The Evaluation of Professional Divisions of Traditional Chinese Medicine in Taiwan through Patient Visit Records of 2012

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Study Design
2.1. Database
2.2. Research Population
2.3. Data Processing
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Data Availability
References
- Zhao, F.J. Study of palace medical system in Tang dynasty. J. Hebei Univ. Econ. Trade 2008, 8, 89–91. [Google Scholar]
- Park, H.K.; Kim, K.W.; Yi, Y.S. The medical study about the development of pediatrics for Song dynasty. J. Korean Med. Class. 2008, 21, 1–20. [Google Scholar]
- Wu, H.Z.; Cheng, P.J. History and features of development of traditional Chinese medicine education. J. Nanjing Univ. Tradit. Chin. Med. 2000, 1, 186–188. [Google Scholar]
- Zhou, H.Y. Synoptic history of Chinese ancient medical education. Ph.D. Thesis, Heilongjiang University, Harbin, China, 2007. [Google Scholar]
- Lung, Y.M. How is traditional Chinese medicine related surgery during the Song period? Bull. Assoc. Hist. Sci. 2012, 17, 72–78. [Google Scholar]
- Li, J.M. The ignored history of surgery in traditional Chinese medicine. J. Nanjing Univ. Tradit. Chin. Med. 2016, 17, 9–13. [Google Scholar]
- Pi, K.L. What is surgical department? Discussing on the content of the history of surgery in Chinese medicine from “Essences of Surgery” (1263). Taiwan J. Clin. Chin. Med. 2015, 20, 1–18. [Google Scholar]
- Chu, P.Y. “Medicine cures only benign illnesses; the Buddha saves only those with the right karma”: The medical market, medical knowledge and patient-physician relationships in the Ming-Qing period. Bull. Inst. Mod. Hist. Acad. Sin. 2010, 68, 1–50. [Google Scholar]
- Liu, S.L.; Zhou, A.F.; Huang, B.S.; Zeng, W.; Lu, W.L.; Shu, J.S. Successful experience of the first batch of prominent senior TCM specialists and enlightenments to TCM talent training. Educ. Chin. Med. 2010, 1, 007. [Google Scholar]
- Pi, K.L. A study on the medical revolution and medical history during the early republican period—The concept and implementation of “Modern Medical History” by Yu Yan (1879–1954). J. Chin. Med. Spec. Ed. 2013, 1, 159–185. [Google Scholar]
- Zhao, Y.F. Study on the Culture of the Miao Witch Doctor in the Qingshui River Basins from Ming and Qing Dynasty. J. Kaili Univ. 2016, 34, 1–9. [Google Scholar]
- Yen, M.C.; Su, Y.C. Preliminary literature review of traditional Chinese medicine: An example of prescription divination in Taiwan temples. J. Chin. Med. Spec. Ed. 2014, 2, 275–293. [Google Scholar]
- Yang, G.D.; Yang, B.; Yan, Z.L.; Li, Q.; Yu, Y. Application and inheritance of TCM herbal notes of Fuxi. West. J. Tradit. Chin. Med. 2016, 29, 68–71. [Google Scholar]
