Effectiveness of Integration and Re-Integration into Work Strategies for Persons with Chronic Conditions: A Systematic Review of European Strategies

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy for the Complete PATHWAYS Review
2.2. Selection Criteria for the Complete PATHWAYS Review
- (a)
- had been published between January 2011 and April 2016;
- (b)
- were published in English;
- (c)
- were intervention studies, namely randomized trials, non-randomized controlled trials, non-controlled pre-post intervention studies;
- (d)
- were observational studies, namely cohort studies, case-control studies, cross-sectional studies, descriptive longitudinal studies,
- (e)
- were qualitative studies;
- (f)
- had been carried out in the 28 countries of the European Union, in Norway, Lichtenstein, Iceland or Switzerland, or in non-European countries with western lifestyle: Canada, United States of America, Australia;
- (g)
- reported on effectiveness regarding at least one of the following work outcomes:
- (1)
- employment status (employed/unemployed);
- (2)
- return to work;
- (3)
- absenteeism (sick leave);
- (4)
- maintain a job;
- (5)
- obtain a job.
- (h)
- investigated variables potentially affecting effectiveness (e.g., views and experiences of involved persons with a given strategy).
- (a)
- persons with chronic diseases in general, i.e., specific conditions are not further specified in the studies or results for different conditions are reported together, and persons with disability in general. Persons with disability were included as usually the majority of people who receive disability benefits have chronic diseases and experience significant levels of disability in daily life [13];
- (b)
- the following disease groups: mental disorders, musculoskeletal disorders, cancer, neurological, metabolic, respiratory and cardiovascular diseases;
- (c)
- the following specific diseases: depression, back and neck pain, migraine, diabetes mellitus, chronic obstructive pulmonary disease and ischemic heart disease.
- (a)
- included participants with mainly other chronic diseases as the ones defined above and only pooled results were reported;
- (b)
- included participants aged <16 or >65 years;
- (c)
- were case report/case series, psychometric studies, letters, comments, editorials, overviews without empirical primary or secondary data, reviews (systematic and non-systematic reviews, health technology assessments) and meta-analyses, protocols, studies reporting exclusively on design or baseline data;
- (d)
- consider neither effectiveness outcomes, for example, studies reporting only on costs resulting from the implementation of strategies nor variables potentially affecting effectiveness;
- (e)
- did not focus on a concrete strategy or group of strategies, for example, studies focusing on factors facilitating return to work after sick leave in general;
- (f)
- were published in other languages than English;
- (g)
- were published before 2011;
- (h)
- had no abstract available.
2.3. Eligibility Assessment for the Complete PATHWAYS Review
2.4. Data Extraction and Data Synthesis for the Complete PATHWAYS Review
2.5. Methodological Assessment for the Complete PATHWAYS Review
- (a)
- shortcomings are unlikely to change study’s conclusions regarding the outcomes of interest;
- (b)
- shortcomings are likely or very likely to change study’s conclusions regarding outcomes of interest.
- -
- Yes. Yes was selected if estimates for relevant work outcomes had an adequate p-value, usually <0.05, or if the confidence interval for the estimate excluded the no-effect value (e.g., the value 1 was not included in the confidence interval of reported odds ratio);
- -
- Unclear. Unclear was selected if the precision of the effect estimate was not reported, results were inconsistent or difficult to interpret (e.g., statistically non-significant but large estimates in subgroup analyses);
