Primary Care Comprehensiveness Can Reduce Emergency Department Visits and Hospitalization in People with Hypertension in South Korea


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
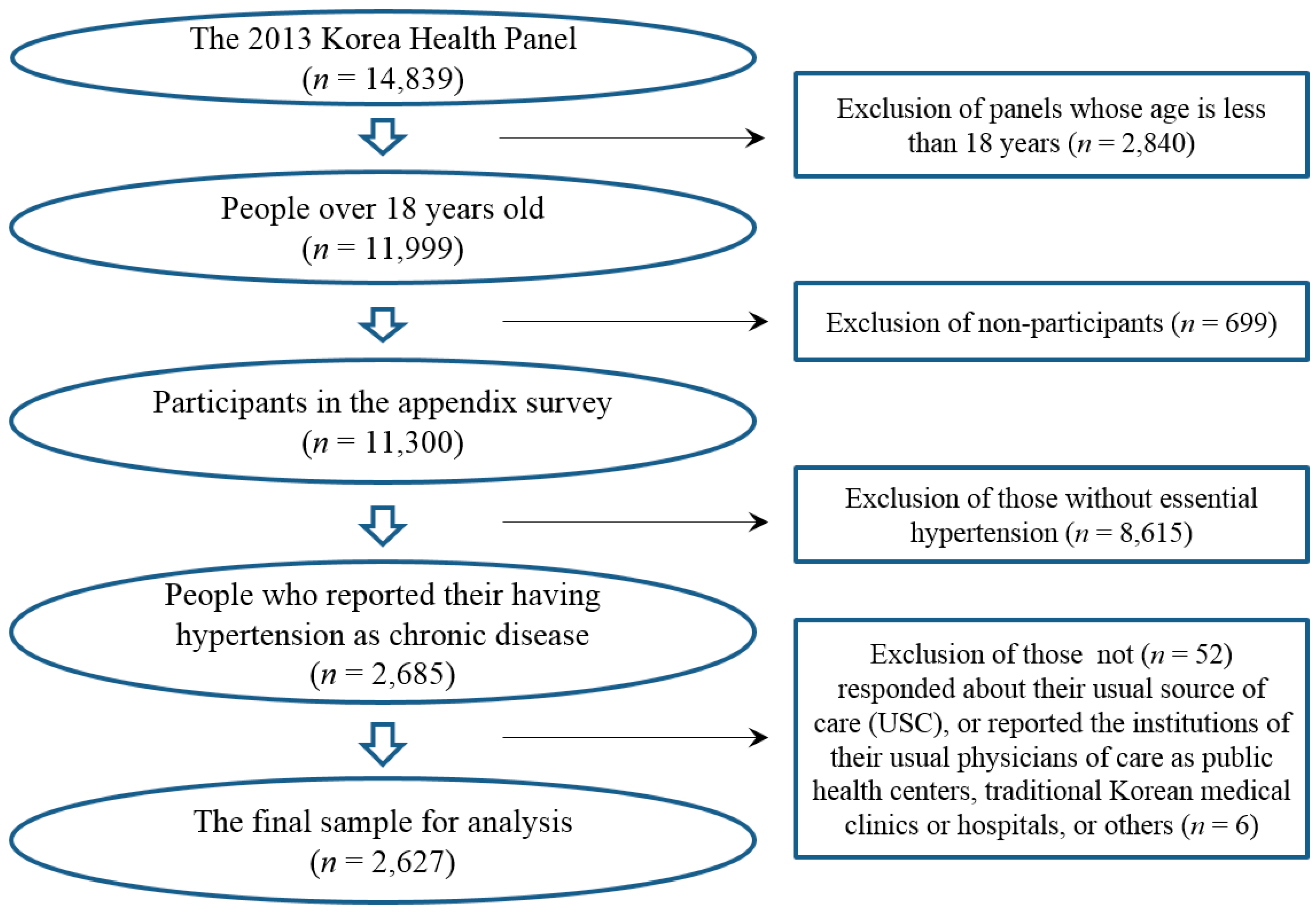
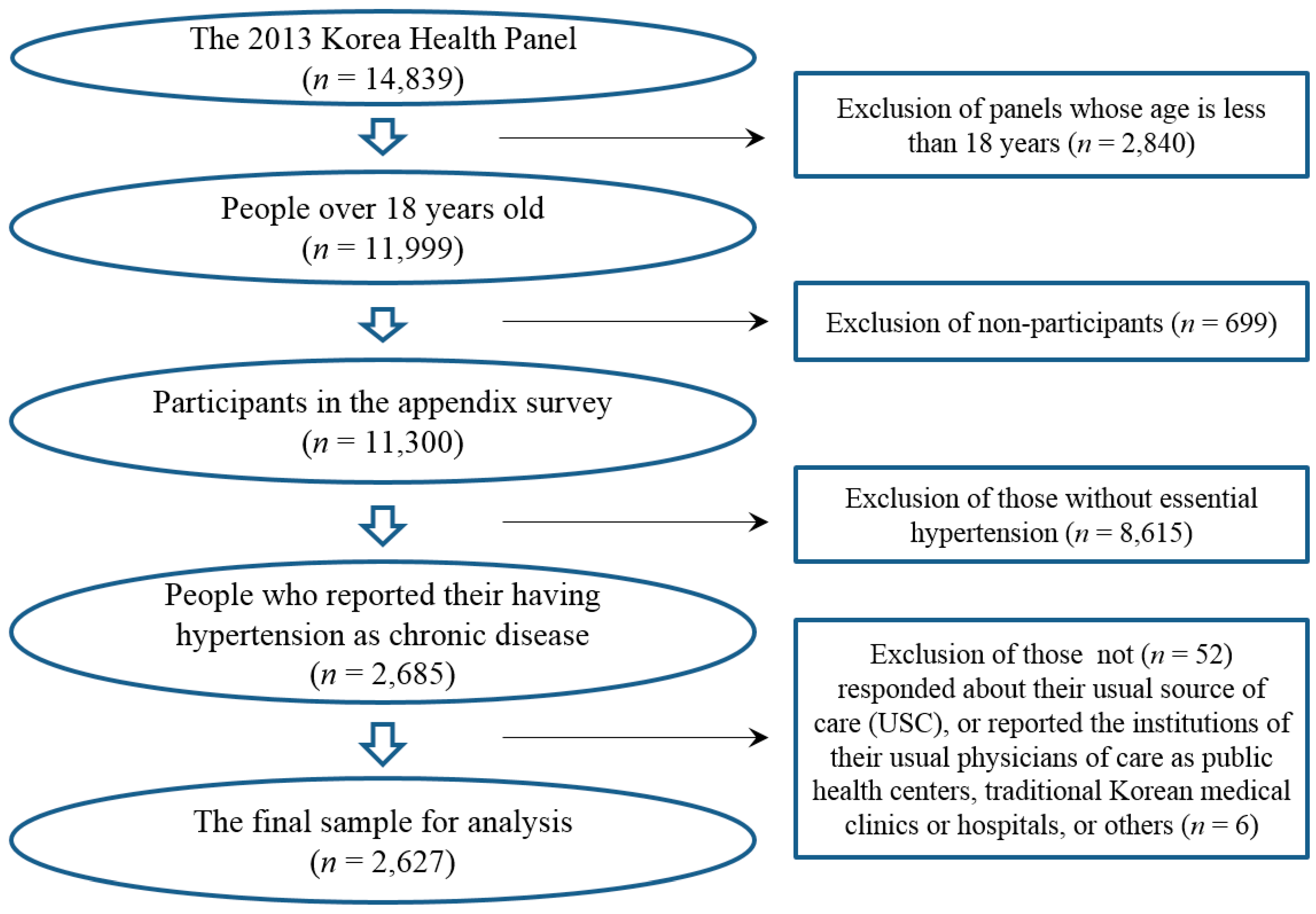
2.2. Sample Selection Process
2.3. Measurement
2.3.1. Sociodemographic Variables
2.3.2. Self-Rated Health Variable
2.3.3. Charlson Comorbidity Index
2.3.4. Variable of Interest
2.4. Statistical Analysis
3. Results
3.1. Sociodemographic Characteristics of Adults with Essential Hypertension by Types of Physicians as a Usual Source of Care
3.2. Adjusted ORs of Types of Physician as a USC for an Experience of ED Visits Within a Year
3.3. Adjusted ORs of Types of Physician as a USC for an Experience of Hospital Admission within a Year
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- GBD 2013 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 79 behavioral, environmental and occupational, and metabolic risk factors or clusters of risks in 188 countries, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 386, 2287–2323. [Google Scholar]
- Aronow, W.S. Treatment of systemic hypertension. Am. J. Cardiovasc. Dis. 2012, 2, 160–170. [Google Scholar] [PubMed]
- Korea Centers for Disease Control and Prevention. The Report of Korea National Health and Nutrition Examination Survey. 2015. Available online: https://knhanes.cdc.go.kr/knhanes/sub04/sub04_03.do?classType=7 (accessed on 18 December 2017).
