Doses of Nearby Nature Simultaneously Associated with Multiple Health Benefits

 , , , ,
, , , ,
Abstract
:1. Background
2. Methods
2.1. Study Area and Survey Design
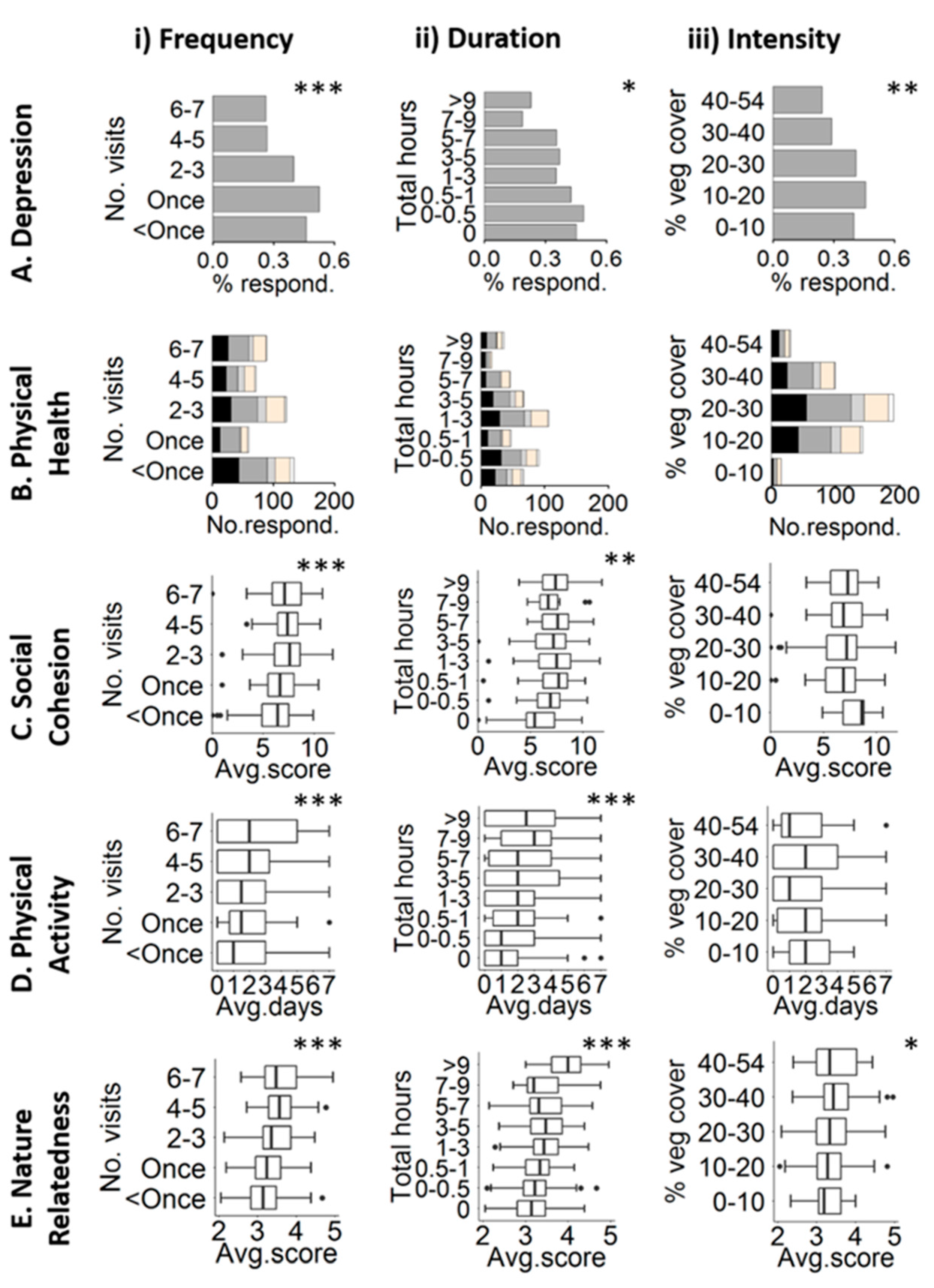
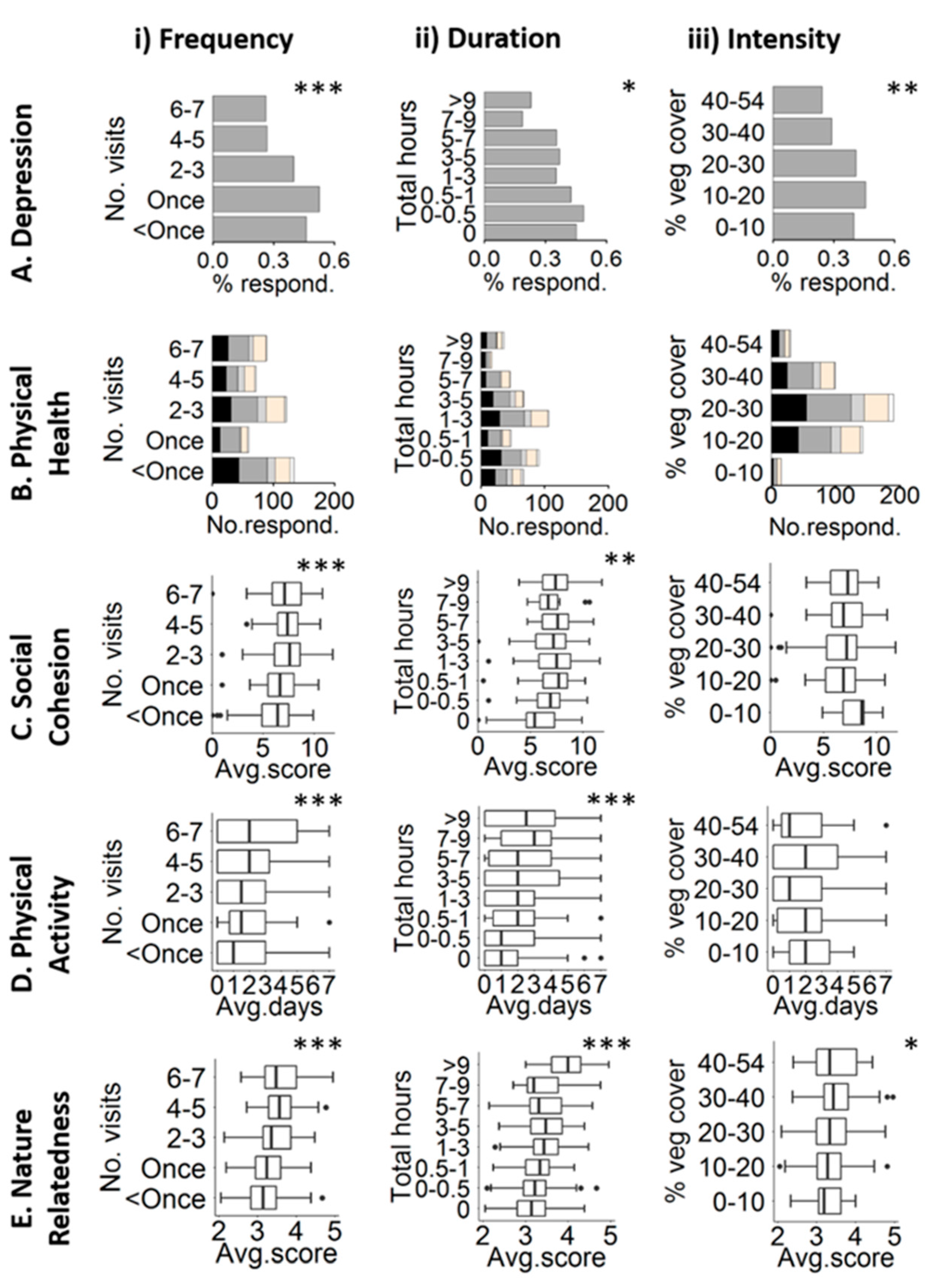
2.2. Health Response Variables
- Mental health (binary): A measure of depression was generated based on the depression component of the short version of the Depression, Anxiety and Stress Scale (DASS 21; [33]). Scores were converted to a binary measure, where 0 indicates no depression and 1 indicates mild or worse depression (see Section 1 in Supplementary Materials). Proposed mechanisms for the delivery of these benefits include improved cognition in individuals with depression [34], reduced rumination and reduced neural activity in an area of the brain linked to the risk of mental illness [12].
