
Enterovirus 71 Neutralizing Antibodies Seroepidemiological Research among Children in Guangzhou, China between 2014 and 2015: A Cross-Sectional Study

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Demographic Information
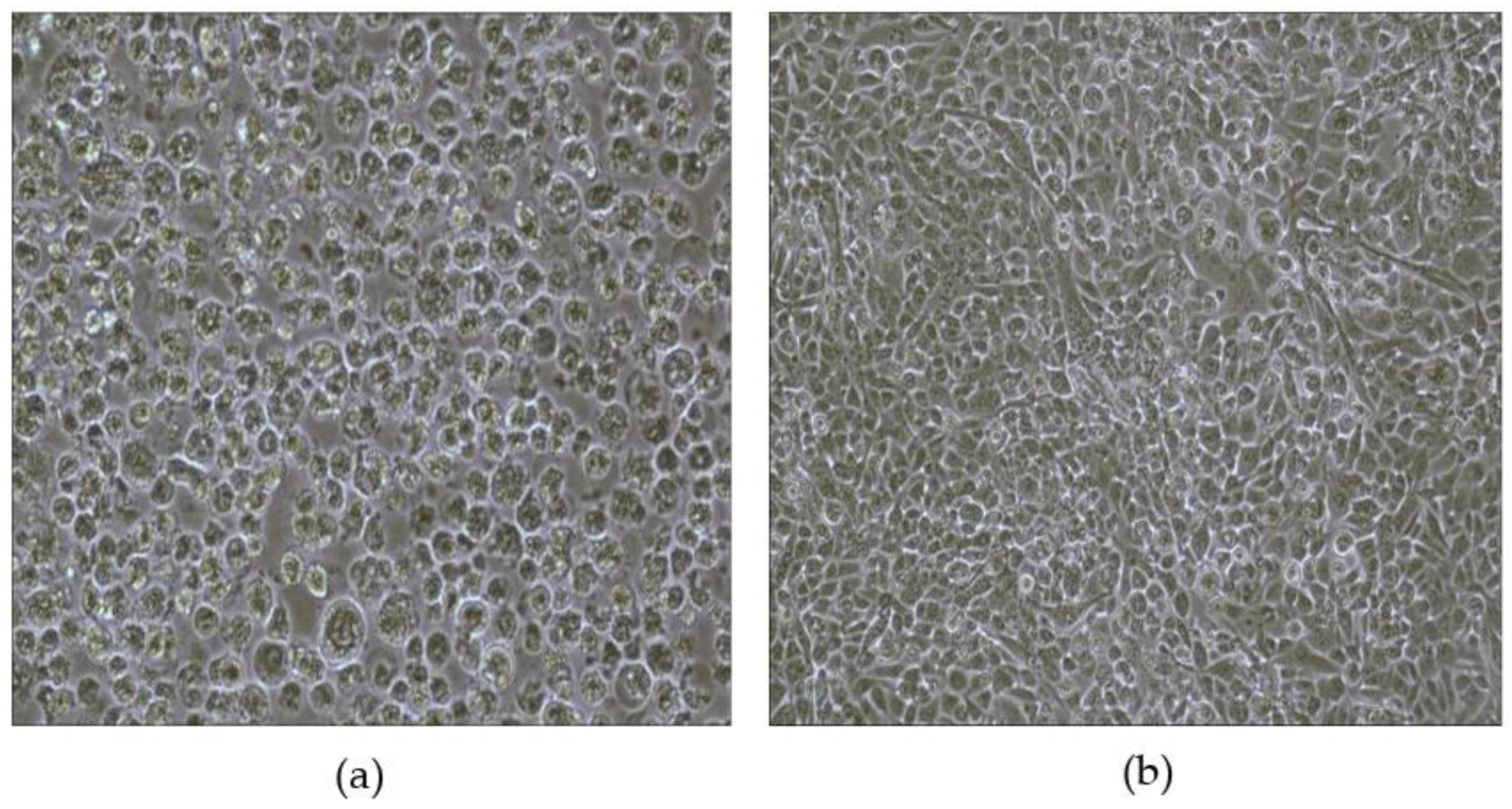
