Reasons for Surgery Cancellation in a General Hospital: A 10-year Study



Abstract
:1. Introduction
2. Methods
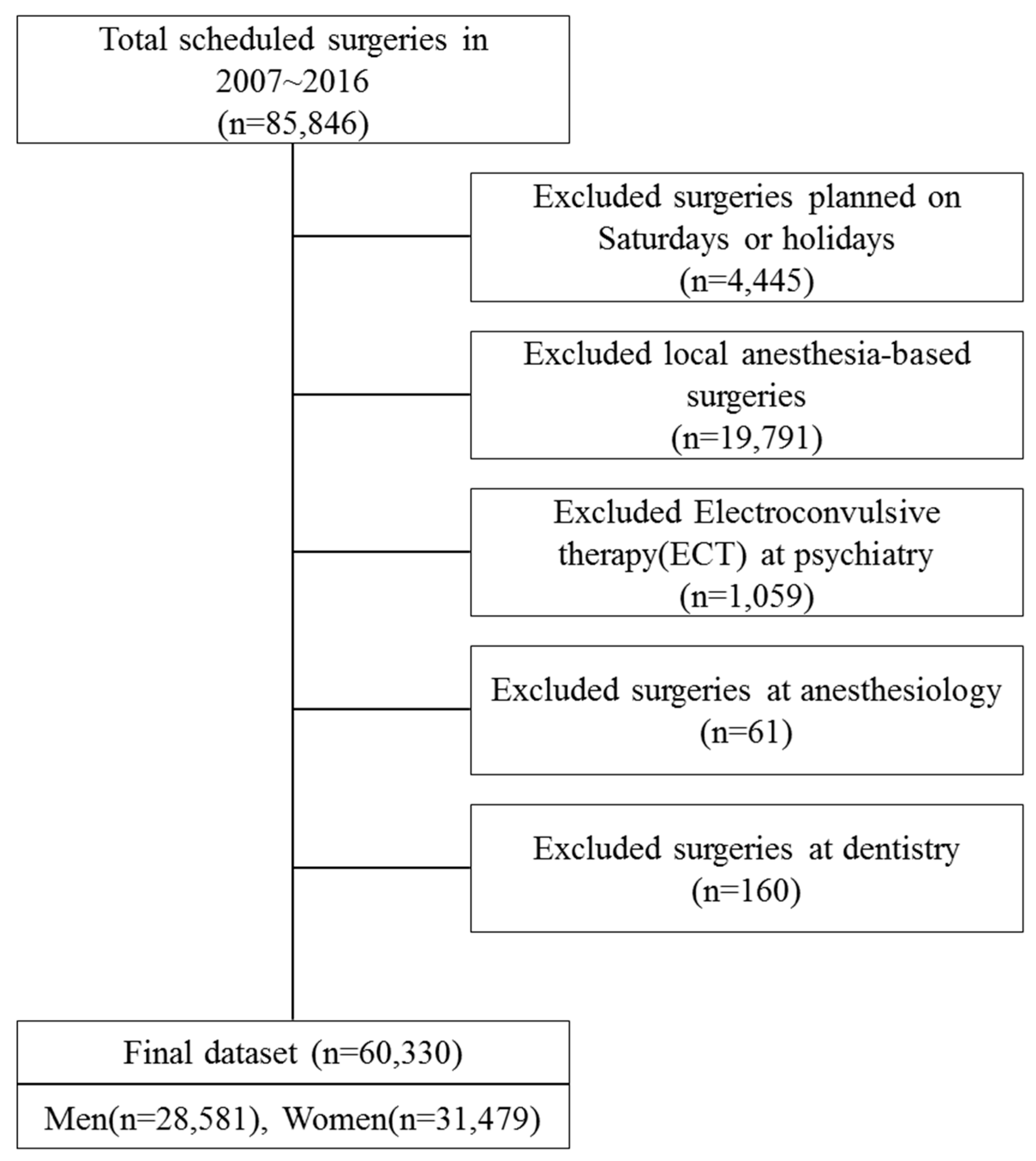
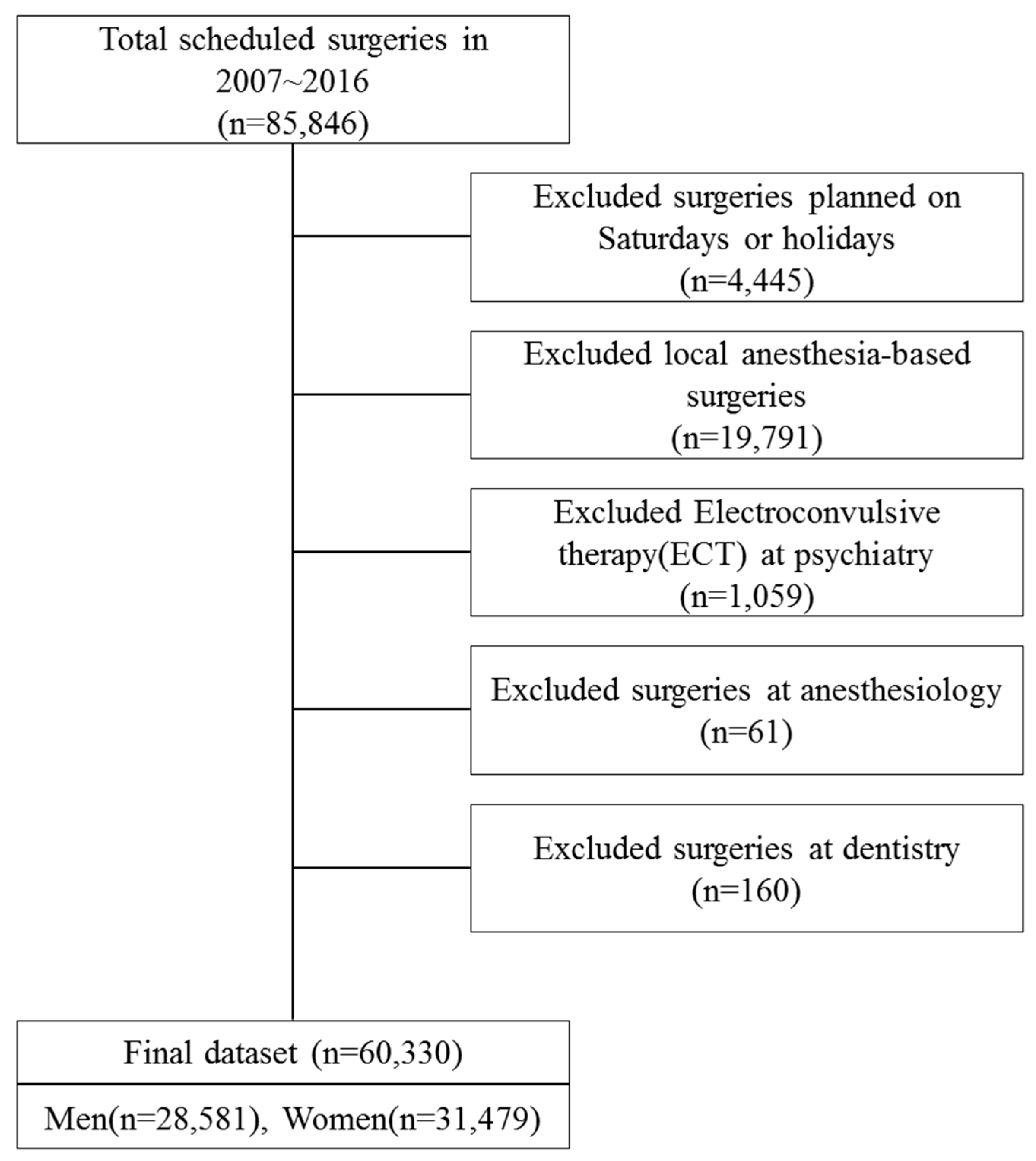
2.1. Data Collection
2.2. Variables
2.3. Statistical Analysis
3. Results
3.1. Comparison of Characteristics Between Performed and Cancelled Surgeries
3.2. Analysis of the Reasons for Cancellation
3.3. Multivariate Analysis on Surgery Cancellation Factors
3.3.1. All Surgeries
3.3.2. Subgroup Analysis by the Type of Surgery
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Song, J.-H.; Ye, M.-H. The intervention study for efficient utilization of operating room. J. Korean Hosp. Assoc. 1992, 21, 27–41. [Google Scholar]
- Kim, K.A. Delayed Use of Operating Rooms in a University Hospital. Master’s Thesis, Graduate School of Public Health, Yonsei University, Seoul, Korea, 2002. [Google Scholar]
- Yoon, S.J.; Choi, K.O.; Yoon, S.M.; Lim, H.J.; Lee, H.W.; Cho, H.; Chang, S.H. A statistical analysis of the causes of cancellation of elective operation. Korean J. Anesthesiol. 2001, 40, 139–143. [Google Scholar] [CrossRef]
- Kim, H.-O. Analysis on Factors for a Cancellation of a Regular Operation and the Study on the Efficient Administration of an Operation Room. Master’s Thesis, Graduate School of Administration, Kyung-Hee University, Seoul, Korea, 1999. [Google Scholar]
- Pollard, J.B.; Olson, L. Early outpatient preoperative anesthesia assessment: Does it help to reduce operating room cancellations? Anesth. Analg. 1999, 89, 502–505. [Google Scholar] [PubMed]
- Ferschl, M.B.; Tung, A.; Sweitzer, B.; Huo, D.; Glick, D.B. Preoperative clinic visits reduce operating room cancellations and delays. Anesthesiol. J. Am. Soc. Anesthesiol. 2005, 103, 855–859. [Google Scholar] [CrossRef]
- You, S.-H.; Cho, S.-H.; Kim, C.-S. Analysis on cancellation rate and reasons for a cancellation of an elective operation. J. Soonchunhyang Med. Sci. 2004, 10, 431–436. [Google Scholar]
- Sanjay, P.; Dodds, A.; Miller, E.; Arumugam, P.; Woodward, A. Cancelled elective operations: An observational study from a district general hospital. J. Health Organ. Manag. 2007, 21, 54–58. [Google Scholar] [CrossRef] [PubMed]
