
Lower Physical Performance in Colder Seasons and Colder Houses: Evidence from a Field Study on Older People Living in the Community

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measurement of Physical Performance
2.3. Measurement of Indoor Temperature
2.4. Statistical Analysis
3. Results
3.1. Baseline Analysis
3.2. Seasonal Differences of Physical Performance
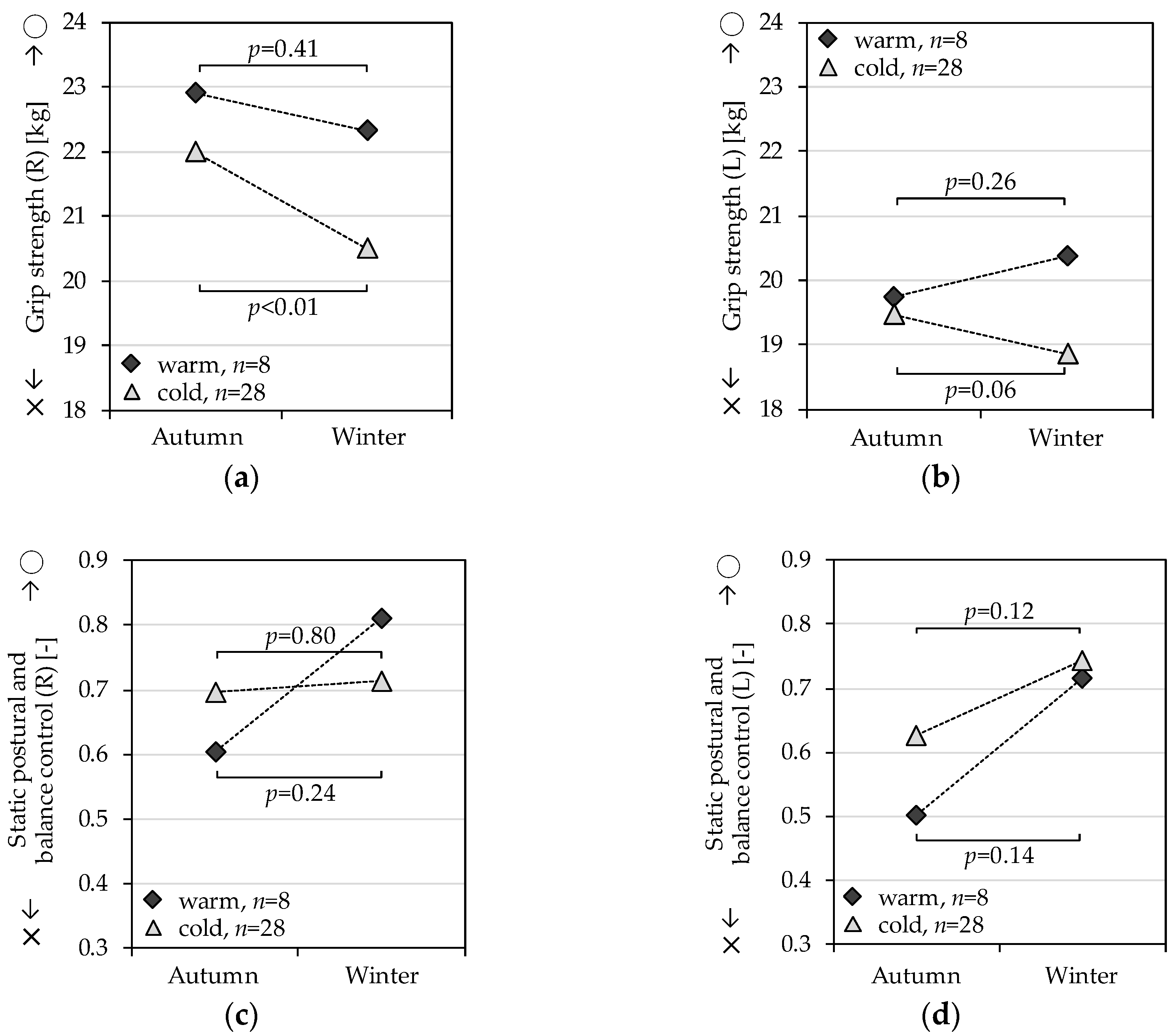
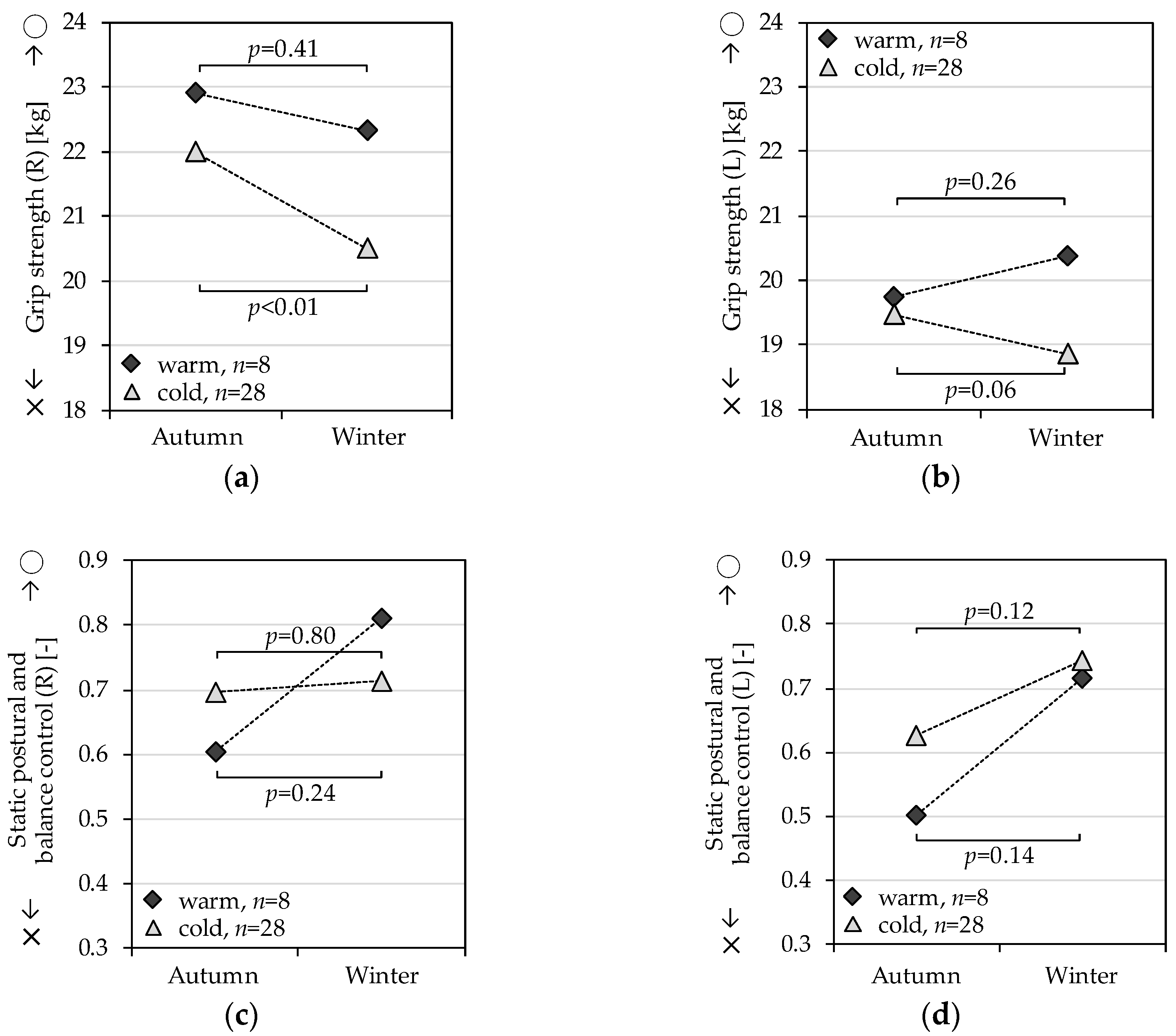
3.3. Influence from Cold Housing on Seasonal Differences of Physical Performance
4. Discussion
Limitations
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Rantanen, T.; Guralnik, J.M.; Foley, D.; Masaki, K.; Leveille, S.; Curb, J.D.; White, L. Midlife hand grip strength as a predictor of old age disability. JAMA 1999, 281, 558–560. [Google Scholar] [CrossRef] [PubMed]
- Rantanen, T.; Masaki, K.; Foley, D.; Izmirlian, G.; White, L.; Guralnik, J.M. Grip strength changes over 27 years in Japanese-American men. J. Appl. Physiol. 1998, 85, 2047–2053. [Google Scholar] [PubMed]
- Visser, M.; Goodpaster, B.H.; Kritchevsky, S.B.; Newman, A.B.; Nevitt, M.; Rubin, S.M.; Simonsick, E.M.; Harris, T.B. Muscle mass, muscle strength, and muscle fat infiltration as predictors of incident mobility limitations in well-functioning older persons. J. Gerontol. 2005, 60, 324–333. [Google Scholar] [CrossRef]
- Karlsson, M.K.; Ribom, E.; Nilsson, J.A.; Ljunggren, O.; Ohlsson, C.; Mellstrom, D.; Lorentzon, M.; Mallmin, H.; Stefanik, M.; Lapidus, J.; et al. Inferior physical performance tests in 10,998 men in the MrOS study is associated with recurrent falls. Age Ageing 2012, 41, 740–746. [Google Scholar] [CrossRef] [PubMed]
