Large-Scale Assessment of Function and Disability in Patients with Parkinson’s Disease Using the Functioning Disability Evaluation Scale-Adult Version


 ,
, 
Abstract
1. Introduction
2. Materials and Methods
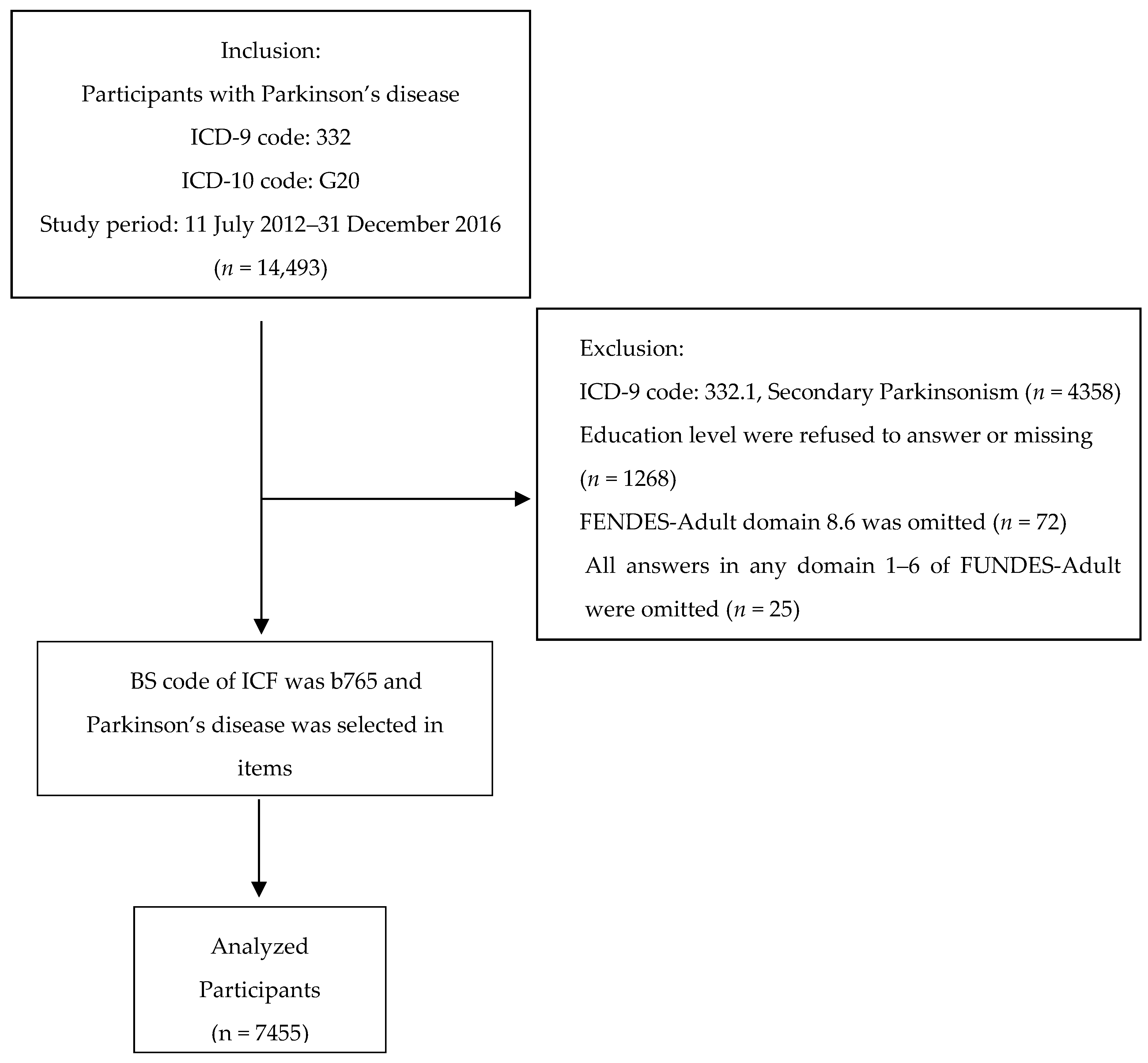
2.1. Sample
2.2. Instruments: Domain and Summary Scores of FUNDES-Adult
2.3. Procedure
3. Results
3.1. Sample Characteristics
3.2. Demographic Data and Walking Status
3.3. Correlation of Demographic Data and Walking Status
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Dorsey, E.R.; Constantinescu, R.; Thompson, J.P.; Biglan, K.M.; Holloway, R.G.; Kieburtz, K.; Marshall, F.J.; Ravina, B.M.; Schifitto, G.; Siderowf, A.; et al. Projected number of people with Parkinson disease in the most populous nations, 2005 through 2030. Neurology 2007, 68, 384–386. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.M.; Wu, R.M.; Lin, J.W.; Liu, Y.C.; Chang, C.H.; Lin, C.H. Time trends in the prevalence and incidence of Parkinson’s disease in Taiwan: A nationwide, population-based study. J. Formos. Med. Assoc. 2016, 115, 531–538. [Google Scholar] [CrossRef] [PubMed]
- Sethi, K. Levodopa unresponsive symptoms in Parkinson disease. Mov. Disord. 2008, 23 (Suppl. 3), S521–S533. [Google Scholar] [CrossRef] [PubMed]
- Archibald, N.; Miller, N.; Rochester, L. Neurorehabilitation in Parkinson disease. Handb. Clin. Neurol. 2013, 110, 435–442. [Google Scholar] [PubMed]
- Chaudhuri, K.R.; Schapira, A.H. Non-motor symptoms of Parkinson’s disease: Dopaminergic pathophysiology and treatment. Lancet Neurol. 2009, 8, 464–474. [Google Scholar] [CrossRef]
- Tolosa, E.; Wenning, G.; Poewe, W. The diagnosis of Parkinson’s disease. Lancet Neurol. 2006, 5, 75–86. [Google Scholar] [CrossRef]
- Schrag, A.; Ben-Shlomo, Y.; Quinn, N. How valid is the clinical diagnosis of Parkinson’s disease in the community? J. Neurol. Neurosurg. Psychiatry 2002, 73, 529–534. [Google Scholar] [CrossRef] [PubMed]
- Organization, W.H. International Classification of Functioning, Disability and Health: ICF; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Quittenbaum, B.H.; Grahn, B. Quality of life and pain in Parkinson’s disease: A controlled cross-sectional study. Park. Relat. Disord. 2004, 10, 129–136. [Google Scholar] [CrossRef]
- Pandya, M.; Kubu, C.S.; Giroux, M.L. Parkinson disease: Not just a movement disorder. Clevel. Clin. J. Med. 2008, 75, 856–864. [Google Scholar] [CrossRef]