3.2. Presence or Absence of CPE
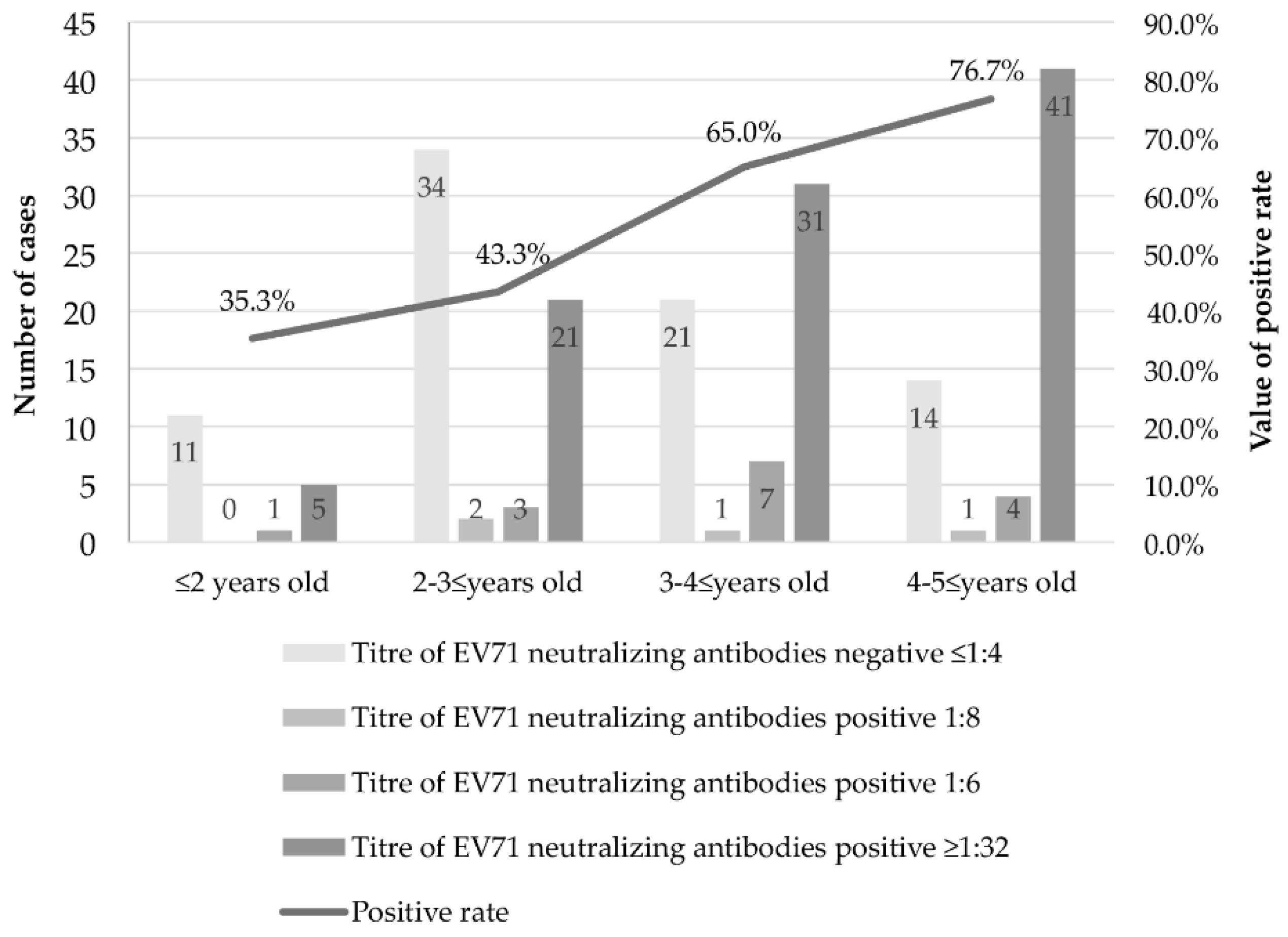
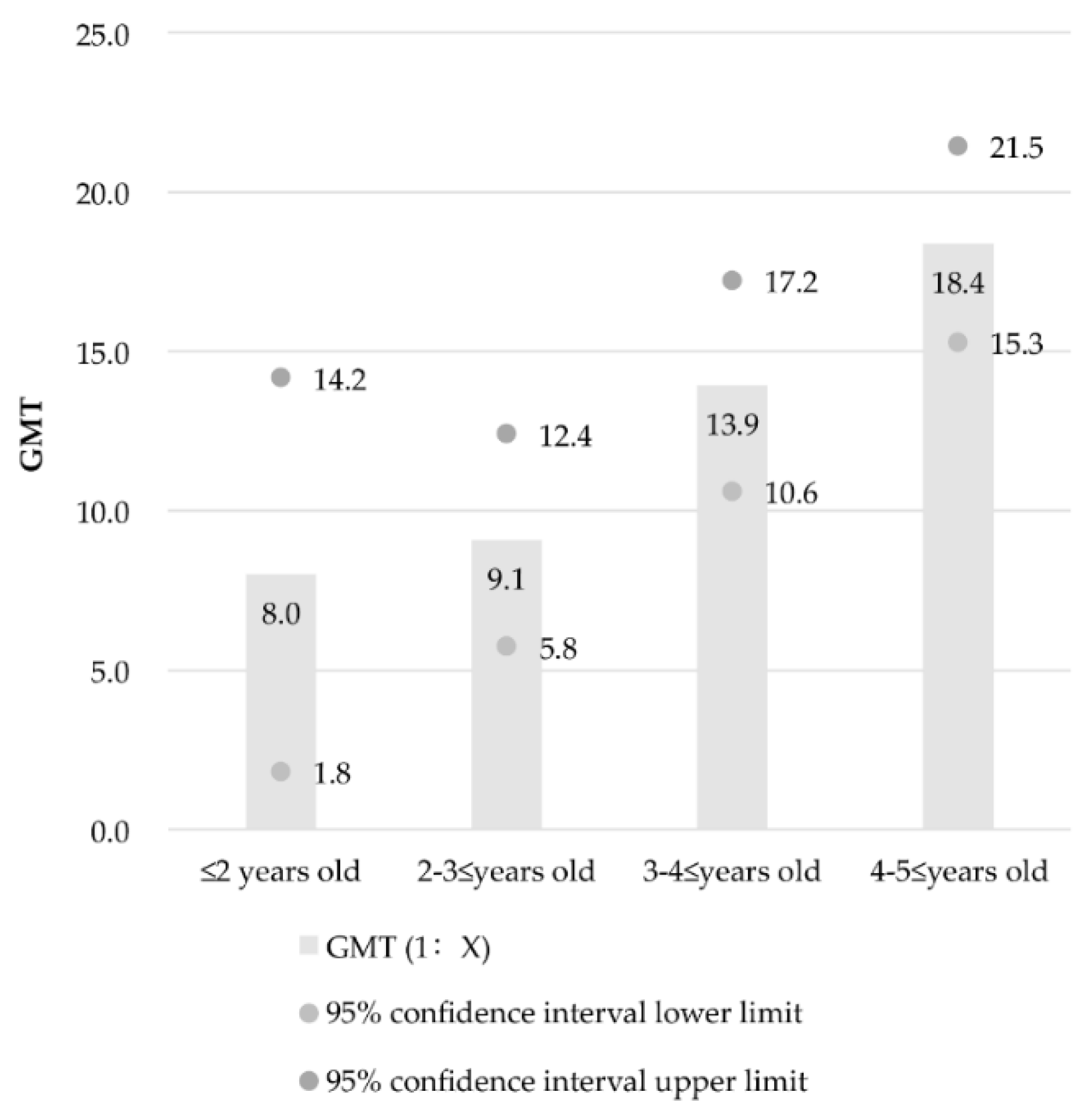
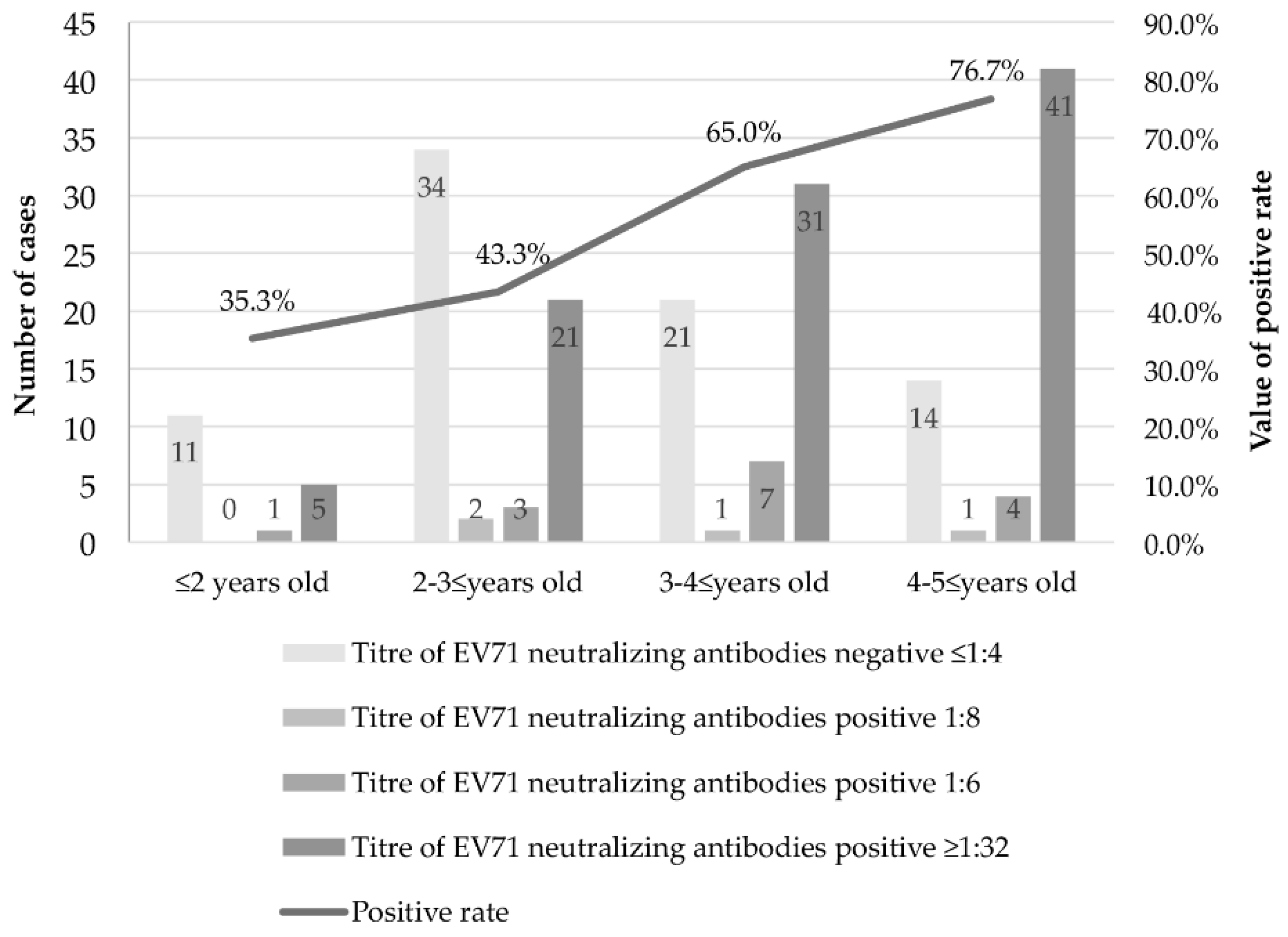