- Macario, A. Are your hospital operating rooms “efficient”? A scoring system with eight performance indicators. Anesthesiol. J. Am. Soc. Anesthesiol. 2006, 105, 237–240. [Google Scholar] [CrossRef]
- Dimitriadis, P.; Iyer, S.; Evgeniou, E. The challenge of cancellations on the day of surgery. Int. J. Surg. 2013, 11, 1126–1130. [Google Scholar] [CrossRef] [PubMed]
- Han, H.J. Preoperative management of chronic disease. J. Korean Med. Assoc. 2014, 57, 826–831. [Google Scholar] [CrossRef]
- Agha, R.A.; Borrelli, M.R.; Vella-Baldacchino, M.; Thavayogan, R.; Orgill, D.P.; Pagano, D.; Pai, P.S.; Basu, S.; McCaul, J.; Millham, F. The strocss statement: Strengthening the reporting of cohort studies in surgery. Int. J. Surg. 2017, 46, 198–202. [Google Scholar] [CrossRef] [PubMed]
- Song, S.O.; Kim, S.Y.; Song, S.K. Reasons of the cancellation of an elective planned surgery. Korean J. Anesthesiol. 1992, 25, 602–609. [Google Scholar] [CrossRef]
- Park, Y.H.; Jin, H.Y. Analysis of cause for cancellation of elective operation. Korean J. Anesthesiol. 2008, 54, 486–492. [Google Scholar] [CrossRef]
- Bae, J.I. Etiology of the cancellation in the elective and emergency surgery. Korean J. Anesthesiol. 1999, 36, 757–763. [Google Scholar] [CrossRef]
- McKendrick, D.R.; Cumming, G.P.; Lee, A.J. A 5-year observational study of cancellations in the operating room: Does the introduction of preoperative preparation have an impact? Saudi J. Anaesth. 2014, 8, S8. [Google Scholar] [CrossRef] [PubMed]
- Cihoda, J.H.; Alves, J.R.; Fernandes, L.A.; Fernandes, L.A. The analysis for the causes of surgical cancellations in a Brazilian university hospital. Care Manag. J. 2015, 16. [Google Scholar] [CrossRef] [PubMed]
- Kaddoum, R.; Fadlallah, R.; Hitti, E.; Fadi, E.-J.; El Eid, G. Causes of cancellations on the day of surgery at a tertiary teaching hospital. BMC Health Serv. Res. 2016, 16, 259. [Google Scholar] [CrossRef] [PubMed]
- Sung, W.-C.; Chou, A.-H.; Liao, C.-C.; Yang, M.-W. Operation cancellation at chang gung memorial hospital. Chang. Gung Med. J. 2010, 33, 568–575. [Google Scholar] [PubMed]
- Kwon, S.T.; Lee, Y.S.; Han, E.; Kim, T.H. Factors associated with no-show in an academic medical center. Korean Public Health Res. 2015, 41, 29–46. [Google Scholar]

