
Prevalence and Risk Factors of Low Health Literacy: A Community-Based Study in Shanghai, China

Abstract
:1. Introduction
2. Materials and Methods
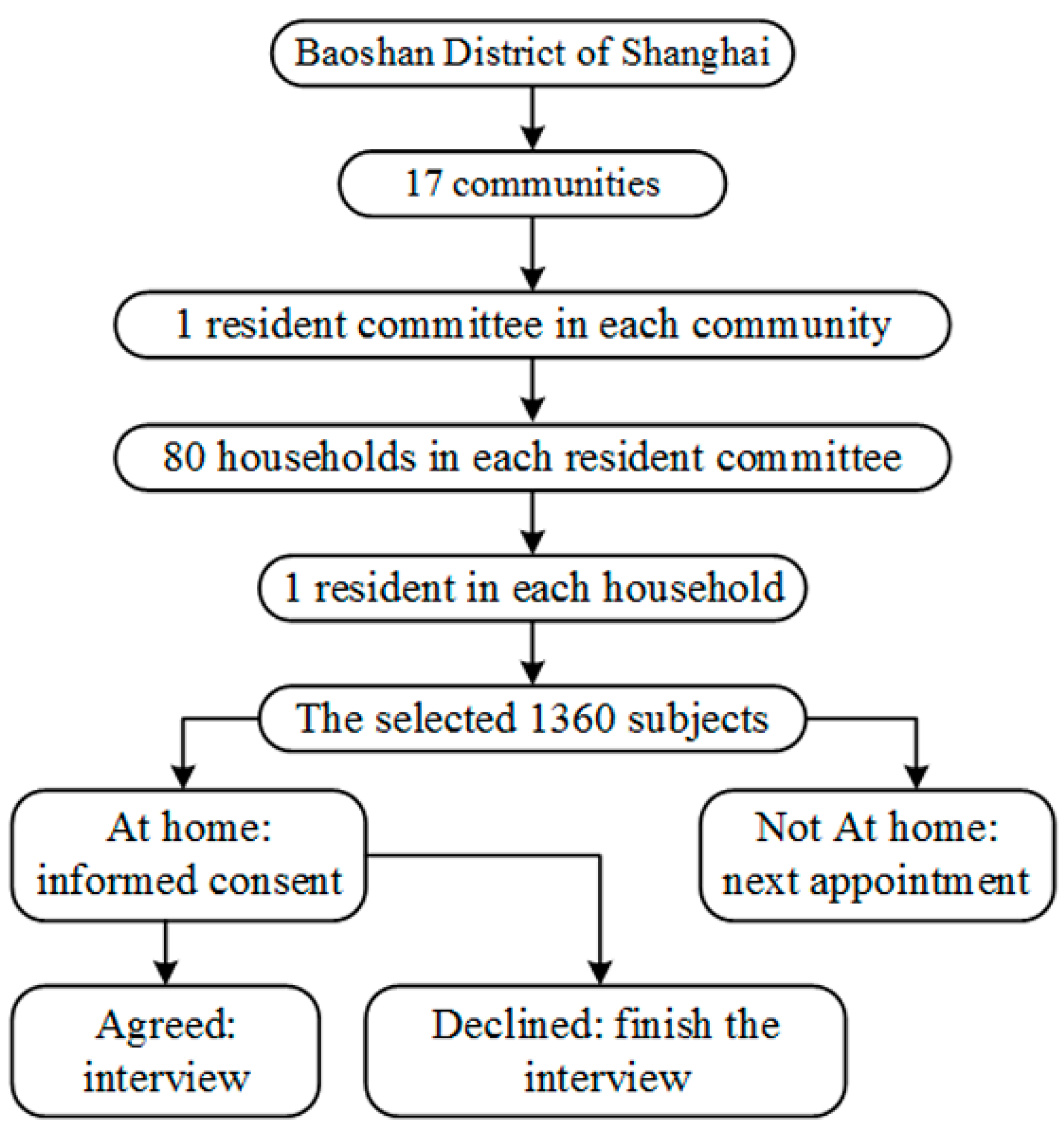
2.1. Study Population and Sampling Design
2.2. Data Collection
2.3. Statistical Analysis
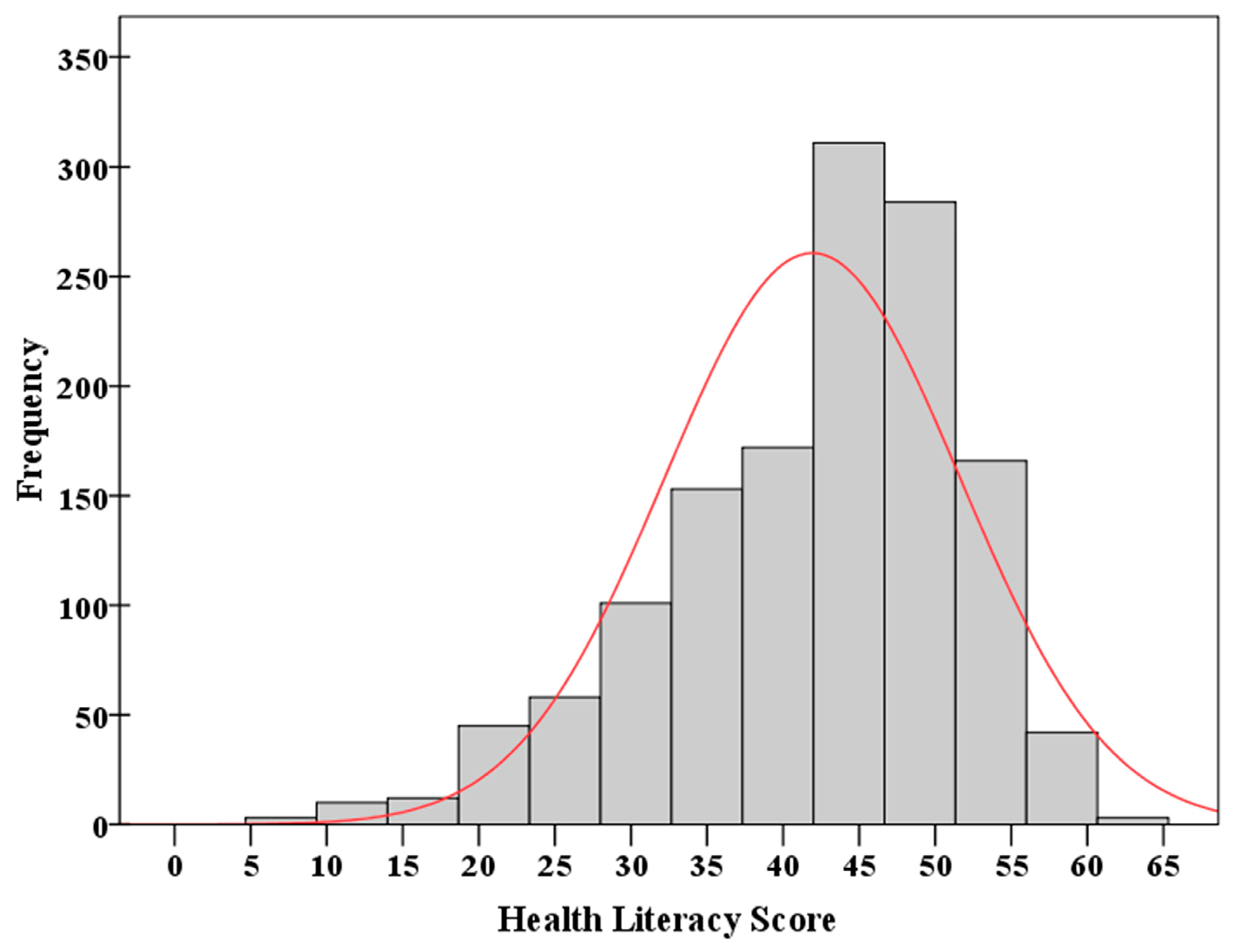
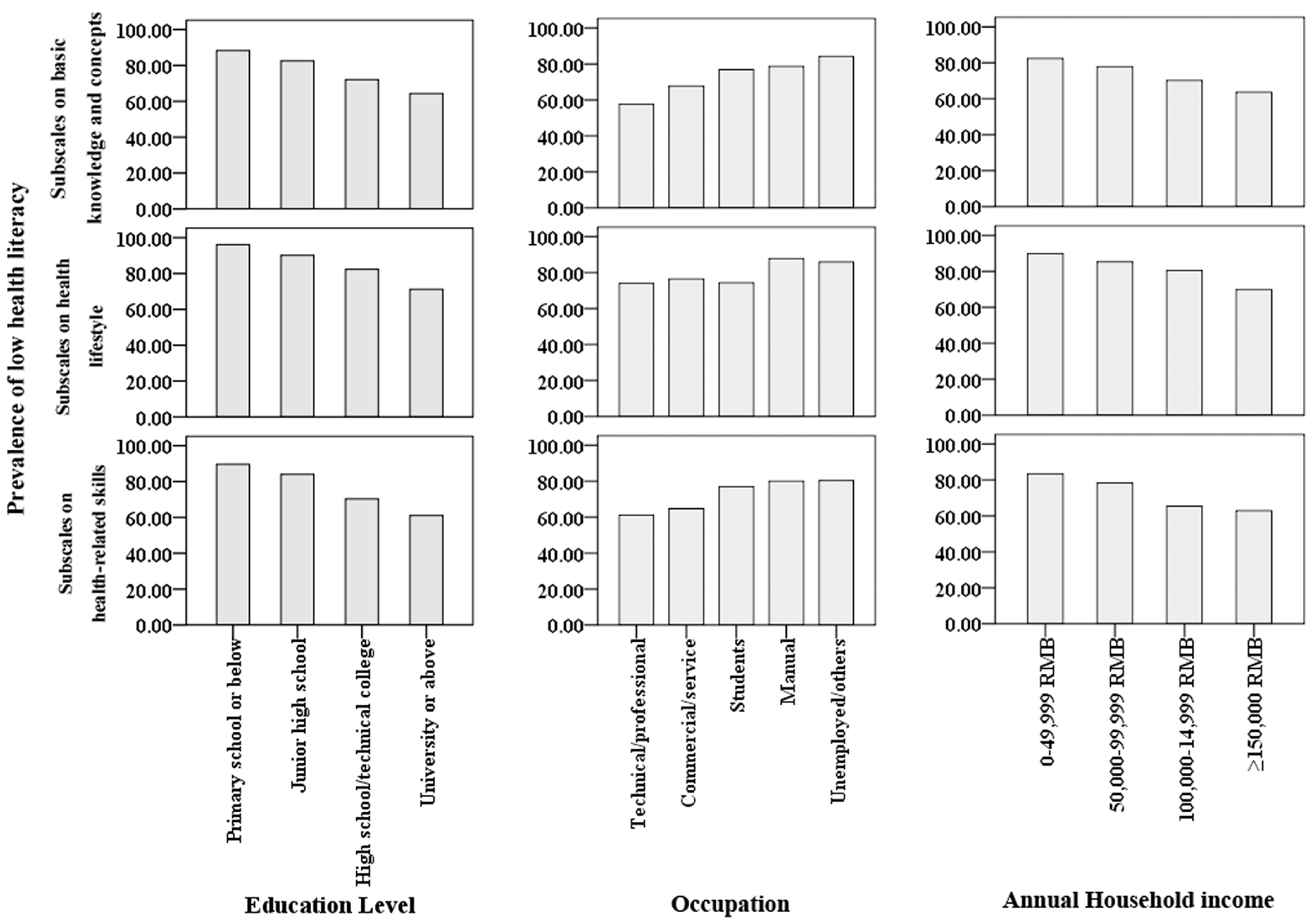
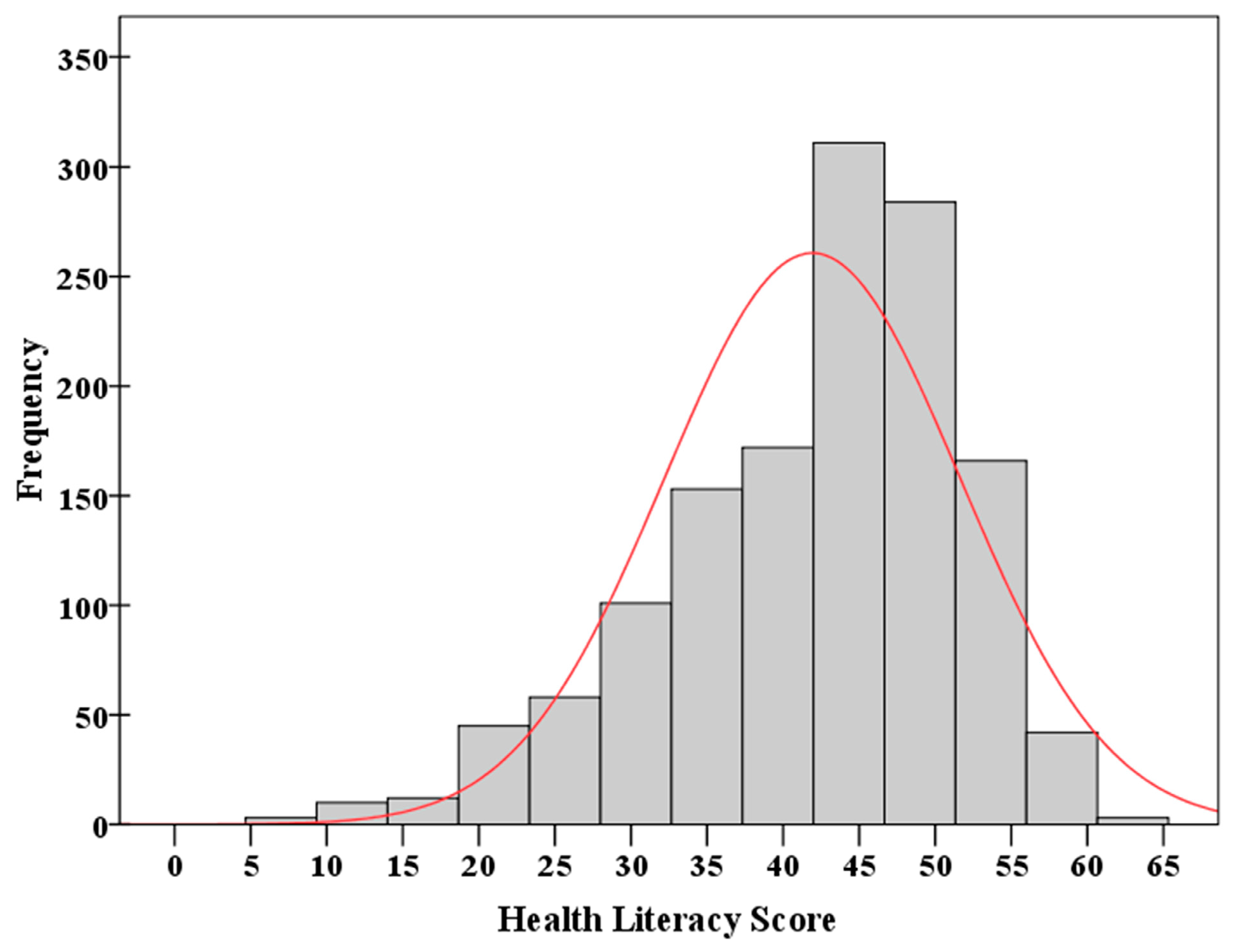
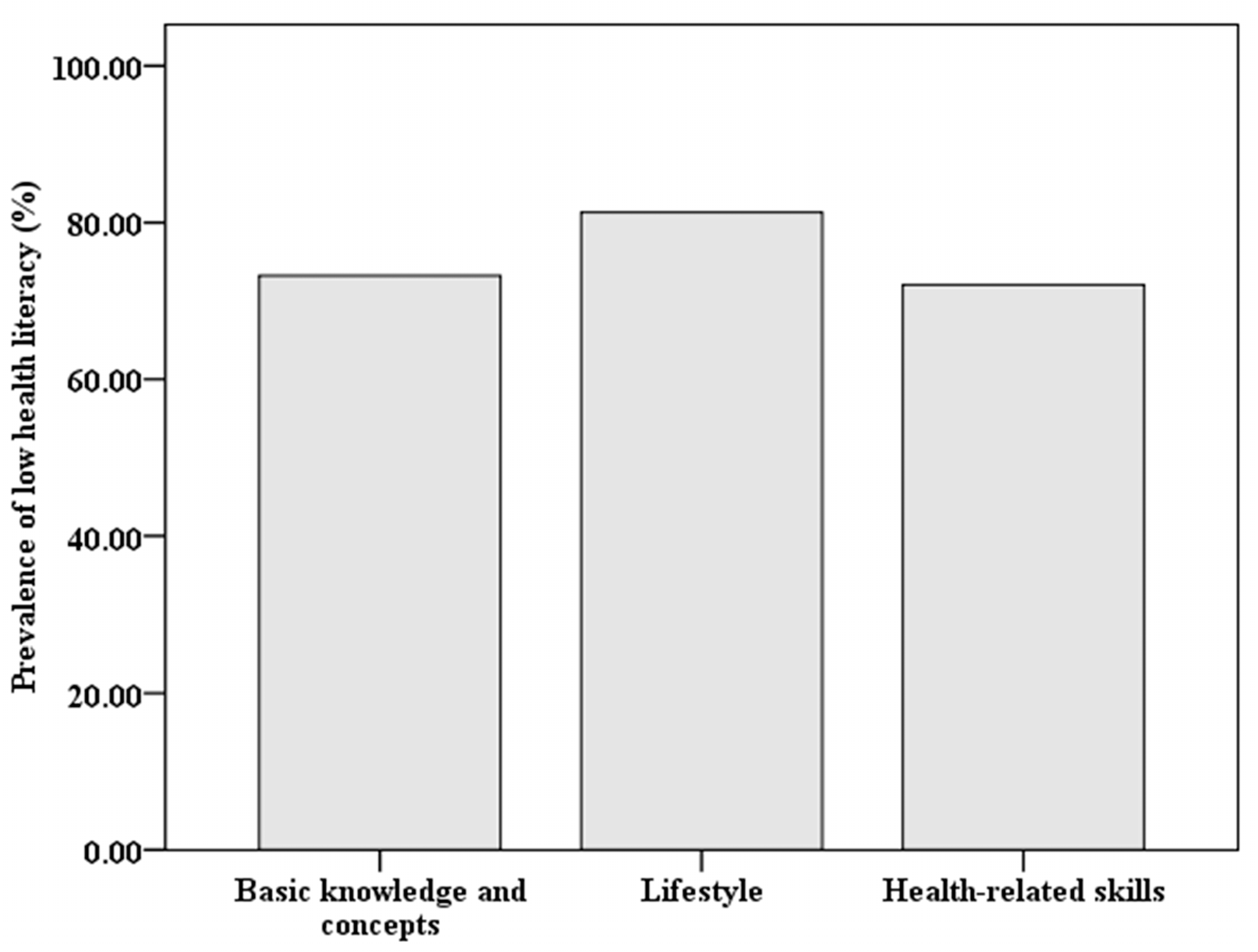
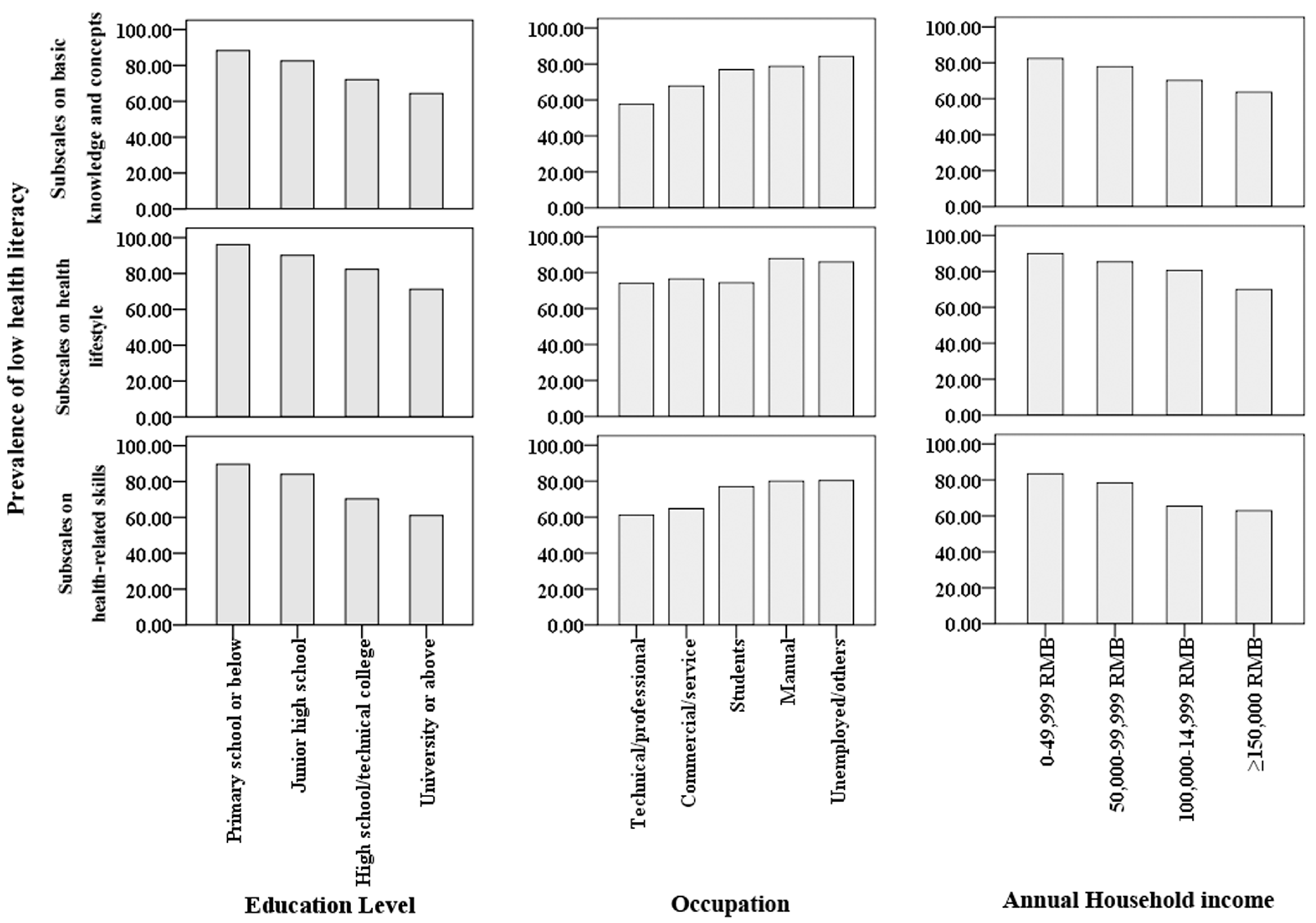