- Yoon, S.S.; Carroll, M.D.; Fryar, C.D. Hypertension prevalence and control among adults: United States, 2011–2014. NCHS Data Briefs 2015, 220, 1–8. [Google Scholar]
- WHO EMRO. High Blood Pressure and the Role of Primary Health Care. Available online: http://www.emro.who.int/pdf/world-health-days/2013/phc-factsheet-2013.pdf?ua=1 (accessed on 18 December 2017).
- Manns, B.J.; Tonelli, M.; Zhang, J.; Campbell, D.J.; Sargious, P.; Ayyalasomayajula, B.; Clement, F.; Johnson, J.A.; Laupacis, A.; Lewanczuk, R.; et al. Enrolment in primary care networks: Impact on outcomes and processes of care for patients with diabetes. CMAJ 2012, 184, E144–E152. [Google Scholar] [CrossRef] [PubMed]
- US Department of Health & Human Services. Medical Expenditure Panel Survey (MEPS) Topics: Usual Source of Care. Available online: http://meps.ahrq.gov/mepsweb/data_stats/MEPS_topics.jsp?topicid=44Z-1 (accessed on 26 December 2017).
- Dinkler, J.M.; Sugar, C.A.; Escarce, J.J.; Ong, M.K.; Mangione, C.M. Does age matter? Association between usual source of care and hypertension control in the US population: Data from NHANES 2007–2012. Am. J. Hypertens. 2016, 29, 934–940. [Google Scholar] [CrossRef] [PubMed]
- Spatz, E.S.; Ross, J.S.; Desai, M.M.; Canavan, M.E.; Krumholz, H.M. Beyond insurance coverage: Usual source of care in the treatment of hypertension and hypercholesterolemia. Data from the 2003–2006 National Health and Nutrition Examination Survey. Am. Heart J. 2010, 160, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Starfield, B.; Shi, L. The medical home, access to care, and insurance: A review of evidence. Pediatrics 2004, 113, 1493–1498. [Google Scholar] [PubMed]
- Blewett, L.A.; Joonson, P.J.; Lee, B.; Scal, P.B. When a usual source of care and usual provider matter: Adult prevention and screening services. J. Gen. Intern. Med. 2008, 23, 1354–1360. [Google Scholar] [CrossRef] [PubMed]
- DeVoe, J.E.; Tillotson, C.J.; Wallace, L.S.; Lesko, S.E.; Pandhi, N. Is health insurance enough? A usual source of care may be more important to ensure a child to receive preventive health counseling. Matern. Child Health J. 2012, 16, 306–315. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.M.; Jeon, H.; Lee, J.H. Having a physician rather than a place as a usual source of care would be better—From 2012 Korea Health Panel Data. J. Korean Med. Sci. 2017, 32, 4–12. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.H. Assessment of primary care level in Korea and comparison with the developed countries. J. Korean Acad. Fam. Med. 2001, 22, 483–497. [Google Scholar]
- Im, G.J.; Min, H.Y.; Choi, J.W.; Lim, S.M.; Park, Y.H. Financial state of primary care physicians under the Korean insurance system. J. Korean Med. Assoc. 2011, 54, 98–111. [Google Scholar] [CrossRef]
- Kwon, S. Thirty years of national health insurance in South Korea: Lessons for achieving universal health care coverage. Health Policy Plan. 2009, 24, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Chun, C.B.; Kim, S.Y.; Lee, J.Y.; Lee, S.Y. Republic of Korea: Health system review. Health Syst. Trans. 2009, 11, 1–184. [Google Scholar]
- An, A.R.; Kim, K.; Lee, J.H.; Sung, N.J.; Lee, S.I.; Hyun, M.K. Having a usual source of care and its associated factors in Korean adults: A cross-sectional study of the 2012 Korea Health Panel Survey. BMC Fam. Pract. 2016, 17, 167. [Google Scholar] [CrossRef] [PubMed]
- Schoen, C.; Osborn, R.; Doty, M.M.; Bishop, M.; Peugh, J.; Murukutla, N. Toward higher-performance health systems: Adults’ health care experiences in seven countries, 2007. Health Aff. 2007, 26, w717–w734. [Google Scholar] [CrossRef] [PubMed]
- OECD. Health at a Glance 2017: OECD Indicators; OECD: Paris, France, 2017. Available online: http://dx.doi.org/10.1787/health_glance-2017-en (accessed on 26 December 2017).