- -
- No. No was selected if data did not support the presence of an effect of the intervention on relevant work outcomes.
3. Results
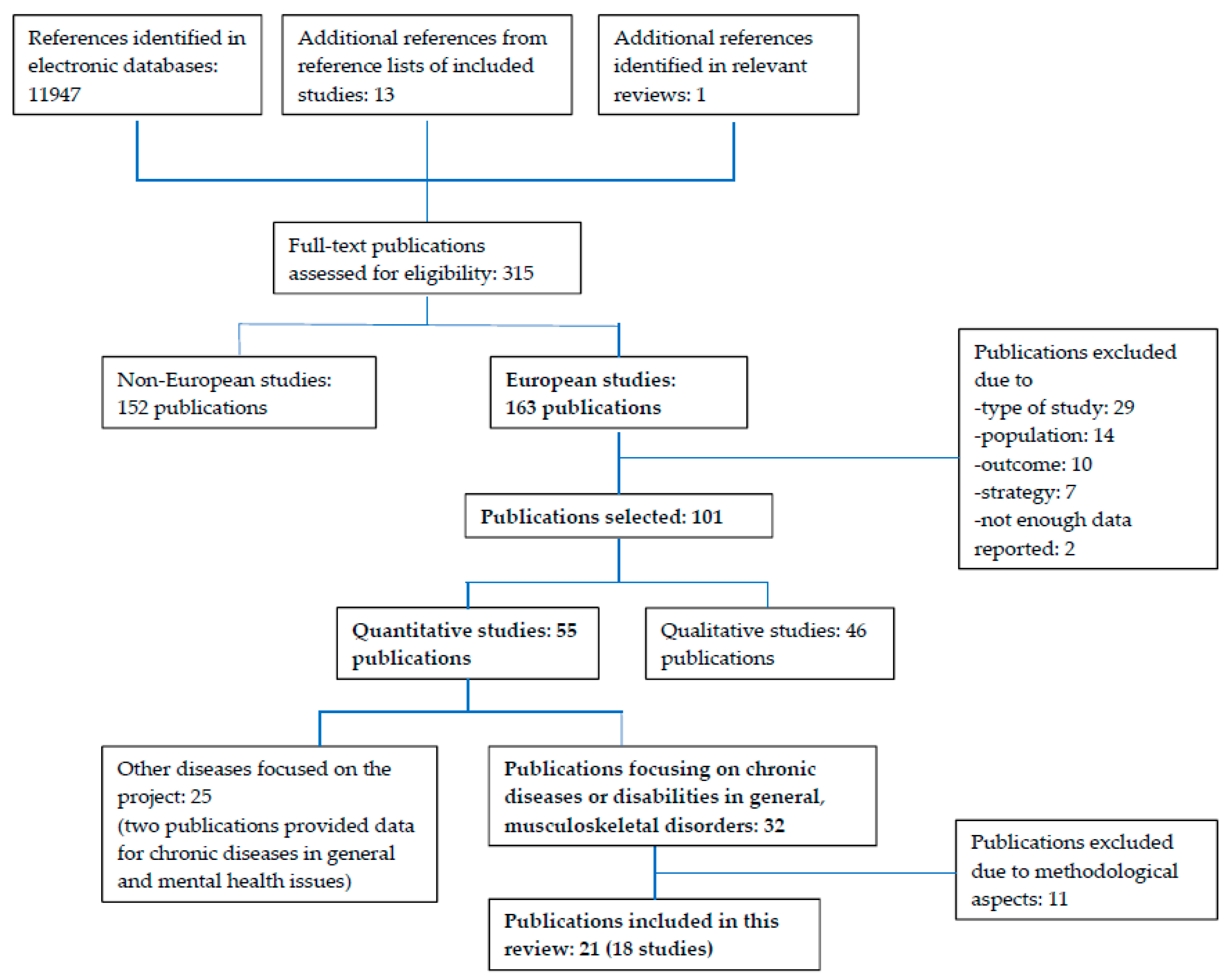
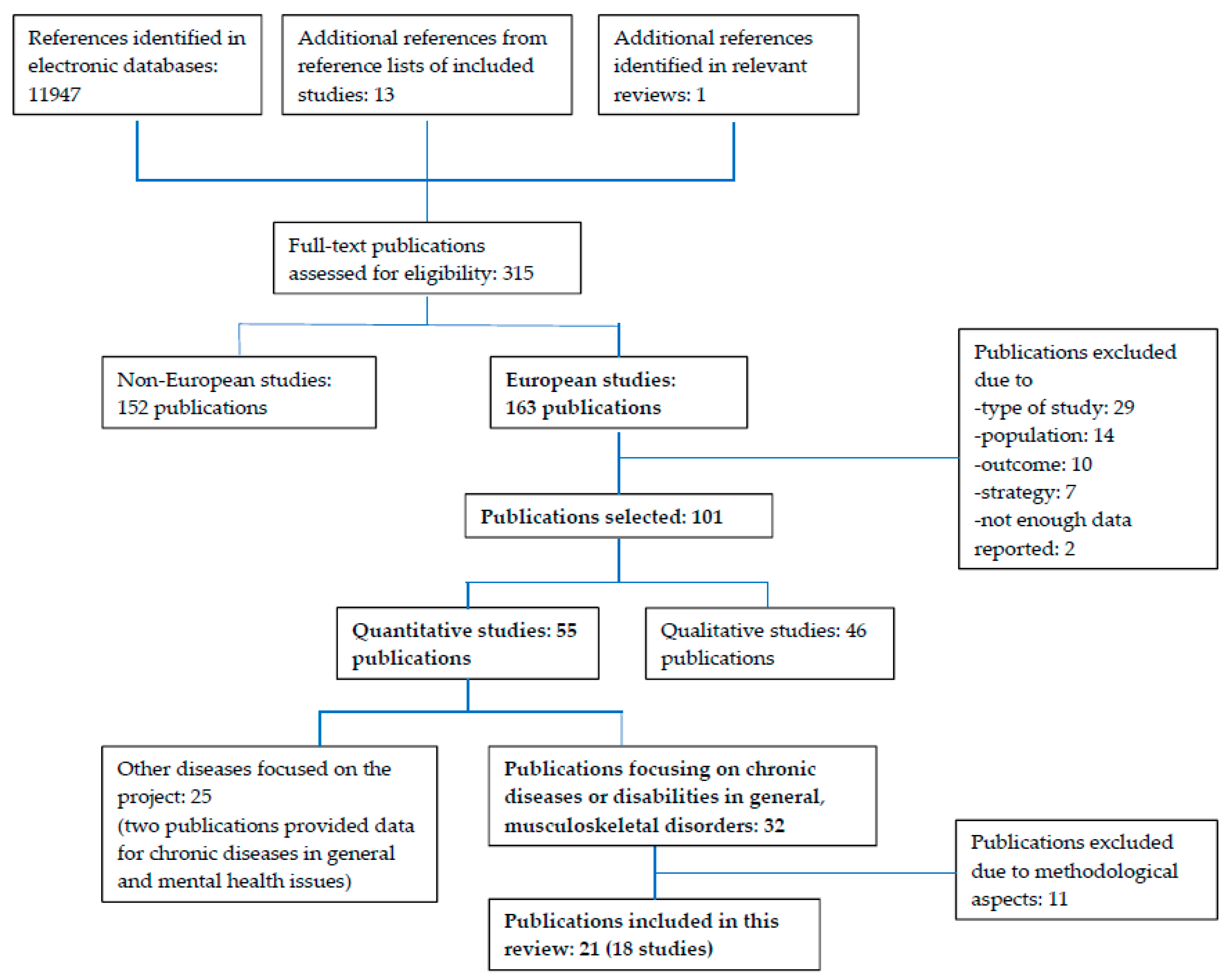
3.1. Study Selection and Characteristics of Studies
3.2. Interventions for Chronic Diseases and Disability in General
3.3. Interventions for Musculoskeletal Disorders
3.4. Interventions by Level
3.4.1. Policy Level
3.4.2. System Level
Disability Support Benefit for Persons with Long-Lasting Disability
Part-Time Sick Leave (PTSL)
Studies Reporting Positive Change
3.5. Service Level
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Alonso, J.; Vilagut, G.; Adroher, N.D.; Chatterji, S.; He, Y.; Andrade, L.H.; Bromet, E.; Bruffaerts, R.; Fayyad, J.; Florescu, S.; et al. Disability mediates the impact of common conditions on perceived health. PLoS ONE 2013, 8, e65858. [Google Scholar] [CrossRef]
- Rodriguez-Blazquez, C.; Damian, J.; Andres-Prado, M.J.; Almazan-Isla, J.; Alcalde-Cabero, E.; Forjaz, M.J.; Castellote, J.M.; Gonzalez-Enriquez, J.; Martinez-Martin, P.; Comin, M.; et al. Associations between chronic conditions, body functions, activity limitations and participation restrictions: A cross-sectional approach in Spanish non-clinical populations. BMJ Open 2016, 6, e010446. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Noncommunicable Diseases. Available online: http://www.who.int/ mediacentre/factsheets/fs355/en/ (accessed on 21 February 2018).
- Grammenos, S. European Comparative Data on Europe 2020 & People with Disabilities; Academic Network of European Disability Experts (ANED): Brussels, Belgium, 2013. [Google Scholar]
- Busse, R.; Blümel, M.; Scheller-Kreinsen, D.; Zentner, A. Tackling Chronic Disease in Europe: Strategies, Interventions and Challenges; World Health Organization on Behalf of the European Observatory on Health Systems and Policies: Geneva, Switzerland, 2010. [Google Scholar]
- Eurostat. Gender Pay Gap Statistics. Available online: http://ec.europa.eu/eurostat/statistics-explained/index.php/Gender_pay_gap_statistics (accessed on 21 February 2018).
- Kessler, R.C.; Greenberg, P.E.; Mickelson, K.D.; Meneades, L.M.; Wang, P.S. The effects of chronic medical conditions on work loss and work cutback. J. Occup. Environ. Med. 2001, 43, 218–225. [Google Scholar] [CrossRef] [PubMed]
- OECD/EU. Health at a Glance: Europe 2016: State of Health in the EU Cycle; OECD Publishing: Paris, France, 2016; Available online: http://dx.doi.org/10.1787/9789264265592-en (accessed on 21 February 2018).
- International Diabetes Federation. IDF Diabetes Atlas, 8th ed.; IDF: Brussels, Belgium, 2017; Available online: http://www.diabetesatlas.org (accessed on 21 February 2018).
- World Health Organization. Global Action Plan for the Prevention and Control of Noncommunicable Diseases in 2013–2020; WHO: Geneva, Switzerland, 2013; Available online: http://apps.who.int/iris/bitstream/10665/94384/1/9789241506236_eng.pdf?ua=1 (accessed on 21 February 2018).
- Scaratti, C.; Leonardi, M.; Silvaggi, F.; Avila, C.; Olaya, B.; Stavroussi, P.; Roca, O.; Burger, H.; Fheodoroff, K.; Tobiasz-Adamczyk, B.; et al. Mapping european welfare models: State of the art of strategies for professional integration and reintegration of persons with chronic diseases including mental health conditions. Int. J. Environ. Res. Public Health 2018. under review. [Google Scholar]
- Dutch National Institute for Public Health and the Environment. Europeans of Retirement Age: Chronic Diseases and Economic Activity; RIVM: Bilthoven, The Netherlands, 2012. Available online: https://ec.europa.eu/health/sites/health/files/major_chronic_diseases/docs/rivm_report_retirement_en.pdf (accessed on 21 February 2018).
