Long-Term Weight Loss Effects of a Behavioral Weight Management Program: Does the Community Food Environment Matter?



 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data
2.2. Intervention
2.3. Research Design
2.4. Sample
2.5. Propensity Score Matching Procedure
2.6. Measures
2.6.1. Body Mass Index (BMI)
2.6.2. MOVE! Exposure
2.6.3. Community Food Environment Exposures
2.6.4. Covariates
2.7. Statistical Model
2.8. Sensitivity Analyses
3. Results
3.1. Descriptive Statistics
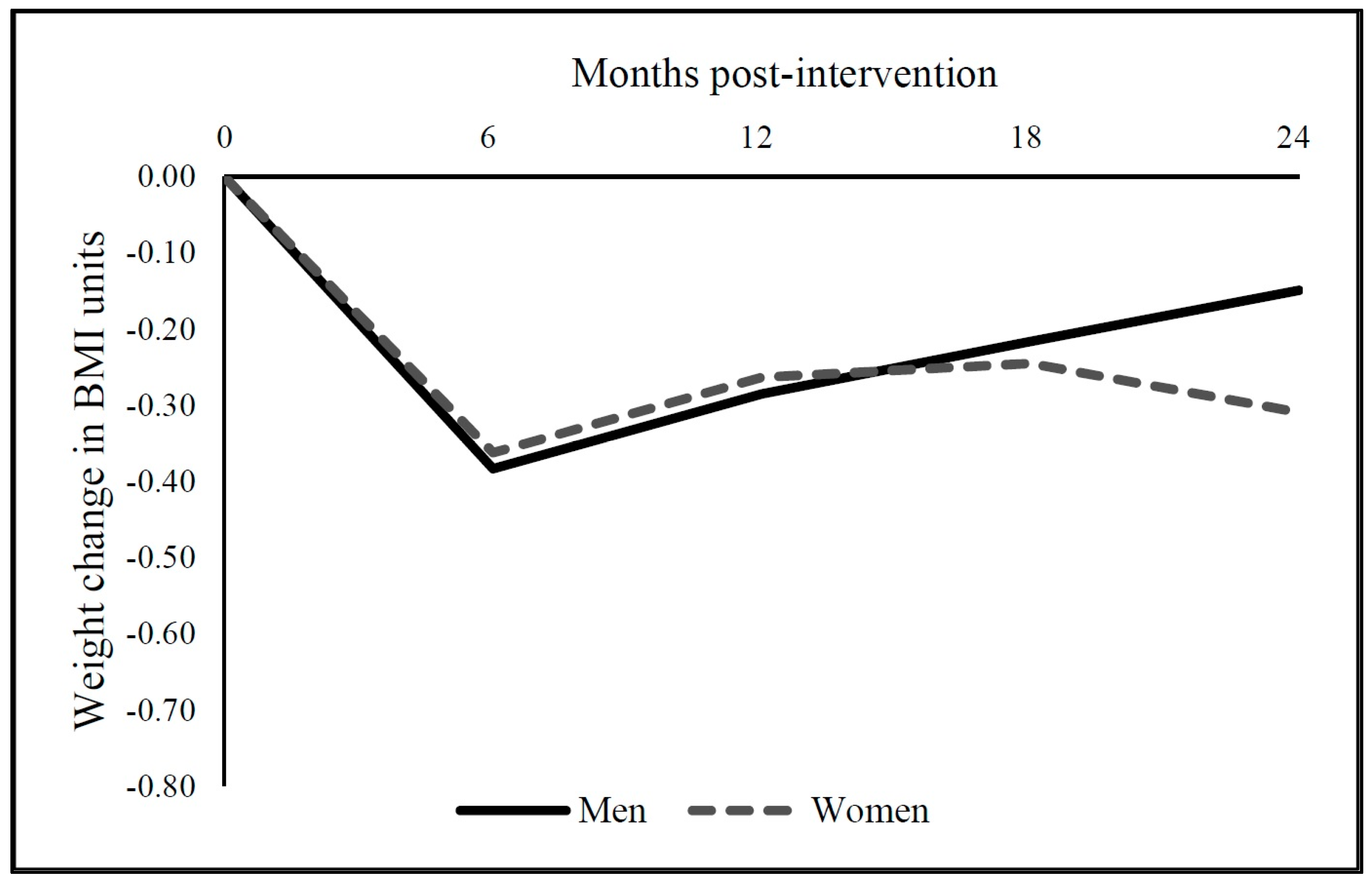
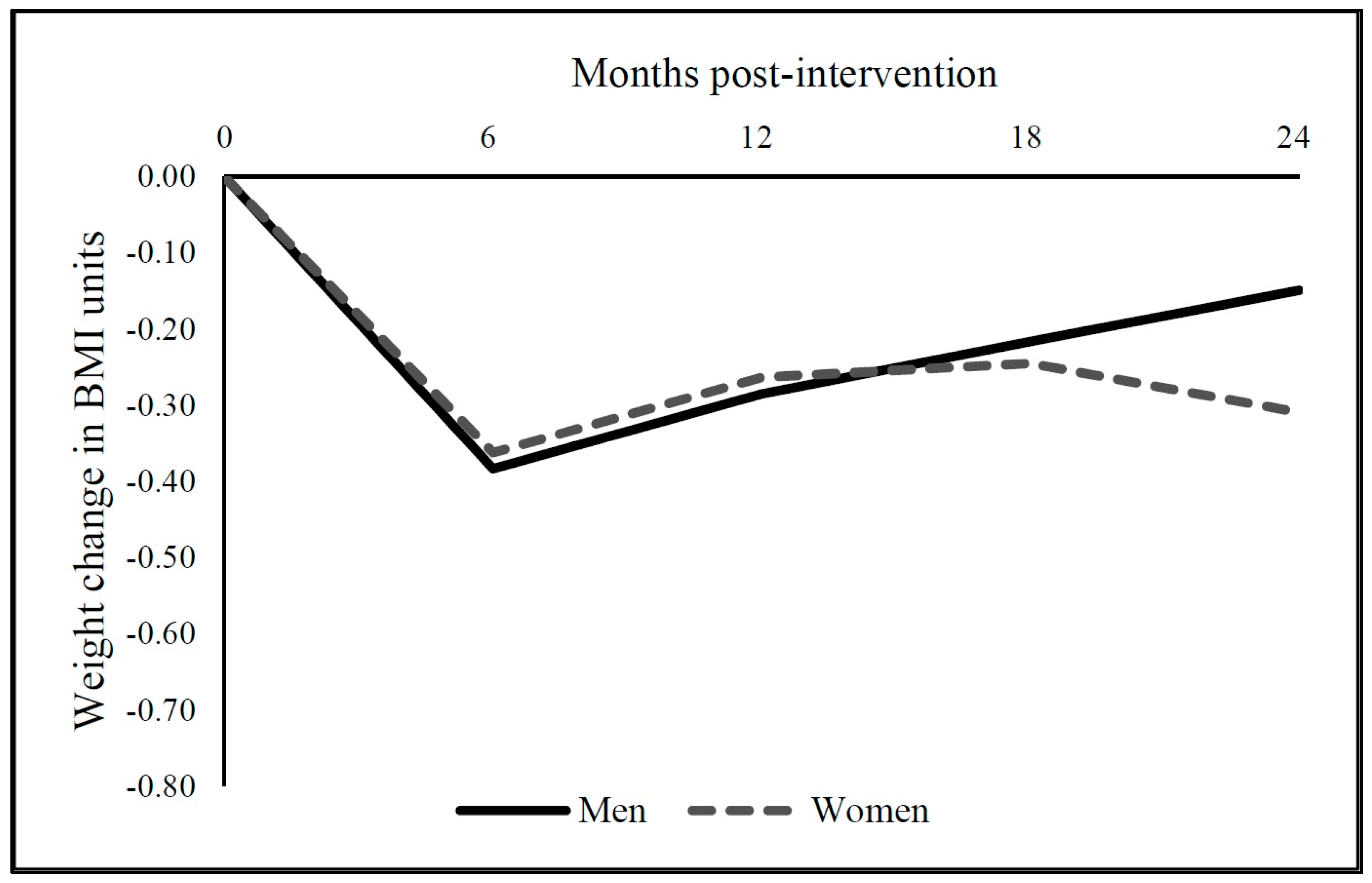
3.2. Average MOVE! Effect on Longer-Term BMI Change at 12, 18, and 24 Months Following Initial 6-Month BMI Change
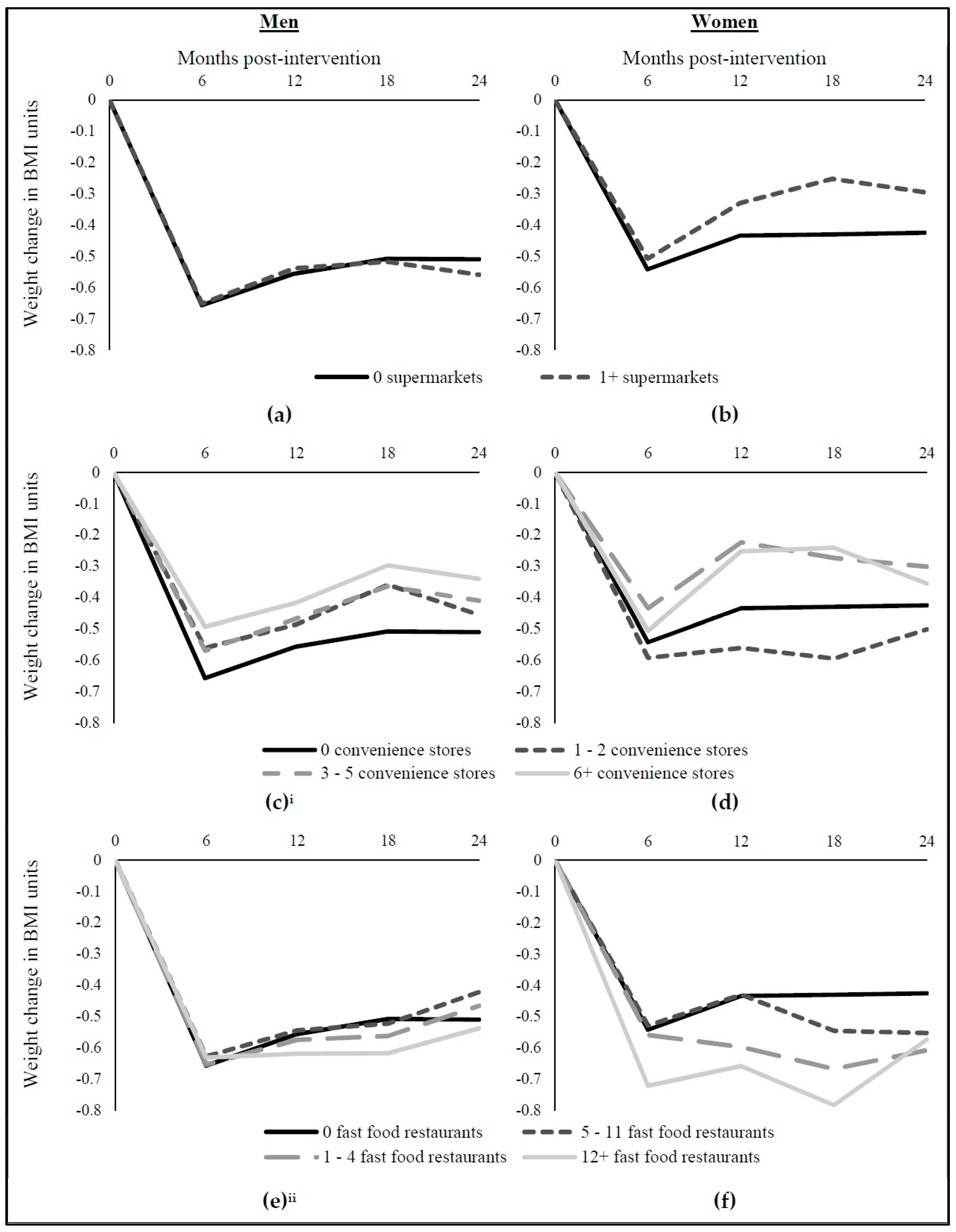
3.3. MOVE! Effect on Longer-Term BMI Change at 12, 18, and 24 Months for Sub-Populations with Different Food Environments
3.4. MOVE! Effect on Longer-Term BMI Change at 12, 18, and 24 Months for Sub-Populations with Different Food Environments among Stayers
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Swift, A. Fewer Americans in this Decade Want to Lose Weight. Gallup Poll Social Series. Available online: http://www.gallup.com/poll/198074/fewer-americans-lose-weight-past-decade.aspx (accessed on 1 July 2017).
- Rueda-Clausen, C.F.; Ogunleye, A.A.; Sharma, A.M. Health benefits of long-term weight-loss maintenance. Annu. Rev. Nutr. 2015, 35, 475–516. [Google Scholar] [CrossRef] [PubMed]
- Ogden, C.L.; Carroll, M.D.; Kit, B.K.; Flegal, K.M. Prevalence of childhood and adult obesity in the United States, 2011–2012. JAMA 2014, 311, 806–814. [Google Scholar] [CrossRef] [PubMed]
- Batsis, J.A.; Gill, L.E.; Masutani, R.K.; Adachi-Mejia, A.M.; Blunt, H.B.; Bagley, P.J.; Lopez-Jimenez, F.; Bartels, S.J. Weight loss interventions in older adults with obesity: A systematic review of randomized controlled trials since 2005. J. Am. Geriatr. Soc. 2017, 65, 257–268. [Google Scholar] [CrossRef] [PubMed]
