Experience and Future Perceived Risk of Floods and Diarrheal Disease in Urban Poor Communities in Accra, Ghana

Abstract
1. Introduction
2. Risk Perceptions
3. Why Focus on Flood-Prone Urban Poor Communities?
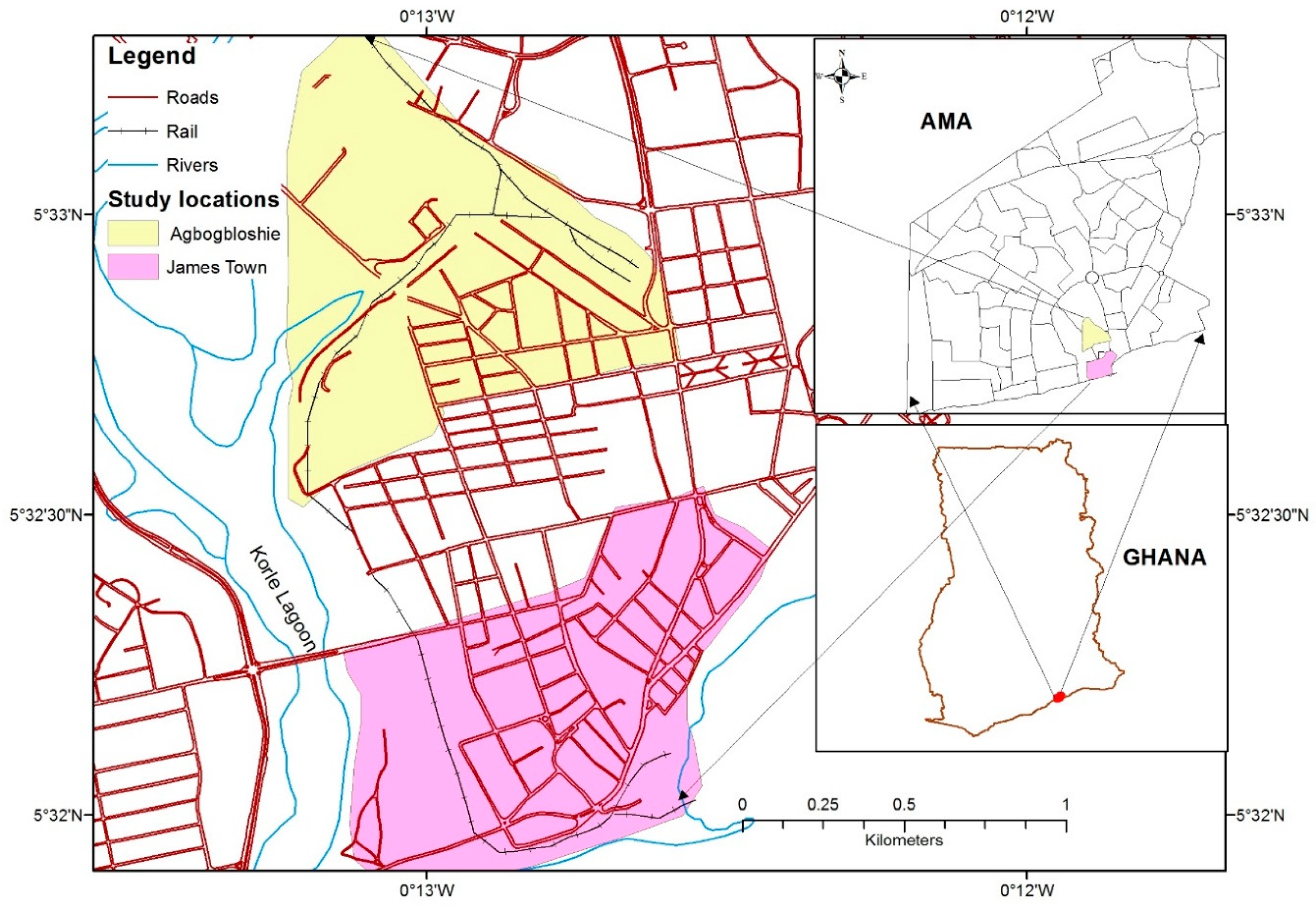
Study Area
4. Methodology
4.1. Dependent Variable
4.2. Independent Variable
4.3. Control Variables
4.4. Analytic Approach
5. Results
5.1. Descriptive Statistics of Outcome, Explanatory and Control Variables
5.2. Factors Associated with Perceived Risk of Diarrheal Disease
5.3. Predictors of Perceived Risk of Diarrheal Disease
6. Discussion
7. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization 2013 Health Topics. Available online: www.who.int/topics/diarrhea/en/ (accessed on 17 December 2014).
