Location of Femoral Fractures in Patients with Different Weight Classes in Fall and Motorcycle Accidents: A Retrospective Cross-Sectional Analysis



Abstract
:1. Background
2. Methods
Study Design
3. Results
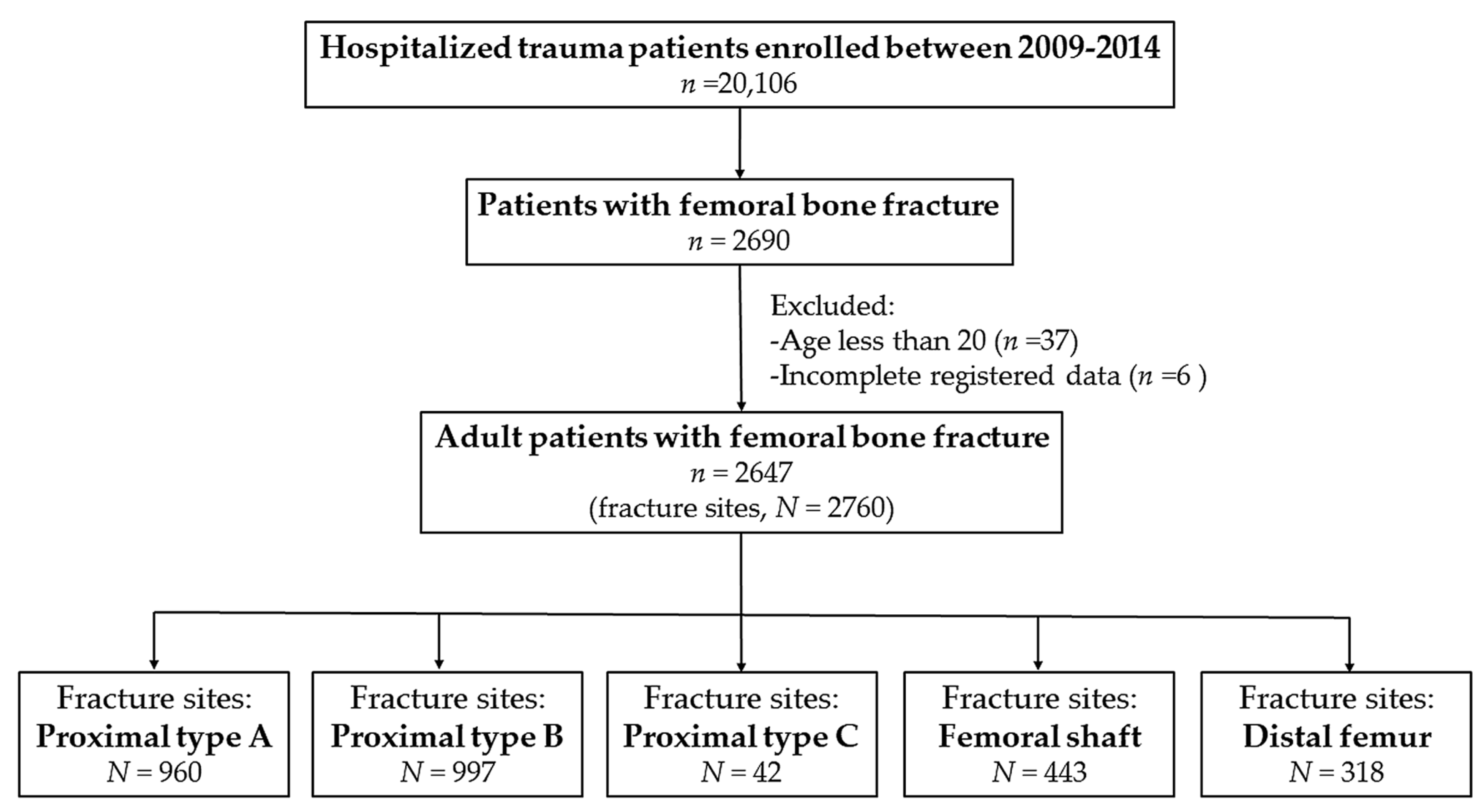
3.1. Characteristics of the Patients with Femoral Fracture
3.2. Location of Femoral Fractures in Patients with Different Injury Mechanisms
3.3. Location of Femoral Fractures in Patients with Different Weight Classes in Fall Accidents
3.4. Location of Femoral Fractures in Patients with Different Weight Classes in Motorcycle Accidents
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Pollack, K.M.; Xie, D.; Arbogast, K.B.; Durbin, D.R. Body mass index and injury risk among US children 9–15 years old in motor vehicle crashes. Inj. Prev. 2008, 14, 366–371. [Google Scholar] [CrossRef] [PubMed]
- Matter, K.C.; Sinclair, S.A.; Hostetler, S.G.; Xiang, H. A comparison of the characteristics of injuries between obese and non-obese inpatients. Obesity 2007, 15, 2384–2390. [Google Scholar] [CrossRef] [PubMed]
- Chan, G.; Chen, C.T. Musculoskeletal effects of obesity. Curr. Opin. Pediatr. 2009, 21, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Kessler, J.; Koebnick, C.; Smith, N.; Adams, A. Childhood obesity is associated with increased risk of most lower extremity fractures. Clin. Orthop. Relat. Res. 2013, 471, 1199–1207. [Google Scholar] [CrossRef] [PubMed]
- Compston, J.E.; Watts, N.B.; Chapurlat, R.; Cooper, C.; Boonen, S.; Greenspan, S.; Pfeilschifter, J.; Silverman, S.; Diez-Perez, A.; Lindsay, R.; et al. Obesity is not protective against fracture in postmenopausal women: GLOW. Am. J. Med. 2011, 124, 1043–1050. [Google Scholar] [CrossRef] [PubMed]
- Beck, T.J.; Petit, M.A.; Wu, G.; LeBoff, M.S.; Cauley, J.A.; Chen, Z. Does obesity really make the femur stronger? BMD, geometry, and fracture incidence in the women’s health initiative-observational study. J. Bone Miner. Res. 2009, 24, 1369–1379. [Google Scholar] [CrossRef] [PubMed]
- Vanhaecht, K.; Sermeus, W.; Peers, J.; Lodewijckx, C.; Deneckere, S.; Leigheb, F.; Boonen, S.; Sermon, A.; Boto, P.; Mendes, R.V.; et al. The impact of care pathways for patients with proximal femur fracture: Rationale and design of a cluster-randomized controlled trial. BMC Health Serv. Res. 2012, 12, 124. [Google Scholar] [CrossRef] [PubMed]
- Griffin, X.L.; Parsons, N.; Zbaeda, M.M.; McArthur, J. Interventions for treating fractures of the distal femur in adults. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef] [PubMed]
