Disability and Its Influencing Factors among the Elderly in a County, Guangxi Province, China

Abstract
1. Introduction
2. Methods
2.1. Study Population
2.2. Activities of Daily Living (ADL) Scale
2.3. Metabolic Syndrome (MetS) Criterion
2.4. Statistical Analysis
3. Results
3.1. Demographic Characteristics
3.2. Disability Rates of ADL, PADL, and IADL in the Elderly People with Different Characteristics
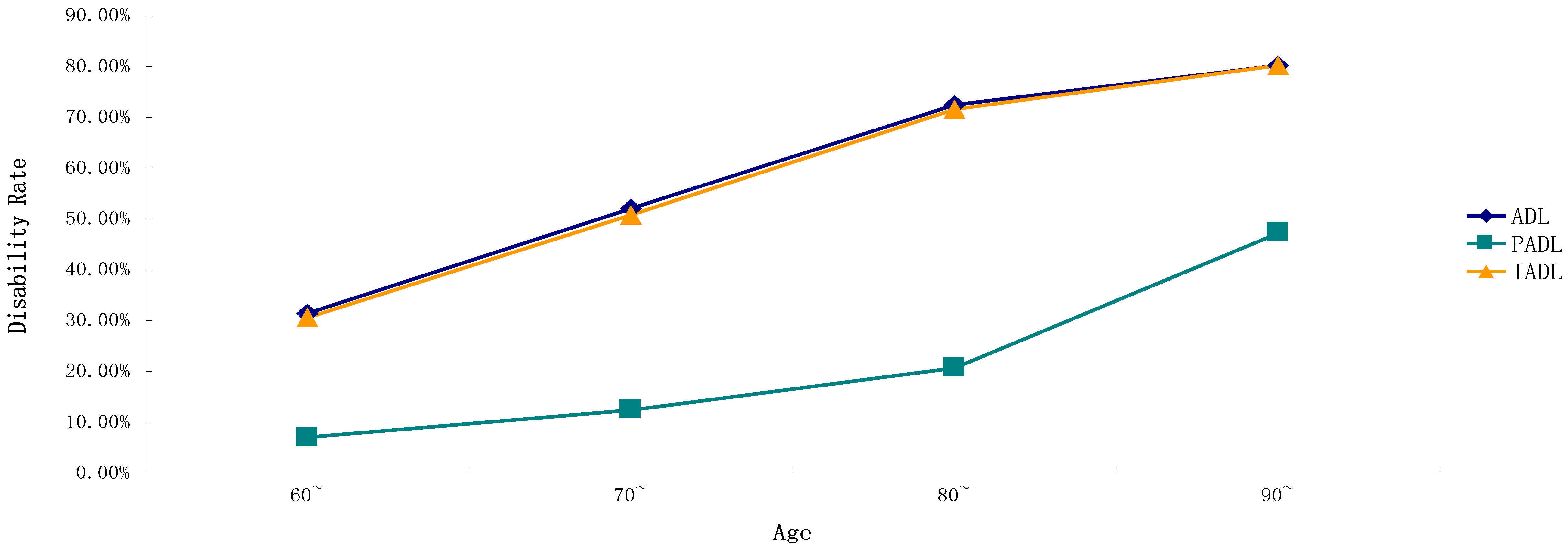
3.3. Trends of Disability Rates among Different Ages in ADL, PADL, IADL, and Their Items
3.4. Binary Logistic Analysis of the Influencing Factors of ADL, PADL, IADL, and 14 Items in the Elderly
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Ethical Approval and Consent to Participate
References
- Guangxi Is at Top of the “71 Longest-Living Cities in China” List. Available online: http://news.gxnews.com.cn/staticpages/20150909/newgx55ef64a8-13537163.shtml (accessed on 15 August 2018).
- Wang, S.; Luo, K.; Liu, Y. Spatio-temporal distribution of human lifespan in China. Sci. Rep. 2015, 5, 13844. [Google Scholar] [CrossRef] [PubMed]
- The Start of the “2016 Top National Internet Media into Hechi-Home of the Long-Livings” Event. Available online: http://news.163.com/16/1128/13/C6VB40GH000187VE.html (accessed on 15 August 2018).