- Mohler, M.J.; Wendel, C.S.; Taylor-piliae, R.E.; Toosizadeh, N.; Najafi, B. Motor performance and physical activity as predictors of prospective falls in community-dwelling older adults by frailty level: Application of wearable technology. Gerontology 2016, 62, 654–664. [Google Scholar] [CrossRef] [PubMed]
- Delbaere, K.; Crombez, G.; Vanderstraeten, G.; Willems, T.; Cambier, D. Fear-related avoidance of activities, falls and physical frailty, A prospective community-based cohort study. Age Ageing 2004, 33, 368–373. [Google Scholar] [CrossRef] [PubMed]
- Beaudart, C.; Reginster, J.Y.; Petermans, J.; Gillain, S.; Quabron, A.; Locquet, M.; Slomian, J.; Buckinx, F.; Bruyère, O. Quality of life and physical components linked to sarcopenia: The SarcoPhAge study. Exp. Gerontol. 2015, 69, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Cheung, S.S.; Reynolds, L.F.; Macdonald, M.A.; Tweedie, C.L.; Urguhart, R.L.; Westwood, D.A. Effects of local and core body temperature on grip force modulation during movement-induced load force fluctuations. Eur. J. Appl. Physiol. 2008, 103, 59–69. [Google Scholar] [CrossRef] [PubMed]
- Piedrahita, H.; Oksa, J.; Rntamäki, H.; Malm, C. Effect of local leg cooling on upper limb trajectories and muscle function and whole body dynamic balance. Eur. J. Appl. Physiol. 2009, 105, 429–438. [Google Scholar] [CrossRef] [PubMed]