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Ratzan, S.C.; Parker, R.M. Introduction. In National Library of Medicine Current Bibliographies in Medicine: Health Literacy; Selden, C.R., Zorn, M., Ratzan, S.C., Parker, R.M., Eds.; National Institutes of Health, U.S. Department of Health and Human Services: Bethesda, MD, USA, 2000; Volume NLM, Pubulic No. CBM 2000-1. Available online: http://www.nlm.nih.gov/pubs/cbm/hliteracy.html (accessed on 1 September 2016).
- Institute of Medicine. Health Literacy: A Prescription to End Confusion; National Academies Press: Washington, DC, USA, 2004. [Google Scholar]
- World Health Organization (WHO). Commission on the Social Determinants of Health. Achieving Health Equity: From Root Causes to Fair Outcomes; WHO: Geneva, Switzerland, 2007. [Google Scholar]
- Gazmararian, J.; Curran, J.; Parker, R.; Bernhardt, J.M.; DeBuono, B.A. Public health literacy in America, an ethical imperative. Am. J. Prev. Med. 2005, 28, 317–322. [Google Scholar] [CrossRef] [PubMed]
- Fisher, W.J. The crucial link between literacy and health. Ann. Intern. Med. 2003, 139, 875–878. [Google Scholar]
- Weiss, B.D.; Blanchard, J.S.; McGee, D.L.; Hart, G.; Warren, B.; Burgoon, M.; Smith, K.J. Illiteracy among Medicaid recipients and its relationship to health care costs. J. Health Care Poor Underserved 1994, 5, 99–111. [Google Scholar] [CrossRef] [PubMed]
- Rudd, R.E.; Moeykens, B.A.; Colton, T.C. Health and Literacy: A Review of Medical and Public Health Literature. In Health and Literacy; Comings, J., Garners, B., Smith, C., Eds.; Jossey-Bass: New York, NY, USA, 1999. [Google Scholar]
