
Hydration, Fluid Intake, and Related Urine Biomarkers among Male College Students in Cangzhou, China: A Cross-Sectional Study—Applications for Assessing Fluid Intake and Adequate Water Intake

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Ethics
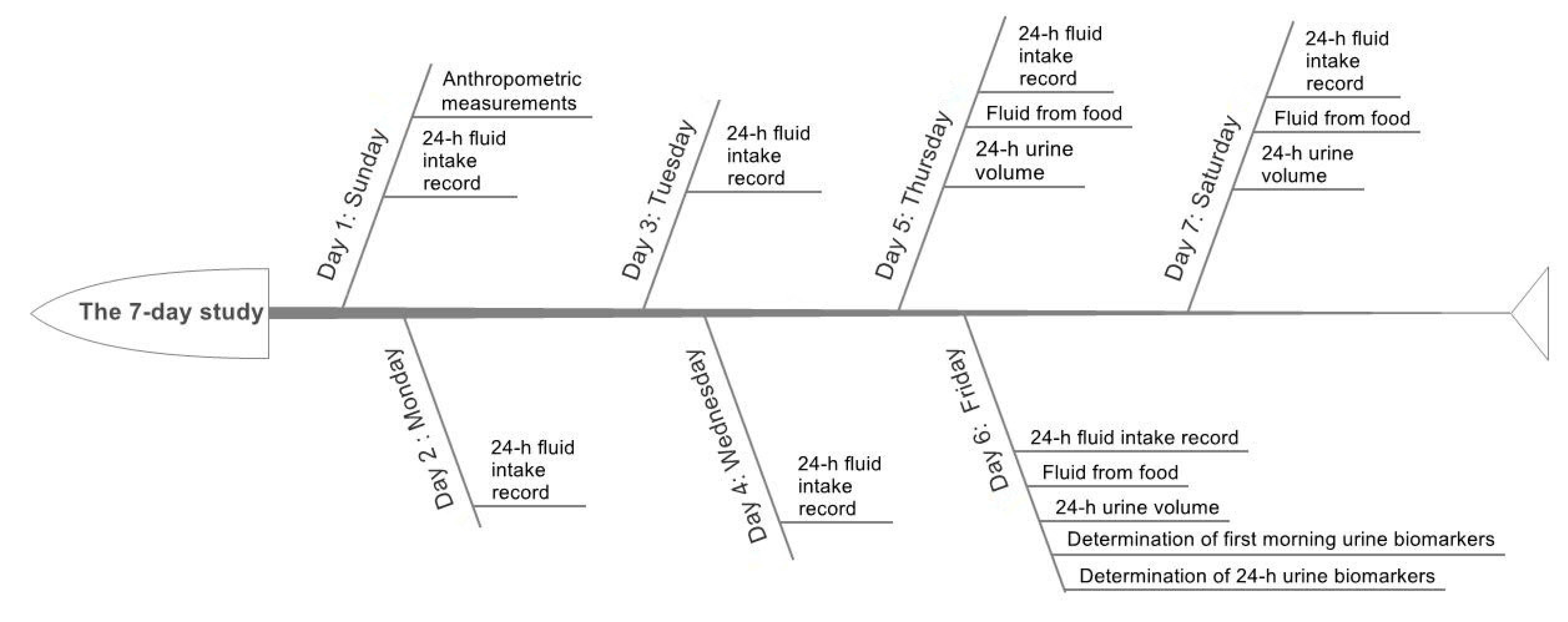
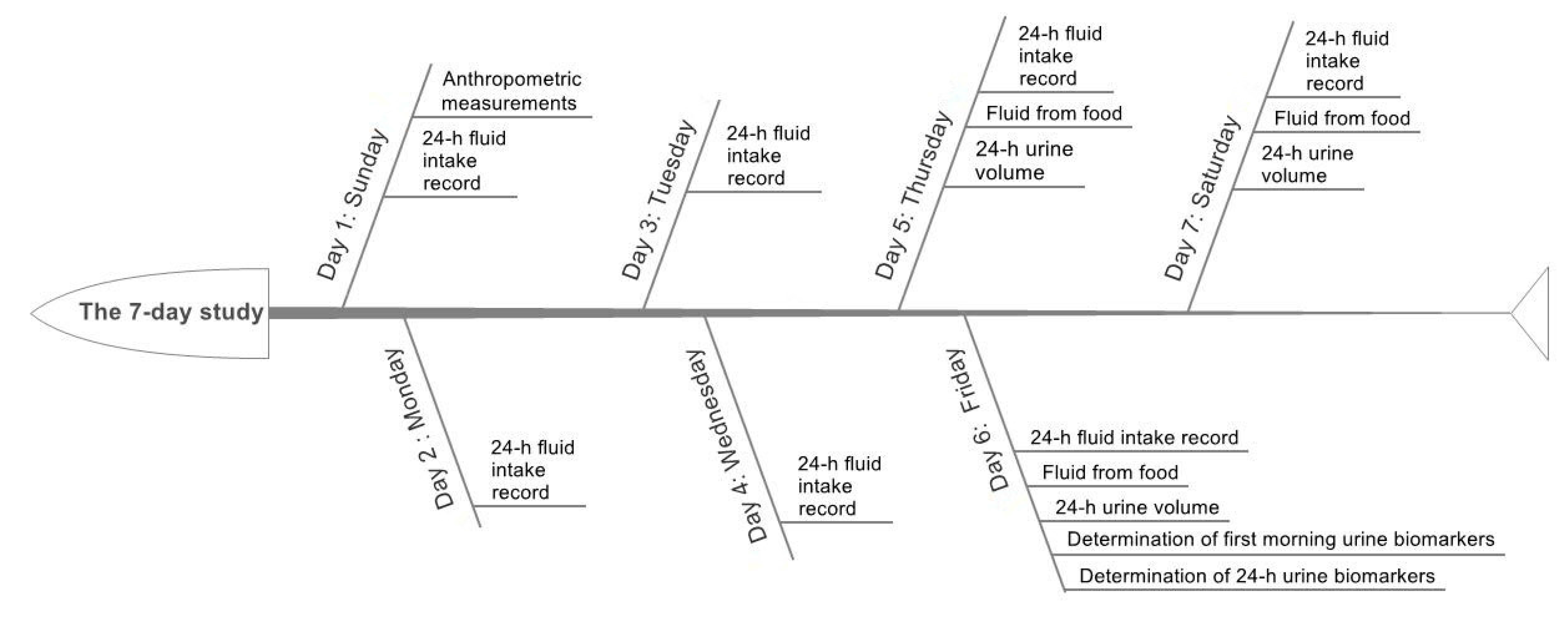
2.3. Study Design and Procedure
2.4. Anthropometric Measurements
2.5. Assessment of Fluid Intake
2.6. Assessment of Urine Biomarkers
2.7. Temperature and Humidity of the Environment
2.8. Statistical Analyses
3. Results
3.1. Characteristics of the Subjects and Environment
3.2. Temperature and Humidity
3.3. Assessment of Fluid Intake
3.4. Assessment of Urine Biomarkers
3.5. Association between Fluid Intake and 24-h Urine Biomarkers
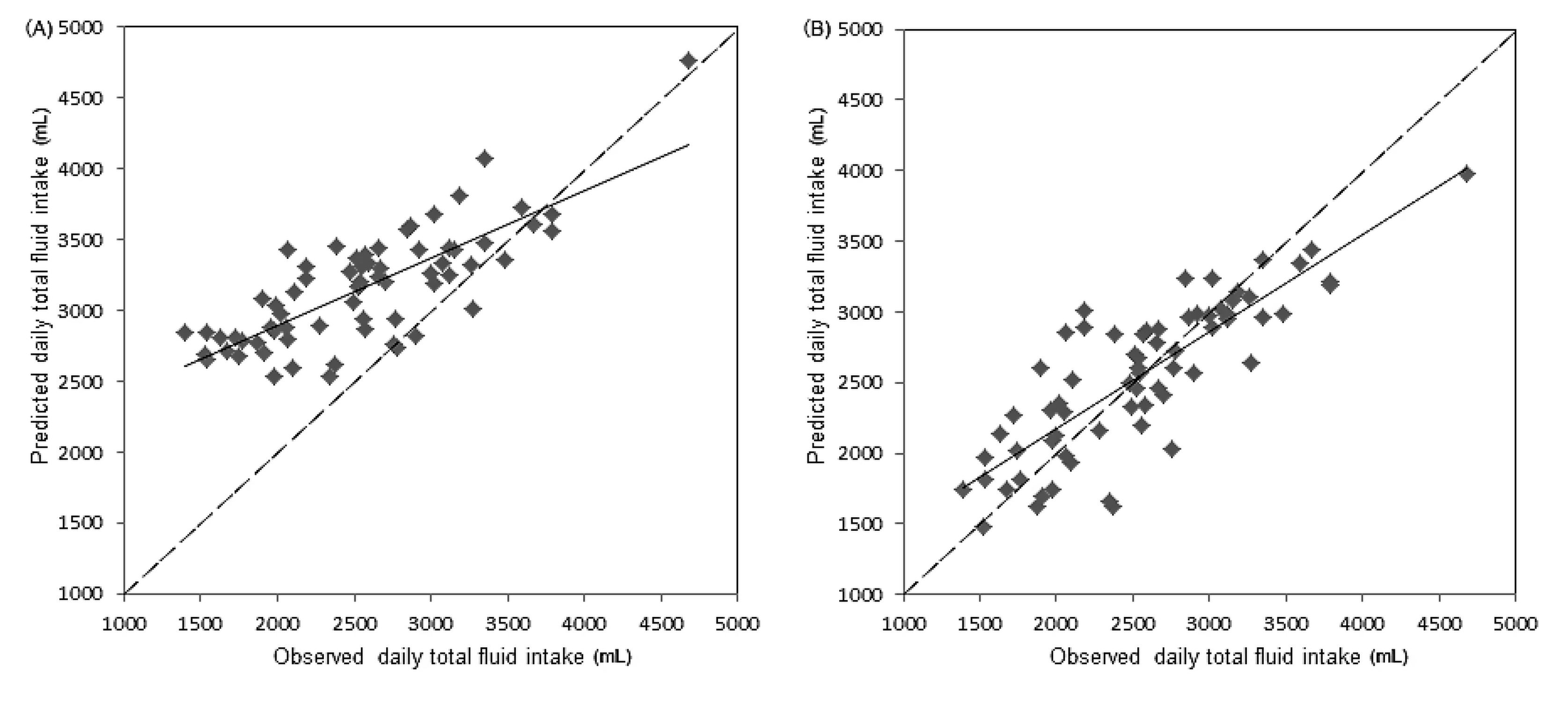
3.6. Partial Least Squares Model of the Relationship between Daily Total Fluid Intake and 24-h Urine Biomarkers
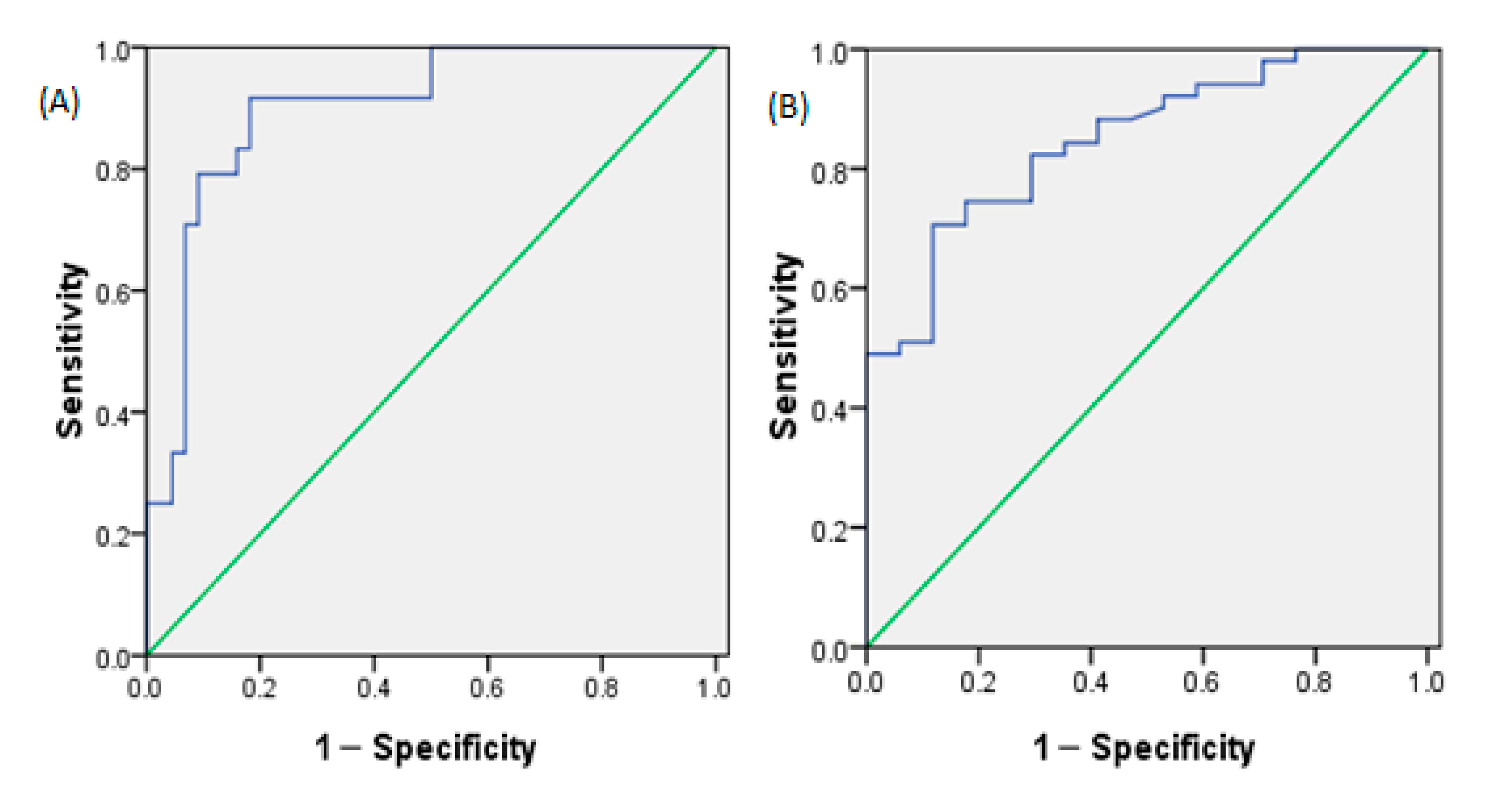
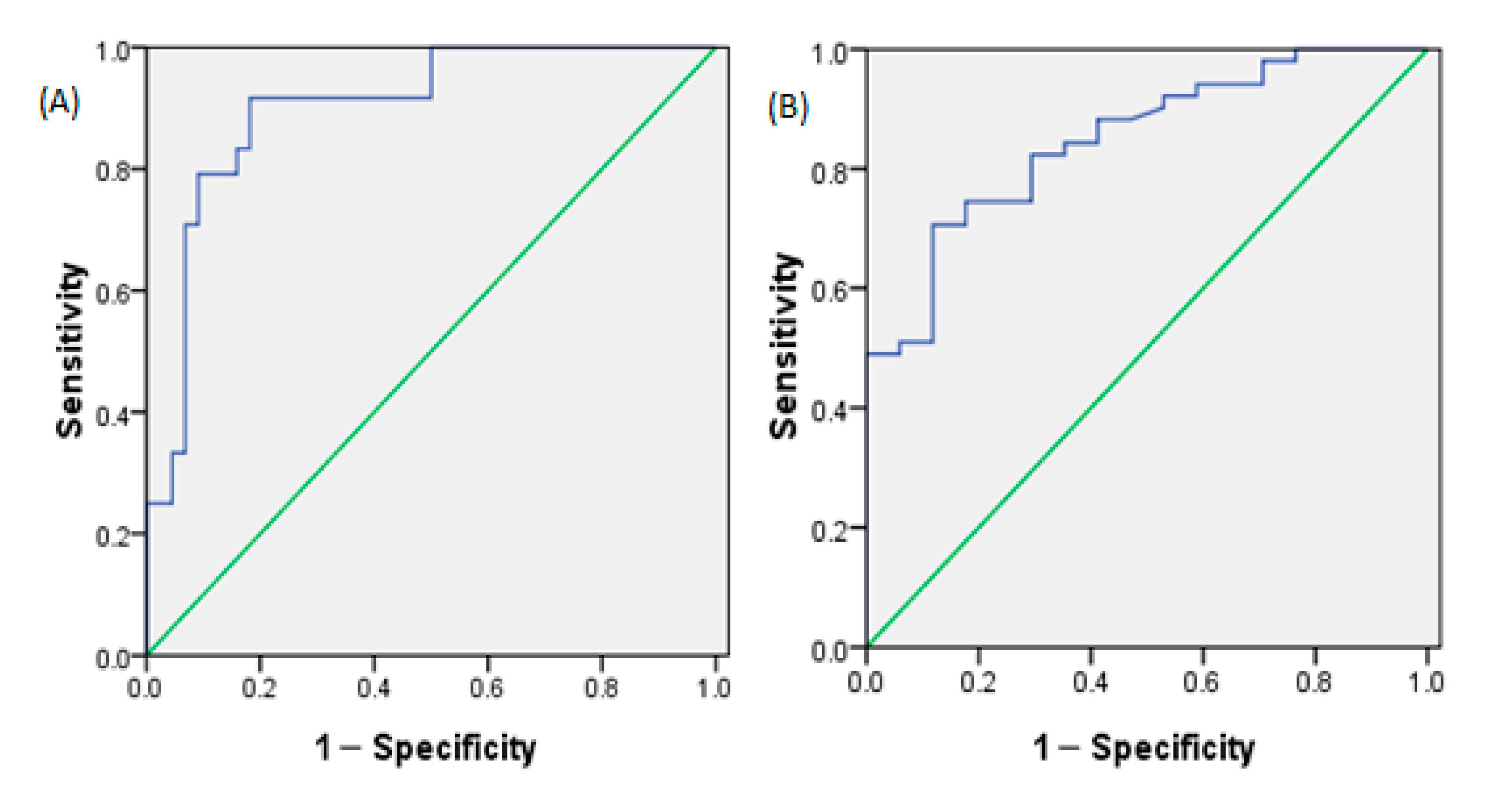
3.7. Determination of the Daily Total Fluid Intake for Assessing Optimal Hydration and Assessing Hypohydration
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- European Food Safety Authority. Scientific Opinion on Dietary Reference Values for Water. EFSA J. 2010, 8, 1459. [Google Scholar]
- Benefer, M.D.; Corfe, B.M.; Russell, J.M.; Short, R.; Barker, M.E. Water intake and post-exercise cognitive performance: An observational study of long-distance walkers and runners. Eur. J. Nutr. 2013, 52, 617–624. [Google Scholar] [CrossRef] [PubMed]