- Liu, S.Y. The obstacles to develop integration of Chinese-Western medicine in post-war Taiwan: Preliminary study in cases of Du Congming and Yung Sibiao. J. Chin. Med. Spec. Ed. 2013, 1, 111–122. [Google Scholar]
- Hsueh, T.P.; Tsai, M.Y.; Hu, W.L.; Huang, S.T.; Hung, Y.C. Correlation of traditional Chinese medicine licensing examination with performance on internship—Experience of a medical center in Southern Taiwan. J. Chin. Med. 2014, 25, 73–81. [Google Scholar] [CrossRef]
- Yang, C.Y.; Yang, H.I. The difference of medical malpractice disputes between traditional Chinese medicine and western medicine in Taiwan district. J. Chin. Med. 2004, 15, 1–15. [Google Scholar]
- Chi, C.H.; Lee, J.L.; Lai, J.S.; Chen, S.C.; Chen, C.Y.; Chang, S.K. Utilization of Chinese medicine in Taiwan. Altern. Ther. Health Med. 1997, 3, 40–53. [Google Scholar] [PubMed]
- Yu, H.M. The Study of Patients’ Self-Paying Behavior in Seeking Chinese Medical Treatments. Master’s Thesis, National Taiwan University, Taipei, Taiwan, 2007. [Google Scholar]
- Chen, Y.C.; Yeh, H.Y.; Wu, J.C.; Haschler, I.; Chen, T.J.; Wetter, T. Taiwan’s National Health Insurance Research Database: Administrative health care database as study object in bibliometrics. Scientometrics 2011, 86, 365–380. [Google Scholar] [CrossRef]
- Chiang, S.N. Examining Key Factors of Service Quality for Chains of Traditional Chinese Medicine Clinic. Master’s Thesis, Chung Hua University, Hsinchu, Taiwan, 2011. [Google Scholar]
- Chen, F.P.; Chen, T.J.; Kung, Y.Y.; Chen, Y.C.; Chou, L.F.; Chen, F.J.; Hwang, S.J. Use frequency of traditional Chinese medicine in Taiwan. BMC Health Serv. Res. 2007, 7, 26. [Google Scholar] [CrossRef] [PubMed]
- Annual Statistical Report on National Health Insurance for the 101 Year of the Republic of China (Taiwan). Available online: Dep.mohw.gov.tw/DOS/np-1982-113.html (accessed on 6 June 2018).
- Hung, C.T.; Huang, Y.T.; Lee, J.L.; Ho, C.C.; Lee, S.F. Traditional Chinese medicine physician manpower in Taiwan. Taiwan J. Chin. Med. 2009, 8, 1–9. [Google Scholar]
- Wu, S.C.; Chu, H.F.; Haung, L.G.; Lei, H.L. How many physicians per 1000 people do we need in Taiwan an international comparison? Taiwan J. Public Health 2003, 22, 279–286. [Google Scholar] [CrossRef]
- Shih, C.C.; Lin, J.G.; Liao, C.C.; Su, Y.C. The utilization of traditional Chinese medicine and associated factors in Taiwan in 2002. Chin. Med. J. 2009, 122, 1544. [Google Scholar] [CrossRef] [PubMed]
- Shih, C.C.; Liao, C.C.; Su, Y.C.; Tsai, C.C.; Lin, J.G. Gender differences in traditional Chinese medicine use among adults in Taiwan. PLoS ONE 2012, 7, e32540. [Google Scholar] [CrossRef] [PubMed]