{kind=link}
| Variables | Total | Surgery | Cancellation | p-Value | ||||
|---|---|---|---|---|---|---|---|---|
| N | % | N | % | |||||
| General characteristics | Sex | Male | 28,851 | 26,258 | 91.0 | 2593 | 9.0 | <0.0001 |
| Female | 31,479 | 29,238 | 92.9 | 2241 | 7.1 | |||
| Age | ≤19 | 9183 | 8429 | 91.8 | 754 | 8.2 | <0.0001 | |
| 20–39 | 14,376 | 13,512 | 94.0 | 864 | 6.0 | |||
| 40–59 | 20,887 | 9227 | 92.1 | 1660 | 8.0 | |||
| 60–79 | 13,850 | 2529 | 90.5 | 1321 | 9.5 | |||
| ≥80 | 2034 | 1799 | 88.5 | 235 | 11.6 | |||
| Admission type | Outpatient/Day surgery clinic | 2117 | 2064 | 97.5 | 53 | 2.5 | <0.0001 | |
| Inpatient | 58,213 | 53,432 | 91.8 | 4781 | 8.2 | |||
| Chronic Disease | N/A | 44,233 | 40,867 | 92.4 | 3366 | 7.6 | <0.0001 | |
| Hypertension | 8775 | 8040 | 91.6 | 735 | 8.4 | |||
| Diabetes | 2543 | 2297 | 90.3 | 246 | 9.7 | |||
| Both | 4779 | 4292 | 89.8 | 487 | 10.2 | |||
| Surgery characteristics | Department | OS (Orthopedic surgery) | 18,694 | 16,883 | 90.3 | 1811 | 9.7 | <0.0001 |
| GS (General surgery) | 10,364 | 9604 | 92.7 | 760 | 7.3 | |||
| OB&GY (Obstetrics & Gynecology) | 7728 | 7427 | 96.1 | 301 | 3.9 | |||
| NS (Neurosurgery) | 3023 | 2706 | 89.5 | 317 | 10.5 | |||
| CS (Thoracic and Cardiovascular Surgery) | 2133 | 1936 | 90.8 | 197 | 9.2 | |||
| PS (Plastic Surgery) | 2216 | 2012 | 90.8 | 204 | 9.2 | |||
| ENT (Ear, Nose & Throat) | 8985 | 8331 | 92.7 | 654 | 7.3 | |||
| EY (Ophthalmology) | 3214 | 3038 | 94.5 | 176 | 5.5 | |||
| UR (Urology) | 3973 | 3559 | 89.6 | 414 | 10.4 | |||
| Type of anesthesia | General anesthesia | 43,638 | 40,387 | 92.6 | 3251 | 7.5 | <0.0001 | |
| Regional anesthesia | 16,692 | 15,109 | 90.5 | 1583 | 9.5 | |||
| Emergency | Emergency | 10,383 | 9962 | 96.0 | 421 | 4.1 | <0.0001 | |
| Planned | 49,947 | 45,534 | 91.2 | 4413 | 8.8 | |||
| Diagnosis | Injury, poisoning and certain other consequences of external causes (S00-T98) | 10,969 | 9851 | 89.8 | 1118 | 10.2 | <0.0001 | |
| Certain infectious and parasitic diseases (A00-B99) | 135 | 114 | 84.4 | 21 | 15.6 | |||
| Neoplasms (C00-D48) | 7457 | 6992 | 93.8 | 465 | 6.2 | |||
