
Lithium in Drinking Water and Incidence of Suicide: A Nationwide Individual-Level Cohort Study with 22 Years of Follow-Up

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
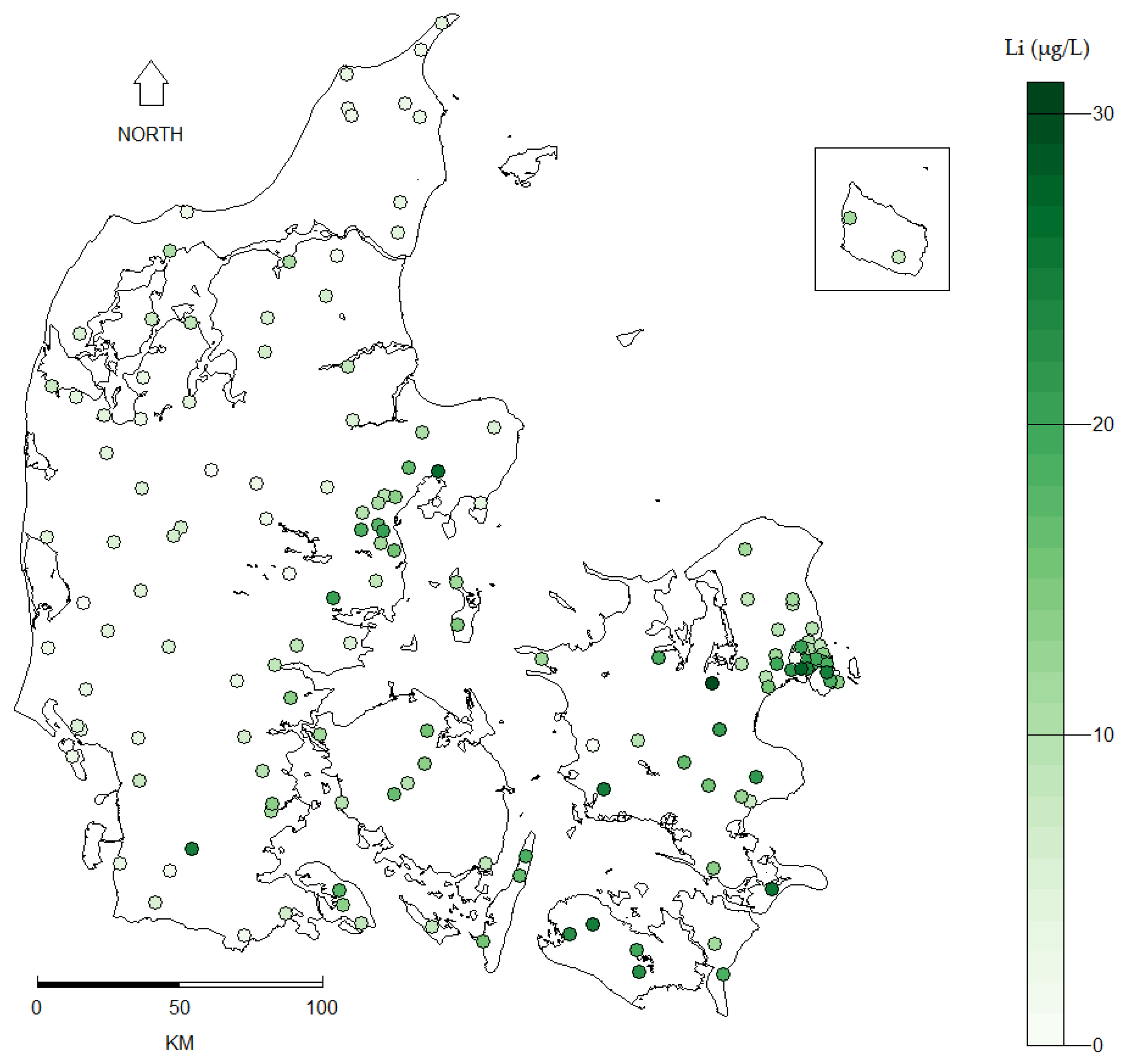
2.2. Lithium Measurements
2.2.1. Stability of Lithium Levels over Time