- Qin, J.; Yu, G.; Xia, T.; Li, Y.; Liang, X.; Wei, P.; Long, B.; Lei, M.; Wei, X.; Tang, X.; et al. Spatio-Temporal Variation of Longevity Clusters and the Influence of Social Development Level on Lifespan in a Chinese Longevous Area (1982–2010). Int. J. Environ. Res. Public Health 2017, 14, 812. [Google Scholar] [CrossRef] [PubMed]
- Fong, J.H.; Feng, J. Comparing the loss of functional independence of older adults in the U.S. and China. Arch. Gerontol. Geriatr. 2018, 74, 123–127. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Li, Z.; Tang, Z.; Sun, F.; Diao, L.; Li, J.; He, Y.; Dong, B.; Li, Y. Prevalence and socio-demographic characteristics of disability in older adults in China: Findings from China Comprehensive Geriatric Assessment Study. Arch. Gerontol. Geriatr. 2017, 73, 199–203. [Google Scholar] [CrossRef] [PubMed]
- Zhai, Z.; Li, L. The megatrends, new features and corresponding pension policies of China’s aging population. J. Shandong Univ. 2016, 3, 27–35. [Google Scholar]
- Fang, Y.; Mao, W.; Gao, R.; Su, P.Y. Analysis of the old-age endowment model in rural China. Chin. J. Gerontol. 2012, 4, 881–883. [Google Scholar]
- Dai, B.Z.; Zhou, L.L.; Mei, Y.J. Old age security in rural China: There is a long way to go. Chin. Med. J. 2013, 126, 4348–4853. [Google Scholar] [PubMed]
- Hodgkin, S.P.; Warburton, J.; Hancock, S. Predicting wellness among rural older Australians: A cross-sectional study. Rural Remote Health 2018, 18, 4547. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Guralnik, J.M. Disability in older adults: Evidence regarding significance, etiology, and risk. J. Am. Geriatr. Soc. 1997, 45, 92–100. [Google Scholar] [CrossRef] [PubMed]
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Downer, B.; Chen, N.W.; Wong, R.; Markides, K.S. Self-Reported Health and Functional Characteristics of Mexican and Mexican American Adults Aged 80 and over. J. Aging Health 2016, 28, 1239–1255. [Google Scholar] [CrossRef] [PubMed]
- Lima-Costa, M.F.; Mambrini, J.V.; Peixoto, S.V.; Malta, D.C.; Macinko, J. Socioeconomic inequalities in activities of daily living limitations and in the provision of informal and formal care for noninstitutionalized older Brazilians: National Health Survey, 2013. Int. J. Equity Health 2016, 15, 137. [Google Scholar] [CrossRef] [PubMed]
- Yin, D. The comparing study on individual factors about elder’s ability of caring for themselves. J. Beijing Adm. Coll. 2007, 1, 86. [Google Scholar]
- Chen, C. Geriatric Nursing; Tsinghua University Press: Beijing, China, 2011. [Google Scholar]
- Huang, W.; Ge, X.; Hou, S.; Gao, G.; Zhang, X.; Yu, Y. Ability of daily living and its influencing factors among rural elderly in Dabieshan Mountain area. Chin. J. Public Health 2012, 7, 884–886. [Google Scholar]
- Penninx, B.W.; Nicklas, B.J.; Newman, A.B.; Harris, T.B.; Goodpaster, B.H.; Satterfield, S.; de Rekeneire, N.; Yaffe, K.; Pahor, M.; Kritchevsky, S.B.; et al. Metabolic syndrome and physical decline in older persons: Results from the Health, Aging and Body Composition Study. J. Gerontol. 2009, 64, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.H.; Lu, J.M.; Wang, S.Y.; Li, C.L.; Liu, L.S.; Zheng, R.P.; Pan, C.Y. Comparison of the diagnostic criteria of metabolic syndrome by International Diabetes Federation and that by Chinese Medical Association Diabetes Branch. Chin. Med. J. 2006, 86, 386–389. [Google Scholar]