- Kato, I.; Toniolo, P.; Zeleniuch-Jacquotte, A.; Shore, R.E.; Koenig, K.L.; Akhmedkhanov, A.; Riboli, E. Diet, smoking and anthropometric indices and postmenopausal bone fractures: A prospective study. Int. J. Epidemiol. 2000, 29, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Looker, A.C.; Flegal, K.M.; Melton, L.J., 3rd. Impact of increased overweight on the projected prevalence of osteoporosis in older women. Osteoporos. Int. 2007, 18, 307–313. [Google Scholar] [CrossRef] [PubMed]
- Hayes, W.C.; Myers, E.R.; Morris, J.N.; Gerhart, T.N.; Yett, H.S.; Lipsitz, L.A. Impact near the hip dominates fracture risk in elderly nursing home residents who fall. Calcif. Tissue Int. 1993, 52, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Rupp, J.D.; Flannagan, C.A.; Kuppa, S.M. Injury risk curves for the skeletal knee-thigh-hip complex for knee-impact loading. Accid. Anal. Prev. 2010, 42, 153–158. [Google Scholar] [CrossRef] [PubMed]
- Bouxsein, M.L.; Szulc, P.; Munoz, F.; Thrall, E.; Sornay-Rendu, E.; Delmas, P.D. Contribution of trochanteric soft tissues to fall force estimates, the factor of risk, and prediction of hip fracture risk. J. Bone Miner. Res. 2007, 22, 825–831. [Google Scholar] [CrossRef] [PubMed]
- Rupp, J.D.; Flannagan, C.A.; Leslie, A.J.; Hoff, C.N.; Reed, M.P.; Cunningham, R.M. Effects of BMI on the risk and frequency of AIS 3+ injuries in motor-vehicle crashes. Obesity 2013, 21, E88–E97. [Google Scholar] [CrossRef] [PubMed]
- Carter, P.M.; Flannagan, C.A.; Reed, M.P.; Cunningham, R.M.; Rupp, J.D. Comparing the effects of age, BMI and gender on severe injury (AIS 3+) in motor-vehicle crashes. Accid. Anal. Prev. 2014, 72, 146–160. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.T.; Liang, C.C.; Rau, C.S.; Hsu, S.Y.; Hsieh, C.H. Alcohol-related hospitalizations of adult motorcycle riders. World J. Emerg. Surg. 2015, 10, 2. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, C.H.; Hsu, S.Y.; Hsieh, H.Y.; Chen, Y.C. Differences between the sexes in motorcycle-related injuries and fatalities at a Taiwanese level I trauma center. Biomed. J. 2017, 40, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, C.H.; Liu, H.T.; Hsu, S.Y.; Hsieh, H.Y.; Chen, Y.C. Motorcycle-related hospitalizations of the elderly. Biomed. J. 2017, 40, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Deasy, C.; Gabbe, B.; Palmer, C.; Babl, F.E.; Bevan, C.; Crameri, J.; Butt, W.; Fitzgerald, M.; Judson, R.; Cameron, P. Paediatric and adolescent trauma care within an integrated trauma system. Injury 2012, 43, 2006–2011. [Google Scholar] [CrossRef] [PubMed]