- Bartman, J.; Cairncross, S. Hygiene, sanitation and water: Forgotten foundations of health. PLoS Med. 2010, 7, e1000367. [Google Scholar] [CrossRef]
- WHO; UNICEF. Progress on Sanitation and Drinking Water 2010 Update; Joint Monitoring Programme for Water Supply and Sanitation; WHO: Geneva, Switzerland; UNICEF: New York, NY, USA, 2010. [Google Scholar]
- Hashizume, M.; Armstrong, B.; Hajat, S.; Wagatsuma, Y.; SG Faruque, A.; Hayashi, T.; Sack, D. Association between climate variability and hospital visits for non-cholera diarrhea in Bangladesh: Effects and vulnerable groups. Int. J. Epidemiol. 2007, 36, 1030–1037. [Google Scholar] [CrossRef] [PubMed]
- Black, R.E.; Cousens, S.; Johnson, H.; Lawn, J.E.; Rudan, I.; Bassani, D.G. Global, regional and national causes of child mortality, 2008. Lancet 2010, 375, 1969–1987. [Google Scholar] [CrossRef]
- Kosek, M.; Bern, C.; Guerrant, R.L. The global burden of diarrheal disease, as estimated from studies published between 1992 and 2000. Bull. WHO 2003, 81, 197–204. [Google Scholar] [PubMed]
- WHO; UNICEF. Joint Monitoring Programme for Water Supply and Sanitation. Meeting the MDG Drinking Water and Sanitation Target: The Urban and Rural Challenges of the Decade, WHO: Geneva, Switzerland; UNICEF: New York, NY, USA, 2006.
- Ghana Health Service. 2016 Annual Report; Ghana Health Service: Accra, Ghana, 2017.
- Santosham, M.; Chandran, A.; Fitzwater, S.; Fischer-Walker, C.; Baqui, A.H.; Black, R. Progress and barriers for the control of diarrheal disease. Lancet 2010, 376, 63–67. [Google Scholar] [CrossRef]
- Smith, K.R.; Woodward, A.; Campbell-Lendrum, D.; Chadee, D.D.; Honda, Y.; Liu, Q.; Olwoch, J.M.; Revich, B.; Sauerborn, R. Human health: Impacts, adaptation, and co-benefits. In Climate Change 2014: Impacts, Adaptation, and Vulnerability. Part A: Global and Sectoral Aspects. Contribution of Working Group II to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change; Field, C.B., Barros, V.R., Dokken, D.J., Mach, K.J., Mastrandrea, M.D., Bilir, T.E., Chatterjee, M., Ebi, K.L., Estrada, Y.O., Genova, R.C., et al., Eds.; Cambridge University Press: Cambridge, UK; New York, NY, USA, 2014; pp. 709–754. [Google Scholar]
- Levy, K.; Woeter, P.A.; Goldstein, S.R.; Callton, J.E. Untangling the impacts of climate change on waterborne disease: A systematic review of relationships between diarrheal disease and temperature, rainfall, flooding, and drought. Environ. Sci. Technol. 2016, 50, 4905–4922. [Google Scholar] [CrossRef] [PubMed]
- Hashizume, M.; Armstrong, B.; Wagatsuma, Y.; Faruque, A.S.G.; Hayashi, T. Rotavirus infections and climate variability in Dhaka, Bangladesh: A time-series analysis. Epidemiol. Infect. 2008, 136, 1281–1289. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.S. Effects of local climate variability on transmission dynamics of cholera in Matlab, Bangladesh. Trans. R. Soc. Trop. Med. Hyg. 2009, 103, 1165–1170. [Google Scholar] [CrossRef]
- Reyburn, R.; Kim, D.R.; Emch, M.; Khatib, A.; von Seidlein, L.; Ali, M. Climate variability and the outbreaks of cholera in Zanzibar, East Africa: A time series analysis. Am. J. Trop. Med. Hyg. 2011, 84, 862–869. [Google Scholar] [CrossRef]
- Ramirez, I.J. Cholera resurgence in Piura, Peru: Examining climate associations during the 1997–1998 El Niño. Geojournal 2015, 80, 129–143. [Google Scholar] [CrossRef]
- Bompangue, N.D.; Giraudoux, P.; Plisnier, P.D.; Mutombo, T.A.; Piarroux, M.; Sudre, B. Dynamics of cholera outbreaks in Great Lakes region of Africa, 1978–2008. Emerg. Infect. Dis. 2011, 17, 2026–2034. [Google Scholar]
- Emch, M.E. Relationships between Flood Control, Kala-azar, and Diarrheal Disease in Bangladesh. Environ. Plan. A 2000, 32, 1051–1063. [Google Scholar] [CrossRef]
- Hashizume, M.; Armstrong, B.; Hajat, S.; Wagatsuma, Y.; Faruque, S.G.A.; Hayashi, T.; Sack, D. Factors determining vulnerability to diarrhea during and after severe floods in Bangladesh. J. Water Health 2008, 6, 323–332. [Google Scholar] [CrossRef] [PubMed]