- Andlin-Sobocki, P.; Jonsson, B.; Wittchen, H.U.; Olesen, J. Cost of disorders of the brain in Europe. Eur. J. Neurol. 2005, 12 (Suppl. 1), 1–27. [Google Scholar] [CrossRef]
- Bovolenta, T.M.; de Azevedo Silva, S.M.C.; Saba, R.A.; Borges, V.; Ferraz, H.B.; Felicio, A.C. Average annual cost of Parkinson’s disease in Sao Paulo, Brazil, with a focus on disease-related motor symptoms. Clin. Interv. Aging 2017, 12, 2095–2108. [Google Scholar] [CrossRef] [PubMed]
- Findley, L.; Aujla, M.; Bain, P.G.; Baker, M.; Beech, C.; Bowman, C.; Holmes, J.; Kingdom, W.K.; MacMahon, D.G.; Peto, V.; et al. Direct economic impact of Parkinson’s disease: A research survey in the United Kingdom. Mov. Disord. 2003, 18, 1139–1145. [Google Scholar] [CrossRef]
- Schedule, W.W.D.A. 2.0 WHODAS 2.0; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Liao, H.-F. Introduction to the application of the functioning scale of the disability evaluation system. Formosan J. Med. 2013, 17, 317–331. [Google Scholar]
- Chiu, W.T.; Yen, C.F.; Teng, S.W.; Liao, H.F.; Chang, K.H.; Chi, W.C.; Wang, Y.H.; Liou, T.H. Implementing disability evaluation and welfare services based on the framework of the International Classification of Functioning, Disability and Health: Experiences in Taiwan. BMC Health Serv. Res. 2013, 13, 416. [Google Scholar] [CrossRef] [PubMed]
- Teng, S.W.; Yen, C.F.; Liao, H.F.; Chang, K.H.; Chi, W.C.; Wang, Y.H.; Liou, T.H. Evolution of system for disability assessment based on the International Classification of Functioning, Disability, and Health: A Taiwanese study. J. Formos. Med. Assoc. 2013, 112, 691–698. [Google Scholar] [CrossRef]
- Üstün, T.B.; Kostanjsek, N.; Chatterji, S.; Rehm, J. Measuring Health and Disability: Manual for WHO Disability Assessment Schedule (WHODAS 2.0); World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Garin, O.; Ayuso-Mateos, J.L.; Almansa, J.; Nieto, M.; Chatterji, S.; Vilagut, G.; Alonso, J.; Cieza, A.; Svetskova, O.; Burger, H. Validation of the “World Health Organization Disability Assessment Schedule, WHODAS-2” in patients with chronic diseases. Health Qual. Life Outcomes 2010, 8, 51. [Google Scholar] [CrossRef] [PubMed]
- Noonan, V.K.; Kopec, J.A.; Noreau, L.; Singer, J.; Chan, A.; Mâsse, L.C.; Dvorak, M.F. Comparing the content of participation instruments using the International Classification of Functioning, Disability and Health. Health Qual. Life Outcomes 2009, 7, 93. [Google Scholar] [CrossRef] [PubMed]