- Lam, L.T.; Yang, L. Is low health literacy associated with overweight and obesity in adolescents: An epidemiology study in a 12–16 years old population, Nanning, China, 2012. Arch. Public Health 2014, 72, 11. [Google Scholar] [CrossRef] [PubMed]
- Williams, M.V.; Baker, D.W.; Parker, R.M.; Nurss, J.R. Relationship of Functional Health Literacy to Patients’ Knowledge of Their Chronic Disease: A Study of Patients with Hypertension and Diabetes. Arch. Intern. Med. 1998, 158, 166–172. [Google Scholar] [CrossRef] [PubMed]
- Paasche-Orlow, M.K.; Parker, R.M.; Gazmararian, J.A.; Nielsen-Bohlman, L.T.; Rudd, R.R. The Prevalence of Limited Health Literacy. J. Gen. Intern. Med. 2005, 20, 175–184. [Google Scholar] [CrossRef] [PubMed]
- Department for Education and Science. The Skills for Life Survey: A National Needs and Impact Survey of Literacy, Numeracy and ICT Skills; Department for Education and Skills: London, UK, 2003.
- Chinese Ministry of Health. Report on the First Chinese Residents Health Literacy Monitoring Program. Available online: http://www.lnjkjy.org.cn/upload/file/20140114/20140114132502_3906.doc (accessed on 20 September 2016).