- Hashizume, M.; Armstrong, B.; Hajat, S.; Wagatsuma, Y.; Faruque, A.S.; Hayashi, T.; Sack, D.A. The effect of rainfall on the incidence of cholera in Bangladesh. Epidemiology 2008, 19, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Carrel, M.; Emch, M.; Streatfield, K.; Yunus, M. Spatio-temporal clustering of cholera: The impact of flood control in Matlab, Bangladesh, 1983–2003. Health Place 2009, 15, 771–782. [Google Scholar] [CrossRef] [PubMed]
- Carrel, M.; Voss, P.; Streatfield, K.; Yunus, M.; Emch, M. Protection from annual flooding is correlated with increased cholera prevalence in Bangladesh. Environ. Health 2010, 9, 13. [Google Scholar] [CrossRef] [PubMed]
- Songsore, J.; Nabila, J.S.; Yangyuoru, Y.; Alve, S.; Bosque-Hamilton, E.K.; Amponsah, P.E.; Alhassan, O.; Satterthwaite, D. Environmental Health Watch and Disaster Monitoring in the Greater Accra Metropolitan Area (GAMA); University of Ghana: Accra, Ghana, 2006. [Google Scholar]
- Brikholz, S.; Muro, M.; Jeffery, P.; Smith, H.M. Rethinking the relationship between flood risk perception and flood management. Sci. Total Environ. 2014, 487, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Slovic, P.; Peters, E. Risk perception and affect. Curr. Dir. Psychol. Sci. 2006, 15, 322–325. [Google Scholar] [CrossRef]
- Alhakami, A.S.; Slovic, P. A psychological study of the inverse relationship between perceived risk and perceived benefit. Risk Anal. 1994, 14, 1085–1096. [Google Scholar] [CrossRef]
- Stuart, C.J.; Susan, J.K. Climate change and coastal environmental risk perceptions in Florida. J. Environ. Manag. 2013, 130, 32–39. [Google Scholar]
- Linnerkamp, F.; Koedam, A.; Baud, I.S.A. Household vulnerability to climate change: Examining perceptions of households of flood risk in Georgetown and Paramaribo. Habitat Int. 2011, 35, 447–456. [Google Scholar] [CrossRef]
- Levy, G.A.; Shea, J.; Sankey, V.W.; Quistberg, A.; Amstrong, K. Measuring perceptions of breast cancer risk. Cancer Epidemiol. Biomak. Prev. 2006, 15, 1893–1898. [Google Scholar] [CrossRef] [PubMed]
- Price, J. Perceptions of colorectal cancer in a socioeconomically disadvantaged population. J. Community Health 1993, 18, 347–362. [Google Scholar] [CrossRef] [PubMed]
- Kellens, W.; Zaalberg, R.; Neutens, T.; Vanneuvile, W.; De Maeyer, P. An analysis of public perception of flood risk on the Belgian Coast. Risk Anal. 2011, 30, 501–511. [Google Scholar] [CrossRef] [PubMed]
- Ludlow, C. Flood Modeling in a Data-Poor Region: A Satellite Data-Supported Flood Model for Accra, Ghana. Presented at the Annual Meeting of the Association for American Geographers, Las Vegas, NV, USA, 22–27 March 2009. [Google Scholar]
- Afeku, K. Urbanization and Flooding in Accra, Ghana. Master’s Thesis, Department of Geography, Miami University, Oxford, OH, USA, 2005. [Google Scholar]
- Codjoe, S.N.A.; Afuduo, S. Geophysical, socio-demographic characteristics and perception of flood vulnerability in Accra, Ghana. Nat. Hazards 2015, 77, 787–804. [Google Scholar] [CrossRef]
- Rain, D.; Engstrom, R.; Ludlow, C.; Antos, S. Accra Ghana: A City Vulnerable to Flooding and Drought-Induced Migration; Background paper; UN-Habitat: Nairobi, Kenya, 2011. [Google Scholar]
- Haines, A.; Patz, J. Health effects of climate change. J. Am. Med. Assoc. 2004, 291, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Boadi, K.O.; Kuitunen, M. Urban waste pollution in the Korle Lagoon, Accra, Ghana. Environmentalist 2002, 22, 302–330. [Google Scholar]
- Huq, S.; Kovats, S.; Reid, H.; Satterthwaite, D. Reducing Risks to Cities from Climate Change: An Environmental or a Development Agenda? Environment & Urbanization Brief no. 15; SAGE Publishing: Thousand Oaks, CA, USA, April 2007. [Google Scholar]
- Ghana Statistical Service. Population and Housing Census: Summary of Final Report; Ghana Statistical Service: Accra, Ghana, 2012.