- Piedrahita, H.; Oksa, J.; Malm, C.; Sormunen, E.; Rintamäki, H. Effects of cooling and clothing on vertical trajectories of the upper arm and muscle functions during repetitive light work. Eur. J. Appl. Physiol. 2008, 104, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Bennett, A.F. Thermal dependence of muscle function. Am. J. Physiol. 1984, 247, 217–229. [Google Scholar]
- Oksa, J.; Rintamäki, H.; Rissanen, S. Muscle performance and electromyogram activity of the lower leg muscles with different levels of cold exposure. Eur. J. Appl. Physiol. 1997, 75, 484–490. [Google Scholar] [CrossRef] [PubMed]
- Collins, K.J.; Easton, J.C.; Belfield-Smith, H.; Exton-Smith, A.N.; Pluck, R.A. Effects of age on body temperature and blood pressure in cold environments. Clin. Sci. 1985, 69, 465–470. [Google Scholar] [CrossRef] [PubMed]
- Budd, G.M. Ergonomic aspects of cold stress and cold adaptation. Scand. J. Work Environ. Health 1989, 15, 15–26. [Google Scholar] [PubMed]
- Lindemann, U.; Oksa, J.; Skelton, D.A.; Beyer, N.; Klenk, J.; Zscheile, J.; Becker, C. Effect of cold indoor environment on physical performance of older women living in the community. Age Ageing 2014, 45, 571–575. [Google Scholar] [CrossRef] [PubMed]
- Turner, R.M.; Hayen, A.; Dunsmuir, W.T.M.; Finch, C.F. Air temperature and the incidence of fall-related hip fracture hospitalisations in older people. Osteoporos. Int. 2011, 22, 1183–1189. [Google Scholar] [CrossRef] [PubMed]