- D’Anci, K.E.; Vibhakar, A.; Kanter, J.H.; Mahoney, C.R.; Taylor, H.A. Voluntary dehydration and cognitive performance in trained college athletes. Percept. Motor Skills 2009, 109, 251–269. [Google Scholar] [CrossRef] [PubMed]
- Edmonds, C.J.; Crombie, R.; Ballieux, H.; Gardner, M.R.; Dawkins, L. Water consumption, not expectancies about water consumption, affects cognitive performance in adults. Appetite 2013, 60, 148–153. [Google Scholar] [CrossRef] [PubMed]
- Arnaoutis, G.; Kavouras, S.A.; Christaki, I.; Sidossis, L.S. Water ingestion improves performance compared with mouth rinse in dehydrated subjects. Med. Sci. Sports Exerc. 2012, 44, 175–179. [Google Scholar] [CrossRef] [PubMed]
- Castellani, J.W.; Muza, S.R.; Cheuvront, S.N.; Sils, I.V.; Fulco, C.S.; Kenefick, R.W.; Beidleman, B.A.; Sawka, M.N. Effect of hypohydration and altitude exposure on aerobic exercise performance and acute mountain sickness. J. Appl. Physiol. 2010, 109, 1792–1800. [Google Scholar] [CrossRef] [PubMed]
- Dai, M.; Zhao, A.; Liu, A.; You, L.; Wang, P. Dietary factors and risk of kidney stone: A case-control study in southern China. J. Renal Nutr. 2012, 23, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, M.D.; Kahn, A.J.; Reiner, A.P.; Tseng, T.Y.; Shikany, J.M.; Wallace, R.B.; Chi, T.; Wactawski-Wende, J.; Jackson, R.D.; O’Sullivan, M.J. Impact of nutritional factors on incident kidney stone formation: A report from the WHI OS. J. Urol. 2012, 187, 1645–1649. [Google Scholar] [CrossRef] [PubMed]