- Chuang, J.F.; Rau, C.S.; Kuo, P.J.; Chen, Y.C.; Hsu, S.Y.; Hsieh, H.Y.; Hsieh, C.H. Traumatic injuries among adult obese patients in southern Taiwan: A cross-sectional study based on a trauma registry system. BMC Public Health 2016, 16, 275. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.T.; Rau, C.S.; Wu, S.C.; Chen, Y.C.; Hsu, S.Y.; Hsieh, H.Y.; Hsieh, C.H. Obese motorcycle riders have a different injury pattern and longer hospital length of stay than the normal-weight patients. Scand. J. Trauma Resusc. Emerg. Med. 2016, 24, 50. [Google Scholar] [CrossRef] [PubMed]
- Byard, R.W.; Langlois, N.E. Letter to the editor—Increasing body weight of motorcycle riders. J. Forensic Sci. 2011, 56, 1661. [Google Scholar] [CrossRef] [PubMed]
- Physical Status: The Use and Interpretation of Anthropometry; Report of a WHO Expert Committee; World Health Organization Technical Report Series; WHO: Geneva, Switzerland, 1995; Volume 854, pp. 1–452.
- Obesity: Preventing and Managing the Global Epidemic; Report of a WHO Consultation; World Health Organization Technical Report Series; WHO: Geneva, Switzerland, 2000; Volume 894, pp. 1–253.
- Muller, M.; Koch, S.N.P.; Schatzker, J. The Comprehensive Classification of Fractures of the Long Bones; Springer: Berlin, Germany, 1990. [Google Scholar]
- De Laet, C.; Oden, A.; Johansson, H.; Johnell, O.; Jonsson, B.; Kanis, J.A. The impact of the use of multiple risk indicators for fracture on case-finding strategies: A mathematical approach. Osteoporos. Int. 2005, 16, 313–318. [Google Scholar] [CrossRef] [PubMed]
- Gregory, J.S.; Aspden, R.M. Femoral geometry as a risk factor for osteoporotic hip fracture in men and women. Med. Eng. Phys. 2008, 30, 1275–1286. [Google Scholar] [CrossRef] [PubMed]
- Keyak, J.H.; Skinner, H.B.; Fleming, J.A. Effect of force direction on femoral fracture load for two types of loading conditions. J. Orthop. Res. 2001, 19, 539–544. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variables | Patients n = 2647 |
|---|---|
| Gender, n (%) | |
| Male | 1153 (43.6) |
| Female | 1494 (56.4) |
| Age (years) | 66.5±19.5 |
| BMI classification, n (%) | |
| Obese | 202 (7.6) |
| Overweight | 643 (24.3) |
| Normal | 1552 (58.6) |
| Underweight | 250 (9.4) |
| Mechanisms, n (%) | |
| Fall | 1719 (64.9) |
| Motorcycle | 690 (26.1) |
| Bicycle | 112 (4.2) |
| Motor vehicle | 54 (2.0) |
| Struck by/against | 44 (1.7) |
| Pedestrian | 28 (1.1) |