- Franz, M.J.; VanWormer, J.J.; Crain, A.L.; Boucher, J.L.; Histon, T.; Caplan, W.; Bowman, J.D.; Pronk, N.P. Weight-Loss Outcomes: A systematic review and meta-analysis of weight-loss clinical trials with a minimum 1-year follow-up. J. Am. Diet. Assoc. 2007, 107, 1755–1767. [Google Scholar] [CrossRef] [PubMed]
- Franz, M.J.; Boucher, J.L.; Rutten-Ramos, S.; VanWormer, J.J. Lifestyle weight-loss intervention outcomes in overweight and obese adults with type 2 diabetes: A systematic review and meta-analysis of randomized clinical trials. J. Acad. Nutr. Diet. 2015, 115, 1447–1463. [Google Scholar] [CrossRef] [PubMed]
- Chan, S.H.; Raffa, S.D. Examining the dose–response relationship in the Veterans Health Administration’s MOVE!® Weight Management Program: A nationwide observational study. J. Gen. Intern. Med. 2017, 32, S18–S23. [Google Scholar] [CrossRef] [PubMed]
- Littman, A.J.; Boyko, E.J.; McDonell, M.B.; Fihn, S.D. Evaluation of a weight management program for veterans. Prev. Chronic. Dis. 2012, 9. [Google Scholar] [CrossRef]
- MacLean, P.S.; Wing, R.R.; Davidson, T.; Epstein, L.; Goodpaster, B.; Hall, K.D.; Levin, B.E.; Perri, M.G.; Rolls, B.J.; Rosenbaum, M. NIH working group report: Innovative research to improve maintenance of weight loss. Obesity 2015, 23, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Kraschnewski, J.L.; Boan, J.; Esposito, J.; Sherwood, N.E.; Lehman, E.B.; Kephart, D.K.; Sciamanna, C.N. Long-term weight loss maintenance in the United States. Int. J. Obes. 2010, 34, 1644–1654. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.W.; Konz, E.C.; Frederich, R.C.; Wood, C.L. Long-term weight-loss maintenance: A meta-analysis of U.S. studies. Am. J. Clin. Nutr. 2001, 74, 579–584. [Google Scholar] [PubMed]