- Li, X.H. Definition and promotion of “Chinese citizens’ health literacy: Basic knowledge and skill”. Chin. J. Health Educ. 2008, 24, 385–388. [Google Scholar]
- Chinese Ministry of Health. 66 Tips of Health: Chinese Resident Health Literacy Manual; People’s Medical Publishing House: Beijing, China, 2008. [Google Scholar]
- Nutbeam, D. The evolving concept of health literacy. Soc. Sci. Med. 2008, 67, 2072–2078. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.H. Introduction of 2012 Chinese residents health literacy monitoring program. Chin. J. Health Educ. 2014, 30, 563–565. [Google Scholar]
- Shen, M.; Hu, M.; Liu, S.; Chang, Y.; Sun, Z. Assessment of the Chinese Resident Health Literacy Scale in a population-based sample in South China. BMC Public Health 2015, 15, 637–647. [Google Scholar] [CrossRef] [PubMed]
- Communique of the National Bureau of Statistics of People’s Republic of China on Major Figures of the 2010 Population Census (No. 1). Available online: http://www.stats.gov.cn/english/newsandcomingevents/t20110428_402722244.htm (accessed on 20 September 2016).
- Wang, X.S.; Guo, H.J.; Wang, L.; Li, X.; Huang, M.; Liu, Z.; Liu, X.; Wang, K.; Alamian, A.; Anderson, J.L. Investigation of Residents’ Health Literacy Status and Its Risk Factors in Jiangsu Province of China. Asia Pac. J. Public Health 2015, 27, 2764–2772. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Wu, S.; Zhang, Y.; Yang, P.; MacIntyre, C.R.; Seale, H.; Wang, Q. Health literacy in Beijing: An assessment of adults’ knowledge and skills regarding communicable diseases. BMC Public Health 2015, 15, 799–807. [Google Scholar] [CrossRef] [PubMed]
- Shanghai Municipal Statistics Bureau. Shanghai Annual Statistics Report; Shanghai Municipal Government: Shanghai, China, 2016.
- Wu, E.; Chen, X.; Guan, Z.; Cao, C.; Rao, H.; Feng, B.; Chan, M.; Fu, S.; Lin, A.; Wei, L.; et al. A comparative study of patients’ knowledge about hepatitis C in the United States and in urban and rural China. Hepatol. Int. 2015, 9, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Beers, B.B.; McDonald, V.J.; Quistberg, D.A.; Ravenell, K.L.; Asch, D.A.; Shea, J.A. Disparities in health literacy between African American and non-African American primary care patients. J. Gen. Intern. Med. 2003, 18, 169. [Google Scholar]
- Gazmararian, J.A.; Baker, D.W.; Williams, M.V. Health literacy among medicare enrollees in a managed care organization. JAMA 1999, 281, 545–551. [Google Scholar] [CrossRef] [PubMed]
- Schillinger, D.; Grumbach, K.; Piettee, J. Association of health literacy with diabetes outcomes. JAMA 2002, 288, 475–482. [Google Scholar] [CrossRef] [PubMed]
- William, M.V.; Parker, R.M.; Baker, D.W. Inadequate functional health literacy among patients at two public hospitals. JAMA 1995, 274, 1677–1682. [Google Scholar] [CrossRef]
- Wong, D.F.K.; Xuesong, H.; Poon, A.; Lam, A.Y.K. Depression literacy among Chinese in Shanghai, China: A comparison with Chinese-speaking Austrilians in Melbourne and Chinese in Hong Kong. Soc. Psychiatry Psychiatr. Epidemiol. 2012, 47, 1235–1242. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Ning, N.; Hao, Y.; Sun, H.; Gao, L.; Jiao, M.; Wu, Q.; Quan, H. Health Literacy in Rural Areas of China: Hypertension Knowledge Survey. Int. J. Environ. Res. Public Health 2013, 10, 1125–1138. [Google Scholar] [CrossRef] [PubMed]
- Shanghai Ethnic and Religions Affairs Committee. Report on the Development of Minority Population in Shanghai. Available online: http://www.shmzw.gov.cn/gb/mzw/shmz/tjb/index.html (accessed on 31 May 2017).