- Oortwijn, W.; Nelissen, E.; Adamini, S.; van den Heuvel, S.; Geuskens, G.; Burdorf, L. Social Determinants State of the Art Reviews-Health of People of Working Age-Full Report; European Commission Directorate General for Health and Consumers: Luxembourg, 2011. [Google Scholar]
- Agovino, M.; Rapposelli, A. Speculation on a Flexicurity Index for Disabled People: The Italian Case. Available online: https://www.researchgate.net/publication/284136632_Speculation_on_a_Flexicurity_Index_for_Disabled_People_The_Italian_Case (accessed on 19 March 2018).
- National Institute for Health and Care Excellence. Methods for the Development of NICE Public Health Guidance; National Institute for Health and Care Excellence (NICE): London, UK, 2012. Available online: http://www.ncbi.nlm.nih.gov/books/NBK395862/ (accessed on 28 June 2016).
- Esteban, E.; Coenen, M.; Ito, E.; Gruber, S.; Scaratti, C.; Leonardi, M.; Vlachou, A.; Muñoz-Murillo, A.; Ávila, C.C.; Brecelj, V.; et al. Views and experiences of persons with chronic diseases about strategies that aim to integrate and re-integrate them at work: A systematic review of qualitative studies. 2018; in preparation. [Google Scholar]
- Muñoz-Murillo, A.; Esteban, E.; Ávila, C.C.; Fheodoroff, K.; Haro, J.M.; Leonardi, M.; Olaya, B. Furthering the evidence of the effectiveness of employment strategies for people with mental health disorders in Europe: A systematic review. Int. J. Environ. Res. Public Health, 2018; under review. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, T.P. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Lopez Frutos, E.M.; Castello, J.V. Equal health, equal work? The role of disability benefits in employment after controlling for health status. Eur. J. Health Econ. 2015, 16, 329–340. [Google Scholar] [CrossRef] [PubMed]
- Johansson, P.; Lindahl, E. Locking-in effects due to early interventions? An evaluation of a multidisciplinary screening programs for avoiding long-term sickness. Eval. Rev. 2012, 36, 323–345. [Google Scholar] [CrossRef] [PubMed]
- Poulsen, O.M.; Aust, B.; Bjorner, J.B.; Rugulies, R.; Hansen, J.V.; Tverborgvik, T.; Winzor, G.; Mortensen, O.S.; Helverskov, T.; Orbaek, P.; et al. Effect of the danish return-to-work program on long-term sickness absence: Results from a randomized controlled trial in three municipalities. Scand. J. Work Environ. Health 2014, 40, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Høgelund, J.; Holm, A.; Eplov, L.F. The effect of part-time sick leave for employees with mental disorders. J. Ment. Health Policy Econ. 2012, 15, 157–170. [Google Scholar] [PubMed]
- Markussen, S.; Mykletun, A.; Røed, K. The case for presenteeism—Evidence from norway’s sickness insurance program. J. Public Econ. 2012, 96, 959–972. [Google Scholar] [CrossRef]
- Kausto, J.; Solovieva, S.; Virta, L.J.; Viikari-Juntura, E. Partial sick leave associated with disability pension: Propensity score approach in a register-based cohort study. BMJ Open 2012, 2, e001752. [Google Scholar] [CrossRef] [PubMed]
- Kausto, J.; Viikari-Juntura, E.; Virta, L.J.; Gould, R.; Koskinen, A.; Solovieva, S. Effectiveness of new legislation on partial sickness benefit on work participation: A quasi-experiment in finland. BMJ Open 2014, 4, e006685. [Google Scholar] [CrossRef] [PubMed]
- Halonen, J.I.; Solovieva, S.; Pentti, J.; Kivimaki, M.; Vahtera, J.; Viikari-Juntura, E. Effectiveness of legislative changes obligating notification of prolonged sickness absence and assessment of remaining work ability on return to work and work participation: A natural experiment in finland. Occup. Environ. Med. 2016, 73, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Steiner, A.S.; Sartori, M.; Leal, S.; Kupper, D.; Gallice, J.P.; Rentsch, D.; Cedraschi, C.; Genevay, S. Added value of an intensive multidisciplinary functional rehabilitation programme for chronic low back pain patients. Swiss Med. Wkly. 2013, 143, w13763. [Google Scholar] [CrossRef] [PubMed]
- Jensen, C.; Jensen, O.K.; Christiansen, D.H.; Nielsen, C.V. One-year follow-up in employees sick-listed because of low back pain: Randomized clinical trial comparing multidisciplinary and brief intervention. Spine 2011, 36, 1180–1189. [Google Scholar] [CrossRef] [PubMed]
- Jensen, C.; Jensen, O.K.; Nielsen, C.V. Sustainability of return to work in sick-listed employees with low-back pain. Two-year follow-up in a randomized clinical trial comparing multidisciplinary and brief intervention. BMC Musculoskelet. Disord. 2012, 13, 156. [Google Scholar] [CrossRef] [PubMed]
- Stapelfeldt, C.M.; Christiansen, D.H.; Jensen, O.K.; Nielsen, C.V.; Petersen, K.D.; Jensen, C. Subgroup analyses on return to work in sick-listed employees with low back pain in a randomised trial comparing brief and multidisciplinary intervention. BMC Musculoskelet. Disord. 2011, 12, 112. [Google Scholar] [CrossRef] [PubMed]
- Vermeulen, S.J.; Anema, J.R.; Schellart, A.J.; Knol, D.L.; van Mechelen, W.; van der Beek, A.J. A participatory return-to-work intervention for temporary agency workers and unemployed workers sick-listed due to musculoskeletal disorders: Results of a randomized controlled trial. J. Occup. Rehabilit. 2011, 21, 313–324. [Google Scholar] [CrossRef] [PubMed]
- Du Bois, M.; Donceel, P. Guiding low back claimants to work: A randomized controlled trial. Spine 2012, 37, 1425–1431. [Google Scholar] [CrossRef] [PubMed]
- Jensen, L.D.; Maribo, T.; Schiottz-Christensen, B.; Madsen, F.H.; Gonge, B.; Christensen, M.; Frost, P. Counselling low-back-pain patients in secondary healthcare: A randomised trial addressing experienced workplace barriers and physical activity. Occup. Environ. Med. 2012, 69, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Myhre, K.; Marchand, G.H.; Leivseth, G.; Keller, A.; Bautz-Holter, E.; Sandvik, L.; Lau, B.; Roe, C. The effect of work-focused rehabilitation among patients with neck and back pain: A randomized controlled trial. Spine 2014, 39, 1999–2006. [Google Scholar] [CrossRef] [PubMed]
- Marchand, G.H.; Myhre, K.; Leivseth, G.; Sandvik, L.; Lau, B.; Bautz-Holter, E.; Roe, C. Change in pain, disability and influence of fear-avoidance in a work-focused intervention on neck and back pain: A randomized controlled trial. BMC Musculoskelet. Disord. 2015, 16, 94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shiri, R.; Martimo, K.P.; Miranda, H.; Ketola, R.; Kaila-Kangas, L.; Liira, H.; Karppinen, J.; Viikari-Juntura, E. The effect of workplace intervention on pain and sickness absence caused by upper-extremity musculoskeletal disorders. Scand. J. Work Environ. Health 2011, 37, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Viikari-Juntura, E.; Kausto, J.; Shiri, R.; Kaila-Kangas, L.; Takala, E.P.; Karppinen, J.; Miranda, H.; Luukkonen, R.; Martimo, K.P. Return to work after early part-time sick leave due to musculoskeletal disorders: A randomized controlled trial. Scand. J. Work Environ. Health 2012, 38, 134–143. [Google Scholar] [CrossRef] [PubMed]
- Andren, D.; Svensson, M. Part-time sick leave as a treatment method for individuals with musculoskeletal disorders. J. Occup. Rehabilit. 2012, 22, 418–426. [Google Scholar] [CrossRef] [PubMed]
- Alford, V.M.; Ewen, S.; Webb, G.R.; McGinley, J.; Brookes, A.; Remedios, L.J. The Use of the International Classification of Functioning, Disability and Health to Understand the Health and functioning experiences of people with chronic conditions from the person perspective: A systematic review. Disabil. Rehabilit. 2015, 37, 655–666. [Google Scholar] [CrossRef] [PubMed]
- GBD 2016 DALYs and HALE Collaborators. Global, regional, and national disability-adjusted life-years (DALYs) for 333 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1260–1344. [Google Scholar]