- Chi, W.C.; Liou, T.H.; Wennie Huang, W.N.; Yen, C.F.; Teng, S.W.; Chang, I.C. Developing a disability determination model using a decision support system in Taiwan: A pilot study. J. Formos. Med. Assoc. 2013, 112, 473–481. [Google Scholar] [CrossRef] [PubMed]
- Chiu, T.Y.; Yen, C.F.; Chou, C.H.; Lin, J.D.; Hwang, A.W.; Liao, H.F.; Chi, W.C. Development of traditional Chinese version of World Health Organization disability assessment schedule 2.0 36–item (WHODAS 2.0) in Taiwan: Validity and reliability analyses. Res. Dev. Disabil. 2014, 35, 2812–2820. [Google Scholar] [CrossRef]
- Yen, C.F.; Hwang, A.W.; Liou, T.H.; Chiu, T.Y.; Hsu, H.Y.; Chi, W.C.; Wu, T.F.; Chang, B.S.; Lu, S.J.; Liao, H.F.; et al. Validity and reliability of the Functioning Disability Evaluation Scale-Adult Version based on the WHODAS 2.0–36 items. J. Formos. Med. Assoc. 2014, 113, 839–849. [Google Scholar] [CrossRef]
- Diamond, S.G.; Markham, C.H.; Hoehn, M.M.; McDowell, F.H.; Muenter, M.D. Effect of age at onset on progression and mortality in Parkinson’s disease. Neurology 1989, 39, 1187–1190. [Google Scholar] [CrossRef] [PubMed]
- Guillard, A.; Chastang, C.; Fenelon, G. [Long-term study of 416 cases of Parkinson disease. Prognostic factors and therapeutic implications]. Rev. Neurol. 1986, 142, 207–214. [Google Scholar] [PubMed]
- Jankovic, J.; Kapadia, A.S. Functional decline in Parkinson disease. Arch. Neurol. 2001, 58, 1611–1615. [Google Scholar] [CrossRef] [PubMed]
- Goetz, C.G.; Tanner, C.M.; Stebbins, G.T.; Buchman, A.S. Risk factors for progression in Parkinson’s disease. Neurology 1988, 38, 1841–1844. [Google Scholar] [CrossRef] [PubMed]
- Christofoletti, G.; McNeely, M.E.; Campbell, M.C.; Duncan, R.P.; Earhart, G.M. Investigation of factors impacting mobility and gait in Parkinson disease. Hum. Mov. Sci. 2016, 49, 308–314. [Google Scholar] [CrossRef]
- Kader, M.; Ullen, S.; Iwarsson, S.; Odin, P.; Nilsson, M.H. Factors Contributing to Perceived Walking Difficulties in People with Parkinson’s Disease. J. Parkinson’s Dis. 2017, 7, 397–407. [Google Scholar] [CrossRef]
- Ustun, T.B.; Chatterji, S.; Kostanjsek, N.; Rehm, J.; Kennedy, C.; Epping-Jordan, J.; Saxena, S.; von Korff, M.; Pull, C. Developing the World Health Organization Disability Assessment Schedule 2.0. Bull. World Health Organ. 2010, 88, 815–823. [Google Scholar] [CrossRef]