- Suzuki, T. Health status of older adults living in the community in Japan: Recent changes and significance in the super-aged society. Geriatr. Gerontol. Int. 2018, 18, 667–677. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, S.L.; Silverstein, M. Observing the onset of disability in older adults. Soc. Sci. Med. 2003, 57, 1875–1889. [Google Scholar] [CrossRef]
- Shimada, H.; Makizako, H.; Lee, S.; Doi, T.; Tsutsumimoto, K.; Harada, K.; Suzuki, T. Impact of Cognitive Frailty on Daily Activities in Older Persons. J. Nutr. Health Aging 2016, 20, 729–735. [Google Scholar] [CrossRef] [PubMed]
- Zhong, Y.Q.; Wang, J.; Zhang, G.J. Analysis on ability of daily living and its influence factors among the elderly. Mod. Prev. Med. 2014, 41, 852–855. [Google Scholar]
- Jing, R.; Li, X.Y.; Yang, S.X. The activity of daily living of rural elderly population in Shandong province and the research of in fluencing factors. Mod. Prev. Med. 2009, 36, 513–515. [Google Scholar]
- Gjonca, E.; Tabassum, F.; Breeze, E. Socioeconomic differences in physical disability at older age. J. Epidemiol. Community Health 2009, 63, 928–935. [Google Scholar] [CrossRef] [PubMed]
- Hoogendijk, E.O.; van der Horst, H.E.; Deeg, D.J.; Frijters, D.H.; Prins, B.A.; Jansen, A.P.; Nijpels, G.; van Hout, H.P. The identification of frail older adults in primary care: Comparing the accuracy of five simple instruments. Age Ageing 2013, 42, 262–265. [Google Scholar] [CrossRef] [PubMed]
- Millan-Calenti, J.C.; Tubio, J.; Pita-Fernandez, S.; Gonzalez-Abraldes, I.; Lorenzo, T.; Fernandez-Arruty, T.; Maseda, A. Prevalence of functional disability in activities of daily living (ADL), instrumental activities of daily living (IADL) and associated factors, as predictors of morbidity and mortality. Arch. Gerontol. Geriatr. 2010, 50, 306–310. [Google Scholar] [CrossRef] [PubMed]
- Deeg, D.J.H.; Huisman, M.; Terwee, C.B.; Comijs, H.C.; Thomese, G.C.F.; Visser, M. Changes in Functional Ability with Ageing and over Time. In Aging in European Societies; Springer: Boston, MA, USA, 2013; pp. 117–132. [Google Scholar]
- Chalise, H.N.; Saito, T.; Kai, I. Functional disability in activities of daily living and instrumental activities of daily living among Nepalese Newar elderly. Public Health 2008, 122, 394–396. [Google Scholar] [CrossRef] [PubMed]
- Wheaton, F.V.; Crimmins, E.M. Female disability disadvantage: A global perspective on sex differences in physical function and disability. Ageing Soc. 2016, 36, 1136–1156. [Google Scholar] [CrossRef] [PubMed]
- Tomioka, K.; Kurumatani, N.; Hosoi, H. Association between Social Participation and Instrumental Activities of Daily Living among Community-Dwelling Older Adults. J. Epidemiol. 2016, 26, 553–561. [Google Scholar] [CrossRef] [PubMed]
- Fried, T.R.; Bradley, E.H.; Williams, C.S.; Tinetti, M.E. Functional disability and health care expenditures for older persons. Arch. Intern. Med. 2001, 161, 2602–2607. [Google Scholar] [CrossRef] [PubMed]
- Luppa, M.; Luck, T.; Weyerer, S.; Konig, H.H.; Brahler, E.; Riedel-Heller, S.G. Prediction of institutionalization in the elderly: A systematic review. Age Ageing 2010, 39, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Brown, R.T.; Diaz-Ramirez, L.G.; Boscardin, W.J.; Lee, S.J.; Steinman, M.A. Functional Impairment and Decline in Middle Age: A Cohort Study. Ann. Intern. Med. 2017, 167, 761–768. [Google Scholar] [CrossRef] [PubMed]
- Salomon, J.A.; Wang, H.; Freeman, M.K.; Vos, T.; Flaxman, A.D.; Lopez, A.D.; Murray, C.J.L. Healthy life expectancy for 187 countries, 1990–2010: A systematic analysis for the Global Burden Disease Study 2010. Lancet 2012, 380, 2144–2162. [Google Scholar] [CrossRef]