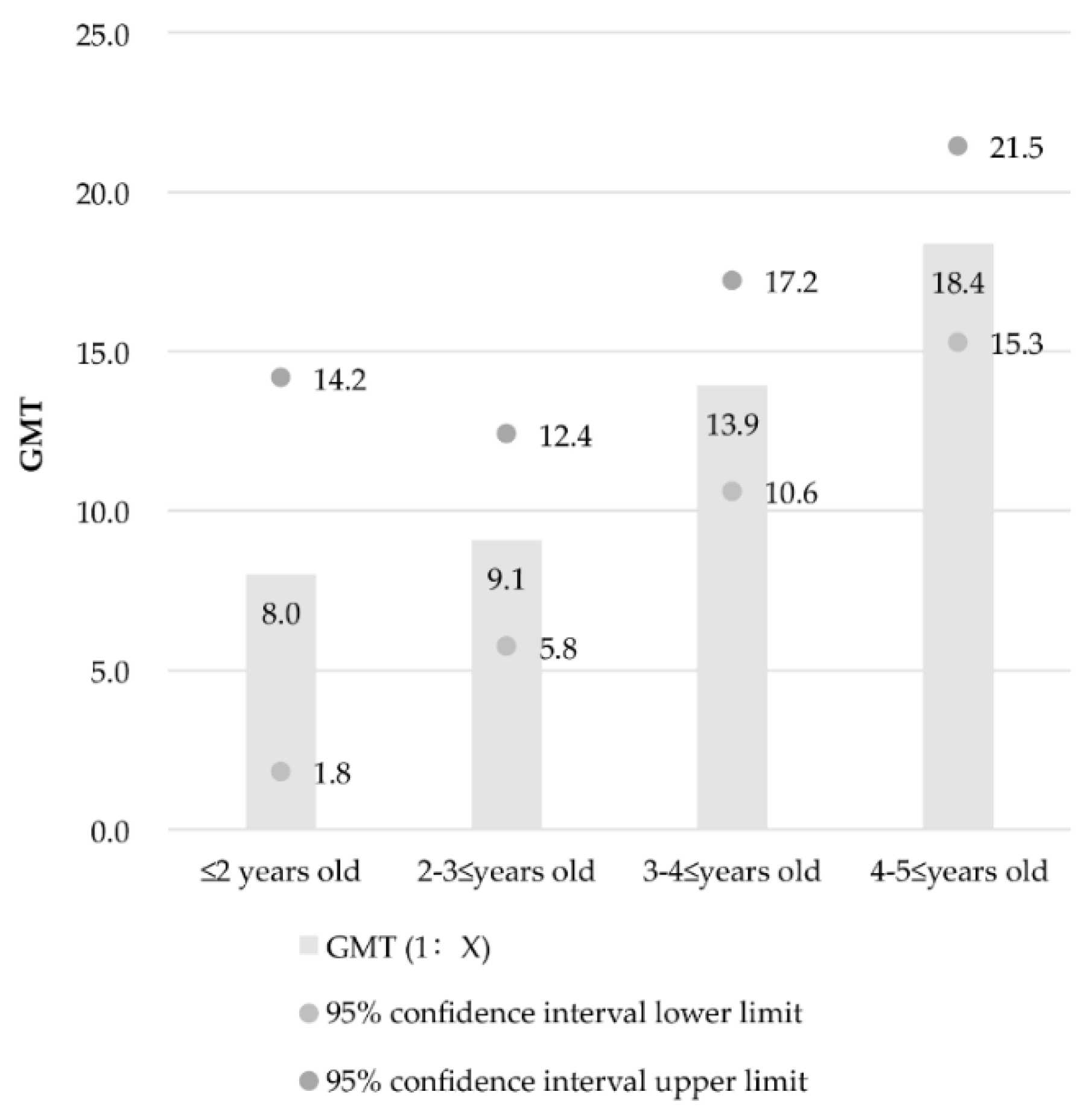
3.3. Results between Different Age Groups
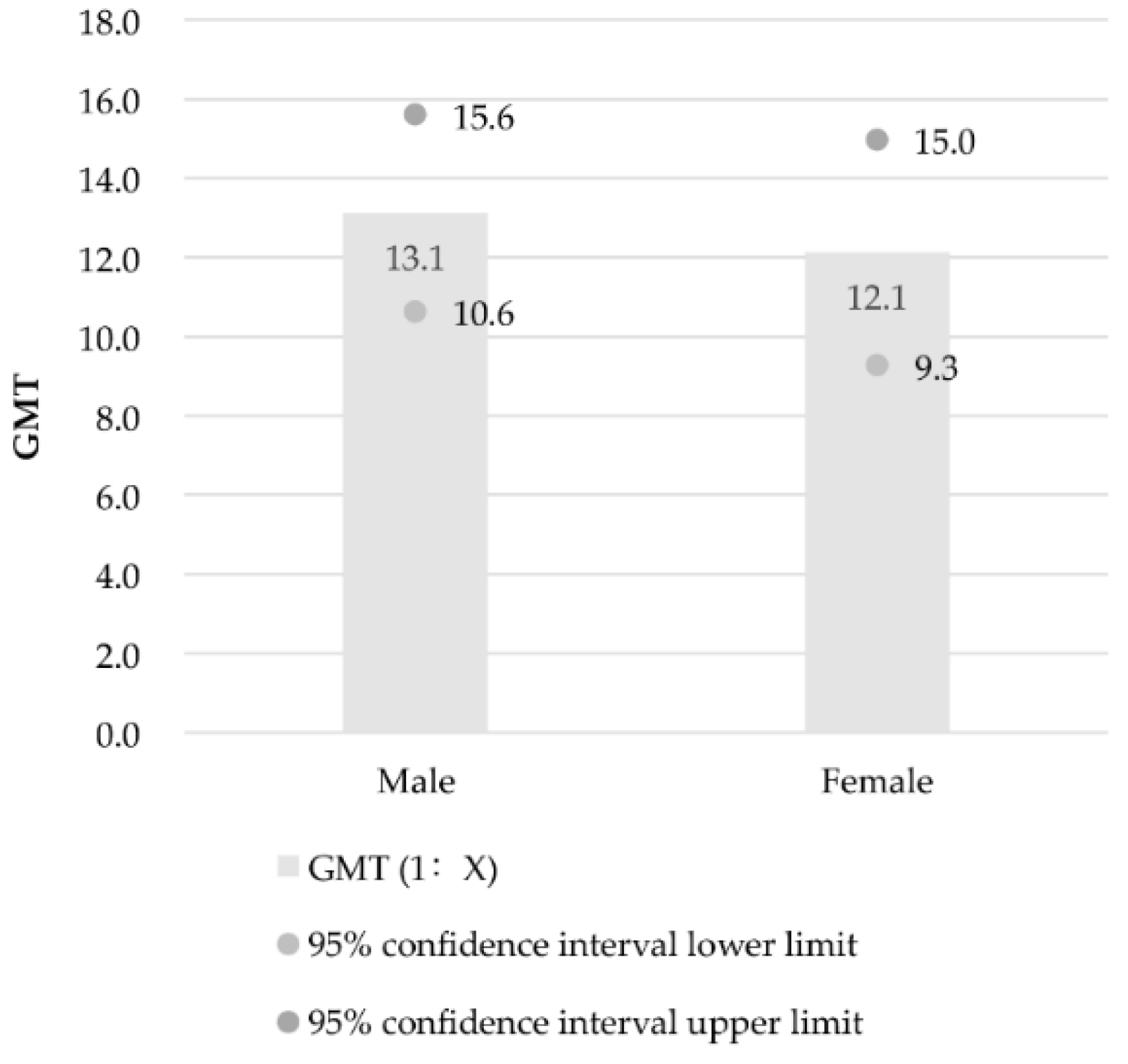