- Federici, S.; Bracalenti, M.; Meloni, F.; Luciano, J.V. World Health Organization disability assessment schedule 2.0: An international systematic review. Disabil. Rehabil. 2017, 39, 2347–2380. [Google Scholar] [CrossRef]
- Goetz, C.G.; Poewe, W.; Rascol, O.; Sampaio, C.; Stebbins, G.T.; Counsell, C.; Giladi, N.; Holloway, R.G.; Moore, C.G.; Wenning, G.K.; et al. Movement Disorder Society Task Force report on the Hoehn and Yahr staging scale: Status and recommendations. Mov. Disord. 2004, 19, 1020–1028. [Google Scholar] [CrossRef]
- Fernandez, H.H.; Lapane, K.L.; Ott, B.R.; Friedman, J.H. Gender differences in the frequency and treatment of behavior problems in Parkinson’s disease. SAGE Study Group. Systematic Assessment and Geriatric drug use via Epidemiology. Mov. Disord. 2000, 15, 490–496. [Google Scholar] [CrossRef]
- Kang, G.A.; Bronstein, J.M. Psychosis in nursing home patients with Parkinson’s disease. J. Am. Med. Dir. Assoc. 2004, 5, 167–173. [Google Scholar] [CrossRef]
- Kuroda, K.; Tatara, K.; Takatorige, T.; Shinsho, F. Effect of physical exercise on mortality in patients with Parkinson’s disease. Acta Neurol. Scand. 1992, 86, 55–59. [Google Scholar] [CrossRef]
- de Goede, C.J.; Keus, S.H.; Kwakkel, G.; Wagenaar, R.C. The effects of physical therapy in Parkinson’s disease: A research synthesis. Arch. Phys. Med. Rehabil. 2001, 82, 509–515. [Google Scholar] [CrossRef] [PubMed]
- Crizzle, A.M.; Newhouse, I.J. Is physical exercise beneficial for persons with Parkinson’s disease? Clin. J. Sport med. Off. J. Can. Acad. Sport Med. 2006, 16, 422–425. [Google Scholar] [CrossRef] [PubMed]
- Picillo, M.; Munhoz, R.P. Medical Management of Movement Disorders. Prog. Neurol. Surg. 2018, 33, 41–49. [Google Scholar] [PubMed]
- Lee, J.M.; Koh, S.B.; Chae, S.W.; Seo, W.K.; Kwon, D.Y.; Kim, J.H.; Oh, K.; Baik, J.S.; Park, K.W. Postural instability and cognitive dysfunction in early Parkinson’s disease. Can. J. Neurol. Sci. 2012, 39, 473–482. [Google Scholar] [CrossRef]
- Allcock, L.M.; Rowan, E.N.; Steen, I.N.; Wesnes, K.; Kenny, R.A.; Burn, D.J. Impaired attention predicts falling in Parkinson’s disease. Park. Relat. Disord. 2009, 15, 110–115. [Google Scholar] [CrossRef]
- van der Kolk, N.M.; de Vries, N.M.; Penko, A.L.; van der Vlugt, M.; Mulder, A.A.; Post, B.; Alberts, J.L.; Bloem, B.R. A remotely supervised home-based aerobic exercise programme is feasible for patients with Parkinson’s disease: Results of a small randomised feasibility trial. J. Neurol. Neurosurg. Psychiatry 2018, 89, 1003–1005. [Google Scholar] [CrossRef]