- Saeki, K.; Obayashi, K.; Kurumatani, N. Short-term effects of instruction in home heating on indoor temperature and blood pressure in elderly people: A randomized controlled trial. J. Hypertens. 2015, 33, 2338–2343. [Google Scholar] [CrossRef] [PubMed]
- Saeki, K.; Obayashi, K.; Iwamoto, J.; Tone, N.; Okamoto, N.; Tomioka, K.; Kurumatani, N. Stronger association of indoor temperature than outdoor temperature with blood pressure in colder months. J. Hypertens. 2014, 32, 1582–1589. [Google Scholar] [CrossRef] [PubMed]
- Baltes, M.M.; Maas, I.; Wilms, H.U.; Borchelt, M.; Little, T.D. Everyday competence in old and very old age: Theoretical considerations and empirical findings. In The Berlin Aging Study: Aging from 70 to 10; Baltes, P.B., Mayer, K.U., Eds.; Cambridge University Press: New York, NY, USA, 1999; pp. 384–402. [Google Scholar]
- Sunikka-Blank, M.; Iwafune, Y. Sustainable building in Japan—Observations on a market transformation policy. Environ. Policy Gov. 2011, 21, 351–363. [Google Scholar] [CrossRef]
- Ministry of Education, Culture, Sports, Science and Technology. Deployment Plan for Physical Performance Test; MEXT: Tokyo, Japan, 2010. (In Japanese)
- Podsiadlo, D.; Richardson, S. The Timed Up & Go: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Mathias, S.; Nayak, U.S.L.; Isaacs, B. Balance in the elderly patient: The “Get-up and Go” test. Arch. Phys. Med. Rehabil. 1986, 67, 387–389. [Google Scholar] [PubMed]
- Public Health England; Shannon, K.; Stephen, D.; Angie, B. Cold Weather Plan for England: Protecting Health and Reducing Harm from Cold Weather; Public Health England: London, UK, 2015.