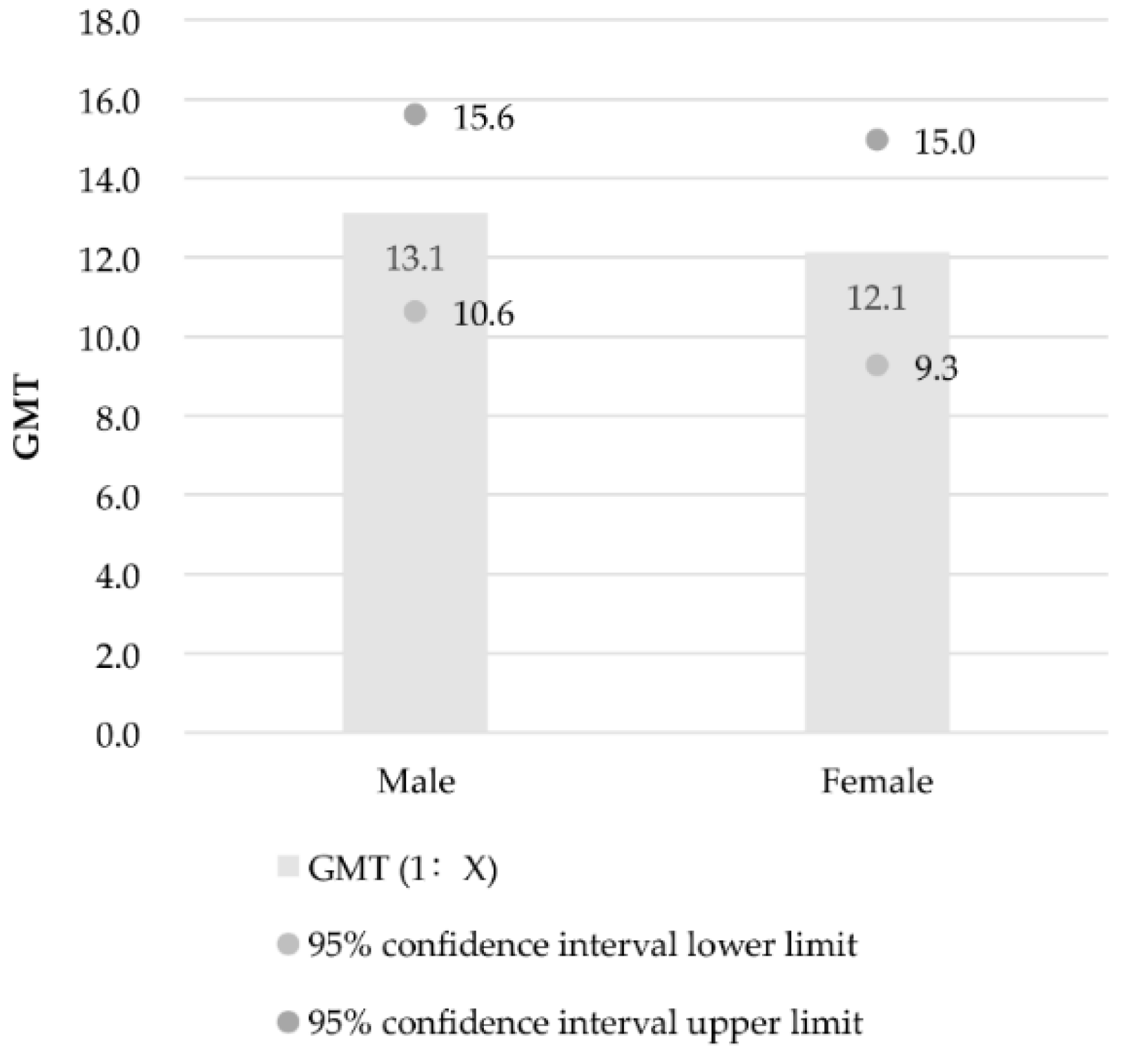
3.4. Results between Different Genders
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- World Health Organization. Hand, Foot and Mouth Disease. Available online: http://www.wpro.who.int/emerging_diseases/HFMD/en/ (accessed on 18 March 2016).