- Ginis, P.; Nieuwboer, A.; Dorfman, M.; Ferrari, A.; Gazit, E.; Canning, C.G.; Rocchi, L.; Chiari, L.; Hausdorff, J.M.; Mirelman, A. Feasibility and effects of home-based smartphone-delivered automated feedback training for gait in people with Parkinson’s disease: A pilot randomized controlled trial. Park. Relat. Disord. 2016, 22, 28–34. [Google Scholar] [CrossRef]
- Vanbellingen, T.; Nyffeler, T.; Nigg, J.; Janssens, J.; Hoppe, J.; Nef, T.; Muri, R.M.; van Wegen, E.E.H.; Kwakkel, G.; Bohlhalter, S. Home based training for dexterity in Parkinson’s disease: A randomized controlled trial. Park. Relat. Disord. 2017, 41, 92–98. [Google Scholar] [CrossRef]


{kind=link}
| Variables | N/% | Mean ± SD | p-Value c |
|---|---|---|---|
| Gender | 0.8439 | ||
| Male | 3719/49.89 | ||
| Female | 3736/50.11 | ||
| Age (years) | <0.0001 | ||
| 18–49 | 150/2.01 | 44.20–5.47 | |
| 50–64 | 1434/19.24 | 59.70 ± 3.84 | |
| 65–74 | 2175/29.18 | 70.69 ± 2.89 | |
| ≧75 | 3696/49.58 | 81.19 ± 4.49 | |
| Total | 7455 | 73.25 ± 10.07 | |
| Residence | <0.0001 | ||
| Community dwelling | 6528/87.57 | ||
| Institution | 927/12.43 | ||
| Work Status | <0.0001 | ||
| Employment | 175/2.35 | ||
| Unemployment | 7280/97.65 | ||
| Education level | <0.0001 | ||
| Above college | 240/3.22 | ||
| Senior High | 850/11.40 | ||
| Junior High | 1036/13.90 | ||
| Primary (include no formal education) | 3991/53.53 | ||
| Illiterate | 1338/17.95 | ||
| Family Economic Status | <0.0001 | ||
| Average | 7381/99.01 | ||
| middle low & low | 74/0.99 | ||
| Urbanization level | <0.0001 | ||
| Urban | 3910/52.45 | ||
| Suburban | 2644/35.47 | ||
| Rural | 901/12.09 | ||
| Domain 8.6 (Motor action) | |||
| Walk for 3 m and return | <0.0001 | ||
| 0 | 595/7.98 | ||
| 1 | 846/11.35 | ||
| 2 | 1128/15.13 | ||
| 3 | 1325/17.77 | ||
| 4 | 3561/47.77 | ||
| Modified Hoehn–Yahr Stage | <0.0001 | ||
| 3 | 2224/29.83 | ||
| 4 | 3140/42.12 | ||
| 5 | 2091/28.05 | ||
| Cognition (domain 1) a | |||
| 1-1 | 7435 | 2.02 ± 1.42 | |
| 1-2 | 7440 | 2.21 ± 1.33 | |
| 1-3 | 7321 | 2.44 ± 1.38 | |
| 1-4 | 6363 | 2.78 ± 1.28 | |
| 1-5 | 7449 | 1.50 ± 1.40 | |
| 1-6 | 7441 | 1.90 ± 1.44 | |
| Mobility (domain 2) a | |||
| 2-1 | 7390 | 3.23 ± 1.04 | |