- Richards, N.C.; Gouda, H.N.; Durham, J.; Rampatige, R.; Rodney, A.; Whittaker, M. Disability, noncommunicable disease and health information. Bull. World Health Organ. 2016, 94, 230–232. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. International Classification of Functioning, Disability and Health: ICF; WHO: Geneva, Switzerland, 2001. [Google Scholar]
- Cieza, A.; Sabariego, C.; Bickenbach, J.; Chatterji, S. Rethinking disability. BMC Med. 2018, 16, 14. [Google Scholar] [CrossRef] [PubMed]
- Gensby, U.; Labriola, M.; Irvin, E.; Amick, B.C.; Lund, T. A classification of components of workplace disability management programs: Results from a systematic review. J. Occup. Rehabilit. 2014, 24, 220–241. [Google Scholar] [CrossRef] [PubMed]
- Ukoumunne, O.C.; Gulliford, M.C.; Chinn, S.; Sterne, J.A.; Burney, P.G. Methods for evaluating area-wide and organisation-based interventions in health and health care: A systematic review. Health Technol. Assess. 1999, 3, iii-92. [Google Scholar] [PubMed]
- Popova, Y.; Kozhevnikova, M. Interdependence of HDI and budget redistribution within the Scandinavian and Continental Social Models. Econ. Manag. 2013, 18, 562–575. [Google Scholar] [CrossRef]
- Eikemo, T.A.; Huisman, M. Health inequalities according to educational level in different welfare regimes: A comparison of 23 European countries. Sociol. Health Illn. 2008, 30, 565–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fenger, H. Welfare Regimes in Central and Eastern Europe: Incorporating Post-Communist Countries in a Welfare Regime Typology. 2007. Available online: http://www.learneurope.eu/files/9913/7483/4204/Welfare_regimes_in_Central_and_Eastern_Europe.pdf (accessed on 21 February 2018).
- European Commission. Employment, Social Affairs & Inclusion. Available online: http://ec.europa.eu/social/main.jsp?catId=102 (accessed on 21 February 2018).
- Vlachou, A.; Stavroussi, P.; Roka, O.; Vasilou, E.; Papadimitriou, D.; Scaratti, C.; Kadyrbaeva, A.; Fheodoroff, K.; Brecelj, V.; Svestkova, O.; et al. Policy guidelines for effective inclusion and re-integration of people with chronic diseases in the workplace: National and European perspectives. Int. J. Environ. Res. Public Health 2018, 15, 493. [Google Scholar] [CrossRef] [PubMed]
- Foitzek, N.; Ávila, C.C.; Ivandic, I.; Bitenc, C.; Cabello, C.; Gruber, S.; Leonardi, M.; Muñoz-Murillo, A.; Scaratti, C.; Tobiasz-Adamczyk, B.; et al. What persons with chronic health conditions need to maintain or return to work–results of an online-survey in seven European countries. Int. J. Environ. Res. Public Health, 2018; under review. [Google Scholar]
- Andren, D.; Andren, T. Part-Time Sick Leave as a Treatment Method? Working Paper in Economics 320; University of Gothenburg: Gothenburg, Sweden, 2008. [Google Scholar]
- Markussen, S.; Mykletun, A.; Røed, K. The Case for Presenteeism; IZA Discussion Paper No. 5343; IZA Institute of Labor Economics: Bonn, Germany, 2010. [Google Scholar]
- Høgelund, J.; Holm, A.; McIntosh, J. Does graded return-to-work improve sick-listed workers’ chance of returning to regular working hours? J. Health Econ. 2010, 29, 158–169. [Google Scholar] [CrossRef] [PubMed]
- Scheel, I.B.; Hagen, K.B.; Herrin, J.; Carling, C.; Oxman, A.D. Blind faith? The effects of promoting active sick leave for back pain patients: A cluster-randomized controlled trial. Spine 2002, 27, 2734–2740. [Google Scholar] [CrossRef] [PubMed]
- Vale, D.; Watts, B.; Franklin, J. The Receding Tide; Understanding Unmet Needs in a Harsher Economic Climate; Research Report; The Young Foundation: London, UK, 2009. [Google Scholar]
- Hoefsmit, N.; Houkes, I.; Nijhuis, F.J. Intervention characteristics that facilitate return to work after sickness absence: A systematic literature review. J. Occup. Rehabilit. 2012, 22, 462–477. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| First Author Year Country Reference | Strategy Study Design Subjects Follow up | Effect on Work-Related Outcomes Supported by Data (Yes/No/Unclear) Employment-Related Outcomes | Further Information |
|---|---|---|---|
| (A) Chronic Disease or Disability | |||
| Policy Strategies | |||
| Agovino M. 2015 Italy [14] | Strategy: co-existence of active labour market policies and passive measures to support PwD Design: cross-sectional, register-based Subjects: people with a disability CG: n.a. IG: n.a. FU: n.a. | YES The combination of active labour market policies to promote the employment of PwD and passive measures to support PwD (i.e., disability pensions) was positively related to the probability of finding a job (p < 0.05) after controlling for labour market variables. RELEVANT OUTCOMES (1) percentage of PwD that are employed | Women: n.r. Yearly data for the period 2006–2011. Strategy: co-existence of
|
| Disability Benefit | |||
| Lopez Frutos E.M. 2015 Spain [19] | Strategy: disability support benefit Design: cross-sectional, register-based Subjects: PwD CG: Certificate of disability without disability support benefit; n = 19,976 IG: Certificate of disability and disability support benefit; n = 27,660 FU: n.a. | NO Being entitled to a disability support benefit showed a significant negative association with the probability of working for individuals in the disability threshold (disability level of 33–44%) after controlling for health and sociodemographic variables (19.3% lower probability of working). For individuals with a degree of disability ≥ 45% there was no statistically significant difference in the probability of working for those receiving a benefit. RELEVANT OUTCOMES (1) employment status | Women 45.6%. The sample includes all individuals that held a certificate of disability in 2008, 2009 or 2010. The certificate of disability is an administrative acknowledgement of a disability degree of 33% or more. Persons with the disability certificate have financial and tax advantages. In addition, persons entitled to a disability support benefit receive a monthly allowance. They are also required to find a different job to the position they had before the disability. |
| Multidisciplinary Intervention | |||
| Johansson P. 2012 Sweden [20] | Strategy: early and holistic evaluation of the need for rehabilitation Design: mixed methods (a-RCT; b-cohort study, register-based) Subjects: individuals on SL and at risk of becoming long-term sick, employed and unemployed CG: usual care; cohort study, n = 37,938; RCT, n = 24 IG: Early and holistic evaluation of the need for rehabilitation; cohort study, n = 1076; RCT, n = 21 FU: RCT approx. 1 year; cohort study approx. 3 year | NO The results from the RCT and the retrospective observational study (controlling for health and sociodemographic variables) did not support a positive effect of the intervention: the sick-spells of the IG lasted longer. RELEVANT OUTCOMES (1) duration of sickness absence Duration of sickness absence: time until leaving the sick spell. | Women: RCT 71–76%; Cohort study 61–65%. RCT: year 2006; Cohort study: 2004–2007; within-subjects analyses 2001–2003 and 2004–2007. Intervention: Multidisciplinary collaboration program (“Resursteam”). Collaboration between the Social Insurance Agency and the primary health care. The sick-listed individual’s medical doctor, her/his case worker, a behaviorist, and a physiotherapist meet regularly to discuss and assess the insured individual’s need for rehabilitation. Goal: to speed up the rehabilitation and reduce absence costs. Comparator: the medical doctor and/or the case worker should suggest a rehabilitation plan. |