| Endocrine, nutritional and metabolic diseases (E00-E90) | 443 | 375 | 84.7 | 68 | 15.4 | |||
| Diseases of the nervous system (G00-G99) | 888 | 785 | 88.4 | 103 | 11.6 | |||
| Diseases of the eye and adnexa (H00-H59) | 2702 | 2587 | 95.7 | 115 | 4.3 | |||
| Diseases of the ear and mastoid process (H60-H95) | 1727 | 1563 | 90.5 | 164 | 9.5 | |||
| Diseases of the circulatory system (I00-I99) | 2553 | 2297 | 90.0 | 256 | 10.0 | |||
| Diseases of the respiratory system (J00-J99) | 5266 | 4929 | 93.6 | 337 | 6.4 | |||
| Diseases of the digestive system (K00-K93) | 7381 | 6841 | 92.7 | 540 | 7.3 | |||
| Diseases of the skin and subcutaneous tissue (L00-L99) | 474 | 422 | 89.0 | 52 | 11.0 | |||
| Diseases of the musculoskeletal system and connective tissue (M00-M99) | 8955 | 8164 | 91.2 | 791 | 8.8 | |||
| Diseases of the genitourinary system (N00-N99) | 5470 | 5049 | 92.3 | 421 | 7.7 | |||
| Pregnancy, childbirth and the puerperium (O00-O99) | 2674 | 2605 | 97.4 | 69 | 2.6 | |||
| Certain conditions originating in the perinatal period (P00-P96) | 56 | 48 | 85.7 | 8 | 14.3 | |||
| Congenital malformations, deformations and chromosomal abnormalities (Q00-Q99) | 1367 | 1219 | 89.2 | 148 | 10.8 | |||
| Symptoms, signs and abnormal clinical and laboratory findings, NEC (R00-R99) | 383 | 294 | 76.8 | 89 | 23.2 | |||
| Surgery schedule characteristics | Year | 2007 | 4694 | 4302 | 91.7 | 392 | 8.4 | 0.4562 |
| 2008 | 5320 | 4891 | 91.9 | 429 | 8.1 | |||
| 2009 | 5227 | 4819 | 92.2 | 408 | 7.8 | |||
| 2010 | 5695 | 5210 | 91.5 | 485 | 8.5 | |||
| 2011 | 6307 | 5826 | 92.4 | 481 | 7.6 | |||
| 2012 | 6483 | 5968 | 92.1 | 515 | 7.9 | |||
| 2013 | 6383 | 5873 | 92.0 | 510 | 8.0 | |||
| 2014 | 6605 | 6040 | 91.5 | 565 | 8.6 | |||
| 2015 | 6573 | 6071 | 92.4 | 502 | 7.6 | |||
| 2016 | 7043 | 6496 | 92.2 | 547 | 7.8 | |||
| Season | spring | 14,467 | 13,345 | 92.2 | 1122 | 7.8 | 0.5001 | |
| Summer | 15,219 | 13,965 | 91.8 | 1254 | 8.2 | |||
| Fall | 14,270 | 13,126 | 92.0 | 1144 | 8.0 | |||
| Winter | 16,374 | 15,060 | 92.0 | 1314 | 8.0 | |||
| Day of week | Mon | 12,003 | 10,909 | 90.9 | 1094 | 9.1 | <0.0001 | |
| Tue | 12,999 | 12,039 | 92.6 | 960 | 7.4 | |||