| 2-2 | 7453 | 2.69 ± 1.34 | |
| 2-3 | 7436 | 2.76 ± 1.33 | |
| 2-4 | 7420 | 3.18 ± 1.13 | |
| 2-5 | 7267 | 3.40 ± 0.95 | |
| FUNDES-Adult b | |||
| Cognition (domain 1) | 7455 | 56.76 ± 30.56 | |
| Mobility (domain 2) | 7455 | 80.47 ± 24.80 | |
| Self-care (domain 3) | 7455 | 72.03 ± 28.65 | |
| Getting along (domain4) | 7455 | 65.68 ± 31.09 | |
| Life activities (domain 5-1) | 7455 | 87.57 ± 21.74 | |
| Participation (domain 6) | 7455 | 57.19 ± 24.19 | |
| Summary | 7455 | 67.17 ± 22.02 |
| Variables | Walk Status a | p-Value f | ||
|---|---|---|---|---|
| Ambulatory (n = 595) | Assisted Ambulatory (n = 3299) | Not Ambulatory (n = 3561) | ||
| Gender (%) | ||||
| Male (n = 3719) | 8.87 | 45.07 | 46.06 | <0.0001 d |
| Female (n = 3736) | 7.09 | 43.44 | 49.46 | <0.0001 d |
| p value | 0.0077 d | 0.3561 d | 0.0237 d | |
| Age (years) (%, Mean ± SD) | ||||
| 18–49 (n = 150) | 34.00, 43.44 ± 5.34 | 54.00, 44.36 ± 5.73 | 12.00, 45.68 ± 4.47 | <0.0001 d |
| 50–64 (n = 1434) | 19.60, 58.81 ± 4.01 | 58.86, 59.62 ± 3.86 | 21.55, 60.70 ± 3.37 | <0.0001 d |
| 65–74 (n = 2175) | 7.77, 69.99 ± 2.86 | 50.11, 70.62 ± 2.89 | 42.11, 70.89 ± 2.87 | <0.0001 d |
| ≧75 (n = 3696) | 2.54, 78.89 ± 2.88 | 34.74, 80.47 ± 4.13 | 62.72, 81.69 ± 4.65 | <0.0001 d |
| p value | <0.0001 d | <0.0001 d | <0.0001 d | |
| Total | 63.84 ± 10.39 | 71.00 ± 9.98 | 76.91 ± 8.32 | <0.0001 e |
| Residence (%) | ||||
| Community dwelling (n = 6528) | 8.96 | 48.38 | 42.66 | <0.0001 d |
| Institution (n = 927) | 1.08 | 15.21 | 83.71 | <0.0001 d |
| p value | <0.0001 d | <0.0001 d | <0.0001 d | |
| Work Status (%) | ||||
| Employment (n = 175) | 40.00 | 51.43 | 8.57 | <0.0001 d |
| Unemployment (n = 7280) | 7.21 | 44.08 | 48.71 | <0.0001 d |
| p value | <0.0001 d | <0.0001 d | <0.0001 d | |
| Education level (%) | ||||
| Above college (n = 240) | 8.33 | 45.83 | 45.83 | <0.0001 d |
| Senior High (n = 850) | 10.71 | 47.65 | 41.65 | <0.0001 d |
| Junior High (n = 1036) | 14.67 | 52.80 | 32.53 | <0.0001 d |
| Primary (include no formal education) (n = 3991) | 7.22 | 44.88 | 47.91 | <0.0001 d |
| Illiterate (n = 1338) | 3.29 | 33.33 | 63.38 | <0.0001 d |
| p value | <0.0001 d | <0.0001 d | <0.0001 d | |
| Modified Hoehn-Yahr Stage | ||||
| Stage 3 (n = 2224) | 19.56 | 61.92 | 18.53 | <0.0001 d |
| Stage 4 (n = 3140) | 4.36 | 49.84 | 45.80 | <0.0001 d |
| Stage 5 (n = 2091) | 1.10 | 17.07 | 81.83 | <0.0001 d |
| p value | <0.0001 d | <0.0001 d | <0.0001 d | |