- Weiss, E.C.; Galuska, D.A.; Kettel Khan, L.; Gillespie, C.; Serdula, M.K. Weight regain in U.S. adults who experienced substantial weight loss, 1999–2002. Am. J. Prev. Med. 2007, 33, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Glanz, K.; Sallis, J.F.; Saelens, B.E.; Frank, L.D. Healthy nutrition environments: Concepts and measures. Am. J. Health Promot. 2009, 19, 330–333. [Google Scholar] [CrossRef]
- Gordon-Larsen, P. Food availability/convenience and obesity. Adv. Nutr. 2014, 5, 809–817. [Google Scholar] [CrossRef] [PubMed]
- Zenk, S.N.; Thatcher, E.; Reina, M.; Odoms-Young, A. Local Food Environments and Diet-Related Health Outcomes: A Systematic Review of Local Food Environments, Body, Weight, and Other Diet-Related Health Outcomes. In Local Food Environments: Food Access in America; Morland, K.B., Ed.; CRC Press: Boca Raton, FL, USA, 2014; pp. 167–204. [Google Scholar]
- Cobb, L.K.; Appel, L.J.; Franco, M.; Jones-Smith, J.C.; Nur, A.; Anderson, C.A. The relationship of the local food environment with obesity: A systematic review of methods, study quality, and results. Obesity (Silver Spring) 2015, 23, 1331–1344. [Google Scholar] [CrossRef] [PubMed]
- Zenk, S.N.; Tarlov, E.; Wing, C.; Matthews, S.A.; Jones, K.K.; Tong, H.; Powell, L.M. Geographic accessibility of food outlets not associated with BMI change in a nationwide cohort of 1.7 million adults. Health Aff. 2017, 36, 1433–1442. [Google Scholar] [CrossRef] [PubMed]
- Zenk, S.N.; Tarlov, E.; Powell, L.M.; Wing, C.; Matthews, S.A.; Slater, S.; Gordon, H.; Fitzgibbon, M. Weight and Veterans’ Environments Study (WAVES) I and II: Rationale, methods, and cohort characteristics. Am. J. Health Promot. 2017, 3. [Google Scholar] [CrossRef] [PubMed]
- Block, J.P.; Christakis, N.A.; O’Malley, A.J.; Subramanian, S.V. Proximity to food establishments and body mass index in the Framingham Heart Study Offspring Cohort over 30 years. Am. J. Epidemiol. 2011, 174, 1108–1114. [Google Scholar] [CrossRef] [PubMed]