| Poulsen O.M. 2014 Denmark [21] | Strategy: multidisciplinary, coordinated and tailored RTW intervention Design: RCT in 3 municipalities: M1, M2, M3 Subjects: adults receiving long-term (≥8 weeks) benefits, employed and unemployment, unlikely to RTW within three months CG: standard management; n: M1 = 489; M2 = 539; M3 = 129 IG: Multidisciplinary, coordinated and tailored RTW; n: M1 = 747; M2 = 809; M3 = 392 FU: 12 months | YES The effect was different in the 3 municipalities and across time frames within each site. In the municipality with the most complex cases, people in the intervention group showed an increased rate of recovery from long-term sickness absence (HR 1.51, 95% CI 1.31–1.74). RELEVANT OUTCOMES (1) recovery from sickness absence Recovery from sickness absence: first week where no sickness absence benefit was given. | Women: 49.5–62.8%. Data collection: 2010–2011. The municipalities are obliged by law to conduct an assessment of every sick-listed beneficiary by the end of the 8th week of sickness absence. At this assessment, beneficiaries are assigned to one of three categories:
CG: ordinary sickness benefit management. IG: Intervention includes designated RTW coordinators and multidisciplinary teams. Work accommodation by health providers was used when appropriate. |
| Part-Time Sick Leave (PTSL)/Part-Time Sick Benefits | |||
| Høgelund J. 2012 Denmark [22] | Strategy: part-time sick leave Design: cohort, survey and register-based Subjects: people with health problems, employed and on SL >8 weeks CG: FTSL; n = n.r. IG: PTSL; n = n.r. Total sample: 226 with mental health issues and 638 with other disorders FU: up to 79 weeks | YES PTSL significantly reduced the duration of SL for employees with health problems other than mental health issues. RELEVANT OUTCOMES (1) time until first return to regular working hours (RWH) RWH: time until the sick benefit ends because the employee report being ready for return to pre-sick leave hours (examples of reasons to end the sick benefit not considered RWH: receipt of disability benefit, flexijob employment, vocational rehabilitation, end of the normal one-year sickness benefit). | Women: employees with non-mental disorders 61% in PTSL and 55% in FTSL. The benefit cases were closed from 1 January through 31 July 2006. These individuals were interviewed by telephone from March through May 2007, on average ten months after their benefit case ended (and the payment of sickness benefit ceased) and 19 months after the sick leave spell started. |
| Markussen S. 2012 Norway [23] | Strategy: graded sickness-absence certificate Design: cohort, register-based Subjects: people on SL > 8 weeks CG: non-graded absence certificate; n = 261,596 IG: graded sickness-absence certificate before the end of week 8; n = 77,655 FU: 2 years | YES Persons with a graded long-term absence certificate showed significant shorter absence durations, less subsequent social security dependency, and higher employment rates (e.g., the expected number of work-days was reduced more than 90 days, the number of saved social security days was around 80–90 days, and the employment probability two years after the sick spell was about 16-fold higher compared to persons receiving a full-time absence certificate). RELEVANT OUTCOMES (1) number of days from the start to the stop of the absence spell (including holidays and days off), (2) number of lost full-time equivalent working days, (3) number of full equivalent days in social security during the 24 months following the end of the spell (4) employment in the 2nd year after starting the spell | Women: CG 53.0%; IG 67.8%. Data collection: 2001–2006. |
| Kausto J. 2012 Finland [24] | Strategy: partial sick leave Design: cohort, register-based Subjects: people with MHP, MSD, cancer and trauma; employed and on SL at least for 60 days, working full time before their leave period CG: FTSL; n = 28,380 IG: PTSL; n = 1047 FU: approx. 12–19 months | YES PTSL was associated with increased subsequent use of partial disability pension (8%, 95% CI 10% to 5%) and decreased use of full disability pension (6%, 95% CI 3% to 9%). The effect was stronger for men (5% and 10%, respectively). Overall results suggest enhanced work retention after PTSL. RELEVANT OUTCOMES (1) maintaining work Full disability pension as an indicator of leaving of the labour market and partial disability pension as indicator of retaining the job despite impaired work ability. | Women Analysis performed with all subjects: CG: 53%, IG: 72%. Analysis performed with matched sample CG: 72%, IG: 72%. Recipients of partial or full sickness benefit whose sick leave period had ended between 1 May and 31 December 2007 were included. |
| Kausto J. 2014 Finland [25] | Strategy: partial sickness leave Design: cohort, register-based Subjects: people with musculoskeletal diseases, mental disorders, traumas and tumours; employed and on SL at least for 60 days CG: FTSL; n = 56,574 (matched subsample, n = 1660) IG: PTSL; n = 1738 (matched subsample, n = 1660) FU: 12 months | YES Work participation in the IG decreased less than in the CG (difference = 5.3%, 95% CI 3.1% to 7.5%). A larger effect was seen in people aged 45–65 years. In analyses with matched subsamples the effect on work participation was stronger (difference = 9.8, 95% CI 5.9% to 13.7%) and shown in all age groups (16–65 years). RELEVANT OUTCOMES (1) work participation Work participation: time the individuals were likely to have participated in gainful employment; approximated as the proportion of time within 365 days when participants had an employment contract and did not receive either partial or full ill-health-related benefits or unemployment benefits. | Women Analysis performed with all subjects: CG: 53%, IG: 71%. Individuals who had received either partial sickness benefit or full sickness benefit in 2007–2008 and whose compensated sickness absence period had ended between 1 January and 31 December 2008 were included. Analyses for the whole population were adjusted for age, sex, income, diagnosis, occupational group, insurance district. Further analyses were performed for matched subsamples similar in age, gross income, number of unemployment days, sickness absence days, rehabilitation days or work participation before the intervention. |
| Notification of Sickness Absence | |||
| Halonen J. 2016 Finland [26] | Strategy: legislative changes obligating notification of prolonged sickness absence and assessment of remaining work (“30-60-90 day rule”) Design: cohort, register-based Subjects: public-sector employees with permanent job contract and on SL for at least 30 calendar days Cohort 1 (reference) n = 6393 Cohort 2 (pre-intervention) n = 6011 Cohort 3 (intervention) n = 5708 FU: 12 months | YES Workers who had been 60 days on sick leave returned to work earlier after introduction of the “30-60-90 day rule” (p = 0.017). The gain in work participation was larger for women than for men (287.8 vs. 70.4 persons-years/10,000 employees) and for the low than the high job status group (409.7 vs. −30.4). The effects diluted over time. RELEVANT OUTCOMES (1) sustainable RTW after 30, 60 and 90 SL-days, (2) monthly work participation after 30, 60 and 90 SL-days (3) gain in annual work participation after 30, 60 and 90 SL-days Sustainable RTW: a minimum of 28 consecutive working days after the sick absence. | Women: approximately 75% (most participants were women due to the nature of public sector jobs in Finland). Three cohorts: 2008/9 (reference), 2010/11 (pre-intervention), 2013/14 (post-intervention). Covariates: sex, age and occupational status. The total sickness absence rates declined from 2008 until 2013 in both the public and the private sector. The gains in work participation days were larger during the intervention than the reference period, suggesting a beneficial effect of the legislative changes. |
| (B) Musculoskeletal Disorders | |||
| Multidisciplinary Interventions | |||