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Risk Factor | OR (95% CI) | p Value | |
|---|---|---|---|
| Education level | |||
| Primary school or below (reference) | |||
| Junior high school | 0.560 (0.127, 2.461) | 0.443 | |
| High school/technical college | 0.190 (0.045, 0.806) | 0.024 | |
| University or above | 0.140 (0.033, 0.599) | 0.008 | |
| Occupation | |||
| Technical/professional (reference) | |||
| Commercial/service | 1.642 (0.995, 2.710) | 0.052 | |
| Students | 2.276 (0.834, 6.211) | 0.108 | |
| Manual | 2.413 (1.302, 4.470) | 0.005 | |
| Unemployed/others | 2.470 (1.237, 4.934) | 0.010 | |
| Annual household income | |||
| ¥0–¥49,999 (reference) | |||
| ¥50,000–¥99,999 | 0.681 (0.342, 1.355) | 0.273 | |
| ¥100,000–¥14,999 | 0.507 (0.255, 1.010) | 0.053 | |
| ≥¥150,000 | 0.432 (0.213, 0.874) | 0.020 |
| Characteristics | Number (%) a | Health Literacy Score | Prevalence of Low Health Literacy | |||
|---|---|---|---|---|---|---|
| Mean ± SD | p Value | Number (%) b | p Value | |||
| Gender | Male | 648 (47.6%) | 41.87 ± 9.75 | 0.876 | 547 (84.4%) | 0.944 |
| Female | 712 (52.4%) | 41.96 ± 9.68 | 602 (84.6%) | |||
| Age group | 15–35 | 353 (26.0%) | 44.07 ± 9.00 | <0.001 | 270 (76.5%) | <0.001 |
| 36–59 | 662 (48.7%) | 42.34 ± 9.06 | 566 (85.5%) | |||
| 60–69 | 345 (25.4%) | 38.91 ± 10.85 | 313 (90.7%) | |||
| Education level | Primary school or below | 77 (5.7%) | 35.39 ± 10.72 | <0.001 | 75 (97.4%) | <0.001 |
| Junior high school | 396 (29.1%) | 38.70 ± 9.66 | 376 (94.9%) | |||
| High school/technical college | 391 (28.8%) | 42.32 ± 9.16 | 330 (84.4%) | |||
| University or above | 496 (36.5%) | 45.19 ± 8.66 | 368 (74.2%) | |||
| Occupation c | Technical/professional | 85 (6.2%) | 45.57 ± 8.40 | <0.001 | 56 (65.9%) | <0.001 |
| Commercial/service | 598 (44.0%) | 43.61 ± 9.64 | 477 (79.8%) | |||
| Students | 39 (2.9%) | 44.36 ± 7.30 | 33 (84.6%) | |||
| Manual | 460 (33.8%) | 40.01 ± 9.38 | 423 (92.0%) | |||
| Unemployed/others | 178 (13.1%) | 38.92 ± 10.09 | 160 (89.9%) | |||
| Annual household income d | ¥0–¥49,999 | 187 (13.8%) | 38.30 ± 9.92 | <0.001 | 176 (94.1%) | <0.001 |
| ¥50,000–¥99,999 | 491 (36.1%) | 40.57 ± 9.51 | 436 (88.8%) | |||
| ¥100,000–¥14,999 | 396 (29.1%) | 43.18 ± 9.54 | 322 (81.3%) | |||
| ≥¥150,000 | 286 (21.0%) | 44.87 ± 9.01 | 215 (75.2%) | |||
| Prevalence of a non-communicable chronic disease | ||||||
| Yes | 383 (28.2%) | 40.32 ± 10.00 | <0.001 | 340 (88.8%) | 0.006 | |
| No | 977 (71.8) | 42.55 ± 9.53 | 809 (82.8%) | |||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, Y.; Wang, L.; Cai, Z.; Bao, L.; Ai, P.; Ai, Z. Prevalence and Risk Factors of Low Health Literacy: A Community-Based Study in Shanghai, China. Int. J. Environ. Res. Public Health 2017, 14, 628. https://doi.org/10.3390/ijerph14060628
Wu Y, Wang L, Cai Z, Bao L, Ai P, Ai Z. Prevalence and Risk Factors of Low Health Literacy: A Community-Based Study in Shanghai, China. International Journal of Environmental Research and Public Health. 2017; 14(6):628. https://doi.org/10.3390/ijerph14060628
Chicago/Turabian StyleWu, Ying, Lu Wang, Zhongyuan Cai, Luqi Bao, Pu Ai, and Zisheng Ai. 2017. "Prevalence and Risk Factors of Low Health Literacy: A Community-Based Study in Shanghai, China" International Journal of Environmental Research and Public Health 14, no. 6: 628. https://doi.org/10.3390/ijerph14060628
APA StyleWu, Y., Wang, L., Cai, Z., Bao, L., Ai, P., & Ai, Z. (2017). Prevalence and Risk Factors of Low Health Literacy: A Community-Based Study in Shanghai, China. International Journal of Environmental Research and Public Health, 14(6), 628. https://doi.org/10.3390/ijerph14060628