- Boone-Heinonen, J.; Diez-Roux, A.V.; Goff, D.C.; Loria, C.M.; Kiefe, C.I.; Popkin, B.M.; Gordon-Larsen, P. The neighborhood energy balance equation: Does Neighborhood Food Retail Environment + Physical Activity Environment = Obesity? The CARDIA Study. PLoS ONE 2013, 8. [Google Scholar] [CrossRef] [PubMed]
- Gibson, D.M. The neighborhood food environment and adult weight status: Estimates from longitudinal data. Am. J. Public Health 2011, 101, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Harmer, P.; Cardinal, B.J.; Bosworth, M.; Johnson-Shelton, D.; Moore, J.M.; Acock, A.; Vongjaturapat, N. Built environment and 1-year change in weight and waist circumference in middle-aged and older adults: Portland Neighborhood Environment and Health Study. Am. J. Epidemiol. 2009, 169, 401–408. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.T.; Laraia, B.A.; Mujahid, M.S.; Blanchard, S.D.; Warton, E.M.; Moffet, H.H.; Karter, A.J. Is a Reduction in Distance to Nearest Supermarket Associated with BMI change among type 2 diabetes patients? Health Place 2016, 40, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Powell, L.M.; Han, E. Adult obesity and the price and availability of food in the United States. Am. J. Agric. Econ. 2011, 93, 378–384. [Google Scholar] [CrossRef]
- Mendez, D.D.; Gary-Webb, T.L.; Goode, R.; Zheng, Y.; Imes, C.C.; Fabio, A.; Duell, J.; Burke, L.E. Neighborhood factors and six-month weight change among overweight individuals in a weight loss intervention. Preventive Med. Rep. 2016, 4, 569–573. [Google Scholar] [CrossRef] [PubMed]
- Fiechtner, L.; Kleinman, K.; Melly, S.; Sharifi, M.; Marshall, R.; Block, J.; Cheng, E.; Taveras, E. Effects of proximity to supermarkets on a randomized trial studying interventions for obesity. Am. J. Public Health 2016, 106, 557–562. [Google Scholar] [CrossRef] [PubMed]
- Tarlov, E.; Zenk, S.N.; Wing, C.; Gordon, H.; Matthews, S.A.; Jones, K.K.; Powell, L. Does effectiveness of weight management programs depend on the food environment? Evidence from a nationwide program. Journal, (under review).