- Jung, J.W.; Sung, N.J.; Park, K.H.; Kim, S.W.; Lee, J.H. Patients’ assessment of community primary and non-primary care physicians in Seoul city of South Korea. Korean J. Fam. Med. 2011, 32, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Eun, S.J.; Kim, H.J.; Jo, M.W. Finding the primary care providers in the specialist-dominant primary care setting of Korea: A cluster analysis. PLoS ONE 2016, 11, e0161937. [Google Scholar] [CrossRef] [PubMed]
- Korea Health Panel. About Korea Health Panel. Available online: https://www.khp.re.kr:444/eng/main.do (accessed on 26 December 2017).
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Deyo, R.A.; Cherkin, D.C.; Ciol, M.A. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J. Clin. Epidemiol. 1992, 45, 613–619. [Google Scholar] [CrossRef]
- Quan, H.; Sundararajan, V.; Halfon, P.; Fong, A.; Burnand, B.; Luthi, J.C.; Saunders, L.D.; Beck, C.A.; Feasby, T.E.; Ghali, W.A. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med. Care 2005, 43, 1130–1139. [Google Scholar] [CrossRef] [PubMed]
- Jung, K.W.; Won, Y.J.; Kong, H.J.; Oh, C.M.; Shin, A.; Lee, J.S. Survival of Korean adult cancer patients by stage at diagnosis, 2006–2010: National cancer registry study. Cancer Res. Treat. 2013, 45, 162–171. [Google Scholar] [CrossRef] [PubMed]
- Kang, C.; Lee, J.H.; Kim, D.K.; Lee, C.; Oh, J.H. Current status of having a usual source of care and its associated factors in Korean adults with hypertension. Korean J. Fam. Pract. 2018. forthcoming. [Google Scholar]
- Starfield, B. Primary Care: Balancing Health Needs, Services, and Technology; Oxford University Press: New York, NY, USA, 1998; pp. 181–183. [Google Scholar]
- Macinko, J.; Starfield, B.; Shi, L. The contribution of primary care systems to health outcomes within Organization for Economic Cooperation and Development (OECD) countries, 1970–1998. Health Serv. Res. 2003, 38, 831–865. [Google Scholar] [CrossRef] [PubMed]
- Starfield, B.; Shi, L.; Macinko, J. Contribution of primary care to health systems and health. Milbank Q. 2005, 83, 457–502. [Google Scholar] [CrossRef] [PubMed]
- Masseria, C.; Irwin, R.; Thomson, S.; Gemmill, M.; Mossialos, E. Primary Care in Europe (Policy Brief); London School of Economics and Political Science: London, UK, 2009. [Google Scholar]
- Kringos, D.S.; Boerma, W.G.W.; Hutchinson, A.; Saltman, R.B. Building Primary Care in a Changing Europe; WHO Regional Office for Europe: Copenhagen, Denmark, 2015. [Google Scholar]
- Mossialos, E.; Djordjevic, A.; Osborn, R.; Sarnak, D. (Eds.) International Profiles of Health Care Systems; The Commonwealth Fund: New York, NY, USA, 2017; Available online: http://www.commonwealthfund.org/publications/fund-reports/2017/may/international-profiles (accessed on 26 December 2017).
- Organization for Economic Cooperation and Development. OECD Reviews of Health Care Quality; Korea 2012: Raising Standards; OECD Publishing: Paris, France, 2012; Available online: http://www.oecd.org/publications/oecd-reviews-of-health-care-quality-korea-9789264173446-en.htm (accessed on 26 December 2017).
