impact interventions”: How a policy of integrated control for Africa’s neglected tropical diseases could benefit the poor. PLoS Med. 2005, 2, e336. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Working to Overcome the Global Impact of Neglected Tropical Diseases: First WHO Report on Neglected Tropical Diseases; WHO: Geneva, Switzerland, 2010. [Google Scholar]
- Rosenberg, M.; Utzinger, J.; Addiss, D.G. Preventive chemotherapy versus innovative and intensified disease management in neglected tropical diseases: A distinction whose shelf life has expired. PLoS Negl. Trop. Dis. 2016, 10, e0004521. [Google Scholar] [CrossRef]
- Secretary-General, U. The United Nations Secretary-General’s High-Level Panel on Access to Medicines Report: Promoting Innovation and Access to Health Technologies. 2016. Available online: http://www.unsgaccessmeds.org/final-report (accessed on 10 February 2018).
- Uniting to Combat NTDs. The London Declaration; Uniting to Combat NTDs (Online), 2016. Available online: https://unitingtocombatntds.org/london-declaration-neglected-tropical-diseases/ (accessed on 10 February 2018).
- Smits, H.L. Prospects for the control of neglected tropical diseases by mass drug administration. Expert Rev. Anti-Infect. Ther. 2009, 7, 37–56. [Google Scholar] [CrossRef]
- World Health Organization. Summary of Global Update on Preventive Chemotherapy Implementation in 2015 Preventive Chemotherapy (PC) is Referred. Wkly. Epidemiol. Rec. 2016, 91, 441–460. [Google Scholar]
- The Review on Antimicrobial Resistance. Tackling Drug-Resistant Infections Globally: Final Report and Recommendations; Wellcome Trust and HM Government: London, UK, 2016. [Google Scholar]
- World Health Organization. Antimicrobial Resistance: Global Report on Surveillance; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- World Health Organization. Global Antimicrobial Resistance Surveillance System (GLASS) Report: Early Implementation 2016–2017; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Tambo, E.; Ai, L.; Zhou, X.; Tambo, E.; Ai, L.; Zhou, X.; Chen, J.H.; Hu, W.; Bergquist, R.; Guo, J.-G.; et al. Surveillance-response systems: The key to elimination of tropical diseases. Infect. Dis. Poverty 2014, 3, 17. [Google Scholar] [CrossRef]
- World Health Organization. FAO/OIE/WHO Tripartite Collaboration on AMR 2019. Available online: https://www.who.int/foodsafety/areas_work/antimicrobial-resistance/tripartite/en/ (accessed on 9 May 2019).
- Rochford, C.; Sridhar, D.; Woods, N.; Saleh, Z.; Hartenstein, L.; Ahlawat, H.; Whiting, E.; Dybul, M.; Cars, O.; Goosby, E.; et al. Global governance of antimicrobial resistance. Lancet 2018, 391, 1976–1978. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Moher, D.; Cook, D.J.; Eastwood, S.; Olkin, I.; Rennie, D.; Stroup, D.F. Improving the quality of reports of meta-analyses of randomised controlled trials: The QUOROM statement. Revista Española de Salud Pública 2000, 74, 107–118. [Google Scholar]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Vandenbroucke, J.P.; Gøtzsche, P.C. The Strengthening the Reporting of Observational Studies in Epidemiology [STROBE] statement: Guidelines for reporting observational studies. Gac. Sanit. 2008, 22, 144–150. [Google Scholar] [CrossRef]
- Thomas, B.; Ciliska, D.; Dobbins, M.; Micucci, S. A process for systematically reviewing the literature: Providing the research evidence for public health nursing interventions. Worldviews Evid. Based Nurs. 2004, 1, 176–184. [Google Scholar] [CrossRef]
- Deeks, J.; Dinnes, J.; D’amico, R.; Sowden, A.J.; Sakarovitch, C.; Song, F.; Petticrew, M.; Altman, D.G. Evaluating Non-Randomised Intervention Studies. Health Technol. Assess. 2003, 7, 1–173. [Google Scholar] [CrossRef]
- University of Washington. Institute for Health Metrics and Evaluation Seattle 2015. Available online: http://www.healthdata.org/ (accessed on 3 April 2018).