- Wing, R.R.; Hamman, R.F.; Bray, G.A.; Delahanty, L.; Edelstein, S.L.; Hill, J.O.; Horton, E.S.; Hoskin, M.A.; Kriska, A.; Lachin, J. Achieving weight and activity goals among diabetes prevention program lifestyle participants. Obesity 2004, 12, 1426–1434. [Google Scholar]
- Hamman, R.F.; Wing, R.R.; Edelstein, S.L.; Lachin, J.M.; Bray, G.A.; Delahanty, L.; Hoskin, M.; Kriska, A.M.; Mayer-Davis, E.J.; Pi-Sunyer, X. Effect of weight loss with lifestyle intervention on risk of diabetes. Diabetes Care 2006, 29, 2102–2107. [Google Scholar] [CrossRef] [PubMed]
- Jones, K. MOVE! Weight Management Program for Veterans. In Proceedings of the National MOVE! Education Meeting, New York, NY, USA, 22 May 2012. [Google Scholar]
- Kinsinger, L.S.; Jones, K.R.; Kahwati, L.; Harvey, R.; Burdick, M.; Zele, V.; Yevich, S.J. Design and dissemination of the MOVE! Weight-Management Program for Veterans. Prev. Chronic. Dis. 2009, 6, A98. [Google Scholar] [PubMed]
- Choose My Plate. Available online: https://www.choosemyplate.gov/ (accessed on 1 July 2017).
- U.S. Department of Veterans Affairs and U.S. Department of Defense. VA/DoD Clinical Practice Guideline for Screening and Management of Overweight and Obesity: Guideline Summary. Available online: https://www.healthquality.va.gov/guidelines/CD/obesity/VADoDCPGManagementOfOverweightAn.dObesityFINAL070714.pdf (accessed on 1 July 2017).
- D’Angelo, H.; Suratkar, S.; Song, H.J.; Stauffer, E.; Gittelsohn, J. Access to food source and food source use are associated with healthy and unhealthy food-purchasing behaviours among low-income African-American adults in Baltimore City. Public Health Nutr. 2011, 14, 1632–1639. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A.; Aggarwal, A.; Hurvitz, P.M.; Monsivais, P.; Moudon, A.V. Obesity and supermarket access: Proximity or price? Am. J. Public Health 2012, 102, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Fuller, D.; Cummins, S.; Matthews, S.A. Does transportation mode modify associations between distance to food store, fruit and vegetable consumption, and BMI in low-income neighborhoods? Am. J. Clin. Nutr. 2013, 97, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Ghosh-Dastidar, B.; Cohen, D.; Hunter, G.; Zenk, S.; Huang, C.; Beckman, R.; Dubowitz, T. Distance to store, food prices, and obesity in urban food deserts. Am. J. Prev. Med. 2014, 47, 587–595. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Han, B.; Cohen, D. Beyond neighborhood food environments: Distance traveled to food establishments in 5 U.S. cities, 2009–2011. Prev. Chronic Dis. 2015, 12, E126. [Google Scholar] [CrossRef] [PubMed]
- Zenk, S.; Schulz, A.; Israel, B.; Mentz, G.; Miranda, P.; Opperman, A.; Odoms-Young, A.M. Food shopping behaviours and exposure to discrimination. Public Health Nutr. 2014, 17, 1167–1176. [Google Scholar] [CrossRef] [PubMed]
- Ver Ploeg, M.; Mancino, L.; Todd, J.E.; Clay, D.M.; Scharadin, B. Where do Americans usually shop for food and how do they travel to get there? Initial findings from the national household food acquisition and purchase survey. Econ. Inf. Bull. 2015, 138. [Google Scholar]
- Charreire, H.; Casey, R.; Salze, P.; Simon, C.; Chaix, B.; Banos, A.; Badariotti, D.; Weber, C.; Oppert, J.M. Measuring the food environment using geographical information systems: A methodological review. Public Health Nutr. 2010, 13, 1773–1785. [Google Scholar] [CrossRef] [PubMed]