| Steiner A.S. 2013 Switzerland [27] | Strategy: multidisciplinary functional rehabilitation program Design: controlled trial Subjects: non-specific LBP CG: muscle reconditioning program (MRP); n = 21 IG: Multidisciplinary functional rehabilitation program (MFRP); n = 24 FU: 9 months | UNCLEAR After excluding subjects not employed or not searching for a job (e.g., housewives or early retirements), more people in the IG were working at follow-up (78% vs. 47%) but the difference was not significant. RELEVANT OUTCOMES (1) RTW (not further described) | Women: CG 52%, IG 42%. Data collection: CG mid-2006-mid 2007, IG end of 2007 to 2008 Intervention: It integrated physical rehabilitation, psychological evaluation, cognitive behavioural methods and occupational therapy with a socio-professional component. Participants in the CG received MRP, the former standard treatment at the study clinic. After the center replaced MRP by MFRP, the IG received the new standard treatment. |
| Jensen C. 2011 Denmark [28] | Strategy: multidisciplinary tailored coordinated intervention Design: RCT Subjects: LBP, employed and on SL for 3–16 weeks IG1: Brief intervention (clinical examination and advise); n = 175 IG2: Multidisciplinary tailored coordinated intervention; n = 176 FU: 12 months | NO There were no differences in number of subjects who achieved RTW (76.0% in IG1 and 71.0% in IG2) and time to RTW (14 weeks in IG1 and 18 weeks in IG2). RELEVANT OUTCOMES (1) RTW (2) Median time until RTW RTW: first 4-week period within the first year after inclusion without social transfer payments; unemployed participants were classified as “RTW,” if they had lost their job during follow-up, but were healthy enough to work, which was a prerequisite to receive unemployment benefits. | Women: CG 50%, IG 54%. Recruitment: November 2004–June 2007. Multidisciplinary Intervention: Clinical examination and advice by a rehabilitation doctor and a physiotherapist; assignment of a case manager, who develops a rehabilitation plan in collaboration with the patient and a multidisciplinary team; the workplace and the social service center are contacted to discuss and coordinate relevant initiatives; the case manager arranges meetings between the participant and each of the other specialists, meetings at the work place and meetings with the social service centre, if relevant. Sample: Specific and non-specific LBP; 56% unskilled worker; >80% wished to get back to same work. |
| Jensen C. 2012 Denmark [29] (same study as Jensen C. 2011) | Strategy: multidisciplinary tailored coordinated intervention Impact of the interventions on sick leave weeks and on different subgroups explored; longer FU than Jensen 2011 FU: 24 months | YES—SUBGROUP DIFFERENCES Results for the general sample: at the two-year follow-up, no statistically significant difference between the brief intervention group and the multidisciplinary group was found. Results for subgroups of patients:
RELEVANT OUTCOMES (1) time to RTW at 1 and 2 years (2) RTW during follow up (3) work status at 1 and 2 years (4) SL weeks (partial or full) at 1 and 2 years RTW: 4-week period without sick or other health-related benefitsOnly sick leave spells of ≥2 weeks were considered | |
| Stapelfeldt C.M. 2011 Denmark [30] (same study as Jensen C. 2011) | Strategy: multidisciplinary tailored coordinated intervention Secondary analyses to identify subgroups that would benefit more from the multidisciplinary intervention; FU considered: 12 months. It also analyses data from further 120 subjects (IG1 n = 60; IG2 n = 60) | YES—SUBGROUP DIFFERENCES When claimants were excluded from the analyses, the multidisciplinary intervention was more effective in the subgroup of participants with low job satisfaction and in subgroups characterised by no influence on work planning and groups at risk of losing their job. Participants with high job satisfaction and those who were able to influence the planning of their work and who had no risk of losing their job benefited more from the brief intervention. RELEVANT OUTCOMES (1) RTWRTW: no sick leave compensation for a period of 4 consecutive weeks. | |
| Vermeulen S. 2011 The Netherlands [31] | Strategy: multidisciplinary intervention promoting involvement of stakeholders Design: RCT Subjects: MSD, unemployed and temporary agency workers on SL 2 to 8 weeks CG: usual care; n = 84 IG: multidisciplinary intervention; n = 79 FU: 12 months | YES The results indicated a non-significant trend towards delayed RTW in the IG in the first 90 days, followed by a significant advantage in RTW rate after 90 days (HR 2.24; (95% CI 1.28–3.94). The intervention had a negative impact on sickness benefit duration, although not statistically significant. This was due to the fact that in most cases the therapeutic workplaces were offered with ongoing sickness benefit. RELEVANT OUTCOMES (1) time to sustainable first RTW at 3, 6, 9 and 12 months (2) time to first sustainable ending of sickness benefit (3) total number of days of sickness benefit at 3, 6, 9 and 12 months Sustainable first RTW: days from randomisation to work in any type of paid work or work resumption with ongoing benefits for at least 28 consecutive days. First sustainable ending of sickness benefit: duration in calendar days from the day of randomization until ending of sickness benefit for at least 28 days. Recurrence of sickness absence with an accepted sickness benefit claim within 28 days after ending of the previous sickness benefit was considered as belonging to the preceding sickness benefit period, on condition that it was due to the same (or related) MSD. | Women: CG 37%, IG 43%. Recruitment: March 2007–September 2008. Comparison: assessment and management of vocational rehabilitation carried out by an insurance physician, a labour expert and a case-manager. Intervention: a RTW coordinator work to stimulate a high degree of involvement of both the sick-listed worker and the labour expert (representing the Social Security Agency), and to reach consensus about a RTW plan. A vocational rehabilitation agency was contracted to find a suitable (therapeutic) workplace matching with the formulated RTW plan. Sample: Volunteers (/interested in participation). |
| Educational Strategies | |||
| Du Bois M. 2012 Belgium [32] | Strategy: Information and advice to stay active by medical advisers during after a disability evaluation Design: RCT Subjects: LBP, employed and in SL CG: disability evaluation; n = 257 IG: disability evaluation followed by information and advice; n = 252 FU: 12 months | YES This intervention was more effective in the long term. Less people in the IG were off work (4% vs. 8%) or had episodes of SL (15% vs. 23%) after 12 months. Time until recurrent SL was lower in the IG (59 vs. 71 days). RELEVANT OUTCOMES (1) RTW rate at 3 and 12 months (2) episodes of sick leave for LBP at 3 and 12 months (3) sick leave duration (mean number of days off work) (4) time until recurrent sick absence | Women: CG 40%, IG 46%. Recruitment: March 2008–September 2008. Comparison: brief disability evaluation without medical advice. Intervention: disability evaluation followed by information and advice (education about nature and course of the disease and about physical and psychological factors involved; encouragement of participants to adopt an active role). |
| Work-Focused Interventions | |||