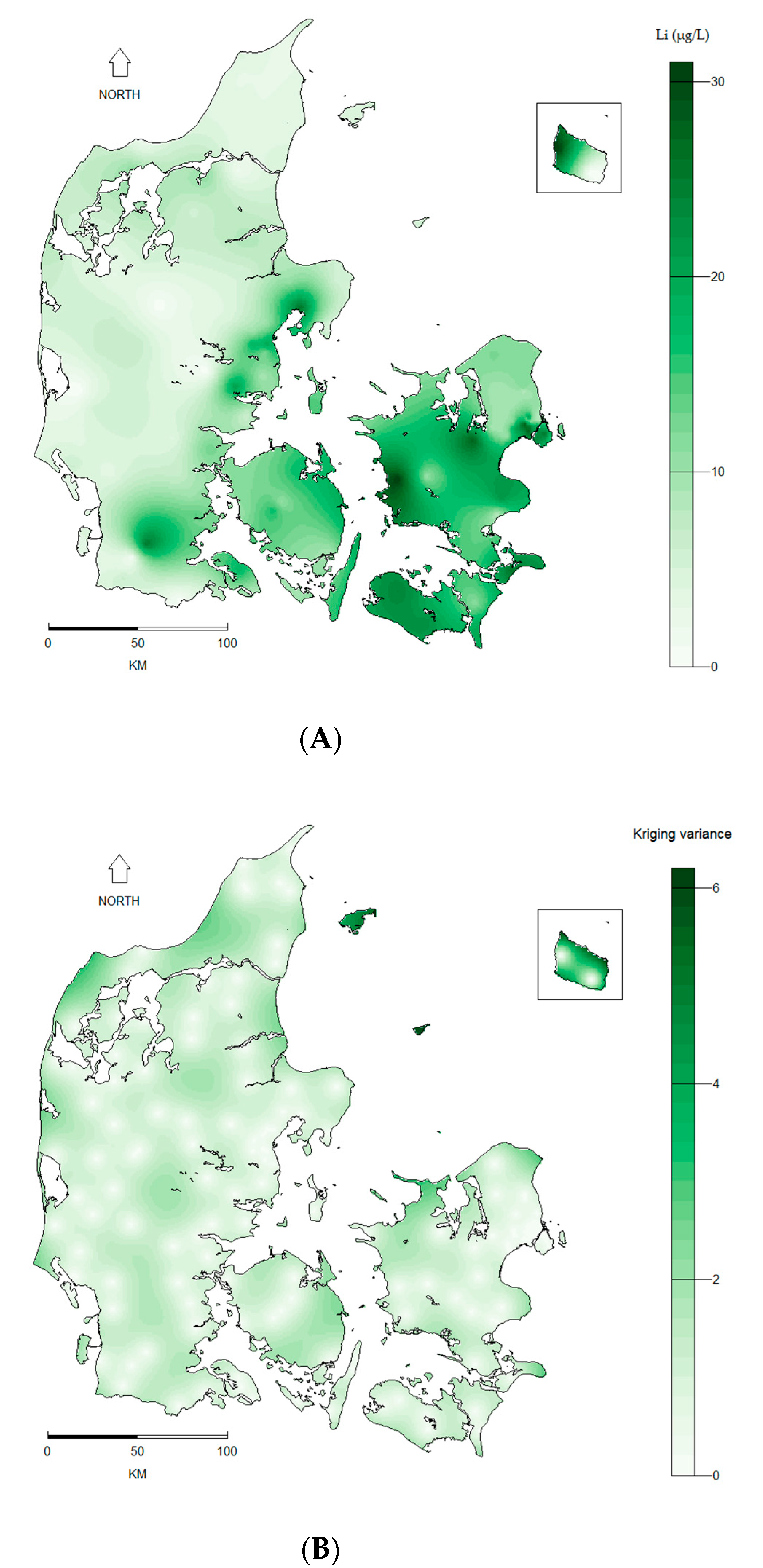
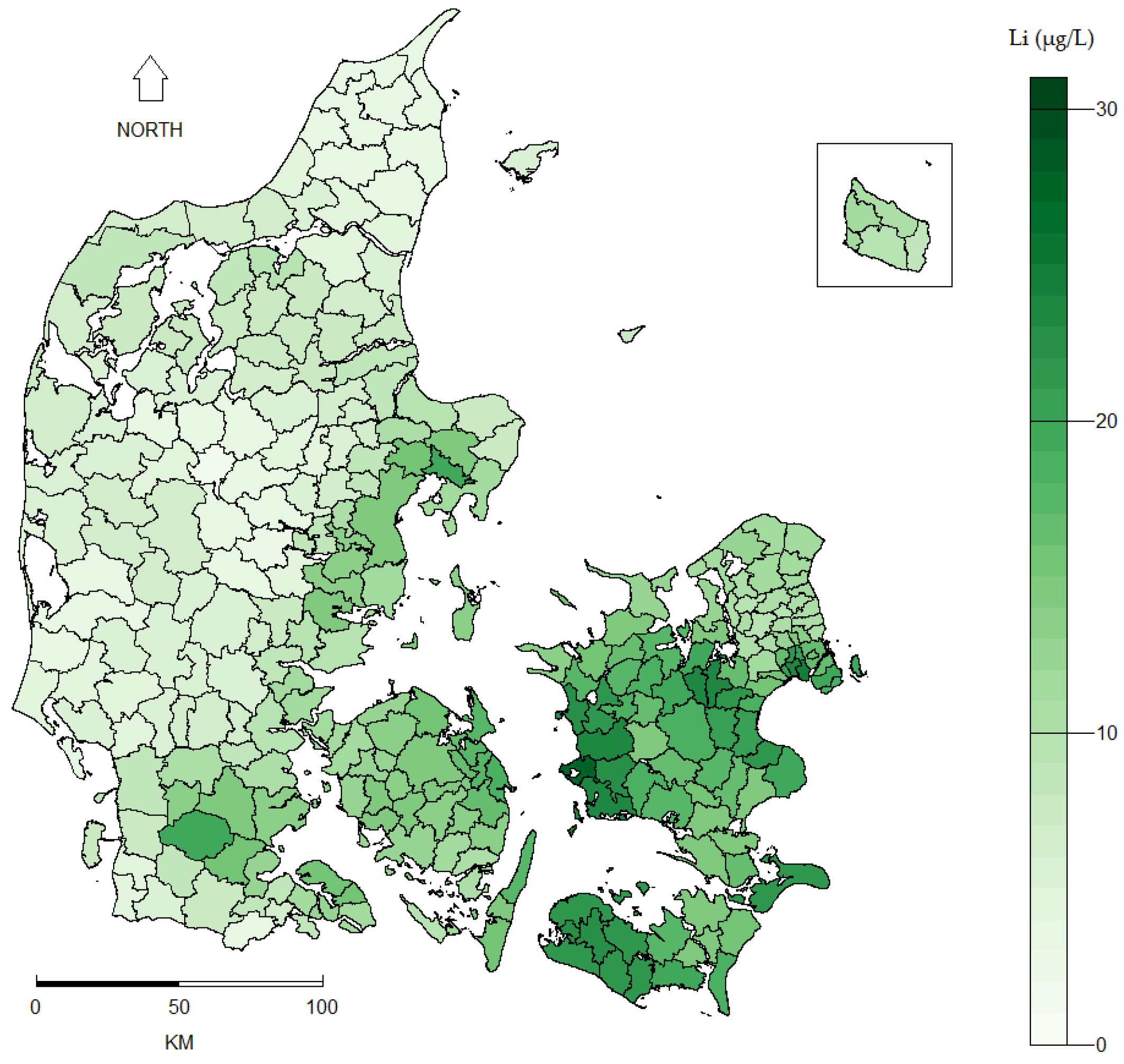
2.2.2. Lithium Exposure Assessment
2.3. Spatial Regression Analysis
2.4. Supplementary Analyses
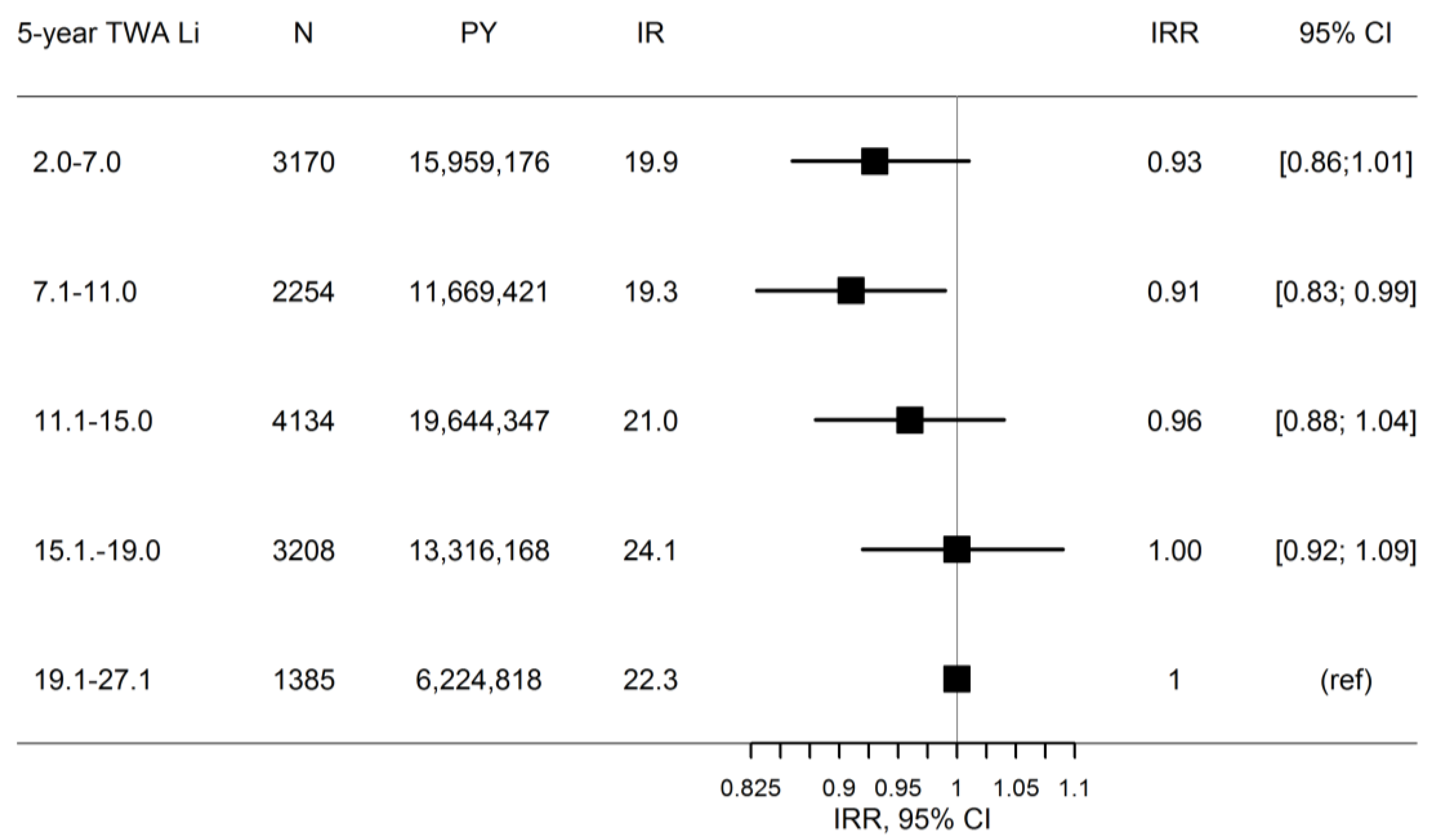
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- World Health Organization. Preventing Suicide: A Global Imperative; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Helweg-Larsen, K.; Kjøller, M.; Juel, K.; Sundaram, V.; Laursen, B.; Kruse, M.; Nørlev, J.; Davidsen, M. Selvmord I Danmark. Markant Fald I Selvmord, Men Stigende Antal Selvmordsforsøg. Hvorfor? Statens Institut for Folkesundhed: København, Denmark, 2006. [Google Scholar]
- StatBank Denmark. Statistics Denmark. Available online: http://www.statistikbanken.dk/UHELD10 (accessed on 25 May 2017).