- Wu, S.; Wang, R.; Zhao, Y.; Ma, X.; Wu, M.; Yan, X.; He, J. The relationship between self-rated health and objective health status: A population-based study. BMC Public Health 2013, 13, 320. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Disease | Diagnostic Codes Compatible to the ICD-10 Coding in the KHP Data | CCI Score |
|---|---|---|
| Diabetes mellitus | E10–E14 | 1 |
| Myocardial infarct | I21, I22, I25 | 1 |
| Congestive heart failure | I50 | 1 |
| Peripheral vascular disease | I70–I79 | 1 |
| Cerebrovascular disease | I60–I69 | 1 |
| Dementia | F03, G30 | 1 |
| Chronic pulmonary disease | J41, J42, J43, J44, J45, J47, J64 | 1 |
| Rheumatic or connective tissue disease | M30–M36, M06 | 1 |
| Gastric or peptic ulcer | K25, K26 | 1 |
| Mild liver disease | B18, B19, K70–K77 | 1 |
| Hemiplegia or paraplegia | G80, G81, G82 | 2 |
| Moderate or severe renal disease | N17–N19 | 2 |
| Any malignancy, including lymphoma and leukemia, except basal cell cancer of skin | C00–C41, C43, C45–C72, C74, C75, C81–C96 | 2 |
| Metastatic solid tumor | C76–C80 | 6 |
| Acquired immune deficiency syndrome | B20-B24 | 6 |
| Variables | Total | Not Having a Usual Physician | Comprehensive CCPs | Non-Comprehensive CCPs | Hospital Specialists | p | |
|---|---|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | n (%) | |||
| Age | 18–49 | 224 (12.1) | 144 (12.7) | 45 (11.4) | 15 (12.9) | 20 (9.6) | 0.370 |
| 50–64 | 756 (37.1) | 457 (36.0) | 155 (36.8) | 52 (44.8) | 92 (39.1) | ||
| 65– | 1647 (50.8) | 1024 (51.3) | 352 (51.9) | 83 (42.3) | 188 (51.3) | ||
| Sex | Male | 1166 (46.8) | 728 (47.2) | 226 (43.5) | 64 (45.0) | 148 (52.0) | 0.201 |
| Female | 1461 (53.2) | 897 (52.8) | 326 (56.5) | 86 (55.0) | 152 (48.0) | ||
| Education (year) | –6 | 1196 (38.9) | 759 (40.3) | 249 (38.1) | 63 (34.9) | 125 (35.0) | 0.132 |
| 7–12 | 1097 (45.0) | 670 (43.9) | 240 (48.4) | 59 (42.5) | 128 (46.4) | ||
| 13– | 334 (16.1) | 196 (15.8) | 63 (13.5) | 28 (22.6) | 47 (18.6) | ||
| Household income (quintile) (missing, 1) | 1st (the lowest) | 765 (24.2) | 460 (23.4) | 199 (29.9) | 32 (18.9) | 74 (21.3) | 0.225 |
| 2nd | 599 (20.9) | 378 (21.1) | 116 (19.6) | 38 (22.3) | 67 (21.7) | ||
| 3rd | 507 (19.7) | 329 (20.4) | 91 (18.1) | 32 (21.6) | 55 (17.6) | ||
| 4th | 410 (17.7) | 242 (17.0) | 86 (18.2) | 25 (17.5) | 57 (20.7) | ||
| 5th (the highest) | 345 (17.5) | 216 (18.1) | 60 (14.2) | 22 (19.7) | 47 (18.7) | ||
| Marital status | Married | 1891 (74.0) | 1175 (74.0) | 389 (72.8) | 109 (77.4) | 218 (74.7) | 0.767 |
| Others 1 | 736 (26.0) | 450 (26.0) | 163 (27.2) | 41 (22.6) | 82 (25.3) | ||
| Health coverage (missing, 1) | Employed | 1696 (64.7) | 1055 (65.8) | 362 (65.9) | 94 (58.0) | 185 (60.1) | 0.029 |
| Self-employed | 690 (26.6) | 433 (26.1) | 137 (25.0) | 46 (36.2) | 74 (26.7) | ||
| Medical Aid or others 2 | 240 (8.7) | 136 (8.1) | 53 (9.1) | 10 (5.8) | 41 (13.2) | ||
| Self-rated health (missing, 99) | Good | 687 (28.0) | 443 (29.5) | 150 (29.2) | 31 (22.4) | 63 (21.8) | 0.018 |