- Ghana Statistical Service. Population and Housing Census of Ghana. Alphabetical List of Localities with Statistics on Their Population, Number of Houses and Households and Average Household Size. The Gazetteer 2 (GA-MY), 59. 2005; Ghana Statistical Service: Accra, Ghana, 2000.
- Ghana Statistical Service. Population and Housing Census of Ghana. Alphabetical List of Localities with Statistics on Their Population, Number of Houses and Households and Average Household Size. The Gazetteer 3 (NA-ZU): 325. 2000; Ghana Statistical Service: Accra, Ghana, 2000.
- Codjoe, S.N.A.; Owusu, G.; Burkett, V. Perceptions, experience and indigenous knowledge of climate change and variability: The case of Accra, a sub-Saharan African city. Reg. Environ. Chang. 2014, 14, 369–383. [Google Scholar] [CrossRef]
- Fobil, J.N.; May, J.; Kraemer, A. Assessing the relationship between socioeconomic conditions and urban environmental quality in Accra, Ghana. Int. J. Environ. Res. Public Health 2010, 7, 125–145. [Google Scholar] [CrossRef]
- Agbodaze, D.; Owusu, S.B. Cockroaches (Periplaneta americana) as carriers of agents of bacterial diarrhea in Accra, Ghana. Cent. Afr. J. Med. 1989, 35, 484–486. [Google Scholar]
- Osumanu, K.I. Household environmental and behavioural determinants of childhood diarrhea morbidity in the Tamale Metropolitan Area (TMA), Ghana. Dan. J. Geogr. 2007, 107, 59–68. [Google Scholar] [CrossRef]
- Njuguna, J. Effects of eliminating open defecation on diarrhoeal morbidity: An ecological study of Nyando and Nambale sub-counties, Kenya. BMC Public Health 2016, 16, 712. [Google Scholar] [CrossRef] [PubMed]
- Pham-Doc, P.; Nguyen-Viet, H.; Hattendorf, J.; Dac, C.P.; Zurbrugg, C.; Zinsstag, J.; Odermatt, P. Diarrhoeal disease among adult population in an agricultural community Hanam province, Vietnam, with high wastewater and excreta reuse. BMC Public Health 2014, 14, 978. [Google Scholar]
- Dodoo, D.K.; Quagraine, E.K.; Okai-Sam, F.; Kambo, J.D.; Headley, J.V. Quality of “sachet” water in the Cape Coast Municipality of Ghana. J. Environ. Sci. Health Part A Toxic/Hazard. Subst. Environ. Eng. 2007, 41, 329–342. [Google Scholar] [CrossRef] [PubMed]
- WHO. Drinking Water. 2006. Available online: www.who.int/water_sanitation_health/monitoring/water.pdf (accessed on 20 May 2015).