- Jones, K.; Zenk, S.N.; Tarlov, E.; Powell, L.; Matthews, S.A.; Horoi, I. A step-by-step approach to improve data quality when using commercial business lists to characterize retail food environments. BMC Res. Notes 2017, 10. [Google Scholar] [CrossRef] [PubMed]
- Ingram, D.D.; Franco, S.J. 2013 NCHS urban-rural classification scheme for counties. Vital Health Stat. 2014, 166, 1–73. [Google Scholar]
- Wedick, N.M.; Yunscheng, M.; Olendzki, B.C.; Procter-Gray, E.; Cheng, J.; Kane, K.J.; Ockene, I.S.; Pagoto, S.L.; Land, T.G.; Li, W. Access to healthy food stores modifies effect of a dietary intervention. Am. J. Prev. Med. 2015, 48, 309–317. [Google Scholar] [CrossRef] [PubMed]
- Gustafson, A.A.; Sharkey, J.; Samuel-Hodge, C.D.; Jones-Smith, J.C.; Cai, J.; Ammerman, A.S. Food store environment modifies intervention effect on fruit and vegetable intake among low-income women in North Carolina. J. Nutr. Metab. 2012. [Google Scholar] [CrossRef] [PubMed]
- Farley, T.A.; Rice, J.; Bodor, J.N.; Cohen, D.A.; Bluthenthal, R.N.; Rose, D. Measuring the food environment: Shelf space of fruits, vegetables, and snack foods in stores. J. Urban Health 2009, 86, 672–682. [Google Scholar] [CrossRef] [PubMed]
- Glanz, K.; Sallis, J.F.; Saelens, B.E.; Frank, L.D. Nutrition Environment Measures Survey in Stores (NEMS-S): Development and evaluation. Am. J. Prev. Med. 2007, 32, 282–289. [Google Scholar] [CrossRef] [PubMed]
- Liese, A.D.; Weis, K.E.; Pluto, D.; Smith, E.; Lawson, A. Food store types, availability, and cost of foods in a rural environment. J. Am. Diet. Assoc. 2007, 107, 1916–1923. [Google Scholar] [CrossRef] [PubMed]
- Zenk, S.N.; Powell, L.M.; Rimkus, L.; Isgor, Z.; Barker, D.C.; Ohri-Vachaspati, P.; Chaloupka, F. Relative and absolute availability of healthier food and beverage alternatives across communities in the United States. Am. J. Public Health 2014, 104, 2170–2178. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Characteristic | Men | Women | ||
|---|---|---|---|---|
| MOVE! Participants | Controls | MOVE! Participants | Controls | |
| Total N | 98,871 | 461,302 | 15,385 | 37,192 |
| Body Mass Index in kg/m2, Mean (Standard Deviation) | ||||
| Body Mass Index (BMI) | 36.09 (6.62) | 36.18 (6.6) | 35.43 (6.45) | 35.51 (6.35) |
| Body Weight Status, % | ||||
| Normal/Underweight | 1.42 | 1.39 | 1.81 | 1.76 |
| Overweight | 14.49 | 14.15 | 18.15 | 17.65 |
| Obese | 84.09 | 84.46 | 80.03 | 80.58 |
| Age, Mean (Standard Deviation) | 59.99 (9.84) | 60.20 (9.73) | 50.11 (10.76) | 50.19 (10.73) |
| Race, % | ||||
| Non-Hispanic White | 63.07 | 62.84 | 49.24 | 49.17 |
| Non-Hispanic Black | 24.14 | 24.35 | 38.38 | 38.63 |
| Non-Hispanic Other | 2.13 | 2.14 | 2.90 | 2.95 |
| Hispanic | 5.61 | 5.68 | 4.59 | 4.53 |
| Unknown | 5.04 | 5.00 | 4.90 | 4.73 |
| Marital Status, % | ||||
| Married | 54.99 | 54.94 | 30.84 | 30.62 |
| Separated/Divorced | 25.19 | 25.16 | 37.32 | 37.55 |
| Widowed | 3.21 | 3.23 | 3.85 | 3.74 |
| Single | 16.14 | 16.19 | 27.34 | 27.45 |
| Unknown | 0.47 | 0.48 | 0.65 | 0.63 |
| Health Status, % | ||||
| Breast Cancer | 0.04 | 0.06 | 2.53 | 2.46 |
| Colon Cancer | 0.81 | 0.82 | 0.31 | 0.27 |
| Cerebrovascular Disease | 6.02 | 6.07 | 3.19 | 3.29 |
| Congestive Heart Failure | 7.99 | 8.24 | 2.07 | 2.05 |
| Depression | 36.19 | 36.6 | 53.24 | 53.53 |
| Diabetes | 45.18 | 45.98 | 21.47 | 21.5 |
| Hyperlipidemia | 63.87 | 64.84 | 41.31 | 41.48 |
| Hypertension | 73.81 | 74.68 | 45.98 | 46.22 |
| Myocardial Infarction | 3.78 | 3.86 | 0.81 | 0.85 |
| Osteoarthritis | 22.57 | 23.58 | 20.06 | 21.25 |
| Census Tract Characteristics, Mean (SD) | ||||