- Hawton, K.; Van Heeringen, K. Suicide. Lancet 2009, 373, 1372–1381. [Google Scholar] [CrossRef]
- Lee, S.I.; Jung, H.Y. Psychosocial risk factors for suicide. Psychiatry Investig. 2006, 3, 15–22. [Google Scholar]
- Sugawara, N.; Yasui-Furukori, N.; Ishii, N.; Iwata, N.; Terao, T. Lithium in tap water and suicide mortality in Japan. Int. J. Environ. Res. Public Health 2013, 10, 6044–6048. [Google Scholar] [CrossRef] [PubMed]
- Bluml, V.; Regier, M.D.; Hlavin, G.; Rockett, I.R.; Konig, F.; Vyssoki, B.; Bschor, T.; Kapusta, N.D. Lithium in the public water supply and suicide mortality in Texas. J. Psychiatr. Res. 2013, 47, 407–411. [Google Scholar] [CrossRef] [PubMed]
- Schrauzer, G.N. Lithium: Occurrence, dietary intakes, nutritional essentiality. J. Am. Coll. Nutr. 2002, 21, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Baldessarini, R.J.; Tondo, L.; Davis, P.; Pompili, M.; Goodwin, F.K.; Hennen, J. Decreased risk of suicides and attempts during long-term lithium treatment: A meta-analytic review. Bipolar Disord. 2006, 8, 625–639. [Google Scholar] [CrossRef] [PubMed]
- Cipriani, A.; Hawton, K.; Stockton, S.; Geddes, J.R. Lithium in the prevention of suicide in mood disorders: Updated systematic review and meta-analysis. Br. Med. J. 2013, 346. [Google Scholar] [CrossRef] [PubMed]
- Grunze, H.; Vieta, E.; Goodwin, G.M.; Bowden, C.; Licht, R.W.; Moller, H.J.; Kasper, S. The World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for the biological treatment of bipolar disorders: Update 2012 on the long-term treatment of bipolar disorder. World J. Biol. Psychiatry Off. J. World Fed. Soc. Biol. Psychiatry 2013, 14, 154–219. [Google Scholar] [CrossRef] [PubMed]
- Reimann, C.; Birke, M. Geochemistry of European Bottled Water; Gebrüder Borntraeger Verlagsbuchhandlung: Stuttgart, Germany, 2010. [Google Scholar]
- Giotakos, O.; Nisianakis, P.; Tsouvelas, G.; Giakalou, V.V. Lithium in the public water supply and suicide mortality in Greece. Biol. Trace Elem. Res. 2013, 156, 376–379. [Google Scholar] [CrossRef] [PubMed]
- Helbich, M.; Leitner, M.; Kapusta, N.D. Geospatial examination of lithium in drinking water and suicide mortality. Int. J. Health Geogr. 2012, 11, 19. [Google Scholar] [CrossRef] [PubMed]
- Kabacs, N.; Memon, A.; Obinwa, T.; Stochl, J.; Perez, J. Lithium in drinking water and suicide rates across the East of England. Br. J. Psychiatry J. Ment. Sci. 2011, 198, 406–407. [Google Scholar] [CrossRef] [PubMed]
- Ohgami, H.; Terao, T.; Shiotsuki, I.; Ishii, N.; Iwata, N. Lithium levels in drinking water and risk of suicide. Br. J. Psychiatry J. Ment. Sci. 2009, 194, 464–465. [Google Scholar] [CrossRef] [PubMed]
- Pompili, M.; Vichi, M.; Dinelli, E.; Pycha, R.; Valera, P.; Albanese, S.; Lima, A.; De Vivo, B.; Cicchella, D.; Fiorillo, A.; et al. Relationships of local lithium concentrations in drinking water to regional suicide rates in Italy. World J. Biol. Psychiatry Off. J. World Fed. Soc. Biol. Psychiatry 2015, 16, 567–574. [Google Scholar] [CrossRef] [PubMed]
- Shiotsuki, I.; Terao, T.; Ishii, N.; Takeuchi, S.; Kuroda, Y.; Kohno, K.; Mizokami, Y.; Hatano, K.; Tanabe, S.; Kanehisa, M.; et al. Trace lithium is inversely associated with male suicide after adjustment of climatic factors. J. Affect. Disord. 2016, 189, 282–286. [Google Scholar] [CrossRef] [PubMed]