- Stoler, J.; Fink, G.; Weeks, J.R.; Otoo, R.A.; Ampofo, J.A.; Hill, A.G. When urban taps run dry: Sachet water consumption and health effects in low-income neighborhoods in Accra, Ghana. Health Place 2012, 18, 250–262. [Google Scholar] [CrossRef]
- Osei, F.B.; Duker, A.A. Spatial dependency of V. cholera prevalence on open space refuse dumps in Kumasi, Ghana: A spatial statistical modelling. Int. J. Health Geogr. 2008, 7, 62. [Google Scholar] [CrossRef]


{kind=link}
| Variables and Their Classification | Coding |
| Mean age of Household Members | Continuous variable |
| Household size | |
| Sex of household head | |
| Male | =1 Male, =2 Female |
| Female | |
| Proportion of household members with some education | |
| No member had education | =1 No member had education, =2 Less than 50% had education, =3 50% and above had education, =4 All members had education |
| Less than 50% had education | |
| 50% and above had education | |
| All members had education | |
| Wealth status | |
| Poorest | =1 Poorest, =2 Poor, =3 Middle, =4 Rich, =5 Richest |
| Poor | |
| Middle | |
| Rich | |
| Richest | |
| Hand washing with soap before eating | |
| Yes | =1 Yes, =2 No |
| No | |
| Hand washing with soap after visiting the toilet | |
| Yes | =1 Yes, =2 No |
| No | |
| Main material on the floor of the house | |
| Sand/Cement/Concrete | =1 Sand/Cement/Concrete, =2 Wood/Wood Planks/Woolen Carpet, =3 Ceramic Tiles/Porcelain Granite/Marble |
| Wood/Wood Planks/Woolen Carpet | |
| Ceramic Tiles/Porcelain Granite/Marble | |
| Main material on the wall of the house | |
| Bamboo with mud | =1 Bamboo with mud, =2 Wood, =3 Plywood, =4 Cement Blocks/Concrete, =5 Other |
| Wood | |
| Plywood | |
| Cement Blocks/Concrete | |
| Other | |
| Main source of drinking water | |
| Piped into dwelling | =1 Piped into dwelling, =2 Piped into yard, =3 Public tap/stand pipe, =4 Sachet water/bottled water |
| Piped into yard | |
| Public tap/stand pipe | |
| Sachet water/bottled water | |
| Type of toilet facility | |
| No facility/bucket pan/pit latrine | =1 No facility/bucket pan/pit latrine, =2 WC/Flush toilet, =3 KVIP, =4 Public toilet |
| WC/Flush toilet | |
| Kumasi Ventilated-Improved Pit (KVIP) | |
| Public toilet | |
| Mode of disposing solid waste | |
| Improved | =1 Improved, =2 Unimproved |
| Unimproved | |
| Used soap to wash hands before eating | |
| Yes | =1 Yes, =2 No |
| No | |
| Used soap to wash hands after visiting toilet | |
| Yes | =1 Yes, =2 No |
| No | |
| Availability of livestock at home | |
| Yes | =1 Yes, =2 No |
| No | |
| Number of times seen cockroaches at home in the past 7 days | |
| Never | =1 Never, =2 1–3 Times, =3 4 or more Times, =4 Don’t Know |
| 1–3 Times | |
| 4 or more Times | |
| Don’t Know | |
| Distance from home to the nearest public toilet | |
| Less than 50 m | =1 Less than 50 m, =2 50 m and above |
| 50 m and above | |
| Distance to the nearest refuse collection point | |
| Less than 50 m | =1 Less than 50 m, =2 50 m and above |
| 50 m and above | |
| Locality | |
| Agbogbloshie | =1 Agbogbloshie, =2 James Town |
| James Town | |
| Variable | Agbogbloshie | James Town | Total | |||
|---|---|---|---|---|---|---|
| Count (Mean) | % (SD) | Count (Mean) | % (SD) | Count (Mean) | % (SD) | |
| Outcome | ||||||
| Household perceived future risk of diarrhea | (18.14) | (22.16) | (4.48) | (6.62) | (11.26) | (17.67) |