| Cognition (domain 1) c (Mean ± SD) | ||||
| 1-1 (Concentration) | 0.88 ± 1.07 | 1.50 ± 1.22 | 2.69 ± 1.31 | <0.0001 e |
| 1-2 (Remembering to do important things) | 1.19 ± 1.05 | 1.75 ± 1.14 | 2.80 ± 1.26 | <0.0001 e |
| 1-3 (Problem-solving) | 1.23 ± 1.22 | 1.97 ± 1.26 | 3.08 ± 1.19 | <0.0001 e |
| 1-4 (Learning a new task) | 1.55 ± 1.27 | 2.32 ± 1.23 | 3.36 ± 0.99 | <0.0001 e |
| 1-5 (Understanding) | 0.49 ± 0.85 | 1.00 ± 1.10 | 2.14 ± 1.43 | <0.0001 e |
| 1-6 (Conversation) | 0.73 ± 1.04 | 1.40 ± 1.21 | 2.56 ± 1.37 | <0.0001 e |
| Mobility (domain 2) c (Mean ± SD) | ||||
| 2-1 (Standing for long periods) | 1.77 ± 1.28 | 2.84 ± 1.02 | 3.84 ± 0.43 | <0.0001 e |
| 2-2 (Standing up from sitting) | 0.66 ± 0.95 | 2.03 ± 1.10 | 3.64 ± 0.70 | <0.0001 e |
| 2-3 (Moving around inside home) | 0.59 ± 0.85 | 2.13 ± 1.10 | 3.71 ± 0.62 | <0.0001 e |
| 2-4 (Getting out of) | 1.29 ± 1.26 | 2.80 ± 1.06 | 3.85 ± 0.44 | <0.0001 e |
| 2-5 (Walking a long distance) | 1.91 ± 1.28 | 3.11 ± 0.93 | 3.92 ± 0.32 | <0.0001 e |
| FUNDES-Adult b (Mean ± SD) | ||||
| Cognition (domain 1) | 27.90 ± 23.19 | 44.90 ± 25.98 | 72.58 ± 26.85 | <0.0001 e |
| Mobility (domain 2) | 37.06 ± 24.94 | 70.88 ± 21.93 | 96.61 ± 8.82 | <0.0001 e |
| Self-care (domain 3) | 28.97 ± 23.80 | 59.73 ± 24.78 | 90.62 ± 16.10 | <0.0001 e |
| Getting along (domain 4) | 34.76 ± 28.32 | 54.77 ± 29.02 | 80.95 ± 24.63 | <0.0001 e |
| Life activities (domain 5-1) | 56.54 ± 29.74 | 82.07 ± 22.59 | 97.85 ± 8.63 | <0.0001 e |
| Participation (domain 6) | 35.74 ± 19.95 | 50.60 ± 21.20 | 66.89 ± 23.05 | <0.0001 e |
| Summary | 35.66 ± 18.08 | 57.84 ± 18.41 | 81.07 ± 14.37 | <0.0001 e |
| β | Odds Ratio(Adjusted) b | 95% Wald Confidence Limits | p-Value | ||
|---|---|---|---|---|---|
| Age (ref. = 18–49) | |||||
| 50–64 | 0.357 | 1.429 | 0.755 | 2.705 | 0.2729 |
| 65–74 | 0.7325 | 2.08 | 1.111 | 3.895 | 0.0221 |
| ≧75 | 1.2065 | 3.342 | 1.791 | 6.235 | 0.0001 |
| Residence (ref. = Community dwelling) | |||||
| Institution | 1.0062 | 2.735 | 2.149 | 3.48 | <0.0001 |
| Modified Hoehn-Yahr Stage (ref. = stage 3) | |||||
| Stage 4 | 0.5777 | 1.782 | 1.51 | 2.103 | <0.0001 |
| Stage 5 | 1.5712 | 4.813 | 3.946 | 5.87 | <0.0001 |
| FUNDES-Adult Standardized Score | |||||
| Cognition | 0.00881 | 1.009 | 1.006 | 1.011 | <0.0001 |
| Mobility | 0.0925 | 1.097 | 1.09 | 1.103 | <0.0001 |