- World Health Organization. Global Action Plan on Antimicrobial Resistance; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- Ponte-Sucre, A.; Gamarro, F.; Dujardin, J.-C.; Barrett, M.P.; López-Vélez, R.; García-Hernández, R.; Pountain, A.l.W.; Mwenechanya, R.; Papadopoulou, B. Drug resistance and treatment failure in leishmaniasis: A 21st century challenge. PLoS Negl. Trop. Dis. 2017, 11, e0006052. [Google Scholar] [CrossRef]
- World Health Organization. Integrated NTD Database; World Health Organization, 2018. Available online: http://www.who.int/neglected_diseases/data/ntddatabase/en/ (accessed on 26 March 2018).
- World Health Organization. Integrating Neglected Tropical Diseases into Global Health and Development: Fourth WHO Report on Neglected Tropical Diseases: Executive Summary; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Krentel, A.; Gyapong, M.; Mallya, S.; Boadu, N.Y.; Amuyunzu-Nyamongo, M.; Stephens, M.; McFarland, D.A. Review of the factors influencing the motivation of community drug distributors towards the control and elimination of neglected tropical diseases (NTDs). PLoS Negl. Trop. Dis. 2017, 11, e0006065. [Google Scholar] [CrossRef]
- Barbé, B.; Verdonck, K.; El-Safi, S.; Khanal, B.; Teav, S.; Kalo, J.R.L.; Ravinetto, R.; Chappuis, F.; Boelaert, M.; Jacobs, J. Rapid diagnostic tests for neglected infectious diseases: Case study highlights need for customer awareness and postmarket surveillance. PLoS Negl. Trop. Dis. 2016, 10, e0004655. [Google Scholar] [CrossRef] [PubMed]
- Peeling, R.W.; Boeras, D.I.; Nkengasong, J. Re-imagining the future of diagnosis of Neglected Tropical Diseases. Comput. Struct. Biotechnol. J. 2017, 15, 271–274. [Google Scholar] [CrossRef]
- Albonico, M.; Levecke, B.; LoVerde, P.; Montresor, A.; Prichard, R.; Vercruysse, J.; Webster, J.P. Monitoring the efficacy of drugs for neglected tropical diseases controlled by preventive chemotherapy. J. Glob. Antimicrob. Resist. 2015, 3, 229–236. [Google Scholar] [CrossRef] [PubMed]
- Webster, J.P.; Molyneux, D.H.; Hotez, P.J.; Fenwick, A. The contribution of mass drug administration to global health: Past, present and future. Phil. Trans. R. Soc. B Biol. Sci. 2014, 369, 20130434. [Google Scholar] [CrossRef]
- Ravinetto, R.; Alirol, E.; Mahendradhata, Y.; Rijal, S.; Lutumba, P.; Sacko, M.; El-Safi, S.; Lim, K.; van Loen, H.; Jacobs, J.; et al. Clinical research in neglected tropical diseases: The challenge of implementing good clinical (laboratory) practices. PLoS Negl. Trop. Dis. 2016, 10, e0004654. [Google Scholar] [CrossRef]
- Keenan, J.D.; Hotez, P.J.; Amza, A.; Stoller, N.E.; Gaynor, B.D.; Porco, T.C.; Lietman, T.M. Elimination and eradication of neglected tropical diseases with mass drug administrations: A survey of experts. PLoS Negl. Trop. Dis. 2013, 7, e2562. [Google Scholar] [CrossRef]
- Zuber, J.A.; Takala-Harrison, S. Multidrug-resistant malaria and the impact of mass drug administration. Infect. Drug Resist. 2018, 11, 299. [Google Scholar] [CrossRef] [PubMed]
- White, N.J. Does antimalarial mass drug administration increase or decrease the risk of resistance? Lancet Infect. Dis. 2017, 17, e15–e20. [Google Scholar] [CrossRef]
- Inci, R.; Ozturk, P.; Mulayim, M.K.; Ozyurt, K.; Alatas, E.T.; Inci, M.F. Effect of the Syrian civil war on prevalence of cutaneous leishmaniasis in southeastern Anatolia, Turkey. Med Sci. Monit. 2015, 21, 2100–2104. [Google Scholar] [CrossRef]