- Shinkai, S.; Watanabe, S.; Kumagai, S.; Fujiwara, Y.; Amano, H.; Yoshida, H.; Shibata, H. Walking speed as a good predictor for the onset of functional dependence in a Japanese rural community population. Age Ageing 2000, 29, 441–446. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Fang, Y.; Mao, F.; Hao, S.; Chen, J.; Yuan, M.; Hong, Y.A. Assessment of Disability among the Elderly in Xiamen of China: A Representative Sample Survey of 14,292 Older Adults. PLoS ONE 2015, 10, e0131014. [Google Scholar] [CrossRef] [PubMed]
- Coppin, A.K.; Ferrucci, L.; Lauretani, F.; Phillips, C.; Chang, M.; Bandinelli, S.; Guralnik, J.M. Low Socioeconomic Status and Disability in Old Age: Evidence From the InChianti Study for the Mediating Role of Physiological Impairments. J. Gerontol. 2006, 61, 86–91. [Google Scholar] [CrossRef]
- Keddie, A.M.; Peek, M.K.; Markides, K.S. Variation in the associations of education, occupation, income, and assets with functional limitations in older Mexican Americans. Ann. Epidemiol. 2005, 15, 579–589. [Google Scholar] [CrossRef] [PubMed]
- Guerra, R.O.; Alvarado, B.E.; Zunzunegui, M.V. Life course, gender and ethnic inequalities in functional disability in a Brazilian urban elderly population. Aging Clin. Exp. Res. 2008, 20, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Ronksley, P.E.; Brien, S.E.; Turner, B.J.; Mukamal, K.J.; Ghali, W.A. Association of alcohol consumption with selected cardiovascular disease outcomes: A systematic review and meta-analysis. BMJ 2011, 342, d671. [Google Scholar] [CrossRef] [PubMed]
- Cabral, D.A.; da Costa, K.G.; Okano, A.H.; Elsangedy, H.M.; Rachetti, V.P.; Fontes, E.B. Improving cerebral oxygenation, cognition and autonomic nervous system control of a chronic alcohol abuser through a three-month running program. Addict. Behav. Rep. 2017, 6, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Stampfer, M.J.; Kang, J.H.; Chen, J.; Cherry, R.; Grodstein, F. Effects of moderate alcohol consumption on cognitive function in women. N. Engl. J. Med. 2005, 352, 245–253. [Google Scholar] [CrossRef] [PubMed]
- Britton, A.; Singh-Manoux, A.; Marmot, M. Alcohol consumption and cognitive function in the Whitehall II Study. Am. J. Epidemiol. 2004, 160, 240–247. [Google Scholar] [CrossRef] [PubMed]
- Neafsey, E.J.; Collins, M.A. Moderate alcohol consumption and cognitive risk. Neuropsychiatr. Dis. Treat. 2011, 7, 465–484. [Google Scholar] [CrossRef] [PubMed]
- Gijsen, R.; Hoeymans, N.; Schellevis, F.G.; Ruwaard, D.; Satariano, W.A.; van den Bos, G.A. Causes and consequences of comorbidity: A review. J. Clin. Epidemiol. 2001, 54, 661–674. [Google Scholar] [CrossRef]
- Ralph, N.L.; Mielenz, T.J.; Parton, H.; Flatley, A.M.; Thorpe, L.E. Multiple chronic conditions and limitations in activities of daily living in a community-based sample of older adults in New York City, 2009. Prev. Chronic Dis. 2013, 10, E199. [Google Scholar] [CrossRef] [PubMed]
- Tinetti, M.E.; McAvay, G.J.; Chang, S.S.; Newman, A.B.; Fitzpatrick, A.L.; Fried, T.R.; Peduzzi, P.N. Contribution of multiple chronic conditions to universal health outcomes. J. Am. Geriatr. Soc. 2011, 59, 1686–1691. [Google Scholar] [CrossRef] [PubMed]
- Uddin, M.J.; Alam, N.; Sarma, H.; Chowdhury, M.A.H.; Alam, D.S.; Niessen, L. Consequences of hypertension and chronic obstructive pulmonary disease, healthcare-seeking behaviors of patients, and responses of the health system: A population-based cross-sectional study in Bangladesh. BMC Public Health 2014, 14, 547. [Google Scholar]