| Wed | 12,123 | 11,164 | 92.1 | 959 | 7.9 | |||
| Thu | 11,751 | 10,833 | 92.2 | 918 | 7.8 | |||
| Fri | 11,454 | 10,551 | 92.1 | 903 | 7.9 | |||
| Total | 60,330 | 55,496 | 92.0 | 4834 | 8.0 | |||
| Reason | Total | Planned Surgery | Emergency Surgery | ||||
|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | ||
| Patient initiated cancellation | Additional treatment and screening before surgery | 1566 | 32.4 | 1414 | 32 | 152 | 36.1 |
| Patient refused surgery | 1444 | 29.9 | 1351 | 30.6 | 93 | 22.1 | |
| Delay due to personal reason | 950 | 19.7 | 921 | 20.9 | 29 | 6.9 | |
| Incomplete Surgical-work up | 66 | 1.4 | 56 | 1.3 | 10 | 2.4 | |
| Change in medical status | 355 | 7.3 | 280 | 6.3 | 75 | 17.8 | |
| Change in treatment plan | 57 | 1.2 | 44 | 1 | 13 | 3.1 | |
| Others | 67 | 1.4 | 64 | 1.5 | 3 | 0.7 | |
| subtotal | 4505 | 93.2 | 4130 | 93.6 | 375 | 89.1 | |
| Hospital initiated cancellation | Surgeon not available | 65 | 1.3 | 56 | 1.3 | 9 | 2.1 |
| Operation in another place | 7 | 0.1 | 6 | 0.1 | 1 | 0.2 | |
| Schedule error | 23 | 0.5 | 16 | 0.4 | 7 | 1.7 | |
| Lack of beds | 28 | 0.6 | 20 | 0.5 | 8 | 1.9 | |
| Equipment not available | 10 | 0.2 | 7 | 0.2 | 3 | 0.7 | |
| Incomplete Medical evaluation | 161 | 3.3 | 149 | 3.4 | 12 | 2.9 | |
| Others | 35 | 0.7 | 29 | 0.7 | 6 | 1.4 | |
| subtotal | 329 | 6.8 | 283 | 6.4 | 46 | 10.9 | |
| Total | 4834 | 100 | 4413 | 100 | 421 | 100 | |
| Variables | OR | 95% CI | ||
|---|---|---|---|---|
| Sex | Male | 1.00 | ||
| Female | 0.87 | 0.82 | 0.93 | |
| Age | ≤19 | 1.00 | ||
| 20–39 | 0.76 | 0.68 | 0.85 | |
| 40–59 | 0.89 | 0.80 | 0.98 | |
| 60–79 | 1.04 | 0.93 | 1.16 | |
| ≥80 | 1.35 | 1.14 | 1.59 | |
| Admission type | Outpatient/Day surgery clinic | 1.00 | ||
| Inpatient | 2.71 | 2.03 | 3.61 | |
| Chronic Disease | N/A | 1.00 | ||
| Hypertension | 0.90 | 0.82 | 0.99 | |
| Diabetes | 1.13 | 0.98 | 1.30 | |
| Both | 1.10 | 0.98 | 1.22 | |
| Department | OS (Orthopedic surgery) | 1.00 | ||
| GS (General surgery) | 0.90 | 0.82 | 0.99 | |
| OB & GY (Obstetrics & Gynecology) | 0.53 | 0.46 | 0.60 | |
| NS (Neurosurgery) | 1.39 | 1.21 | 1.59 | |
| CS (Thoracic and Cardiovascular Surgery) | 0.98 | 0.84 | 1.15 | |