- Alaya, A.; Sakly, R.; Nouri, A.; Najjar, M.F.; Belgith, M.; Jouini, R. Idiopathic urolithiasis in Tunisian children: A report of 134 cases. Saudi J. Kidney Dis. Transplant. 2013, 24, 1055–1061. [Google Scholar] [CrossRef]
- Strippoli, G.F.; Craig, J.C.; Rochtchina, E.; Flood, V.M.; Wang, J.J.; Mitchell, P. Fluid and nutrient intake and risk of chronic kidney disease. Nephrology 2011, 16, 326–334. [Google Scholar] [CrossRef] [PubMed]
- Momeni, M.; Gharedaghi, Z.; Amin, M.M.; Poursafa, P.; Mansourian, M. Does water hardness have preventive effect on cardiovascular disease? Int. J. Prev. Med. 2014, 5, 159–163. [Google Scholar] [PubMed]
- Knezović, N.J.; Memić, M.; Mabić, M.; Huremović, J.; Mikulić, I. Correlation between water hardness and cardiovascular diseases in Mostar city, Bosnia and Herzegovina. J. Water Health 2014, 12, 817–823. [Google Scholar] [CrossRef] [PubMed]
- Catling, L.A.; Abubakar, I.; Lake, I.R.; Swift, L.; Hunter, P.R. A systematic review of analytical observational studies investigating the association between cardiovascular disease and drinking water hardness. J. Water Health 2008, 6, 433–442. [Google Scholar] [CrossRef] [PubMed]