| Explanatory Variables | ||||||
| Experience of 26 October 2011 flooding and experience of diarrhea within 4 weeks after the flood | ||||||
| Household experienced flood and had at least a reported case of diarrhea | 104 | 52.3 | 15 | 7.4 | 119 | 29.7 |
| Household experienced flood but had no reported case of diarrhea | 46 | 23.1 | 17 | 8.4 | 63 | 15.7 |
| Household did not experience flood but had at least a reported case of diarrhea | 26 | 13.1 | 52 | 25.7 | 78 | 19.5 |
| Household did not experience flood and had no reported case of diarrhea | 23 | 11.6 | 118 | 58..4 | 141 | 35.2 |
| Sex | ||||||
| Male | 117 | 58.8 | 110 | 54.5 | 227 | 56.6 |
| Female | 82 | 41.2 | 92 | 45.5 | 174 | 43.4 |
| Mean age of household members | (25.20) | (8.76) | (32.67) | (14.45) | (28.96) | (12.53) |
| Education of household members | ||||||
| Less than 50% had education | 5 | 2.5 | 6 | 3.0 | 11 | 2.7 |
| 50% and more had education | 53 | 26.6 | 51 | 25.2 | 104 | 25.9 |
| All members had education | 141 | 70.9 | 145 | 71.8 | 286 | 71.3 |
| Household size | (2.22) | (0.85) | (2.19) | (0.99) | (2.2) | (0.926) |
| Main material on floor of house | ||||||
| Sand/Cement/Concrete | 167 | 83.9 | 147 | 72.8 | 314 | 78.3 |
| Wood/Wood Planks/Woolen Carpet | 25 | 12.6 | 47 | 23.3 | 72 | 18.0 |
| Ceramic Tiles/Porcelain Granite/Marble | 7 | 3.5 | 8 | 4.0 | 15 | 3.7 |
| Main material on wall of house | ||||||
| Bamboo with mud | 14 | 7.0 | 7 | 3.5 | 21 | 5.2 |
| Wood | 112 | 56.3 | 91 | 45.0 | 2013 | 50.6 |
| Plywood | 30 | 15.1 | 23 | 11.4 | 53 | 13.2 |
| Cement Blocks/Concrete | 39 | 19.6 | 75 | 37.1 | 114 | 28.4 |
| Other | 4 | 2.0 | 6 | 3.0 | 10 | 2.5 |
| Wealth status | ||||||
| Poorest | 20 | 10.1 | 60 | 29.7 | 80 | 20.0 |
| Poor | 11 | 5.5 | 69 | 34.2 | 80 | 20.0 |
| Middle | 46 | 23.1 | 35 | 17.3 | 81 | 20.2 |
| Rich | 61 | 30.7 | 19 | 9.4 | 80 | 20.0 |
| Richest | 61 | 30.7 | 19 | 9.4 | 80 | 20.0 |
| Main source of drinking water | ||||||
| Piped into dwelling | 1 | 0.5 | 22 | 10.9 | 23 | 5.7 |
| Piped into yard | 6 | 3.0 | 17 | 8.4 | 23 | 5.7 |
| Public tap/stand pipe | 45 | 22.6 | 51 | 25.2 | 96 | 23.9 |
| Sachet water/bottled water | 147 | 73.9 | 112 | 55.4 | 259 | 64.6 |
| Type of toilet facility | ||||||
| No facility/bucket pan/pit latrine | 1 | 0.5 | 10 | 5.0 | 11 | 2.7 |
| WC/Flush toilet | 0 | 0.0 | 20 | 9.9 | 20 | 5.7 |
| Kumasi Ventilated-Improved Pit (KVIP) | 20 | 10.1 | 10 | 5.0 | 30 | 7.5 |
| Public toilet | 178 | 89.4 | 162 | 80.2 | 340 | 84.8 |
| Mode of disposing solid waste | ||||||
| Improved | 118 | 59.3 | 167 | 82.7 | 285 | 71.1 |
| Unimproved | 81 | 40.7 | 35 | 17.3 | 116 | 28.9 |
| Used soap to wash hands before eating | ||||||
| Yes | 46 | 23.1 | 57 | 28.2 | 103 | 25.7 |
| No | 153 | 76.9 | 145 | 71.8 | 298 | 74.3 |
| Used soap to wash hands after visiting toilet | ||||||
| Yes | 86 | 43.2 | 71 | 35.1 | 157 | 39.2 |
| No | 113 | 56.8 | 131 | 64.9 | 244 | 60.8 |
| Availability of livestock at home | ||||||
| Yes | 4 | 2.0 | 11 | 5.4 | 15 | 3.7 |
| No | 195 | 98.0 | 191 | 94.6 | 386 | 96.3 |
| Number of times seen cockroaches at home in the past 7 days | ||||||
| Never | 36 | 18.1 | 53 | 26.2 | 89 | 22.2 |
| 1–3 Times | 36 | 18.1 | 76 | 37.6 | 112 | 27.9 |
| 4 or more Times | 126 | 63.3 | 64 | 31.7 | 190 | 47.4 |
| Don’t Know | 1 | .5 | 9 | 4.5 | 10 | 2.5 |