- Vita, A.; De Peri, L.; Sacchetti, E. Lithium in drinking water and suicide prevention: A review of the evidence. Int. Clin. Psychopharmacol. 2015, 30, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Rothman, K.J.; Greenland, S.; Lash, T.L. Modern Epidemiology; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2008; pp. 519–522. [Google Scholar]
- Voutchkova, D.; Schullehner, J.; Knudsen, N.; Jørgensen, L.; Ersbøll, A.; Kristiansen, S.; Hansen, B. Exposure to Selected Geogenic Trace Elements (I, Li, and Sr) from Drinking Water in Denmark. Geosciences 2015, 5, 45–66. [Google Scholar] [CrossRef]
- Pedersen, C.B. The Danish Civil Registration System. Scand. J. Public Health 2011, 39, 22–25. [Google Scholar] [CrossRef] [PubMed]
- Thygesen, L.C.; Ersbøll, A.K. Danish population-based registers for public health and health-related welfare research: Introduction to the supplement. Scand. J. Public Health 2011, 39, 8–10. [Google Scholar] [CrossRef] [PubMed]
- Helweg-Larsen, K. The Danish register of causes of death. Scand. J. Public Health 2011, 39, 26–29. [Google Scholar] [CrossRef] [PubMed]
- Petersson, F.; Baadsgaard, M.; Thygesen, L.C. Danish registers on personal labour market affiliation. Scand. J. Public Health 2011, 39, 95–98. [Google Scholar] [CrossRef] [PubMed]
- Voutchkova, D.D.; Ernstsen, V.; Hansen, B.; Sorensen, B.L.; Zhang, C.; Kristiansen, S.M. Assessment of spatial variation in drinking water iodine and its implications for dietary intake: A new conceptual model for Denmark. Sci. Total Environ. 2014, 493, 432–444. [Google Scholar] [CrossRef] [PubMed]
- Appelo, C.A.J.; Postma, D. Geochemistry, Groundwater and Pollution, 2nd ed.; A.A. Balkema Publishers: Leiden, The Netherlands, 2005. [Google Scholar]
- Pfeiffer, D.; Robinson, T.; Stevenson, M.; Stevens, K.B.; Rogers, D.J.; Clements, A.C. Spatial Analysis in Epidemiology; Oxford University Press: New York, NY, USA, 2008; pp. 73–80. [Google Scholar]
- Waller, L.A.; Gotway, C.A. Applied Spatial Statistics for Public Health Data; John Wiley & Sons: Hoboken, NJ, USA, 2004; Volume 368, pp. 301–312. [Google Scholar]
- Dupont, W.D. Statistical Modeling for Biomedical Researchers: A Simple Introduction to the Analysis of Complex Data; Cambridge University Press: Cambridge, UK, 2009. [Google Scholar]
- Gräler, B.; Pebesma, E.; Heuvelink, G. Spatio-temporal interpolation using gstat. R J. 2016, 8, 204–218. [Google Scholar]
- Pebesma, E.J. Multivariable geostatistics in S: The gstat package. Comput. Geosci. 2004, 30, 683–691. [Google Scholar] [CrossRef]
- Indenrigs- og Sundhedsministeriet. Kommunalreformen: Kort Fortalt; Indenrigs- og Sundhedsministeriet: Copenhagen, Denmark, 2005. [Google Scholar]
- Pebesma, E.J.; Bivand, R.S. Classes and methods for spatial data in R. R News 2005, 5, 9–13. [Google Scholar]
- Bivand, R.S.; Pebesma, E.; Gómez-Rubio, V. Applied Spatial Data Analysis with R, 2nd ed.; Springer: Berlin, Germany, 2013. [Google Scholar]
- Kawamoto, M.; Echt, A.; Reh, C. Health Hazard Evaluation Report; Report No. HETA 96-0016-2777; CDC NIOSH: Joplin, MO, USA, 1999.