- Shih, C.-C. The Study on the Utilization of Traditional Chinese Medicine among People in Taiwan: The Effects of Medical Resources, Sociodemographic Factors and Health Behaviors, in College of Chinese Medicines; National Digital Library of Theses and Dissertations in Taiwan, China Medical University: Taichung, Taiwan, 2011; p. 253. [Google Scholar]
- Huang, H.C.; Chen, Y.F.; Lu, C.N.; Chen, T.Y.; Yang, S.H.; Lin, C.H.; Wu, C.L.; Lee, K.H. Investigation of personnel training and occupational activities in Chinese Traumatology in Taiwan. J. Chin. Med. 2012, 23, 113–132. [Google Scholar]
- Liu, J.K. A Theoretical Analysis of Physician Specialty Choice, In College of Social Sciences. Master’s Thesis, Chinese Culture University, Taipei, Taiwan, 2012. [Google Scholar]
- Lin, M.H.; Chang, H.T.; Tu, C.Y.; Chen, T.J.; Hwang, S.J. Prevalence of polyherbacy in ambulatory visits to traditional Chinese medicine clinics in Taiwan. Int. J. Environ. Res. Public Health 2015, 12, 9639–9657. [Google Scholar] [CrossRef] [PubMed]
- Chang, L.C.; Huang, N.; Chou, Y.J.; Lee, C.H.; Kao, F.Y.; Huang, Y.T. Utilization patterns of Chinese medicine and Western medicine under the National Health Insurance Program in Taiwan, a population-based study from 1997 to 2003. BMC Health Serv. Res. 2008, 8, 170. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.H.; Chang, H.T.; Tu, C.Y.; Chen, T.J.; Hwang, S.J. Doctor-shopping behaviors among traditional Chinese medicine users in Taiwan. Int. J. Environ. Res. Public Health 2015, 12, 9237–9247. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, S.C.; Lai, J.N.; Lee, C.F.; Hu, F.C.; Tseng, W.L.; Wang, J.D. The prescribing of Chinese herbal products in Taiwan: A cross-sectional analysis of the national health insurance reimbursement database. Pharmacoepidemiol. Drug Saf. 2008, 17, 609–619. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.H.; Ang, T.F.A.; Chiang, T.C.; Kaplan, W.A. Growing concerns and controversies to Taiwan’s National Health Insurance—What are the lessons from mainland China, South Korea and Singapore? Int. J. Health Plan. Manag. 2018, 33, e357–e366. [Google Scholar] [CrossRef] [PubMed]
- Hsing, A.W.; Ioannidis, J.P. Nationwide Population Science: Lessons From the Taiwan National Health Insurance Research Database. JAMA Int. Med. 2015, 175, 1527–1529. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
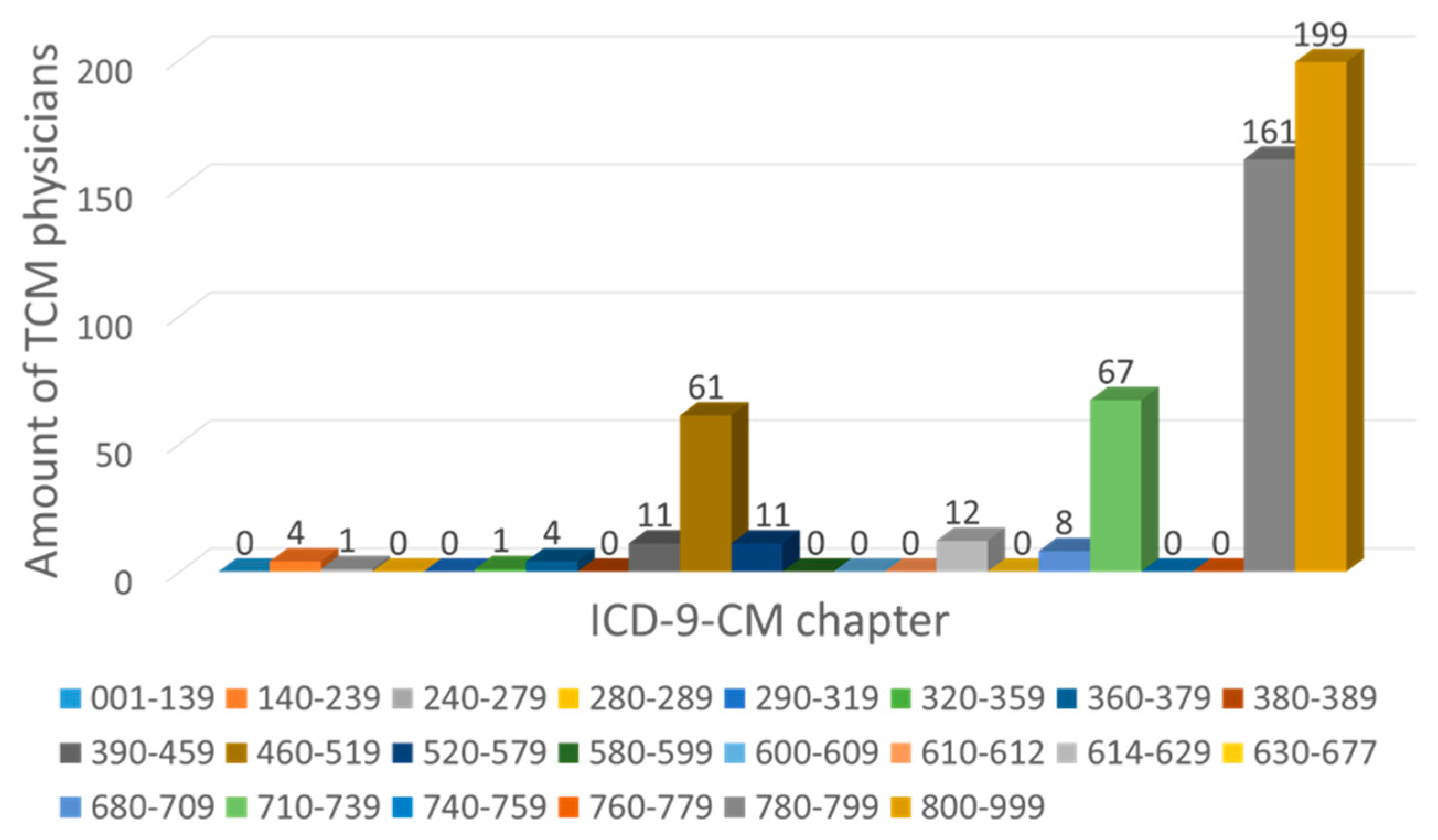
| Range of ICD-9-CM Codes | Description for Each Group |
|---|---|
| 001–139 | Infectious and Parasitic Diseases |
| 140–239 | Neoplasms |