- Cheuvront, S.N.; Fraser, C.G.; Kenefick, R.W.; Ely, B.R.; Sawka, M.N. Reference change values for monitoring dehydration. Clin. Chem. Lab. Med. 2011, 49, 1033–1037. [Google Scholar] [CrossRef] [PubMed]
- Munoz, C.X.; Swokla, B.; Bellego, L.L. Hydration biomarkers and dietary fluid consumption of women. J. Am. Acad. Nutr. Diet. 2012, 112, 1056–1061. [Google Scholar]
- Perrier, E.; Rondeau, P.; Poupin, M.; Le, B.L.; Armstrong, L.E.; Lang, F.; Stookey, J.; Tack, I.; Vergne, S.; Klein, A. Relation between urinary hydration biomarkers and total fluid intake in healthy adults. Eur. J. Clin. Nutr. 2013, 67, 939–943. [Google Scholar] [CrossRef] [PubMed]
- Erica, P.; Sébastien, V.; Alexis, K.; Marie, P.; Pascale, R.; Le, B.L.; Armstrong, L.E.; Lang, F.; Jodi, S.; Ivan, T. Hydration biomarkers in free-living adults with different levels of habitual fluid consumption. Br. J. Nutr. 2013, 109, 1678–1687. [Google Scholar]
- Perrier, E.; Demazières, A.; Girard, N.; Pross, N.; Osbild, D.; Metzger, D.; Guelinckx, I.; Klein, A. Circadian variation and responsiveness of hydration biomarkers to changes in daily water intake. Eur. J. Appl. Physiol. 2013, 113, 2143–2151. [Google Scholar] [CrossRef] [PubMed]
- Mckenzie, A.L.; Perrier, E.T.; Guelinckx, I.; Kavouras, S.A.; Aerni, G.; Lee, E.C.; Volek, J.S.; Maresh, C.M.; Armstrong, L.E. Relationships between hydration biomarkers and total fluid intake in pregnant and lactating women. Eur. J. Nutr. 2016, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Padrao, P.; Neto, M.; Pinto, M.; Oliveira, A.C.; Moreira, A.; Moreira, P. Urinary hydration biomarkers and dietary intake in children. Nutr. Hosp. 2016, 33 (Suppl. 3), 35–40. [Google Scholar] [CrossRef] [PubMed]