| PS (Plastic Surgery) | 1.06 | 0.90 | 1.24 | |
| ENT (Ear, Nose & Throat) | 0.75 | 0.68 | 0.84 | |
| EY (Ophthalmology) | 0.66 | 0.56 | 0.79 | |
| UR (Urology) | 1.08 | 0.97 | 1.21 | |
| Type of anesthesia | General anesthesia | 1.00 | ||
| Regional anesthesia | 1.15 | 1.07 | 1.24 | |
| Emergency | Emergency | 1.00 | ||
| Planned | 2.45 | 2.21 | 2.73 | |
| Season | spring | 1.00 | ||
| Summer | 1.08 | 1.00 | 1.18 | |
| Fall | 1.05 | 0.96 | 1.14 | |
| Winter | 1.03 | 0.95 | 1.12 | |
| Day of week | Mon | 1.00 | ||
| Tue | 0.79 | 0.72 | 0.87 | |
| Wed | 0.87 | 0.79 | 0.96 | |
| Thu | 0.86 | 0.79 | 0.95 | |
| Fri | 0.86 | 0.78 | 0.94 | |
| Variables | OR | 95% CI | ||
|---|---|---|---|---|
| Sex | Male | 1.00 | ||
| Female | 0.88 | 0.82 | 0.94 | |
| Age | ≤19 | 1.00 | ||
| 20–39 | 0.76 | 0.68 | 0.85 | |
| 40–59 | 0.86 | 0.77 | 0.96 | |
| 60–79 | 0.98 | 0.87 | 1.10 | |
| ≥80 | 1.20 | 1.00 | 1.45 | |
| Admission type | Outpatient/Day surgery clinic | 1.00 | ||
| Inpatient | 3.24 | 2.37 | 4.44 | |
| Chronic Disease | N/A | 1.00 | ||
| Hypertension | 0.91 | 0.83 | 1.00 | |
| Diabetes | 1.10 | 0.95 | 1.28 | |
| Both | 1.11 | 0.99 | 1.25 | |
| Department | OS (Orthopedic surgery) | 1.00 | ||
| GS (General surgery) | 1.01 | 0.92 | 1.12 | |
| OB & GY (Obstetrics & Gynecology) | 0.53 | 0.46 | 0.61 | |
| NS (Neurosurgery) | 1.63 | 1.41 | 1.89 | |
| CS (Thoracic and Cardiovascular Surgery) | 0.99 | 0.84 | 1.17 | |
| PS (Plastic Surgery) | 0.99 | 0.83 | 1.17 | |
| ENT (Ear, Nose & Throat) | 0.75 | 0.67 | 0.84 | |
| EY (Ophthalmology) | 0.68 | 0.57 | 0.82 | |
| UR (Urology) | 1.08 | 0.96 | 1.22 | |
| Type of anesthesia | General anesthesia | 1.00 | ||
| Regional anesthesia | 1.14 | 1.05 | 1.23 | |
| Season | spring | 1.00 | ||
| Summer | 1.06 | 0.97 | 1.16 | |
| Fall | 1.03 | 0.94 | 1.13 | |
| Winter | 1.01 | 0.92 | 1.10 | |
| Day of week | Mon | 1.00 | ||
| Tue | 0.80 | 0.73 | 0.88 | |
| Wed | 0.90 | 0.82 | 0.99 | |
| Thu | 0.89 | 0.81 | 0.98 | |
| Fri | 0.88 | 0.80 | 0.97 | |
| Variables | OR | 95% CI | ||
|---|---|---|---|---|
| Sex | Male | 1.00 | ||
| Female | 0.85 | 0.68 | 1.06 | |
| Age | ≤19 | 1.00 | ||
| 20–39 | 0.72 | 0.50 | 1.05 | |
| 40–59 | 1.10 | 0.78 | 1.53 | |