| Population Density (1000 people/mi2) | 4.76 (10.15) | 4.77 (9.96) | 4.42 (8.60) | 4.46 (8.79) |
| % Below Poverty | 15.41 (11.96) | 15.48 (12.03) | 16.12 (11.66) | 16.21 (11.66) |
| Median Household Income | 52,911 (21,868) | 52,847 (21,854) | 51,309 (20,339) | 51,194 (20,238) |
| Urbanicity, % | ||||
| Large Central Metro | 32.01 | 32.08 | 32.05 | 32.19 |
| Large Fringe Metro | 22.83 | 22.57 | 21.47 | 21.48 |
| Medium Metro | 30.02 | 29.89 | 32.59 | 32.35 |
| Small Metro | 15.14 | 15.46 | 13.89 | 13.99 |
| Census Division, % | ||||
| New England | 4.60 | 4.71 | 2.63 | 2.65 |
| Middle Atlantic | 10.83 | 10.76 | 8.03 | 8.06 |
| East North Central | 17.77 | 18.23 | 14.23 | 15.04 |
| West North Central | 6.50 | 6.35 | 6.29 | 5.54 |
| South Atlantic Delaware | 21.06 | 21.02 | 26.37 | 26.56 |
| East South Central | 4.91 | 4.59 | 6.38 | 6.19 |
| West South Central | 12.30 | 11.67 | 15.41 | 14.97 |
| Mountain Arizona | 10.58 | 11.07 | 10.17 | 10.65 |
| Pacific Alaska | 11.44 | 11.59 | 10.50 | 10.36 |
| Supermarkets a, % | ||||
| 0 Store | 44.79 | 44.33 | 44.37 | 44.29 |
| 1 + Store | 55.21 | 55.67 | 55.63 | 55.71 |
| Convenience Stores b, % | ||||
| 0 Store | 21.53 | 21.18 | 18.75 | 18.71 |
| 1–2 Stores | 22.50 | 22.51 | 23.17 | 23.58 |
| 3–5 Stores | 25.50 | 25.71 | 27.75 | 26.92 |
| 6 + Stores | 30.48 | 30.61 | 30.33 | 30.79 |
| Fast Food Restaurants b, % | ||||
| 0 Restaurant | 18.81 | 18.57 | 17.56 | 17.88 |
| 1–4 Restaurants | 25.17 | 24.65 | 26.07 | 25.54 |
| 5–11 Restaurants | 26.97 | 27.53 | 28.20 | 27.71 |
| 12 + Restaurants | 29.06 | 29.25 | 28.16 | 28.88 |
| Grocery Stores a, % | ||||
| 0 Store | 49.83 | 49.44 | 49.48 | 49.17 |
| 1 + Stores | 50.17 | 50.56 | 50.52 | 50.83 |
| Parks b, % | ||||
| 0 Park | 29.28 | 28.88 | 30.95 | 30.18 |
| 1 Park | 17.55 | 17.31 | 18.23 | 18.77 |
| 2–3 Parks | 24.53 | 24.85 | 24.45 | 24.48 |
| 4 + Parks | 28.65 | 28.96 | 26.37 | 26.56 |
| Fitness Facilities b, % | ||||
| 0 Facility | 25.90 | 25.58 | 25.54 | 25.32 |
| 1–2 Facilities | 27.97 | 28.14 | 29.94 | 29.99 |
| 3–4 Facilities | 18.20 | 18.29 | 18.44 | 18.33 |
| 5 + Facilities | 27.93 | 28.00 | 26.08 | 26.36 |
| Men | Women | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Food Outlet Access | 6 mo | 12 mo | 18 mo | 24 mo | 6 mo | 12 mo | 18 mo | 24 mo | |
| b (SE) | b (SE) | b (SE) | b (SE) | b (SE) | b (SE) | b (SE) | b (SE) | ||
| MOVE! Effect a,b | −0.657 *** | 0.101 *** | 0.048 | −0.002 | −0.542 *** | 0.108 | 0.004 | 0.005 | |
| (0.025) | (0.027) | (0.026) | (0.031) | (0.070) | (0.079) | (0.073) | (0.094) | ||
| Supermarkets a,c | |||||||||
| 1 + Store | 0.006 | 0.012 | −0.027 | −0.040 | 0.034 | 0.070 | 0.074 | −0.048 | |
| (0.025) | (0.030) | (0.024) | (0.034) | (0.060) | (0.082) | (0.072) | (0.104) | ||
| Fast Food Restaurants a,c | |||||||||
| 1–4 Restaurants | 0.030 | −0.018 | −0.026 | 0.103 * | 0.014 | −0.009 | −0.120 | −0.012 | |
| (0.033) | (0.039) | (0.033) | (0.041) | (0.085) | (0.100) | (0.098) | (0.126) | ||
| 5–11 Restaurants | 0.004 | −0.022 | −0.036 | 0.099 | −0.016 | −0.147 | −0.074 | 0.055 | |
| (0.042) | (0.050) | (0.038) | (0.053) | (0.108) | (0.149) | (0.123) | (0.160) | ||
| 12 + Restaurants | 0.026 | −0.089 | −0.046 | 0.081 | −0.179 | −0.045 | −0.129 | 0.205 | |
| (0.049) | (0.054) | (0.044) | (0.061) | (0.124) | (0.154) | (0.156) | (0.181) | ||
| Convenience Stores a,c | |||||||||
| 1–2 Stores | 0.097 ** | −0.026 | 0.078 * | −0.094 * | −0.050 | −0.076 | −0.038 | 0.088 | |
| (0.031) | (0.036) | (0.032) | (0.042) | (0.084) | (0.116) | (0.108) | (0.145) | ||