- Ma, G.; Zhang, Q.; Liu, A.; Zuo, J.; Zhang, W.; Zou, S.; Li, X.; Lu, L.; Pan, H.; Hu, X. Fluid intake of adults in four Chinese cities. Nutr. Rev. 2012, 70 (Suppl. 2), S105–S110. [Google Scholar] [CrossRef] [PubMed]
- Grigg, D. The worlds of tea and coffee: Patterns of consumption. GeoJournal 2002, 57, 283–294. [Google Scholar] [CrossRef]
- Liu, J.; Hhg, S. Food consumption patterns and their effect on water requirement in China. Hydrol. Earth Syst. Sci. 2008, 5, 27–50. [Google Scholar] [CrossRef]
- Institute of Medicine (US). DRI, Dietary Reference Intakes for Water, Potassium, Sodium, Chloride, and Sulfate; National Academy Press: Washington, DC, USA, 2005. [Google Scholar]
- Sm, D.U.; Hu, X.Q.; Zhang, Q.; Wang, X.J.; Pan, H.; Gao, J.M.; Song, J.; Gao, C.L.; He, Z.F.; Ma, G.S. Daily intake of plain water and beverages of primary and middle school students in four cities of China. Zhonghua Yu Fang Yi Xue Za Zhi 2013, 47, 202. [Google Scholar]
- Fu, C.; Jiang, Z.; Guan, Z.; He, J.; Xu, Z.-F. Regional Climate Studies of China; Springer: Heidelberg, Germany, 2008. [Google Scholar]
- Zhang, Y.Y.; Liu, P.Y.; Lu, Y.; Davies, K.M.; Dvornyk, V.; Recker, R.R.; Deng, H.W. Race and sex differences and contribution of height: A study on bone size in healthy Caucasians and Chinese. Am. J. Hum. Biol. 2005, 17, 568–575. [Google Scholar] [CrossRef] [PubMed]