- Dunlop, D.D.; Manheim, L.M.; Sohn, M.W.; Liu, X.; Chang, R.W. Incidence of functional limitation in older adults: The impact of gender, race, and chronic conditions. Arch. Phys. Med. Rehabil. 2002, 83, 964–971. [Google Scholar] [CrossRef] [PubMed]
- He, W.; Larsen, L.J. (Eds.) USCB: Older Americans with a Disability: 2008–2012; American Community Survey Reports, ACS-29; Government Printing Office: Washington, DC, USA, 2014.
- Remillard, E.T.; Fausset, C.B.; Fain, W.B. Aging with Long-Term Mobility Impairment: Maintaining Activities of Daily Living via Selection, Optimization, and Compensation. Gerontologist 2017. [Google Scholar] [CrossRef] [PubMed]
- Roriz-Cruz, M.; Rosset, I.; Wada, T.; Sakagami, T.; Ishine, M.; Roriz-Filho, J.S.; Cruz, T.R.; Rodrigues, R.P.; Resmini, I.; Sudoh, S.; et al. Stroke-independent association between metabolic syndrome and functional dependence, depression, and low quality of life in elderly community-dwelling Brazilian people. J. Am. Geriatr. Soc. 2007, 55, 374–382. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Xu, H.; Yang, L.; Jiang, J.; Dong, B. Metabolic syndrome and disability in Chinese nonagenarians and centenarians. Aging Clin. Exp. Res. 2017, 30, 913–949. [Google Scholar] [CrossRef]
- Lee, J.S.W.; Auyeung, T.W.; Leung, J.; Kwok, T.; Leung, P.C.; Woo, J. Physical Frailty in Older Adults is Associated with Metabolic and Atherosclerotic Risk Factors and Cognitive Impairment Independent of Muscle Mass. J. Nutr. Health Aging 2011, 15, 857–862. [Google Scholar] [CrossRef] [PubMed]
- Blaum, C.S.; West, N.A.; Haan, M.N. Is the Metabolic Syndrome, with or without Diabetes, Associated with Progressive Disability in Older Mexican Americans? J. Gerontol. Med. Sci. 2007, 62, 766–773. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Item | All Participants (n,%) | ADL (n = 998) | PADL (n = 266) | IADL (n = 976) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Impairment (n,%) | χ2 | p Value | Impairment (n,%) | χ2 | p Value | Impairment (n,%) | χ2 | p Value | ||
| Gender | 160.392 | <0.001 | 0.416 | 0.519 | 167.684 | <0.001 | ||||
| Male | 950 (41.3%) | 264 (27.8%) | 105 (11.1%) | 252 (26.5%) | ||||||
| Female | 1350 (58.7%) | 734 (54.4%) | 161 (11.9%) | 724 (53.6%) | ||||||
| Age | 195.903 | <0.001 | 165.98 | <0.001 | 196.725 | <0.001 | ||||
| 60~ | 1223 (53.2%) | 384 (31.4%) | 86 (7.0%) | 374 (30.6%) | ||||||
| 70~ | 855 (37.2%) | 445 (52.0%) | 106 (12.4%) | 434 (50.8%) | ||||||
| 80~ | 116 (5.0%) | 84 (72.4%) | 24 (20.7%) | 83 (71.6%) | ||||||
| 90~ | 106 (4.6%) | 85 (80.2%) | 50 (47.2%) | 85 (80.2%) | ||||||
| Ethnic | 0.898 | 0.638 | 5.467 | 0.065 | 1.874 | 0.392 | ||||
| Han | 317 (13.8%) | 134 (42.3%) | 49 (15.5%) | 127 (40.1%) | ||||||
| Zhuang | 1869 (81.3%) | 810 (43.3%) | 205 (11.0%) | 795 (42.5%) | ||||||
| Others | 114 (5.0%) | 54 (47.4%) | 12 (10.5%) | 54 (47.4%) | ||||||
| Occupation | 31.777 | <0.001 | 2.22 | 0.136 | 31.073 | <0.001 | ||||
| Farmer | 2147 (93.3%) | 965 (44.9%) | 254 (11.8%) | 944 (44.0%) | ||||||
| Others | 153 (6.7%) | 33 (21.6%) | 12 (7.8%) | 32 (20.9%) | ||||||
| Marital status | 77.550 | <0.001 | 25.15 | <0.001 | 81.273 | <0.001 | ||||
| Divorced/Widowed | 736 (32.0%) | 417 (56.7%) | 121 (16.4%) | 412 (56.0%) | ||||||
| Married | 1564 (68.0%) | 581 (37.1%) | 145 (9.3%) | 564 (36.1%) | ||||||
| Level of education | 223.042 | <0.001 | 5.826 | 0.054 | 236.274 | <0.001 | ||||