- Zhang, W.; Ji, Z.; Guo, P.; Gu, J.; Yu, S.; Hao, Y. Epidemiological features and trends of Hand, Foot and Mouth Disease in Guangdong Province, 2009–2012. J. Sun Yat-Sen Univ. Med. Sci. 2014, 35, 607–613. [Google Scholar]
- Jin, Y.; Zhang, J.; Sun, J.; Chang, Z. Epidemiology of hand, foot and mouth disease in mainland of China, 2011. Dis. Surveill. 2012, 27, 676–679. [Google Scholar]
- Lum, L.C.; Wong, K.T.; Lam, S.K.; Chua, K.B.; Goh, A.Y.T. Neurogenic pulmonary oedema and enterovirus 71 encephalomyelitis. Lancet 1998, 352, 1391. [Google Scholar] [CrossRef]
- National Health and Family Planning Commission of the People’s Republic of China. Guidebook of Hand-Foot-And-Mouth Disease Diagnosis and Treatments (2010 Edition). 2010. Available online: http://www.nhfpc.gov.cn/yzygj/s3593g/201306/6d935c0f43cd4a1fb46f8f71acf8e245.shtml (accessed on 18 March 2016). [Google Scholar]
- Diedrich, S.; Weinbrecht, A.; Schreier, E. Seroprevalence and molecular epidemiology of enterovirus 71 in Germany. Arch. Virol. 2009, 154, 1139–1142. [Google Scholar] [CrossRef] [PubMed]
- Gomes, M.L.C.; Castro, C.M.O.; Oliveira, M.J.C.; Da Silva, E.E. Neutralizing antibodies to enterovirus 71 in Belém, Brazil. Mem. Ins. Oswaldo Cruz 2002, 97, 47–49. [Google Scholar] [CrossRef]
- Ooi, E.-E.; Phoon, M.-C.; Ishak, B.; Chan, S.-H. Seroepidemiology of Human enterovirus 71, Singapore. Emerg. Infect. Dis. 2002, 8, 995–997. [Google Scholar] [CrossRef] [PubMed]
- Lin, K.H.; Hwang, K.P.; Ke, G.M.; Wang, C.F.; Ke, L.Y.; Hsu, Y.T.; Tung, Y.C.; Chu, P.Y.; Chen, B.H.; Chen, H.L.; et al. Evolution of EV71 genogroup in Taiwan from 1998 to 2005: An emerging of subgenogroup C4 of EV71. J. Med. Virol. 2006, 78, 254–262. [Google Scholar] [CrossRef] [PubMed]
- Shih, S.R.; Ho, M.S.; Lin, K.H.; Wu, S.L.; Chen, Y.T.; Wu, C.N.; Lin, T.Y.; Chang, L.Y.; Tsao, K.C.; Ning, H.C.; et al. Genetic analysis of enterovirus 71 isolated from fatal and non-fatal cases of hand, foot and mouth disease during an epidemic in Taiwan, 1998. Virus Res. 2000, 68, 127–136. [Google Scholar] [CrossRef]
- Zhou, S.; Li, L.; He, Y. Seroepidemiological preliminary investigation of enterovirus 71 in Shenzhen. J. Trop. Med. 2007, 7, 66–67. [Google Scholar]
- Huang, X.Y.; Liu, G.H.; Chen, H.M.; Kang, K.; Li, X.L.; Du, Y.H.; Wei, H.Y.; Deng, W.B.; Wang, H.F.; Xu, Y.L.; et al. Seroepidemiological study of enterovirus 71 in Henan Province. J. Pathog. Biol. 2010, 8, 19. [Google Scholar]
- Sun, B.; Gao, J.; Chen, D.; Dou, H.; Zhu, C. Study on the recessive infection of hand, foot and mouth disease (HFMD) virus in children. Pract. Prev. Med. 2014, 21, 914–916. [Google Scholar]
- Mao, G.; Liu, X.; Zhao, Y. Study on neutralization antibody to enterovirus 71 in patients with hand-foot-mouth disease. Chin. J. Gen. Pract. 2012, 10, 1368. [Google Scholar]
- Xu, Y.; Yang, L.; Qi, J.-J.; Li, S.; Xin, Y.; Huang, X.-Y.; Xu, B.-L. Seroepidemiological study of enterovirus 71 among healthy children during 2010 to 2012 in Henan Province of China. Chin. J. Viral Dis. 2014, 4, 141–143. [Google Scholar]
- Rong, X.; Li, X.; Tian, X.; Zhou, R.; Fu, Y.; Peng, T. Seroepidemiology investigation of EV71 neutralizing activity in healthy blood donors in Guangzhou. Chin. J. Blood Transfus. 2010, 23, 197–200. [Google Scholar]
- Scotti, P.D. End-point dilution and plaque assay methods for titration of cricket paralysis virus in cultured drosophila cells. J. Gen. Virol. 1977, 35, 393–396. [Google Scholar] [CrossRef] [PubMed]
- Smither, S.J.; Lear-Rooney, C.; Biggins, J.; Pettitt, J.; Lever, M.S.; Olinger, G.G., Jr. Comparison of the plaque assay and 50% tissue culture infectious dose assay as methods for measuring filovirus infectivity. J. Virol. Methods. 2013, 193, 565–571. [Google Scholar] [CrossRef] [PubMed]
- Reed, L.J.; Muench, H. A simple method of estimating fifty percent endpoints. Am. J. Hyg. 1938, 27, 493–497. [Google Scholar]
- National Health and Family Planning Commission of the People’s Republic of China. Guidebook of Hand-Foot-And-Mouth Disease Prevention and Control (2009 edition). Available online: http://www.gov.cn/gzdt/2009-06/04/content_1332078.htm (accessed on 5 February 2016).