| Distance from home to the nearest public toilet | ||||||
| Less than 50 m | 69 | 34.7 | 64 | 31.7 | 133 | 33.2 |
| 50 m and above | 130 | 65.3 | 138 | 68.3 | 268 | 66.8 |
| Distance to the nearest refuse collection point | ||||||
| Less than 50 m | 105 | 52.8 | 199 | 98.5 | 304 | 75.8 |
| 50 m and above | 94 | 47.2 | 3 | 1.5 | 97 | 24.2 |
| N | 199 | 202 | 401 | |||
| Variable | Mean Perceived Risk of Diarrhea (SD) | F | p-Value |
|---|---|---|---|
| Experience of 26 October 2011 flooding and experience of diarrhea within 4 weeks after the flood | 44.4 | 0.001 | |
| Household experienced flood and had at least a reported case of diarrhea | 22.94 (23.05) | ||
| Household experienced flood but had no reported case of diarrhea | 2.54 (7.82) | ||
| Household did not experience flood but had at least a reported case of diarrhea | 15.06 (16.64) | ||
| Household did not experience flood and had no reported case of diarrhea | 3.19 (6.33) | ||
| Sex | 6.965 | 0.009 | |
| Male | 13.28 (20.01) | ||
| Female | 8.62 (13.63) | ||
| Mean age of household members | r = −0.199 | 0.001 | |
| Education of household members | 0.325 | 0.722 | |
| No member/less 50% had education | 15.45 (20.67) | ||
| 50% and more had education | 10.96 (171.98) | ||
| All members had education | 11.21 (17.47) | ||
| Household size | r = −0.055 | 0.276 | |
| Main material on floor of house | 0.472 | 0.624 | |
| Sand/Cement/Concrete | 10.91 (16.24) | ||
| Wood/Wood Planks/Woolen Carpet | 13.06 (23.30) | ||
| Ceramic Tiles/Porcelain Granite/Marble | 10.00 (15.58) | ||
| Main material on wall of house | 10.744 | 0.001 | |
| Bamboo with mud | 18.10 (14.36) | ||
| Wood | 10.34 (15.84) | ||
| Plywood | 23.40 (27.10) | ||
| Cement Blocks/Concrete | 5.92 (12.40) | ||
| Other | 12.00 (15.59) | ||
| Wealth status | 0.688 | 0.600 | |
| Poorest | 13.35 (18.65) | ||
| Poor | 12.17 (18.69) | ||
| Middle | 10.86 (17.17) | ||
| Rich | 10.13 (19.38) | ||
| Richest | 9.36 (13.61) | ||
| Main source of drinking water | 2.93 | 0.033 | |
| Piped into dwelling | 2.17 (5.18) | ||
| Piped into yard | 6.52 (8.85) | ||
| Public tap/stand pipe | 12.29 (17.50) | ||
| Sachet water/bottled water | 12.10 (18.74) | ||
| Type of toilet facility | 3.69 | 0.012 | |
| No facility/bucket pan/pit latrine | 5.45 (6.88) | ||
| WC/Flush toilet | 5.75 (7.48) | ||
| Kumasi Ventilated-Improved Pit (KVIP) | 20.17 (28.90) | ||
| Public toilet | 10.99 (16.78) | ||
| Mode of disposing solid waste | 2.134 | 0.145 | |
| Improved | 10.44 (15.37) | ||
| Unimproved | 13.28 (22.25) | ||
| Used soap to wash hands before eating | 0.175 | 0.676 | |
| Yes | 10.63 (18.25) | ||
| No | 11.48 (17.48) | ||
| Used soap to wash hands after visiting toilet | 0.000 | 0.989 | |
| Yes | 11.27 (19.86) | ||
| No | 11.25 (16.13) | ||
| Availability of livestock at home | 1.758 | 0.186 | |
| Yes | 5.33 (11.26) | ||
| No | 11.49 (17.83) | ||
| Number of times seen cockroaches at home in the past 7 days | 8.714 | 0.001 | |
| Never | 7.64 (11.36) | ||
| 1–3 Times | 7.01 (11.79) | ||
| 4 or more Times | 15.84 (21.80) | ||
| Don’t Know | 4.00 (6.99) | ||
| Distance from home to the nearest public toilet | 2.400 | 0.122 | |
| Less than 50 m | 9.32 (17.02) | ||
| 50 m and above | 12.22 (17.92) | ||
| Distance to the nearest refuse collection point | 43.32 | 0.001 | |
| Less than 50 m | 8.14 (14.33) | ||
| 50 m and above | 21.03 (22.89) | ||