| AIS, n (%) | |
| Head/Neck | 229 (8.7) |
| Face | 137 (5.2) |
| Thorax | 130 (4.9) |
| Abdomen | 78 (2.9) |
| ISS, median (IQR) | 9 (9–9) |
| <16 | 2489 (94.0) |
| 16–24 | 81 (3.1) |
| ≥25 | 77 (2.9) |
| Variables | Fall n = 1765 (I) | Motorcycle n = 744 (II) | Bicycle n = 113 (III) | Motor Vehicle n = 61 (IV) | Struck by/against n = 48 (V) | Pedestrian n = 29 (VI) |
|---|---|---|---|---|---|---|
| Proximal-A | 737 (41.8) | 158 (21.2) | 40 (35.4) | 8 (13.1) | 9 (18.8) | 8 (27.6) |
| Proximal-B | 799 (45.3) | 115 (15.5) | 57 (50.4) | 6 (9.8) | 12 (25.0) | 8 (27.6) |
| Proximal-C | 4 (0.2) | 28 (3.8) | 1 (0.9) | 9 (14.8) | 0 (0.0) | 0 (0.0) |
| Shaft | 112 (6.3) | 276 (37.1) | 6 (5.3) | 25 (41.0) | 18 (37.5) | 6 (20.7) |
| Distal | 113 (6.4) | 167 (22.4) | 9 (8.0) | 13 (21.3) | 9 (18.8) | 7 (24.1) |
| Variables | OR (95%CI) | p | OR (95%CI) | p | OR (95%CI) | p | OR (95%CI) | p | OR (95%CI) | p |
|---|---|---|---|---|---|---|---|---|---|---|
| II vs. I | III vs. I | IV vs. I | V vs. I | VI vs. I | ||||||
| Proximal-A | 0.4 (0.31–0.46) | <0.001 | 0.8 (0.51–1.14) | 0.183 | 0.2 (0.10–0.45) | <0.001 | 0.3 (0.16–0.67) | 0.001 | 0.5 (0.23–1.21) | 0.125 |
| Proximal-B | 0.2 (0.18–0.28) | <0.001 | 1.2 (0.84–1.80) | 0.284 | 0.1 (0.06–0.31) | <0.001 | 0.4 (0.21–0.78) | 0.005 | 0.5 (0.20–1.05) | 0.058 |
| Proximal-C | 17.2 (6.02–49.26) | <0.001 | 3.9 (0.44–35.46) | 0.267 | 76.2 (22.73–255.44) | <0.001 | — | 1.000 | — | 1.000 |
| Shaft | 8.7 (6.83–11.09) | <0.001 | 0.8 (0.36–1.93) | 0.660 | 10.2 (5.94–17.68) | <0.001 | 8.9 (4.79–16.38) | <0.001 | 3.9 (1.54–9.65) | 0.010 |
| Distal | 4.2 (3.27–5.47) | <0.001 | 1.3 (0.62–2.57) | 0.514 | 4.0 (2.08–7.52) | <0.001 | 3.4 (1.60–7.14) | 0.004 | 4.7 (1.95–11.12) | 0.002 |
| Variables | Obese n = 108 (II) | Overweight n = 415 (III) | Underweight n = 185 (IV) | Normal n = 1057 (I) | OR (95%CI) | p | OR (95%CI) | p | OR (95%CI) | p |
|---|---|---|---|---|---|---|---|---|---|---|
| II vs. I | III vs. I | IV vs. I | ||||||||
| Proximal-A | 39 (36.1) | 170 (41.0) | 91 (49.2) | 437 (41.3) | 0.8 (0.53–1.21) | 0.292 | 1.0 (0.78–1.24) | 0.894 | 1.4 (1.00–1.88) | 0.046 |
| Proximal-B | 36 (33.3) | 162 (39.0) | 87 (47.0) | 514 (48.6) | 0.5 (0.35–0.80) | 0.002 | 0.7 (0.54–0.85) | 0.001 | 0.9 (0.69–1.28) | 0.688 |
| Proximal-C | 0 (0.0) | 3 (0.7) | 0 (0.0) | 1 (0.1) | — | 1.000 | 7.7 (0.80–74.13) | 0.070 | — | 1.000 |
| Shaft | 15 (13.9) | 36 (8.7) | 6 (3.2) | 55 (5.2) | 2.9 (1.60–5.40) | <0.001 | 1.7 (1.12–2.68) | 0.013 | 0.6 (0.26–1.44) | 0.255 |