| Literacy | 1038 (41.3%) | 612 (59.0%) | 134 (12.9%) | 605 (58.3%) | ||||||
| Primary school | 797 (34.7%) | 295 (37.0%) | 92 (11.5%) | 289 (36.3%) | ||||||
| Junior high school and above | 465 (20.2%) | 91 (19.6%) | 40 (8.6%) | 82 (17.6%) | ||||||
| Current smoking | 65.144 | <0.001 | 0.288 | 0.295 | 66.161 | <0.001 | ||||
| Without | 1917 (83.3%) | 904 (47.2%) | 228 (11.9%) | 886 (46.2%) | ||||||
| With | 381 (16.7%) | 94 (24.7%) | 38 (10.0%) | 90 (23.6%) | ||||||
| Alcohol use | 66.522 | <0.001 | 3.481 | 0.062 | 69.965 | <0.001 | ||||
| Without | 1763 (76.7%) | 847 (48.0%) | 216 (12.3%) | 832 (47.2%) | ||||||
| With | 537 (23.3%) | 151 (28.1%) | 50 (9.3%) | 144 (26.8%) | ||||||
| Chronic conditions | 3.322 | 0.345 | 35.134 | <0.001 | 2.975 | 0.396 | ||||
| 0 | 788 (34.3%) | 340 (43.1%) | 55 (7.0%) | 337 (42.8%) | ||||||
| 1 | 995 (43.3%) | 449 (45.1%) | 120 (12.1%) | 436 (43.8%) | ||||||
| 2 | 390 (17.0%) | 160 (41.0%) | 67 (17.2%) | 154 (39.5%) | ||||||
| 3 | 127 (5.5%) | 49 (38.6%) | 24 (18.9%) | 49 (38.6%) | ||||||
| Metabolic Syndrome | 8.000 | 0.005 | 17.352 | <0.001 | 6.002 | 0.014 | ||||
| Without | 1764 (76.7%) | 737 (41.8%) | 177 (10.0%) | 724 (41.0%) | ||||||
| With | 536 (23.3%) | 261 (48.7%) | 89 (16.6%) | 252 (47.0%) | ||||||
| Item | Total | 60~ | 70~ | 80~ | ≥90 | χ2 | p Value |
|---|---|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | n (%) | |||
| ADL | 998 (43.4%) | 384 (31.4%) | 445 (52.0%) | 84 (72.4%) | 85 (80.2%) | 191.989 | <0.001 |
| PADL | 266 (11.6%) | 86 (7.0%) | 106 (12.4%) | 24 (20.7%) | 50 (47.2%) | 138.334 | <0.001 |
| IADL | 976 (42.4%) | 374 (30.6%) | 434 (50.8%) | 83 (71.6%) | 85 (80.2%) | 193.711 | <0.001 |
| Walking | 224 (9.7%) | 73 (6.0%) | 89 (10.4%) | 19 (16.4%) | 43 (40.6%) | 114.135 | <0.001 |
| Eating | 59 (2.6%) | 8 (0.7%) | 18 (30.6%) | 6 (5.2%) | 27 (25.5%) | 158.834 | <0.001 |
| Dressing | 70 (3.0%) | 12 (1.0%) | 22 (2.6%) | 6 (5.2%) | 30 (28.3%) | 158.023 | <0.001 |
| Grooming | 69 (3.0%) | 13 (1.1%) | 19 (2.2%) | 7 (6.0%) | 30 (28.3%) | 76.049 | <0.001 |
| Bathing | 142 (6.2%) | 38 (3.1%) | 50 (5.8%) | 13 (11.5%) | 41 (44.4%) | 153.701 | <0.001 |
| Toileting | 102 (4.4%) | 26 (2.1%) | 33 (3.9%) | 10 (8.6%) | 33 (31.1%) | 134.112 | <0.001 |
| Using the telephone | 599 (26.0%) | 191 (15.6%) | 275 (32.2%) | 62 (53.4%) | 71 (67.0%) | 222.151 | <0.001 |
| Financial management | 275 (12.0%) | 72 (5.9%) | 108 (12.6%) | 38 (32.8%) | 57 (53.8%) | 234.731 | <0.001 |
| Using public vehicles | 712 (31.0%) | 266 (21.7%) | 316 (37.0%) | 62 (53.4%) | 68 (64.2%) | 144.48 | <0.001 |
| Preparing a meal | 216 (9.4%) | 48 (3.9%) | 81 (9.5%) | 28 (24.1%) | 59 (55.7%) | 275.191 | <0.001 |
| Performing household tasks | 157 (6.8%) | 32 (2.6%) | 47 (5.5%) | 20 (17.2%) | 58 (54.7%) | 302.783 | <0.001 |
| Taking medication | 122 (5.3%) | 26 (2.1%) | 52 (6.1%) | 13 (11.2%) | 31 (29.2%) | 130.917 | <0.001 |
| Doing some washing | 195 (8.5%) | 54 (4.4%) | 61 (7.1%) | 24 (20.7%) | 57 (53.8%) | 232.805 | <0.001 |
| Grocery shopping | 272 (11.8%) | 64 (5.2%) | 107 (12.5%) | 38 (32.8%) | 63 (59.4%) | 287.099 | <0.001 |
| Item | Gender | Age | Marital Status | ||
| Female = Reference | 60~ = Reference | Married = Reference | |||
| Male OR (95%CI) | 70~OR (95%CI) | 80~OR (95%CI) | 90~OR (95%CI) | NO Married OR (95%CI) | |
| ADL | 0.579 (0.441–0.759) | 2.270 (1.867–2.759) | 4.719 (2.998–7.429) | 6.249 (3.667–10.648) | 1.193 (0.971–1.464) |
| PADL | 1.267 (0.853–1.882) | 1.815 (1.328–2.480) | 3.864 (2.251–6.634) | 17.948 (10.464–30.786) | 1.065 (0.780–1.455) |