- Schone, D.; Valenzuela, T.; Lord, S.R.; Bruin, E.D. The effect of interactive cognitive-motor training in reducing fall risk in older people: A systematic review. BMC Geriatr. 2014, 14. [Google Scholar] [CrossRef] [PubMed]
- Wood, L.R.; Blagojevic-Bucknall, M.; Stynes, S.; D’Cruz, D.; Mullis, R.; Whittle, R.; Peat, G.; Foster, N.E. Impairment-targeted exercises for older adults with knee pain: A proof-of-principle study (TargET-Knee-Pain). BMC Musculoskel. Disord. 2016, 17. [Google Scholar] [CrossRef] [PubMed]
- Howe, T.E.; Rochester, L.; Neil, F.; Skelton, D.A.; Ballinger, C. Exercise for improving balance in older people. Cochrane Database Syst. Rev. 2011, 9. [Google Scholar] [CrossRef]
- Johansson, G.; Jarnlo, G. Balance training in 70-year-old women. Physiother. Theory Pract. 1991, 7, 121–125. [Google Scholar] [CrossRef]
- Weerdesteyn, V.; Rijken, H.; Geurts, A.C.; Smits-Engelsman, B.C.; Mulder, T.; Duysens, J. A five-week exercise program can reduce falls and improve obstaxle avoidance in the elderly. Gerontology 2006, 52, 131–141. [Google Scholar] [CrossRef] [PubMed]
- Wolsfon, L.; Whipple, R.; Derby, C.; Judge, J.; King, M.; Amerman, P.; Schmidt, J.; Smyers, D. Balance and strength training in older adults: Intervention gains and Tai Chi maintenance. J. Am. Geriatr. Soc. 1996, 44, 498–506. [Google Scholar] [CrossRef]
- Sallinen, J.; Stenholm, S.; Heliövaara, M.; Sainio, P.; Koskinen, S. Hand-grip strength cut points to screen older persons at risk for mobility limitation. J. Am. Geriatr. Soc. 2010, 58, 1721–1726. [Google Scholar] [CrossRef] [PubMed]
- Rantanen, T. Muscle strength, disability and mortality. Scand. J. Med. Sci. Sports 2003, 13, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Taekema, D.G.; Gussekloo, J.; Maier, A.B.; Westendorp, R.G.; de Craen, A.J. Handgrip strength as a predictor of functional, psychological and social health. A prospective population-based study among the oldest old. Age Ageing 2010, 39, 331–337. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W. Hand-grip dynamometry predicts future out-comes in aging adults. J. Geriatr. Phys. Ther. 2008, 31, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Ling, C.H.; Taekema, D.; de Craen, A.J.; Gussekloo, J.; Westendorp, R.G.; Maier, A.B. Handgrip strength and mortality in the oldest old population: The Leiden 85-plus study. CMAJ 2010, 182, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Ramos, N.M.M.; Almeida, R.M.S.F.; Simões, M.L.; Pereira, P.F. Knowledge discovery of indoor environment patterns in mild climate countries based on data mining applied to in-situ measurements. Sustain. Cities Soc. 2017, 30, 37–48. [Google Scholar] [CrossRef]
- Trevisan, C.; Veronese, N.; Maggi, S.; Baggio, G.; Toffanello, E.D.; Zambon, S.; Sartori, L.; Musacchio, E.; Perissinotto, E.; Crepaldi, G.; et al. Factors influencing transitions between frailty states in elderly adults: The Progetto Veneto Anziani longitudinal study. J. Am. Geriatr. Soc. 2016. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variable | Participants from Physical Performance Assessment (n = 98) | Participants with Indoor Temperature Measurement (n = 36) | ||
|---|---|---|---|---|
| Age, (years), mean (SD) | 79.43 | (7.69) | 81.38 | (5.81) |
| BMI, (kg/m2), mean (SD) | 22.73 | (3.13) | 22.85 | (3.12) |
| Female, n (%) | 54 | (55.10) | 19 | (52.78) |
| Economic satisfaction, n (%) | ||||
| Very satisfied | 9 | (9.18) | 6 | (16.67) |
| Somewhat satisfied | 67 | (68.37) | 20 | (55.56) |
| Not very satisfied | 14 | (15.29) | 7 | (19.44) |