| 60–79 | 1.69 | 1.17 | 2.45 | |
| ≥80 | 2.93 | 1.83 | 4.69 | |
| Admission type | Outpatient/Day surgery clinic | 1.00 | ||
| Inpatient | 0.42 | 0.21 | 0.86 | |
| Chronic Disease | N/A | 1.00 | ||
| Hypertension | 0.82 | 0.60 | 1.12 | |
| Diabetes | 1.30 | 0.84 | 2.02 | |
| Both | 0.94 | 0.65 | 1.35 | |
| Department | OS (Orthopedic surgery) | 1.00 | ||
| GS (General surgery) | 0.37 | 0.27 | 0.51 | |
| OB & GY (Obstetrics & Gynecology) | 0.44 | 0.27 | 0.70 | |
| NS (Neurosurgery) | 0.53 | 0.37 | 0.78 | |
| CS (Thoracic and Cardiovascular Surgery) | 0.84 | 0.49 | 1.43 | |
| PS (Plastic Surgery) | 1.40 | 0.92 | 2.14 | |
| ENT (Ear, Nose & Throat) | 0.63 | 0.37 | 1.09 | |
| EY (Ophthalmology) | 0.77 | 0.37 | 1.63 | |
| UR (Urology) | 1.03 | 0.73 | 1.45 | |
| Type of anesthesia | General anesthesia | 1.00 | ||
| Regional anesthesia | 1.23 | 0.95 | 1.59 | |
| Season | spring | 1.00 | ||
| Summer | 1.30 | 0.98 | 1.73 | |
| Fall | 1.21 | 0.90 | 1.63 | |
| Winter | 1.19 | 0.89 | 1.61 | |
| Day of week | Mon | 1.00 | ||
| Tue | 0.76 | 0.57 | 1.01 | |
| Wed | 0.62 | 0.46 | 0.84 | |
| Thu | 0.66 | 0.49 | 0.90 | |
| Fri | 0.65 | 0.48 | 0.88 | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, H.S.; Lee, Y.S.; Lee, S.G.; Kim, J.M.; Kim, T.H. Reasons for Surgery Cancellation in a General Hospital: A 10-year Study. Int. J. Environ. Res. Public Health 2019, 16, 7. https://doi.org/10.3390/ijerph16010007
Cho HS, Lee YS, Lee SG, Kim JM, Kim TH. Reasons for Surgery Cancellation in a General Hospital: A 10-year Study. International Journal of Environmental Research and Public Health. 2019; 16(1):7. https://doi.org/10.3390/ijerph16010007
Chicago/Turabian StyleCho, Hyun Sun, Ye Seol Lee, Sang Gyu Lee, Ji Man Kim, and Tae Hyun Kim. 2019. "Reasons for Surgery Cancellation in a General Hospital: A 10-year Study" International Journal of Environmental Research and Public Health 16, no. 1: 7. https://doi.org/10.3390/ijerph16010007
APA StyleCho, H. S., Lee, Y. S., Lee, S. G., Kim, J. M., & Kim, T. H. (2019). Reasons for Surgery Cancellation in a General Hospital: A 10-year Study. International Journal of Environmental Research and Public Health, 16(1), 7. https://doi.org/10.3390/ijerph16010007