| Jensen L.D.2012Denmark[33] | Strategy: Counselling addressing workplace barriers and physical activity Design: RCT Subjects: LBP, employed and expressing concerns about the ability to maintain their current job CG: usual care; n = 150 IG: counselling addressing workplace barriers and physical activity; n = 150 FU: 3 months | UNCLEAR The intervention had a significant effect for self-reports of SL due to LBP for more than 8 weeks (RR 11.78; 95% CI 1.56 to 88.96) and for cumulated SL days due to LPB (RR 2.57; 95% CI 1.52 to 4.37) without considering the approx. 25% loss to FU. However, per register data on SL of more than 2 weeks due to all causes (outcomes available for all participants), there was no significant difference between the CG and the IG (with and without considering patients lost to FU). RELEVANT OUTCOMES (1) proportion of patients accumulating 8 weeks of sick leave (2) duration of sick leave | Women (based on individuals who completed baseline and follow up): CG (n = 114) 59%, IG (n = 110) 51%. Recruitment: November 2006–April 2009. Intervention: counselling by an occupational physician, aiming at removing experienced workplace barriers as well as at enhancing physical activity of moderate intensity, on pain, function and sick leave after 3 months. Two counselling sessions integrated in LBP secondary care and one workplace visit, if necessary to evaluate the work conditions. Comparison: Usual care would typically consist of a brief instruction in exercises, or readmission to a general practitioner for further contact with a physiotherapist or chiropractic treatment. |
| Myhre K. 2014 Norway [34] | Strategy: work-focused intervention additional to multidisciplinary intervention Design: RCT Subjects: neck and back pain, employed, on sick leave between 4 and 12 weeks CG: multidisciplinary intervention (brief or comprehensive); n = 202 IG: additional work-focused intervention; n = 203 FU: 12 months | NO ADDED VALUE TO A MULTIDISCIPLINARY INTERVENTION Adding work-focus in specialist care did not result in better effect of multidisciplinary interventions. The intervention was not significantly more successful in decreasing time to RTW (except for subjects ≥ 41 y). The intervention had no effect on the total number of subjects achieving RTW. But the work-focused intervention was not inferior to interventions that focus on physical activity and pain. RELEVANT OUTCOMES (1) number of days until sustainable RTW (2) RTWS ustainable RTW: first 5-week period after random assignment without sickness benefits, a work assessment allowance pension, or a disability pension. RTW was designated when patients receiving a partial disability pension prior to inclusion returned to their partial disability. | Women: CG 49%, IG 44%. Recruitment: August 2009–August 2011. Intervention: a case worker analyses together with the patient work and RTW difficulties; they develop a RTW schedule and discuss relevant issues for a meeting with the employer; if sick-leave compensation is an issue, the caseworkers contact municipal social services. |
| Marchand G.H. 2015 [35] (same study as Myhre K. 2014) | Secondary analysis to explore secondary clinical outcomes and the influence of some factors on primary and secondary outcomes. | SUPPORT FOR DIFFERENTIAL SUBGROUP EFFECTS Younger age, low anxiety score and improvement in fear avoidance beliefs of work were positive predictors of RTW in IG as well as in CG. | |
| Shiri R. 2011 Finland [36] | Strategy: Early ergonomic intervention Design: RCT Subjects: upper-extremity pain (different diagnoses), employed CG: Standard medical care; n = 86 IG: early ergonomic intervention; n = 91 FU: 12 months | UNCLEAR The results suggested that an early ergonomic intervention reduces sickness absence due to any MSD. During the 4–12-month period, the number of people with sickness absence due to any MSD was lower in the IG when diagnosed by a nurse (1% vs. 8%, p = 0.02) and when certified by physician or nurse (20% vs. 32%, p = 0.07). The number of days in sick absence due to any MSD diagnosed by a nurse was significantly lower in the IG when diagnosed by a nurse (p = 0.02) but not when certified by physician or nurse (p = 0.57). RELEVANT OUTCOMES (1) employees with sick absence in first 3 months and in 4–12 months, (2) sickness absence days in first 3 months and in 4–12 months | Women: 87.3%. Study period: February 2006–December 2007 Intervention: After the clinical examination, the physician contacts the employer, and a visit by the occupational physiotherapist is scheduled. The workplace is assessed and possible changes to achieve an ergonomic improvement discussed with the employee and supervisor. |
| Part-Time Sick Leave (PTSL) | |||
| Viikari-Juntura E. 2012 Finland [37] | Strategy: Part-time sick leave Design: RCT Subjects: persons with MSD (neck, shoulders, back and extremities), in SL CG: FTSL; n = 31 IG: PTSL; n = 31 FU: 12 months | UNCLEAR Results suggested better work participation outcomes after PTSL compared with FTSL. Workers on PTSL achieved sooner RTW that sustained at least 4 weeks (12 versus 20 days, p = 0.10; adjusted HR = 1.84, 95% CI 1.20–2.82). The number of sickness absence days along the 1-year follow up and the number of recurrent sick leaves per person was about 20% lower in the IG (level of significance not reported). Time to first recurrent sick leave was similar in both groups. RELEVANT OUTCOMES (1) time to sustained RTW (2) number of PTSL-days at 6 time points during 12 month follow-up, (3) number of FTSL-days, (4) proportion of potential work time of the sick days, (5) number of recurrent sick spells per person year, (6) time after end of initial sick leave to the first recurrent sick spell Sustained RTW: the worker continued to work without recurrent sick leave ≥2 weeks or ≥4 weeks after the end of part- or full-time sickness absence. | Women: CG 97%, IG 97%. Recruitment: November 2006–December 2009. Partial sickness allowance was introduced in Finland in 2007. Once introduced, the benefit could be used only after uninterrupted full-time sick leave for >60 working days up to 2010. Research funds were used to compensate the employers for part-time sick leave. |
| Andren D. 2012 Sweden [38] | Strategy: part-time sick leave Design: cohort study, register-based Subjects: MSD, employed and in SL CG: FTSL; n = 1037 IG: PTSL; n = 133 FU: 330 days | YES Workers had a 0.25 higher likelihood of full recovery if assigned to PTSL than FTSL. The average treatment effect of PTSL was 25%. RELEVANT OUTCOMES (1) RTW with full recovery of lost work capacity. | Women: 60%. Selection of subjects: February 2001. PTSL: individuals are covered by the sickness insurance with 25, 50, or 75% sick leave. |
| Author Year | Country | Targeted Population | Strategy (Name) | Strategy (Description) | Multidisciplinary | Interagency/Collaboration | Individualized | Early Intervention | Education Participants | Education Others | Self-Management | Workplace Involved | PTSL Allowed | Data Support Effect on Outcomes |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Agovino M. 2015 [14] | Italy | Mixed, people with disability | Flexicurity | Combination of labour market flexibility and high levels of social security. | Yes | |||||||||
| Lopez Frutos E.M. 2015 [19] | Spain | Mixed, people with a certificate of disability | Disability support benefit | Disability support benefits provide monthly allowances while, at the same time, requiring the individual to find a job different to the position they had before the disability. | No | Yes | No | |||||||
| Halonen J. 2016 [26] | Finland | Public employees with permanent job contract, on sick leave for ≥30 calendar days | Law- mandated notification of prolonged sick leave (“30-60-90 day rule”) | The legislative change emphasize early notification of both the Occupational Health Service (OHS) and the Social Insurance Institution of prolonged sickness absence as well as the collaboration of the employee, the OHS and the employer in the assessment of possibilities to continue working. | Yes | Yes | Yes | Yes | Yes | Yes | ||||
| Kausto J. 2012 [24] | Finland | Employed and on long-term sick leave | Partial sick leave | Partial sick leave is indicated if part-time work is not supposed to hinder recovery. It cannot exceed 72 days. Use is voluntary and the decision is taken in collaboration by the patient, the employer and the physician. | Yes | Yes | Yes | Yes | ||||||