| β | Odds Ratio (Adjusted) b | 95% Wald Confidence Limits | p-Value | ||
|---|---|---|---|---|---|
| Age (ref. = 18–49) | |||||
| 50–64 | 0.7268 | 2.068 | 0.926 | 4.62 | 0.0763 |
| 65–74 | 1.1036 | 3.015 | 1.367 | 6.649 | 0.0062 |
| ≧75 | 1.5754 | 4.833 | 2.2 | 10.617 | <0.0001 |
| Residence (ref. = Community dwelling) | |||||
| Institution | 0.9376 | 2.554 | 1.964 | 3.321 | <0.0001 |
| Modified Hoehn-Yahr Stage (ref. = stage 3) | |||||
| Stage 4 | 0.4128 | 1.511 | 1.245 | 1.835 | <0.0001 |
| Stage 5 | 1.3037 | 3.683 | 2.926 | 4.635 | <0.0001 |
| FUNDES-Adult Raw Score | |||||
| Cognition Q1 | 0.2654 | 1.304 | 1.203 | 1.413 | <0.0001 |
| Cognition Q2 | −0.1878 | 0.829 | 0.758 | 0.906 | <0.0001 |
| Mobility Q1 | 0.258 | 1.294 | 1.092 | 1.534 | 0.0029 |
| Mobility Q2 | 0.5845 | 1.794 | 1.583 | 2.033 | <0.0001 |
| Mobility Q3 | 0.7469 | 2.111 | 1.833 | 2.43 | <0.0001 |
| Mobility Q5 | 0.5 | 1.649 | 1.342 | 2.025 | <0.0001 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, T.-H.; Liou, T.-H.; Chou, K.-R.; Chi, W.-C.; Yen, C.-F.; Liao, H.-F.; Tseng, I.-J. Large-Scale Assessment of Function and Disability in Patients with Parkinson’s Disease Using the Functioning Disability Evaluation Scale-Adult Version. Int. J. Environ. Res. Public Health 2018, 15, 2788. https://doi.org/10.3390/ijerph15122788
Hsu T-H, Liou T-H, Chou K-R, Chi W-C, Yen C-F, Liao H-F, Tseng I-J. Large-Scale Assessment of Function and Disability in Patients with Parkinson’s Disease Using the Functioning Disability Evaluation Scale-Adult Version. International Journal of Environmental Research and Public Health. 2018; 15(12):2788. https://doi.org/10.3390/ijerph15122788
Chicago/Turabian StyleHsu, Tzu-Herng, Tsan-Hon Liou, Kuei-Ru Chou, Wen-Chou Chi, Chia-Feng Yen, Hua-Fang Liao, and Ing-Jy Tseng. 2018. "Large-Scale Assessment of Function and Disability in Patients with Parkinson’s Disease Using the Functioning Disability Evaluation Scale-Adult Version" International Journal of Environmental Research and Public Health 15, no. 12: 2788. https://doi.org/10.3390/ijerph15122788
APA StyleHsu, T.-H., Liou, T.-H., Chou, K.-R., Chi, W.-C., Yen, C.-F., Liao, H.-F., & Tseng, I.-J. (2018). Large-Scale Assessment of Function and Disability in Patients with Parkinson’s Disease Using the Functioning Disability Evaluation Scale-Adult Version. International Journal of Environmental Research and Public Health, 15(12), 2788. https://doi.org/10.3390/ijerph15122788