| Distal | 18 (16.7) | 44 (10.6) | 1 (0.5) | 50 (4.7) | 4.0 (2.26–7.20) | <0.001 | 2.4 (1.57–3.64) | <0.001 | 0.1 (0.02–0.80) | 0.008 |
| Variables | Obese n = 92 (II) | Overweight n = 206 (III) | Underweight n = 47 (IV) | Normal n = 399 (I) | OR (95%CI) | p | OR (95%CI) | p | OR (95%CI) | p |
|---|---|---|---|---|---|---|---|---|---|---|
| II vs. I | III vs. I | IV vs. I | ||||||||
| Proximal-A | 19 (20.7) | 40 (19.4) | 12 (25.5) | 87 (21.8) | 0.9 (0.53–1.63) | 0.809 | 0.9 (0.57–1.31) | 0.494 | 1.2 (0.61–2.47) | 0.561 |
| Proximal-B | 7 (7.6) | 25 (12.1) | 12 (25.5) | 71 (17.8) | 0.4 (0.17–0.86) | 0.016 | 0.6 (0.39–1.04) | 0.071 | 1.6 (0.78–3.20) | 0.197 |
| Proximal-C | 5 (5.4) | 9 (4.4) | 1 (2.1) | 13 (3.3) | 1.7 (0.59–4.91) | 0.353 | 1.4 (0.57–3.23) | 0.489 | 0.6 (0.08–5.05) | 1.000 |
| Shaft | 34 (37.0) | 80 (38.8) | 18 (38.3) | 144 (36.1) | 1.0 (0.65–1.66) | 0.876 | 1.1 (0.80–1.59) | 0.508 | 1.1 (0.59–2.05) | 0.766 |
| Distal | 27 (29.3) | 52 (25.2) | 4 (8.5) | 84 (21.1) | 1.6 (0.94–2.59) | 0.086 | 1.3 (0.85–1.88) | 0.242 | 0.3 (0.12–1.02) | 0.051 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, M.-W.; Liu, H.-T.; Huang, C.-Y.; Chien, P.-C.; Hsieh, H.-Y.; Hsieh, C.-H. Location of Femoral Fractures in Patients with Different Weight Classes in Fall and Motorcycle Accidents: A Retrospective Cross-Sectional Analysis. Int. J. Environ. Res. Public Health 2018, 15, 1082. https://doi.org/10.3390/ijerph15061082
Chang M-W, Liu H-T, Huang C-Y, Chien P-C, Hsieh H-Y, Hsieh C-H. Location of Femoral Fractures in Patients with Different Weight Classes in Fall and Motorcycle Accidents: A Retrospective Cross-Sectional Analysis. International Journal of Environmental Research and Public Health. 2018; 15(6):1082. https://doi.org/10.3390/ijerph15061082
Chicago/Turabian StyleChang, Meng-Wei, Hang-Tsung Liu, Chun-Ying Huang, Peng-Chen Chien, Hsiao-Yun Hsieh, and Ching-Hua Hsieh. 2018. "Location of Femoral Fractures in Patients with Different Weight Classes in Fall and Motorcycle Accidents: A Retrospective Cross-Sectional Analysis" International Journal of Environmental Research and Public Health 15, no. 6: 1082. https://doi.org/10.3390/ijerph15061082
APA StyleChang, M.-W., Liu, H.-T., Huang, C.-Y., Chien, P.-C., Hsieh, H.-Y., & Hsieh, C.-H. (2018). Location of Femoral Fractures in Patients with Different Weight Classes in Fall and Motorcycle Accidents: A Retrospective Cross-Sectional Analysis. International Journal of Environmental Research and Public Health, 15(6), 1082. https://doi.org/10.3390/ijerph15061082