| Not satisfied at all | 7 | (7.14) | 3 | (8.33) |
| No answer | 1 | (1.02) | 0 | (0.0) |
| Building age, n (%) | ||||
| 0–10 years | 11 | (11.22) | 5 | (13.89) |
| 11–20 years | 9 | (9.18) | 2 | (5.56) |
| 21–30 years | 24 | (24.49) | 7 | (19.44) |
| 31–40 years | 18 | (18.37) | 9 | (25.00) |
| More than 41 years | 35 | (35.71) | 13 | (36.11) |
| Window glass panes, n (%) | ||||
| One glass pane | 71 | (72.45) | 26 | (72.22) |
| Two glass panes | 27 | (27.55) | 10 | (27.78) |
| Room temperature, (°C) mean (SD) | ||||
| Living room | 16.76 | (1.64) | ||
| Bedroom | 15.46 | (1.83) | ||
| Dressing room | 14.59 | (1.91) | ||
| Variable | Autumn | Winter | p-Value | ||
|---|---|---|---|---|---|
| Grip strength, (kg), R, n = 98 | 21.47 | (7.33) | 20.05 | (7.25) | <0.0001 |
| Grip strength, (kg), L, n = 98 | 19.71 | (6.84) | 19.09 | (7.12) | 0.009 |
| Static postural and balance control, (-), R, n = 94 | 0.71 | (0.41) | 0.61 | (0.50) | 0.018 |
| Static postural and balance control, (-), L, n = 93 | 0.68 | (0.46) | 0.59 | (0.45) | 0.020 |
| Balance and gait function, (sec), R, n = 98 | 12.57 | (8.77) | 12.61 | (7.39) | 0.938 |
| Balance and gait function, (sec), L, n = 98 | 12.79 | (10.30) | 12.58 | (7.32) | 0.743 |
| Variable | Age (Years) | BMI (kg/m2) | Sex | Economic Satisfaction |
|---|---|---|---|---|
| Grip strength, (kg), R, n = 98 | 0.00 | 0.00 | −0.02 | 0.01 |
| Grip strength, (kg), L, n = 98 | 0.00 | 0.00 | 0.00 | −0.02 |
| Static postural and balance control, (-), R, n = 94 | 0.00 | −0.01 | −0.40 | −0.26 |
| Static postural and balance control, (-), L, n = 93 | −0.01 | 0.00 | 0.30 | 0.02 |
| All variables were not significant. | ||||
| Variable | Cold | Warm | p-Value | ||
|---|---|---|---|---|---|
| Sex, n (%) | |||||
| Male | 12 | (42.85) | 5 | (62.50) | 0.434 |
| Female | 16 | (57.14) | 3 | (37.50) | |
| Age, (years), mean (SD) | 82.08 | 5.78 | 79.13 | 6.10 | 0.221 |
| BMI, (kg/m2), mean (SD) | 22.79 | 3.14 | 23.05 | 3.46 | 0.846 |
| Economic satisfaction, n (%) | |||||
| Very satisfied | 0 | (0.00) | 0 | (0.00) | 0.546 |
| Somewhat satisfied | 12 | (42.85) | 5 | (62.50) | |
| Not very satisfied | 13 | (46.43) | 2 | (25.00) | |
| Not satisfied at all | 3 | (10.71) | 1 | (12.50) | |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hayashi, Y.; Schmidt, S.M.; Malmgren Fänge, A.; Hoshi, T.; Ikaga, T. Lower Physical Performance in Colder Seasons and Colder Houses: Evidence from a Field Study on Older People Living in the Community. Int. J. Environ. Res. Public Health 2017, 14, 651. https://doi.org/10.3390/ijerph14060651
Hayashi Y, Schmidt SM, Malmgren Fänge A, Hoshi T, Ikaga T. Lower Physical Performance in Colder Seasons and Colder Houses: Evidence from a Field Study on Older People Living in the Community. International Journal of Environmental Research and Public Health. 2017; 14(6):651. https://doi.org/10.3390/ijerph14060651
Chicago/Turabian StyleHayashi, Yukie, Steven M. Schmidt, Agneta Malmgren Fänge, Tanji Hoshi, and Toshiharu Ikaga. 2017. "Lower Physical Performance in Colder Seasons and Colder Houses: Evidence from a Field Study on Older People Living in the Community" International Journal of Environmental Research and Public Health 14, no. 6: 651. https://doi.org/10.3390/ijerph14060651
APA StyleHayashi, Y., Schmidt, S. M., Malmgren Fänge, A., Hoshi, T., & Ikaga, T. (2017). Lower Physical Performance in Colder Seasons and Colder Houses: Evidence from a Field Study on Older People Living in the Community. International Journal of Environmental Research and Public Health, 14(6), 651. https://doi.org/10.3390/ijerph14060651