- Lee, D. CARBayes: An R package for Bayesian spatial modeling with conditional autoregressive priors. J. Stat. Softw. 2013, 55, 1–24. [Google Scholar] [CrossRef]
- Lee, D. A comparison of conditional autoregressive models used in Bayesian disease mapping. Spat. Spatio-Temporal Epidemiol. 2011, 2, 79–89. [Google Scholar] [CrossRef] [PubMed]
- Rue, H.; Martino, S.; Chopin, N. Approximate Bayesian inference for latent Gaussian models by using integrated nested Laplace approximations. J. R. Stat. Soc Ser. B (Stat. Methodol.) 2009, 71, 319–392. [Google Scholar] [CrossRef]
- Martins, T.G.; Simpson, D.; Lindgren, F.; Rue, H. Bayesian computing with INLA: New features. Comput. Stat. Data Anal. 2013, 67, 68–83. [Google Scholar] [CrossRef]
- Borgan, O.; Goldstein, L.; Langholz, B. Methods for the analysis of sampled cohort data in the cox proportional hazards model. Ann. Stat. 1995, 23, 1749–1778. [Google Scholar] [CrossRef]
- Thygesen, L.C.; Ersboll, A.K. When the entire population is the sample: Strengths and limitations in register-based epidemiology. Eur. J. Epidemiol. 2014, 29, 551–558. [Google Scholar] [CrossRef] [PubMed]
- Rygaard, M.; Arvin, E.; Binning, P.J. The valuation of water quality: Effects of mixing different drinking water qualities. Water Res. 2009, 43, 1207–1218. [Google Scholar] [CrossRef] [PubMed]
- Schullehner, J.; Hansen, B. Nitrate exposure from drinking water in Denmark over the last 35 years. Environ. Res. Lett. 2014, 9, 095001. [Google Scholar] [CrossRef]
- Schullehner, J.; Jensen, N.L.; Thygesen, M.; Hansen, B.; Sigsgaard, T. Drinking water nitrate estimation at household-level in Danish population-based long-term epidemiologic studies. J. Geochem. Explor. 2017. [Google Scholar] [CrossRef]
- Gotway, C.A.; Wolfinger, R.D. Spatial prediction of counts and rates. Stat. Med. 2003, 22, 1415–1432. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, B.L.; Møller, R.R. Evaluation of total groundwater abstraction from public waterworks in Denmark using principal component analysis. Geol. Surv. Den. Greenl. Bull. 2013, 28, 37–40. [Google Scholar]
- Helbich, M.; Leitner, M.; Kapusta, N.D. Lithium in drinking water and suicide mortality: Interplay with lithium prescriptions. Br. J. Psychiatry J. Ment. Sci. 2015, 207, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Kessing, L.V.; Sondergard, L.; Kvist, K.; Andersen, P.K. Suicide risk in patients treated with lithium. Arch. Gen. Psychiatry 2005, 62, 860–866. [Google Scholar] [CrossRef] [PubMed]
- Sondergard, L.; Lopez, A.G.; Andersen, P.K.; Kessing, L.V. Mood-stabilizing pharmacological treatment in bipolar disorders and risk of suicide. Bipolar Disord. 2008, 10, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Kovacsics, C.E.; Gottesman, I.; Gould, T.D. Lithium’s antisuicidal efficacy: Elucidation of neurobiological targets using endophenotype strategies. Ann. Rev. Pharmacol. Toxicol. 2009, 49, 175–198. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Covariate | Variance Estimate (σ2) | Standard Error (SE) | % of Total Variance |
|---|---|---|---|
| Borehole | 0.62 | 0.038 | 74.7% |
| Sampling-depth within borehole | 0.14 | 0.011 | 16.9% |
| Residual a | 0.07 | 0.002 | 8.4% |
| Total | 0.83 |
| Variable | Category | N (%) | Five-Year Time-Weighted Average Lithium Exposure Level (μg/L) N (Row %) | ||||
|---|---|---|---|---|---|---|---|
| 2.0 to 7.0 | 7.1 to 11.0 | 11.1 to 15.0 | 15.1 to 19.0 | 19.1 to 27.1 | |||
| Overall | - | 3,740,113 | 870,515 | 635,331 | 1,099,608 | 796,428 | 338,231 |
| Gender | Female | 1,925,833 (51.5%) | 441,681 (22.9%) | 325,554 (16.9%) | 565,959 (29.4%) | 419,036 (21.8%) | 173,603 (9.0%) |