- Zhang, Y.; MacArthur, C.; Mubila, L.; Baker, S. Control of neglected tropical diseases needs a long-term commitment. BMC Med. 2010, 8, 67. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Data | Neglected Tropical Diseases (NTDs) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Human African Trypanosomiasis (Studied Drugs) | Leishmaniasis (Studied Drug) | Onchocerciasis (Studied Drug) | Schistosomiasis (Studied Drug) | Soil-Transmitted Helminths (Studied Drugs) | Trachoma (Studied Drug) | ||||||
| Eflornithine | Melarsoprol | Pentamidine | Suramin | Amphotericin B | Ivermectin | Praziquantel | Albendazole | Mebendazole | Azithromycin | ||
| Study Design | Experimental | 2 | 6 | 1 | 1 | 5 | 3 | 1 | 2 | 2 | 6 |
| Observational | 8 | 14 | 12 | 7 | 7 | 4 | 18 | 3 | 2 | 4 | |
| Study Settings | Not Specified | 4 | 3 | 3 | 2 | 0 | 0 | 1 | 2 | 0 | 1 |
| Rural | 4 | 17 | 6 | 5 | 2 | 7 | 13 | 3 | 4 | 9 | |
| Urban | 2 | 0 | 4 | 1 | 10 | 0 | 5 | 0 | 0 | 0 | |
| Gender | Both | 7 | 18 | 12 | 3 | 7 | 4 | 14 | 5 | 4 | 10 |
| Female only | 1 | 0 | 0 | 0 | 1 | 0 | 3 | 0 | 0 | 0 | |
| Male only | 2 | 2 | 1 | 5 | 4 | 3 | 2 | 0 | 0 | 0 | |
| Age Range | Adults | 6 | 8 | 3 | 5 | 5 | 4 | 6 | 0 | 0 | 0 |
| Children | 0 | 0 | 1 | 1 | 1 | 0 | 7 | 5 | 3 | 8 | |
| Both | 4 | 12 | 8 | 2 | 6 | 3 | 6 | 0 | 1 | 2 | |
| Resistance by Tests | YES | 9 | 18 | 13 | 8 | 9 | 6 | 18 | 5 | 4 | 9 |
| NO | 1 | 2 | 0 | 0 | 3 | 1 | 1 | 0 | 0 | 1 | |
| Clinical Resistance | YES | 6 | 6 | 7 | 7 | 10 | 0 | 4 | 1 | 0 | 4 |
| NO | 64 | 14 | 6 | 1 | 2 | 7 | 15 | 4 | 4 | 6 | |
| Countries of Study | Angola, Cote d’Ivoire, Democratic Republic of Congo, Germany, South Sudan, Uganda, and Western Australia | Angola, Cameroon, Cote d’Ivoire, Central African Republic (CAR), Democratic Republic of Congo, Equatorial Guinea, Kenya, South Sudan, Tanzania, and Uganda | Angola, Central African Republic (CAR), Cote d’Ivoire, Democratic Republic of Congo, Equatorial Guinea, South Sudan, and Uganda | Belgium, Cameroon, Democratic Republic of Congo, India, England, Malawi and Tanzania | Brazil, China, Ethiopia, India, Sudan, and Kenya | Cameroon, Ghana, and South Sudan | China, Cote d’Ivoire, Egypt, Kenya, South Sudan, Tanzania, Uganda, and Zambia | Brazil, Cambodia, Cameroon, Ethiopia, Haiti, India, Indonesia, Kenya, Panama, Tanzania, and Vietnam | Indonesia and Tanzania | Ethiopia, Nepal, and Tanzania | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Akinsolu, F.T.; Nemieboka, P.O.; Njuguna, D.W.; Ahadji, M.N.; Dezso, D.; Varga, O. Emerging Resistance of Neglected Tropical Diseases: A Scoping Review of the Literature. Int. J. Environ. Res. Public Health 2019, 16, 1925. https://doi.org/10.3390/ijerph16111925
Akinsolu FT, Nemieboka PO, Njuguna DW, Ahadji MN, Dezso D, Varga O. Emerging Resistance of Neglected Tropical Diseases: A Scoping Review of the Literature. International Journal of Environmental Research and Public Health. 2019; 16(11):1925. https://doi.org/10.3390/ijerph16111925
Chicago/Turabian StyleAkinsolu, Folahanmi T., Priscilla O. Nemieboka, Diana W. Njuguna, Makafui N. Ahadji, Dora Dezso, and Orsolya Varga. 2019. "Emerging Resistance of Neglected Tropical Diseases: A Scoping Review of the Literature" International Journal of Environmental Research and Public Health 16, no. 11: 1925. https://doi.org/10.3390/ijerph16111925
APA StyleAkinsolu, F. T., Nemieboka, P. O., Njuguna, D. W., Ahadji, M. N., Dezso, D., & Varga, O. (2019). Emerging Resistance of Neglected Tropical Diseases: A Scoping Review of the Literature. International Journal of Environmental Research and Public Health, 16(11), 1925. https://doi.org/10.3390/ijerph16111925