| Moderate | 1119 (45.7) | 671 (45.2) | 252 (46.5) | 77 (52.7) | 119 (43.0) | ||
| Poor | 722 (26.3) | 438 (25.4) | 135 (24.3) | 39 (24.9) | 110 (35.2) | ||
| CCI score | 0 | 1445 (57.5) | 937 (59.7) | 320 (61.5) | 91 (63.2) | 97 (35.7) | <0.001 |
| 1 | 763 (28.1) | 449 (27.0) | 168 (28.3) | 43 (25.7) | 103 (34.5) | ||
| 2 or higher | 419 (14.4) | 239 (13.3) | 64 (10.2) | 16 (11.1) | 100 (29.8) | ||
| ED visit, yearly | Yes | 289 (10.6) | 188 (11.1) | 43 (7.1) | 14 (11.5) | 44 (13.9) | 0.033 |
| No | 2338 (89.4) | 1437 (88.9) | 509 (92.9) | 136 (88.5) | 256 (86.1) | ||
| Admission, yearly | Yes | 501 (17.2) | 307 (16.9) | 82 (12.5) | 27 (18.7) | 85 (26.7) | <0.001 |
| No | 2126 (82.8) | 1318 (83.1) | 470 (87.5) | 123 (81.3) | 215 (73.3) | ||
| Total | 2627 (100) | 1625 (100) | 552 (100) | 150 (100) | 300 (100) | ||
| Variables | Model 1 | Model 2 | |||||
|---|---|---|---|---|---|---|---|
| OR | 95% CI | p | OR | 95% CI | p | ||
| Age | 18–49 | 1 | 1 | ||||
| 50–64 | 0.64 | 0.39–1.04 | 0.073 | 0.62 | 0.37–1.02 | 0.057 | |
| 65– | 0.81 | 0.49–1.34 | 0.413 | 0.73 | 0.44–1.23 | 0.242 | |
| Sex | Male | 1 | 1 | ||||
| Female | 0.95 | 0.68–1.32 | 0.749 | 0.92 | 0.66–1.29 | 0.623 | |
| Education (year) | –6 | 1 | 1 | ||||
| 7–12 | 0.92 | 0.64–1.32 | 0.642 | 0.99 | 0.68–1.43 | 0.942 | |
| 13– | 0.92 | 0.54–1.59 | 0.771 | 1.07 | 0.62–1.85 | 0.810 | |
| Household income (quintile) (missing, 1) | 1st (the lowest) | 1 | 1 | ||||
| 2nd | 1.13 | 0.74–1.72 | 0.580 | 1.12 | 0.73–1.72 | 0.600 | |
| 3rd | 0.85 | 0.53–1.39 | 0.523 | 0.92 | 0.56–1.50 | 0.723 | |
| 4th | 1.27 | 0.79–2.06 | 0.326 | 1.36 | 0.83–2.21 | 0.222 | |
| 5th (the highest) | 0.73 | 0.41–1.28 | 0.269 | 0.75 | 0.42–1.33 | 0.328 | |
| Marital status | Married | 1 | 1 | ||||
| Others | 1.32 | 0.93–1.87 | 0.118 | 1.31 | 0.92–1.86 | 0.132 | |
| Health coverage (missing, 1) | Employed | 1 | 1 | ||||
| Self-employed | 0.98 | 0.69–1.37 | 0.890 | 0.97 | 0.69–1.37 | 0.856 | |
| Medical Aid or others 1 | 1.70 | 1.02–2.85 | 0.044 | 1.36 | 0.80–2.31 | 0.261 | |
| Self-rated health (missing, 99) | Poor | 1 | |||||
| Moderate | 0.52 | 0.37–0.73 | < 0.001 | ||||
| Good | 0.40 | 0.27–0.61 | < 0.001 | ||||
| Charlson Comorbidity Index score | 0 | 1 | |||||
| 1 | 0.85 | 0.59–1.21 | 0.362 | ||||
| 2 or higher | 1.48 | 1.00–2.20 | 0.052 | ||||
| Types of physicians as a USC | Not having a usual physician | 1 | 1 | ||||
| CCPs, comprehensive | 0.59 | 0.39–0.89 | 0.013 | 0.61 | 0.40–0.93 | 0.023 | |
| CCPs, non-comprehensive | 1.09 | 0.61–1.95 | 0.780 | 1.08 | 0.60–1.95 | 0.803 | |
| Hospital specialists | 1.26 | 0.83–1.91 | 0.275 | 1.11 | 0.73–1.71 | 0.623 | |
| Hosmer and Lemeshow goodness-of-fit test | p = 0.834 | p = 0.183 | |||||
| Concordance index | C = 0.606 | C = 0.650 | |||||
| Variables | Model 1 | Model 2 | |||||
|---|---|---|---|---|---|---|---|
| OR | 95% CI | p | OR | 95% CI | p | ||
| Age | 18–49 | 1 | 1 | ||||
| 50–64 | 1.73 | 1.01–2.99 | 0.048 | 1.64 | 0.95–2.83 | 0.078 | |