| Locality | 70.393 | 0.001 | |
| Agbogbloshie | 18.14 (22.16) | ||
| James Town | 4.48 (6.62) |
| Robust | Robust | |||||
|---|---|---|---|---|---|---|
| Coefficient | Std. Err. | Coefficient | Std. Err. | |||
| Variable | Model 1 | Model 2 | ||||
| Experience of 26 October 2011 flooding and experience of diarrhea within 4 weeks after (RC is Experienced flood and had diarrhea) | ||||||
| Household experienced flood but had no reported case of diarrhea | −20.402 | *** | 2.331 | −17.813 | *** | 2.213 |
| Household did not experience flood but had at least a reported case of diarrhea | −7.877 | ** | 2.830 | −1.816 | 2.836 | |
| Household did not experience flood and had no reported case of diarrhea | −19.750 | *** | 2.181 | −11.727 | *** | 2.257 |
| Sex (RC is Male) | ||||||
| Female | −2.791 | * | 1.392 | |||
| Mean age of household members | −0.171 | 0.283 | ||||
| Wealth status (RC is poorest) | ||||||
| Poor | −0.812 | 2.230 | ||||
| Middle | −0.522 | 2.185 | ||||
| Rich | 1.006 | 2.362 | ||||
| Richest | 0.467 | 1.977 | ||||
| Main material on wall of house (RC is Bamboo with mud) | ||||||
| Wood | −3.483 | 2.606 | ||||
| Plywood | 8.662 | ** | 3.598 | |||
| Cement Blocks/Concrete | −4.660 | 2.867 | ||||
| Other | −1.965 | 3.823 | ||||
| Main source of drinking water (RC is public tap/stand pipe | ||||||
| Piped into dwelling | 1.849 | 1.571 | ||||
| Piped into yard | 0.269 | 1.896 | ||||
| Sachet water/bottled water | 2.059 | 1.658 | ||||
| Type of toilet facility (RC is public toilet) | ||||||
| No facility/bucket pan/pit latrine | 1.956 | 1.868 | ||||
| WC/Flush toilet | 4.222 | 2.336 | ||||
| Kumasi Ventilated-Improved Pit (KVIP) | 7.443 | 4.713 | ||||
| Number of times seen cockroaches at home in the past 7 days (RC is never) | ||||||
| 1–3 Times | −0.469 | 1.481 | ||||
| 4 or more Times | 1.275 | 1.595 | ||||
| Don’t Know | 1.653 | 3.120 | ||||
| Distance to the nearest refuse collection point (RC is Less than 50 m) | ||||||
| 50 m and above | 2.265 | 2.661 | ||||
| Locality (RC is Agbogbloshie) | ||||||
| James Town | −8.600 | *** | 1.980 | |||
| Constant | 22.941 | *** | 2.114 | 24.26546 | *** | 3.514 |
| R2 | 0.251 | 0.397 | ||||
| F-Statistic | (3, 397) = 39.18 *** | (24, 376) = 9.45 *** | ||||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abu, M.; Codjoe, S.N.A. Experience and Future Perceived Risk of Floods and Diarrheal Disease in Urban Poor Communities in Accra, Ghana. Int. J. Environ. Res. Public Health 2018, 15, 2830. https://doi.org/10.3390/ijerph15122830
Abu M, Codjoe SNA. Experience and Future Perceived Risk of Floods and Diarrheal Disease in Urban Poor Communities in Accra, Ghana. International Journal of Environmental Research and Public Health. 2018; 15(12):2830. https://doi.org/10.3390/ijerph15122830
Chicago/Turabian StyleAbu, Mumuni, and Samuel Nii Ardey Codjoe. 2018. "Experience and Future Perceived Risk of Floods and Diarrheal Disease in Urban Poor Communities in Accra, Ghana" International Journal of Environmental Research and Public Health 15, no. 12: 2830. https://doi.org/10.3390/ijerph15122830
APA StyleAbu, M., & Codjoe, S. N. A. (2018). Experience and Future Perceived Risk of Floods and Diarrheal Disease in Urban Poor Communities in Accra, Ghana. International Journal of Environmental Research and Public Health, 15(12), 2830. https://doi.org/10.3390/ijerph15122830