| Kausto J. 2014 [25] | Finland | Employed and on long-term sick leave | Partial sick leave | Partial sick leave is indicated if part-time work is not supposed to hinder recovery. It cannot exceed 72 days. Use is voluntary and the decision is taken in collaboration by the patient, the employer and the physician. | Yes | Yes | Yes | Yes | ||||||
| Markussen S. 2012 [23] | Norway | Employed and on long term sick leave | Graded sickness absence certificate | Graded sickness absence certificate within the first 8-weeks of sickness absence and for up to 8-weeks. | Yes | Yes | In part | Yes | Yes | |||||
| Høgelund J. 2012 [22] | Denmark | Employed and on long-term sick leave (> 8 weeks) | Part-time sick leave | Part-time sick leave allows employees on full-time sick leave to work temporarily at reduced working hours. The employer and the employee must make an agreement about the job contents and working hours. Employee receives the normal hourly wage for the hours worked and sickness benefit for the hours off work, and may gradually increase working hours. | Yes | Yes | Yes | Yes | ||||||
| Johansson P. 2012 [20] | Sweden | Employed and unemployed sick-listed individuals at risk of becoming long-term sick | Resursteam | Multidisciplinary collaboration program consisting of an early and holistic evaluation of the need for rehabilitation. Collaboration between the Social insurance Agency and the primary health care. | Yes | Yes | Yes | Yes | No | Yes | No | |||
| Poulsen O. 2014 [21] | Denmark | Working-age adults with a disability receiving long-term sickness benefits (>8 weeks) | Multidisciplinary, coordinated and tailored RTW intervention | Intervention includes designated RTW coordinators and multidisciplinary teams. Work accommodation by health providers was used when appropriate | Yes | Yes | Yes | Yes | Yes | Yes |
| First Author Year | Country | Targeted Population | Strategy (Name) | Strategy (Description) | Multidisciplinary | Interagency Collaboration | Individualized | Early Intervention | Education Participants | Education Others | Self-Management | Workplace or Employer Involved | PTSL Allowed | Data Support Effect on Outcomes |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Du Bois M. 2012 [32] | Belgium | Employees, sick listed (> one month) with LBP | Information and advice | Information and advice to stay active by medical advisers after a disability evaluation. | Yes | Yes | Yes | Yes | ||||||
| Jensen L.D. 2012 [33] | Denmark | Employed LBP patients expressing concerns about the ability to maintain their current job | Counselling | Counselling by an occupational physician addressing experienced workplace barriers and physical activity. | Yes | Yes | Yes | Yes | Yes | Yes | Unclear | |||
| Vermeulen S. 2011 [31] | The Netherlands | Unemployed and temporary agency workers; back, neck, other pain | Multidisciplinary intervention | Stepwise communication process to identify and solve obstacles for return to work, resulting in a consensus-based plan. The role of the return to work coordinator is to stimulate a high degree of involvement of both the sick-listed worker and the labour expert. A vocational rehabilitation agency was contracted to find a suitable workplace matching with the RTW plan. | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | ||
| Jensen C. 2011 Jensen C. 2012 Stapelfeldt C.M. 2011 [28,29,30] | Denmark | Employees, sick listed with LBP for 3 to 16 weeks | Multidisciplinary intervention | Examination by a rehabilitation doctor and a physiotherapist and reassuring explanations. A case manager conducts a comprehensive interview and designs a tailored rehabilitation plan to be discussed in the multidisciplinary team; the case manager contacts the work place and the municipal job centre to discuss and coordinate initiatives. | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No(Jensen C. 2011) Yes, per group (Jensen C. 2012 and Stapelfeldt C.M. 2011) | |
| Viikari-Juntura E. 2012 [37] | Finland | Employed, sick-listed with MSDs | Part-time sick leave | Reduced work hours with task modification, if required. | Yes | Yes | Yes | Yes | Unclear | |||||
| Shiri R. 2011 [36] | Finland | Employed; seeking help for upper-extremity pain (different diagnoses) | Ergonomic intervention | Ergonomic intervention. After the clinical examination, the physician contacts the employer, and a visit by the occupational physiotherapist is scheduled. The workplace is assessed and possible accommodations discussed with the employee and supervisor. | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Unclear | ||
| Myhre K. 2014 Marchand G.H. 2015 [34,35] | Norway | Employed neck and back pain patients, sick-listed for 1 to 12 months and referred to secondary care | Work-focused rehabilitation | A case worker analyses together with the patient work and RTW difficulties; they develop a RTW schedule; they and discuss relevant issues for a meeting with the employer; if sick-leave compensation is an issue, the caseworkers contact municipal social services. | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No added value to multidisciplinary intervention (2014) Support for subgroup effects(2015) | ||
| Steiner A.A. 2013 [27] | Switzerland | Persons with chronic LBP, non-specific LBP with or without radiating leg pain | Multidisciplinary functional rehabilitation program | Sessions included: (1) cardiorespiratory fitness, muscular strength, muscular flexibility, stabilization exercises, relaxation, proprioception and water gymnastics; (2) occupational therapy with emphasis on individual professional and daily life situations; (3) patient education sessions based on a non-injury model and the biopsychosocial model; and (4) one hour per week of support group led by a psychiatrist. Personalized, realistic and measurable objectives were defined individually. | Yes | Yes | Yes | Yes | Intervention at the workplace not possible for all participants | Unclear |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sabariego, C.; Coenen, M.; Ito, E.; Fheodoroff, K.; Scaratti, C.; Leonardi, M.; Vlachou, A.; Stavroussi, P.; Brecelj, V.; Kovačič, D.S.; et al. Effectiveness of Integration and Re-Integration into Work Strategies for Persons with Chronic Conditions: A Systematic Review of European Strategies. Int. J. Environ. Res. Public Health 2018, 15, 552. https://doi.org/10.3390/ijerph15030552
Sabariego C, Coenen M, Ito E, Fheodoroff K, Scaratti C, Leonardi M, Vlachou A, Stavroussi P, Brecelj V, Kovačič DS, et al. Effectiveness of Integration and Re-Integration into Work Strategies for Persons with Chronic Conditions: A Systematic Review of European Strategies. International Journal of Environmental Research and Public Health. 2018; 15(3):552. https://doi.org/10.3390/ijerph15030552
Chicago/Turabian StyleSabariego, Carla, Michaela Coenen, Elizabeth Ito, Klemens Fheodoroff, Chiara Scaratti, Matilde Leonardi, Anastasia Vlachou, Panayiota Stavroussi, Valentina Brecelj, Dare S. Kovačič, and et al. 2018. "Effectiveness of Integration and Re-Integration into Work Strategies for Persons with Chronic Conditions: A Systematic Review of European Strategies" International Journal of Environmental Research and Public Health 15, no. 3: 552. https://doi.org/10.3390/ijerph15030552
APA StyleSabariego, C., Coenen, M., Ito, E., Fheodoroff, K., Scaratti, C., Leonardi, M., Vlachou, A., Stavroussi, P., Brecelj, V., Kovačič, D. S., & Esteban, E. (2018). Effectiveness of Integration and Re-Integration into Work Strategies for Persons with Chronic Conditions: A Systematic Review of European Strategies. International Journal of Environmental Research and Public Health, 15(3), 552. https://doi.org/10.3390/ijerph15030552