| 3–5 Stores | 0.088 * | 0.001 | 0.055 | −0.044 | 0.108 | 0.103 | −0.054 | −0.033 | |
| (0.037) | (0.042) | (0.038) | (0.048) | (0.103) | (0.141) | (0.120) | (0.145) | ||
| 6 + Stores | 0.164 *** | −0.025 | 0.072 | −0.041 | 0.036 | 0.146 | 0.007 | −0.120 | |
| (0.040) | (0.045) | (0.040) | (0.055) | (0.134) | (0.181) | (0.132) | (0.168) | ||
| Stayers | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Men (n = 460,466) | Women (n = 39,426) | ||||||||
| Food Outlet Access | 6 mo | 12 mo | 18 mo | 24 mo | 6 mo | 12 mo | 18 mo | 24 mo | |
| b (SE) | b (SE) | b (SE) | b (SE) | b (SE) | b (SE) | b (SE) | b (SE) | ||
| MOVE! Effect a,b | −0.507 *** | 0.129 *** | 0.086 ** | 0.011 | −0.413 *** | 0.314 * | 0.012 | 0.140 | |
| (0.025) | (0.030) | (0.029) | (0.036) | (0.097) | (0.122) | (0.102) | (0.109) | ||
| Supermarkets a,c | |||||||||
| 1 + Store | 0.008 | 0.031 | −0.007 | −0.008 | −0.025 | 0.104 | 0.056 | −0.049 | |
| (0.035) | (0.036) | (0.029) | (0.039) | (0.076) | (0.108) | (0.095) | (0.129) | ||
| Fast Food Restaurants a,c | |||||||||
| 1–4 Restaurants | 0.006 | −0.013 | −0.021 | 0.103 * | 0.044 | −0.073 | 0.081 | −0.330 * | |
| (0.035) | (0.043) | (0.039) | (0.047) | (0.109) | (0.219) | (0.168) | (0.161) | ||
| 5–11 Restaurants | 0.033 | −0.069 | 0.016 | 0.049 | 0.001 | −0.236 | 0.214 | −0.151 | |
| (0.053) | (0.055) | (0.049) | (0.060) | (0.130) | (0.265) | (0.217) | (0.206) | ||
| 12 + Restaurants | 0.065 | −0.154 * | −0.029 | 0.098 | −0.083 | −0.133 | 0.095 | 0.044 | |
| (0.064) | (0.063) | (0.051) | (0.068) | (0.154) | (0.280) | (0.225) | (0.228) | ||
| Convenience Stores a,c | |||||||||
| 1–2 Stores | 0.084 * | −0.038 | 0.051 | −0.059 | −0.042 | −0.006 | −0.123 | −0.118 | |
| (0.035) | (0.040) | (0.037) | (0.048) | (0.103) | (0.174) | (0.154) | (0.200) | ||
| 3–5 Stores | 0.071 | −0.002 | 0.027 | −0.022 | 0.055 | 0.332 | −0.432 | −0.051 | |
| (0.043) | (0.047) | (0.044) | (0.057) | (0.118) | (0.256) | (0.281) | (0.186) | ||
| 6 + Stores | 0.107 | −0.009 | −0.003 | −0.019 | −0.063 | 0.237 | −0.377 | −0.142 | |
| (0.056) | (0.056) | (0.051) | (0.066) | (0.148) | (0.260) | (0.244) | (0.233) | ||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zenk, S.N.; Tarlov, E.; Wing, C.; Matthews, S.A.; Tong, H.; Jones, K.K.; Powell, L.M. Long-Term Weight Loss Effects of a Behavioral Weight Management Program: Does the Community Food Environment Matter? Int. J. Environ. Res. Public Health 2018, 15, 211. https://doi.org/10.3390/ijerph15020211
Zenk SN, Tarlov E, Wing C, Matthews SA, Tong H, Jones KK, Powell LM. Long-Term Weight Loss Effects of a Behavioral Weight Management Program: Does the Community Food Environment Matter? International Journal of Environmental Research and Public Health. 2018; 15(2):211. https://doi.org/10.3390/ijerph15020211
Chicago/Turabian StyleZenk, Shannon N., Elizabeth Tarlov, Coady Wing, Stephen A. Matthews, Hao Tong, Kelly K. Jones, and Lisa M. Powell. 2018. "Long-Term Weight Loss Effects of a Behavioral Weight Management Program: Does the Community Food Environment Matter?" International Journal of Environmental Research and Public Health 15, no. 2: 211. https://doi.org/10.3390/ijerph15020211
APA StyleZenk, S. N., Tarlov, E., Wing, C., Matthews, S. A., Tong, H., Jones, K. K., & Powell, L. M. (2018). Long-Term Weight Loss Effects of a Behavioral Weight Management Program: Does the Community Food Environment Matter? International Journal of Environmental Research and Public Health, 15(2), 211. https://doi.org/10.3390/ijerph15020211