- Wohlfarth, G.W.; Moav, R.; Hulata, G. Genetic differences between the Chinese and European races of common carp: 5. Differential adaptation to manure and artificial feeds. Theor. Appl. Genet. 1990, 79, 693–698. [Google Scholar] [CrossRef] [PubMed]
- Perrier, E.T.; Buendiajimenez, I.; Vecchio, M.; Armstrong, L.E.; Tack, I.; Klein, A. Twenty-Four-Hour Urine Osmolality as a Physiological Index of Adequate Water Intake. Dis. Markers 2015, 2015, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Pross, N.; Demazières, A.; Girard, N.; Barnouin, R.; Metzger, D.; Klein, A.; Perrier, E.; Guelinckx, I. Effects of changes in water intake on mood of high and low drinkers. PLoS ONE 2014, 9, e94754. [Google Scholar] [CrossRef] [PubMed]
- Finn, K.J.; Saintmaurice, P.F.; Karsai, I.; Ihász, F.; Csányi, T. Agreement Between Omron 306 and Biospace InBody 720 Bioelectrical Impedance Analyzers (BIA) in Children and Adolescents. Res. Q. Exerc. Sport 2015, 86 (Suppl. 1), S58–S65. [Google Scholar] [CrossRef] [PubMed]
- Du, B.D.; Du, B.E. A formula to estimate the approximate surface area if height and weight be known. 1916. Nutrition 1989, 5, 303–311. [Google Scholar]
- Standardization Administration of China. National Food Safety Standard GB 5009.3-2010: Determination of Moisture in Foods; China Standard Press: Beijing, China, 2010.