- Chen, R.; Pan, R.; Lai, Z.; Mo, H.; Zhang, Y.; Zhou, H. Testing enterovirus 71 and CAV16 neutralizing antibodies in healthy population by micro-cytopathic-effect. Chin. J. Prev. Med. 2013, 14, 362–365. [Google Scholar]
- Li, J.; Xu, Y.; Wang, Q. Investigation of enterovirus 71 antibody levels among children in the Longgang District, City of Shenzhen. J. Pathog. Biol. 2012, 7, 924–926. [Google Scholar]
- Kuang, L.; Wang, C.B.; Liang, Z.F.; Zhong, J.Y.; Xiao, M.S.; Zhu, B. Investigation on enterovirus 71 antibody levels among children in Guangzhou area. Chin. J. Evid. Based Pediatr. 2011, 6, 211–214. [Google Scholar]
- Zeng, M.; El Khatib, N.F.; Tu, S.; Ren, P.; Xu, S.; Zhu, Q.; Mo, X.; Pu, D.; Wang, X.; Altmeyer, R. Seroepidemiology of enterovirus 71 infection prior to the 2011 season in children in Shanghai. J. Clin. Virol. 2012, 53, 285–289. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Yi, L.; Su, J.; Ke, C.; Zeng, H.; Guan, D.; Ma, C.; Zhang, W.; Xiao, H.; Li, H. Seroprevalence of human enterovirus 71 and Coxsackievirus A16 in Guangdong, China, in pre- and post-2010 HFMD epidemic period. PLoS ONE 2013. [Google Scholar] [CrossRef] [PubMed]
- Linsuwanon, P.; Puenpa, J.; Huang, S.W.; Wang, Y.F.; Mauleekoonphairoj, J.; Wang, J.R.; Poovorawan, Y. Epidemiology and seroepidemiology of human enterovirus 71 among Thai populations. J. Biomed. Sci. 2014, 21. [Google Scholar] [CrossRef] [PubMed]
- A Phase II, Safety and Efficacy Study of Inactivated EV 71 Vaccine (Human Diploid Cell, KMB-17) in Chinese Infants. Available online: https://clinicaltrials.gov/ct2/show?term=HFMD+EV71+vaccine+or+Enterovirus+type+71+inactivated+vaccines&cntry1=ES%3ACN&rank=3 (accessed on 5 February 2016).
- Zhu, F.C.; Meng, F.Y.; Li, J.X.; Li, X.L.; Mao, Q.Y.; Tao, H.; Zhang, Y.T.; Yao, X.; Chu, K.; Chen, Q.H.; et al. Efficacy, safety, and immunology of an inactivated alum-adjuvant enterovirus 71 vaccine in children in China: A multicentre, randomized, double-blind, placebo-controlled, phase 3 trial. Lancet 2013, 381, 2024–2032. [Google Scholar] [CrossRef]
- Rabenau, H.F.; Richter, M.; Doerr, H.W. Hand, foot and mouth disease: Seroprevalence of Coxsackie A16 and enterovirus 71 in Germany. Med. Microbiol. Immun. 2010, 199, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Horwood, P.F.; Andronico, A.; Tarantola, A.; Salje, H.; Duong, V.; Mey, C.; Ly, S.; Dussart, P.; Cauchemez, S.; Buchy, P. Seroepidemiology of human enterovirus 71 infection among children, Cambodia. Emerg. Infect. Dis. 2016, 22, 92–95. [Google Scholar] [CrossRef] [PubMed]
- Chang, L.Y.; King, C.C.; Hsu, K.H.; Ning, H.C.; Tsao, K.C.; Li, C.C.; Huang, Y.C.; Shih, S.R.; Chiou, S.T.; Chen, P.Y.; et al. Risk factors of enterovirus 71 infection and associated hand, foot, and mouth disease/herpangina in children during an epidemic in Taiwan. Pediatrics 2002, 109. [Google Scholar] [CrossRef]

© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, D.; Chen, Y.; Chen, X.; He, Z.; Zhu, X.; Hao, Y. Enterovirus 71 Neutralizing Antibodies Seroepidemiological Research among Children in Guangzhou, China between 2014 and 2015: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2017, 14, 319. https://doi.org/10.3390/ijerph14030319
Zhang D, Chen Y, Chen X, He Z, Zhu X, Hao Y. Enterovirus 71 Neutralizing Antibodies Seroepidemiological Research among Children in Guangzhou, China between 2014 and 2015: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2017; 14(3):319. https://doi.org/10.3390/ijerph14030319
Chicago/Turabian StyleZhang, Dingmei, Yan Chen, Xiashi Chen, Zhenjian He, Xun Zhu, and Yuantao Hao. 2017. "Enterovirus 71 Neutralizing Antibodies Seroepidemiological Research among Children in Guangzhou, China between 2014 and 2015: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 14, no. 3: 319. https://doi.org/10.3390/ijerph14030319
APA StyleZhang, D., Chen, Y., Chen, X., He, Z., Zhu, X., & Hao, Y. (2017). Enterovirus 71 Neutralizing Antibodies Seroepidemiological Research among Children in Guangzhou, China between 2014 and 2015: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 14(3), 319. https://doi.org/10.3390/ijerph14030319