| 240–279 | Endocrine, Nutritional, and Metabolic Diseases and Immunity Disorders |
| 280–289 | Diseases of the Blood and Blood-forming Organs |
| 290–319 | Mental Disorders |
| 320–359 | Disorders of the Nervous System |
| 360–379 | Disorders of the Eye And Adnexa |
| 380–389 | Diseases of the Ear And Mastoid Process |
| 390–459 | Diseases of the Circulatory System |
| 460–519 | Diseases of the Respitory System |
| 520–579 | Diseases of the Digestive System |
| 580–599 | Diseases of Urinary System |
| 600–609 | Diseases of Male Genital Organs |
| 610–612 | Disorders of Breast |
| 614–629 | Diseases of Female Genital Organs |
| 630–677 | Complications of Pregnancy, Child Birth, and the Puerperium |
| 680–709 | Diseases of the Skin and Subcutaneous Tissue |
| 710–739 | Diseases of the Musculoskeletal System and Connective Tissue |
| 740–759 | Congenital Abnormalities |
| 760–779 | Certain Conditions Originating in the Perinatal Period |
| 780–799 | Symptoms, Signs and Ill-defined Conditions |
| 800–999 | Injury and Poisoning |
| V01–V82 | Supplementary Classification of External Causes of Injury and Poisoning |
| E800–E999 | Supplementary Classification of Factors Influencing Health Status and Contact with Health Services |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, T.-P.; Tsai, C.-H.; Su, Y.-T.; Wang, C.-C.; Chen, T.-J.; Chang, C.-M.; Chen, F.-P. The Evaluation of Professional Divisions of Traditional Chinese Medicine in Taiwan through Patient Visit Records of 2012. Int. J. Environ. Res. Public Health 2018, 15, 1992. https://doi.org/10.3390/ijerph15091992
Wu T-P, Tsai C-H, Su Y-T, Wang C-C, Chen T-J, Chang C-M, Chen F-P. The Evaluation of Professional Divisions of Traditional Chinese Medicine in Taiwan through Patient Visit Records of 2012. International Journal of Environmental Research and Public Health. 2018; 15(9):1992. https://doi.org/10.3390/ijerph15091992
Chicago/Turabian StyleWu, Ta-Peng, Cheng-Hung Tsai, Yu-Ting Su, Chu-Chiao Wang, Tzeng-Ji Chen, Ching-Mao Chang, and Fang-Pey Chen. 2018. "The Evaluation of Professional Divisions of Traditional Chinese Medicine in Taiwan through Patient Visit Records of 2012" International Journal of Environmental Research and Public Health 15, no. 9: 1992. https://doi.org/10.3390/ijerph15091992
APA StyleWu, T.-P., Tsai, C.-H., Su, Y.-T., Wang, C.-C., Chen, T.-J., Chang, C.-M., & Chen, F.-P. (2018). The Evaluation of Professional Divisions of Traditional Chinese Medicine in Taiwan through Patient Visit Records of 2012. International Journal of Environmental Research and Public Health, 15(9), 1992. https://doi.org/10.3390/ijerph15091992