- Institute for Nutrition and Health, Chinese Center for Disease Control and Prevention. China Food Composition; Peking University Medicine Press: Beijing, China, 2009. [Google Scholar]
- Burchfield, J.M.; Ganio, M.S.; Kavouras, S.A.; Adams, J.D.; Gonzalez, M.A.; Ridings, C.B.; Moyen, N.E.; Tucker, M.A. 24-h Void number as an indicator of hydration status. Eur. J. Clin. Nutr. 2015, 69, 638–641. [Google Scholar] [CrossRef] [PubMed]
- Stookey, J.D.; Brass, B.; Holliday, A.; Arieff, A. What is the cell hydration status of healthy children in the USA? Preliminary data on urine osmolality and water intake. Public Health Nutr. 2012, 15, 2148–2156. [Google Scholar] [CrossRef] [PubMed]
- Mckenzie, A.L.; Muñoz, C.X.; Ellis, L.A.; Perrier, E.T.; Guelinckx, I.; Klein, A.; Kavouras, S.A.; Armstrong, L.E. Urine color as an indicator of urine concentration in pregnant and lactating women. Eur. J. Nutr. 2017, 56, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, L.E.; Johnson, E.C.; Mckenzie, A.L.; Muñoz, C.X. An empirical method to determine inadequacy of dietary water. Nutrition 2016, 32, 79–82. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| All Subjects (n = 68) | Optimal Hydration (n = 24) | Middle Hydration (n = 27) | Hypohydration (n = 17) | F | p | |
|---|---|---|---|---|---|---|
| Age (years) | 19.9 ± 1.1 | 20.3 ± 1.2 | 19.7 ± 1.1 | 19.5 ± 0.8 | 2.931 | 0.060 |
| Height (cm) | 174.0 ± 5.2 | 173.1 ± 4.6 | 174.6 ± 5.3 | 174.4 ± 6.0 | 0.594 | 0.555 |
| Weight (kg) | 67.9 ± 10.8 | 67.0 ± 11.0 | 67.8 ± 12.2 | 69.5 ± 8.3 | 0.249 | 0.780 |
| BMI (kg/m2) | 22.4 ± 3.6 | 22.4 ± 3.5 | 22.2 ± 4.0 | 22.9 ± 3.2 | 0.173 | 0.842 |
| Waist circumference (cm) | 79.2 ± 9.0 | 79.6 ± 7.9 | 78.9 ± 10.6 | 79.2 ± 8.1 | 0.046 | 0.955 |
| Body surface area (m2) | 1.813 ± 0.133 | 1.796 ± 0.135 | 1.814 ± 0.148 | 1.835 ± 0.106 | 0.430 | 0.652 |
| Body protein content (kg) | 10.7 ± 1.2 | 10.5 ± 1.2 | 10.6 ± 1.2 | 11.0 ± 1.0 | 1.086 | 0.343 |
| Percent body fat mass (%) | 20.1 ± 6.8 | 20.7 ± 6.9 | 19.7 ± 7.4 | 19.8 ± 5.9 | 0.144 | 0.866 |
| Indoors | Outdoors | |||
|---|---|---|---|---|
| Temperature (°C) | Humidity (%) | Temperature (°C) | Humidity (%) | |
| Sunday | 15.3 | 33 | 11.6 | 32 |
| Monday | 16.9 | 34 | 12.5 | 32 |
| Tuesday | 14.6 | 31 | 5.4 | 35 |
| Wednesday | 15.2 | 32 | 5.6 | 34 |
| Thursday | 13.9 | 33 | 6.1 | 35 |
| Friday | 13.1 | 31 | 6.9 | 35 |
| Saturday | 12.0 | 34 | 10.0 | 42 |
| All Subjects (n = 68) | Optimal Hydration (n = 24) | Middle Hydration (n = 27) | Hypohydration (n = 17) | F | p | |
|---|---|---|---|---|---|---|
| Daily total fluid intake (mL) | 2553 ± 653 | 3114 ± 543 # | 2405 ± 467 ‡ | 1995 ± 407 † | 28.956 | 0.000 * |
| Percentage meeting adequate total fluid intake (based on intake recommendations in China) (%) | 17 (25.0) | 14 (58.3) # | 3 (6.8) | 0 (0.0) † | 22.667 | 0.000 * |
| Percent meeting the EFSA fluid intake recommendations (%) | 38 (55.9) | 22 (91.7) | 12 (17.6) | 7 (10.3) † | 3.608 | 0.165 |
| Daily fluid intake from food (mL) | 1211 ± 232 | 1381 ± 202 # | 1155 ± 202 | 1059 ± 165 † | 15.628 | 0.000 * |
| Daily total drinking fluid (mL) | 1342 ± 468 | 1733 ± 399 # | 1250 ± 342 ‡ | 936 ± 281 † | 27.410 | 0.000 * |
| Percentage meeting adequate total drinking fluid intake (based on intake recommendations in China) (%) | 16 (23.5) | 13 (54.2) # | 3 (6.8) | 0 (0.0) † | 20.065 | 0.000 * |