| IADL | 0.573 (0.436–0.753) | 2.221 (1.825–2.703) | 4.626 (2.945–7.266) | 6.356 (3.726–10.843) | 1.212 (0.987–1.489) |
| Walking | 1.094 (0.714–1.676) | 1.813 (1.296–2.537) | 3.602 (2.001–6.485) | 17.407 (9.909–30.578) | 0.955 (0.681–1.339) |
| Eating | 2.488 (1.147–5.397) | 2.811 (1.193–6.623) | 7.207 (2.318–22.406) | 47.160 (17.762–125.216) | 1.445 (0.732–2.852) |
| Dressing | 2.235 (1.096–4.557) | 2.313 (1.119–4.780) | 4.733 (1.658–13.513) | 39.150 (16.154–90.096) | 1.321 (0.712–2.448) |
| Grooming | 2.466 (1.206–5.045) | 1.857 (0.896–3.849) | 5.334 (1.970–14.443) | 37.118 (15.777–87.327) | 1.246 (0.664–2.340) |
| Bathing | 1.652 (0.982–2.779) | 1.773 (1.134–2.772) | 4.107 (2.019–8.355) | 25.002 (13.240–47.212) | 1.159 (0.758–1.772) |
| Toileting | 1.686 (0.926–3.070) | 1.782 (1.040–3.053) | 4.520 (2.015–10.140) | 24.885 (12.229–50.638) | 1.282 (0.779–2.112) |
| Using the telephone | 0.726 (0.527–1.001) | 2.362 (1.884–2.962) | 4.550 (2.958–6.999) | 6.597 (4.069–10.695) | 1.263 (1.007–1.584) |
| Financial management | 1.297 (0.854–1.968) | 1.936 (1.401–2.676) | 5.095 (3.135–8.280) | 9.631 (5.821–15.936) | 1.711 (1.267–2.312) |
| Using public vehicles | 0.444 (0.329–0.599) | 2.037 (1.655–2.508) | 3.473 (2.280–5.290) | 4.802 (3.008–7.665) | 1.110 (0.896–1.374) |
| Preparing a meal | 1.766 (1.130–2.761) | 2.392 (1.630–3.509) | 8.393 (4.772–14.762) | 41.319 (22.916–74.499) | 1.067 (0.746–1.525) |
| Performing household tasks | 1.776 (1.059–2.980) | 2.054 (1.278–3.300) | 8.208 (4.275–15.761) | 54.054 (28.304–103.231) | 1.231 (0.801–1.891) |
| Taking medication | 1.739 (1.002–3.020) | 2.681 (1.637–4.391) | 5.267 (2.508–11.062) | 19.318 (9.774–38.181) | 1.292 (0.832–2.006) |
| Doing some washing | 1.452 (0.914–2.308) | 1.470 (0.996–2.170) | 5.071 (2.882–8.920) | 23.393 (13.342–41.016) | 1.235 (0.856–1.784) |
| Grocery shopping | 1.173 (0.774–1.780) | 2.319 (1.660–3.241) | 7.674 (4.651–12.664) | 25.275 (14.722–43.392) | 1.281 (0.939–1.748) |
| Item | Education Level | Smoking | Alcohol Use | ||
| High = Reference | Without Smoking = Reference | Without Alcohol Use = Reference | |||
| Low OR (95%CI) | Average OR (95%CI) | With Smoking OR (95%CI) | With Alcohol use OR (95%CI) | ||
| ADL | 2.844 (2.076–3.897) | 1.667 (1.246–2.230) | 0.835 (0.610–1.143) | 0.847 (0.648–1.107) | |
| PADL | 1.154 (0.714–1.868) | 1.310 (0.857–2.001) | 0.983 (0.628–1.539) | 0.724 (0.486–1.078) | |
| IADL | 3.116 (2.260–4.297) | 1.834 (1.360–2.472) | 0.849 (0.617–1.168) | 0.834 (0.636–1.094) | |
| Walking | 1.088 (0.650–1.821) | 1.204 (0.762–1.903) | 0.870 (0.530–1.429) | 0.810 (0.527–1.244) | |
| Eating | 1.822 (0.582–5.700) | 2.300 (0.807–6.557) | 1.336 (0.554–3.221) | 0.395 (0.164–0.953) | |
| Dressing | 1.899 (0.669–5.391) | 2.375 (0.914–6.170) | 1.163 (0.510–2.656) | 0.450 (0.203–1.000) | |
| Grooming | 1.896 (0.663–5.421) | 2.486 (0.954–6.476) | 0.978 (0.419–2.284) | 0.463 (0.208–1.030) | |
| Bathing | 1.441 (0.735–2.826) | 1.549 (0.849–2.825) | 1.073 (0.588–1.959) | 0.520 (0.297–0.908) | |
| Toileting | 0.900 (0.416–1.945) | 1.270 (0.655–2.463) | 1.027 (0.525–2.008) | 0.605 (0.326–1.122) | |
| Using the telephone | 4.422 (2.880–6.791) | 2.054 (1.354–3.117) | 0.827 (0.549–1.245) | 0.686 (0.489–0.961) | |
| Financial management | 2.593 (1.515–4.441) | 1.341 (0.799–2.252) | 0.878 (0.529–1.458) | 0.714 (0.461–1.105) | |
| Using public vehicles | 2.738 (1.661–3.404) | 1.631 (1.159–2.296) | 1.112 (0.775–1.595) | 0.780 (0.576–1.056) | |