| Male | 1,814,280 (48.5%) | 428,834 (23.6%) | 309,777 (17.1%) | 533,649 (29.4%) | 377,392 (20.8%) | 164,628 (9.1%) | |
| Age (years) | 21 to 29 | 680,857 (18.2%) | 148,436 (21.8%) | 106,798 (15.7%) | 214,690 (31.5%) | 158,474 (23.3%) | 52,459 (7.7%) |
| 30 to 39 | 715,654 (19.1%) | 168,975 (23.6%) | 117,535 (16.4%) | 214,604 (30.0%) | 152,048 (21.3%) | 62,492 (8.7%) | |
| 40 to 49 | 762,730 (20.4%) | 178,197 (23.4%) | 134,614 (17.7%) | 226,273 (29.7%) | 150,552 (19.7%) | 73,094 (9.6%) | |
| 50 to 59 | 538,850 (14.4%) | 128,434 (23.8%) | 95,146 (17.7%) | 158,237 (29.4%) | 102,869 (19.1%) | 54,164 (10.1%) | |
| 60 to 69 | 480,608 (12.9%) | 114,943 (23.9%) | 83,822 (17.4%) | 135,738 (28.2%) | 97,048 (20.2%) | 49,057 (10.2%) | |
| 70 to 79 | 369,255 (9.9%) | 86,757 (23.5%) | 64,085 (17.4%) | 99,956 (27.1%) | 85,957 (23.3%) | 32,500 (8.8%) | |
| ≥80 | 192,159 (5.1%) | 44,773 (23.3%) | 33,331 (17.4%) | 50,110 (26.1%) | 49,480 (25.8%) | 14,465 (7.5%) | |
| Employment | Employed | 2,509,874 (67.1%) | 592,316 (23.6%) | 433,552 (17.3%) | 746,324 (29.7%) | 507,688 (20.2%) | 229,994 (9.2%) |
| Unemployed | 232,701 (6.2%) | 49,327 (21.2%) | 36,262 (15.6%) | 70,786 (30.4%) | 53,781 (23.1%) | 22.545 (9.7%) | |
| Outside labor force | 997,538 (26.7%) | 228,872 (22.9%) | 165,517 (16.6%) | 282,498 (28.3%) | 234,959 (23.6%) | 85,692 (8.6%) | |
| Civil status | Cohabiting | 2,524,134 (67.5%) | 626,256 (24.8%) | 448,595 (17.8%) | 743,470 (29.5%) | 468,507 (18.6%) | 237,306 (9.4%) |
| Living alone | 1,215,979 (32.5%) | 224,259 (20.1%) | 186,736 (15.4%) | 356,138 (29.3%) | 327,921 (27.0%) | 100,925 (8.3%) | |
| Ethnicity | Danish origin | 3,620,674 (96.8%) | 857.037 (23.7%) | 618,360 (17.1%) | 1,063,430 (29.4%) | 754,484 (20.8%) | 327,363 (9.0%) |
| Immigrant/descendant | 119,439 (3.2%) | 13,478 (11.3%) | 16,971 (14.2%) | 36,178 (30.3%) | 41,944 (35.1%) | 10,868 (9.1%) | |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Knudsen, N.N.; Schullehner, J.; Hansen, B.; Jørgensen, L.F.; Kristiansen, S.M.; Voutchkova, D.D.; Gerds, T.A.; Andersen, P.K.; Bihrmann, K.; Grønbæk, M.; et al. Lithium in Drinking Water and Incidence of Suicide: A Nationwide Individual-Level Cohort Study with 22 Years of Follow-Up. Int. J. Environ. Res. Public Health 2017, 14, 627. https://doi.org/10.3390/ijerph14060627
Knudsen NN, Schullehner J, Hansen B, Jørgensen LF, Kristiansen SM, Voutchkova DD, Gerds TA, Andersen PK, Bihrmann K, Grønbæk M, et al. Lithium in Drinking Water and Incidence of Suicide: A Nationwide Individual-Level Cohort Study with 22 Years of Follow-Up. International Journal of Environmental Research and Public Health. 2017; 14(6):627. https://doi.org/10.3390/ijerph14060627
Chicago/Turabian StyleKnudsen, Nikoline N., Jörg Schullehner, Birgitte Hansen, Lisbeth F. Jørgensen, Søren M. Kristiansen, Denitza D. Voutchkova, Thomas A. Gerds, Per K. Andersen, Kristine Bihrmann, Morten Grønbæk, and et al. 2017. "Lithium in Drinking Water and Incidence of Suicide: A Nationwide Individual-Level Cohort Study with 22 Years of Follow-Up" International Journal of Environmental Research and Public Health 14, no. 6: 627. https://doi.org/10.3390/ijerph14060627
APA StyleKnudsen, N. N., Schullehner, J., Hansen, B., Jørgensen, L. F., Kristiansen, S. M., Voutchkova, D. D., Gerds, T. A., Andersen, P. K., Bihrmann, K., Grønbæk, M., Kessing, L. V., & Ersbøll, A. K. (2017). Lithium in Drinking Water and Incidence of Suicide: A Nationwide Individual-Level Cohort Study with 22 Years of Follow-Up. International Journal of Environmental Research and Public Health, 14(6), 627. https://doi.org/10.3390/ijerph14060627