| 65– | 2.54 | 1.47–4.40 | 0.001 | 2.23 | 1.28–3.89 | 0.005 | |
| Sex | Male | 1 | 1 | ||||
| Female | 0.86 | 0.66–1.13 | 0.277 | 0.84 | 0.64–1.11 | 0.227 | |
| Education (year) | –6 | 1 | 1 | ||||
| 7–12 | 0.88 | 0.66–1.18 | 0.383 | 0.93 | 0.70–1.26 | 0.650 | |
| 13– | 0.55 | 0.34–0.89 | 0.015 | 0.60 | 0.37–0.98 | 0.041 | |
| Household income (quintile) (missing, 1) | 1st (the lowest) | 1 | 1 | ||||
| 2nd | 0.79 | 0.56–1.12 | 0.187 | 0.78 | 0.55–1.10 | 0.153 | |
| 3rd | 0.76 | 0.52–1.11 | 0.157 | 0.79 | 0.54–1.16 | 0.232 | |
| 4th | 0.82 | 0.55–1.23 | 0.335 | 0.85 | 0.57–1.28 | 0.441 | |
| 5th (the highest) | 0.71 | 0.46–1.11 | 0.138 | 0.75 | 0.48–1.17 | 0.203 | |
| Marital status | Married | 1 | 1 | ||||
| Others | 0.98 | 0.73–1.32 | 0.888 | 0.98 | 0.73–1.33 | 0.914 | |
| Health coverage (missing, 1) | Employed | 1 | 1 | ||||
| Self-employed | 0.84 | 0.63–1.11 | 0.221 | 0.81 | 0.60–1.08 | 0.143 | |
| Medical Aid or others 1 | 1.41 | 0.91–2.18 | 0.130 | 1.11 | 0.71–1.75 | 0.640 | |
| Self-rated health (missing, 99) | Poor | 1 | |||||
| Moderate | 0.64 | 0.48–0.84 | 0.001 | ||||
| Good | 0.49 | 0.35–0.68 | < 0.001 | ||||
| Charlson Comorbidity Index score | 0 | 1 | |||||
| 1 | 1.41 | 1.07–1.87 | 0.015 | ||||
| 2 or higher | 1.81 | 1.30–2.53 | < 0.001 | ||||
| Types of physicians as a USC | Not having a usual physician | 1 | 1 | ||||
| CCPs, comprehensive | 0.66 | 0.48–0.92 | 0.015 | 0.69 | 0.49–0.96 | 0.027 | |
| CCPs, non-comprehensive | 1.26 | 0.78–2.05 | 0.342 | 1.28 | 0.79–2.09 | 0.316 | |
| Hospital specialists | 1.80 | 1.29–2.51 | 0.001 | 1.52 | 1.07–2.14 | 0.018 | |
| Hosmer and Lemeshow goodness-of-fit test | p = 0.076 | p = 0.220 | |||||
| Concordance index | C = 0.622 | C = 0.663 | |||||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sung, N.-J.; Choi, Y.-J.; Lee, J.-H. Primary Care Comprehensiveness Can Reduce Emergency Department Visits and Hospitalization in People with Hypertension in South Korea. Int. J. Environ. Res. Public Health 2018, 15, 272. https://doi.org/10.3390/ijerph15020272
Sung N-J, Choi Y-J, Lee J-H. Primary Care Comprehensiveness Can Reduce Emergency Department Visits and Hospitalization in People with Hypertension in South Korea. International Journal of Environmental Research and Public Health. 2018; 15(2):272. https://doi.org/10.3390/ijerph15020272
Chicago/Turabian StyleSung, Nak-Jin, Yong-Jun Choi, and Jae-Ho Lee. 2018. "Primary Care Comprehensiveness Can Reduce Emergency Department Visits and Hospitalization in People with Hypertension in South Korea" International Journal of Environmental Research and Public Health 15, no. 2: 272. https://doi.org/10.3390/ijerph15020272
APA StyleSung, N.-J., Choi, Y.-J., & Lee, J.-H. (2018). Primary Care Comprehensiveness Can Reduce Emergency Department Visits and Hospitalization in People with Hypertension in South Korea. International Journal of Environmental Research and Public Health, 15(2), 272. https://doi.org/10.3390/ijerph15020272