| Preparing a meal | 1.748 (0.974–3.137) | 1.649 (0.972–2.796) | 0.896 (0.527–1.524) | 0.537 (0.333–0.865) | |
| Performing household tasks | 1.052 (0.530–2.090) | 1.407 (0.767–2.580) | 0.735 (0.387–1.398) | 0.491 (0.278–0.866) | |
| Taking medication | 1.666 (0.821–3.381) | 1.333 (0.696–2.552) | 0.998 (0.528–1.887) | 0.656 (0.369–1.168) | |
| Doing some washing | 2.113 (1.115–4.005) | 2.273 (1.265–4.087) | 1.017 (0.586–1.764) | 0.598 (0.364–0.982) | |
| Grocery shopping | 1.915 (1.114–3.293) | 1.463 (0.880–2.433) | 0.891 (0.528–1.504) | 0.517 (0.325–0.820) | |
| Item | Number of Chronic Conditions | Metabolic Syndrome | |||
| 0 = Reference | Without Mets = Reference | ||||
| 1 OR (95%CI) | ≥2 OR (95%CI) | With Mets OR (95%CI) | |||
| ADL | 1.208 (0.980–1.490) | 1.066 (0.830–1.369) | 1.298 (1.044–1.613) | ||
| PADL | 2.625 (1.800–3.828) | 4.431 (2.954–6.645) | 1.690 (1.257–2.272) | ||
| IADL | 1.161 (0.941–1.434) | 1.036 (0.805–1.332) | 1.240 (0.996–1.543) | ||
| Walking | 2.723 (1.806–4.104) | 4.813 (3.110–7.451) | 1.584 (1.153–2.175) | ||
| Eating | 1.052 (0.539–2.053) | 1.811 (0.859–3.820) | 1.792 (0.974–3.299) | ||
| Dressing | 1.406 (0.764–2.591) | 1.741 (0.852–3.556) | 1.654 (0.944–2.900) | ||
| Grooming | 1.363 (0.734–2.530) | 1.783 (0.870–3.654) | 2.010 (1.153–3.504) | ||
| Bathing | 1.654 (1.018–2.668) | 4.168 (2.509–6.922) | 1.467 (0.981–2.193) | ||
| Toileting | 1.495 (0.889–2.515) | 2.071 (1.153–3.719) | 2.185 (1.399–3.413) | ||
| Using the telephone | 0.957 (0.757–1.209) | 0.788 (0.590–1.053) | 1.202 (0.943–1.533) | ||
| Financial management | 1.040 (0.761–1.422) | 0.983 (0.668–1.446) | 1.468 (1.081–1.994) | ||
| Using public vehicles | 1.084 (0.871–1.349) | 0.895 (0.685–1.168) | 1.199 (0.957–1.502) | ||
| Preparing a meal | 1.765 (1.164–2.675) | 4.313 (2.772–6.710) | 1.871 (1.333–2.626) | ||
| Performing household tasks | 1.233 (0.777–1.956) | 2.552 (1.547–4.212) | 2.408 (1.626–3.565) | ||
| Taking medication | 1.818 (1.102–3.000) | 3.394 (1.985–5.803) | 1.492 (0.978–2.277) | ||
| Doing some washing | 1.326 (0.891–1.974) | 2.368 (1.531–3.665) | 1.520 (1.066–2.166) | ||
| Grocery shopping | 1.883 (1.319–2.687) | 2.749 (1.845–4.096) | 1.576 (1.156–2.147) | ||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, S.; Qin, J.; Li, Y.; Wei, Y.; Long, B.; Cai, J.; Tang, J.; Xu, X.; Yu, G.; Zhang, Z. Disability and Its Influencing Factors among the Elderly in a County, Guangxi Province, China. Int. J. Environ. Res. Public Health 2018, 15, 1967. https://doi.org/10.3390/ijerph15091967
Chen S, Qin J, Li Y, Wei Y, Long B, Cai J, Tang J, Xu X, Yu G, Zhang Z. Disability and Its Influencing Factors among the Elderly in a County, Guangxi Province, China. International Journal of Environmental Research and Public Health. 2018; 15(9):1967. https://doi.org/10.3390/ijerph15091967
Chicago/Turabian StyleChen, Shiyi, Jian Qin, You Li, Yi Wei, Bingshuang Long, Jiansheng Cai, Jiexia Tang, Xia Xu, Guoqi Yu, and Zhiyong Zhang. 2018. "Disability and Its Influencing Factors among the Elderly in a County, Guangxi Province, China" International Journal of Environmental Research and Public Health 15, no. 9: 1967. https://doi.org/10.3390/ijerph15091967
APA StyleChen, S., Qin, J., Li, Y., Wei, Y., Long, B., Cai, J., Tang, J., Xu, X., Yu, G., & Zhang, Z. (2018). Disability and Its Influencing Factors among the Elderly in a County, Guangxi Province, China. International Journal of Environmental Research and Public Health, 15(9), 1967. https://doi.org/10.3390/ijerph15091967