| All Subjects (n = 68) | Optimal Hydration (n = 24) | Middle Hydration (n = 27) | Hypohydration (n = 17) | F | p | |
|---|---|---|---|---|---|---|
| 24-h urine volume (mL) | 1358 ± 460 | 1653 ± 420 # | 1338 ± 393 ‡ | 975 ± 307 † | 15.621 | 0.000 * |
| 24-h urine osmolality (mOsm/kg) | 653 ± 201 | 452 ± 43 # | 657 ± 86 ‡ | 932 ± 104 † | 183.120 | 0.000 * |
| 24-h urine USG | 1.011 ± 0.003 | 1.014 ± 0.003 # | 1.019 ± 0.003 ‡ | 1.010 ± 0.003 † | 29.127 | 0.000 * |
| 24-h urine pH | 6.5 ± 0.3 | 6.7 ± 0.4 | 6.7 ± 0.3 | 6.9 ± 0.3 | 2.557 | 0.085 |
| 24-h urine potassium (mmol/L) | 27.7 ± 11.8 | 19.2 ± 5.2 # | 26.5 ± 5.2 ‡ | 41.5 ± 13.8 † | 37.169 | 0.000 * |
| 24-h urine sodium (mmol/L) | 164 ± 53 | 127 ± 33 # | 152 ± 20 ‡ | 235 ± 43 † | 62.393 | 0.000 * |
| 24-h urine chloride (mmol/L) | 142 ± 53 | 105 ± 27.4 # | 129 ± 18.1 ‡ | 215 ± 48.0 † | 66.222 | 0.000 * |
| Daily Total Fluid Intake | Fluid Intake from Food | Daily Total Drinking Water | ||||
|---|---|---|---|---|---|---|
| r | p | r | p | r | p | |
| All subjects (n = 68) | ||||||
| 24-h urine volume | 0.76 | 0.000 * | 0.7 | 0.000 * | 0.72 | 0.000 * |
| 24-h urine osmolality | −0.76 | 0.000 * | −0.63 | 0.000 * | −0.75 | 0.000 * |
| 24-h USG | −0.56 | 0.000 * | −0.47 | 0.000 * | −0.54 | 0.000 * |
| 24-h pH | −0.25 | 0.072 | −0.19 | 0.359 | −0.25 | 0.038 * |
| Potassium (mmol/L) | −0.5 | 0.000 * | −0.45 | 0.000 * | −0.47 | 0.000 * |
| Sodium (mmol/L) | −0.61 | 0.000 * | −0.45 | 0.000 * | −0.62 | 0.000 * |
| Chloride (mmol/L) | −0.57 | 0.000 * | −0.42 | 0.001 * | −0.59 | 0.000 * |
| VIP > 0.8 | VIP < 0.8 | ||
|---|---|---|---|
| 24-h urine volume | 1.41 | 24-h urine potassium concentration | 0.84 |
| 24-h urine osmolality | 1.17 | 24-h urine pH | 0.45 |
| 24-h urine-specific gravity | 0.91 | ||
| 24-h urine sodium concentration | 0.98 | ||
| 24-h urine chloride concentration | 0.98 | ||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, N.; Du, S.; Tang, Z.; Zheng, M.; Yan, R.; Zhu, Y.; Ma, G. Hydration, Fluid Intake, and Related Urine Biomarkers among Male College Students in Cangzhou, China: A Cross-Sectional Study—Applications for Assessing Fluid Intake and Adequate Water Intake. Int. J. Environ. Res. Public Health 2017, 14, 513. https://doi.org/10.3390/ijerph14050513
Zhang N, Du S, Tang Z, Zheng M, Yan R, Zhu Y, Ma G. Hydration, Fluid Intake, and Related Urine Biomarkers among Male College Students in Cangzhou, China: A Cross-Sectional Study—Applications for Assessing Fluid Intake and Adequate Water Intake. International Journal of Environmental Research and Public Health. 2017; 14(5):513. https://doi.org/10.3390/ijerph14050513
Chicago/Turabian StyleZhang, Na, Songming Du, Zhenchuang Tang, Mengqi Zheng, Ruixia Yan, Yitang Zhu, and Guansheng Ma. 2017. "Hydration, Fluid Intake, and Related Urine Biomarkers among Male College Students in Cangzhou, China: A Cross-Sectional Study—Applications for Assessing Fluid Intake and Adequate Water Intake" International Journal of Environmental Research and Public Health 14, no. 5: 513. https://doi.org/10.3390/ijerph14050513
APA StyleZhang, N., Du, S., Tang, Z., Zheng, M., Yan, R., Zhu, Y., & Ma, G. (2017). Hydration, Fluid Intake, and Related Urine Biomarkers among Male College Students in Cangzhou, China: A Cross-Sectional Study—Applications for Assessing Fluid Intake and Adequate Water Intake. International Journal of Environmental Research and Public Health, 14(5), 513. https://doi.org/10.3390/ijerph14050513