- Physical health (ordinal): Respondents scored their own general health on a five-point scale from very poor to very good [35]. This scale is related to morbidity and mortality rates and is a strong predictor of health status and outcomes [36]. Proposed mechanisms behind benefit delivery include temperature regulation and pollution filtration by vegetation (reviewed by [27,37]).
- Social health (linear): Perceptions of social cohesion were estimated based on three previously developed scales that measure trust, reciprocal exchange within communities and general community cohesion ([38,39,40], see Section 2 in Supplementary Materials). The average score across questions for each scale was calculated, highest (4) to the lowest (0). Average scores were then summed to provide a scale from highest (12) to lowest (0). Appealing green spaces promote a sense of connection to the outside world that generalizes to most people; this allows enhanced social and community interactions, leading to improved perceptions of cohesion and well-being [41].
- Physical behaviour (Poisson): This is a self-reported indication of the number of days respondents exercised for a minimum of 30 min during the survey week (the duration recommended by the UK government) [42]. Appealing green spaces promote use [10] and willingness to travel greater distances for use [43]. Further, green exercise can enhance health benefits relative to built-up or indoor environments [30].
- Nature orientation (linear): Respondents provided a measure of their affective, cognition and experiential relationship with the natural world (nature relatedness scale) [31]. Responses were aggregated according to [31], with a higher score indicating a stronger orientation towards nature. Engagement with the natural world increases feelings of connection, unity or being part of the natural world, which has been linked to psychological health [44]. Indeed, increased nature connection has been associated with improved mental health [45] and subjective well-being [46,47].
2.3. Nature Dose
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Keniger, L.E.; Gaston, K.J.; Irvine, K.N.; Fuller, R.A. What are the benefits of interacting with nature? Int. J. Environ. Res. Public Health 2013, 10, 913–935. [Google Scholar] [CrossRef] [PubMed]
- Hartig, T.; Mitchell, R.; de Vries, S.; Frumkin, H. Nature and health. Annu. Rev. Public Health 2014, 35, 207–228. [Google Scholar] [CrossRef] [PubMed]
- White, M.P.; Alcock, I.; Wheeler, B.W.; Depledge, M.H. Would you be happier living in a greener urban area? A fixed-effects analysis of panel data. Psychol. Sci. 2013, 24, 920–928. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, R.; Popham, F. Effect of exposure to natural environment on health inequalities: An observational population study. Lancet 2008, 372, 1655–1660. [Google Scholar] [CrossRef]
- Donovan, G.H.; Butry, D.T.; Michael, Y.L.; Prestemon, J.P.; Liebhold, A.M.; Gatziolis, D.; Mao, M.Y. The relationship between trees and human health evidence from the spread of the emerald ash borer. Am. J. Prev. Med. 2013, 44, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Kingsley, J.Y.; Townsend, M. “Dig In” to social capital: Community gardens as mechanisms for growing urban social connectedness. Urban Policy Res. 2006, 24, 525–537. [Google Scholar] [CrossRef]
- Sugiyama, T.; Francis, J.; Middleton, N.J.; Owen, N.; Giles-Corti, B. Associations between recreational walking and attractiveness, size, and proximity of neighborhood open spaces. Am. J. Public Health 2010, 100, 1752–1757. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.; Ory, M.G.; Yoon, J.; Forjuoh, S.N. Neighborhood walking among overweight and obese adults: Age variations in barriers and motivators. J. Community Health 2013, 38, 12–22. [Google Scholar] [CrossRef] [PubMed]
- Lin, B.B.; Gaston, K.J.; Fuller, R.A.; Wu, D.; Bush, R.; Shanahan, D.F. How green is your garden? Urban form and socio-demographic factors influence yard vegetation, visitation, and ecosystem service benefits. Landsc. Urban Plan. 2017, 157, 239–246. [Google Scholar] [CrossRef]
- Shanahan, D.F.; Cox, D.T.C.; Fuller, R.A.; Hancock, S.; Lin, B.B.; Anderson, K.; Bush, R.; Gaston, K.J. Variation in experiences of nature across a gradient of tree cover in compact and sprawling cities. Landsc. Urban Plan. 2017, 157, 231–238. [Google Scholar] [CrossRef]
- Hanski, I.; von Hertzen, L.; Fyhrquist, N.; Koskinen, K.; Torppa, K.; Laatikainen, T.; Karisola, P.; Auvinen, P.; Paulin, L.; Nakela, M.J.; et al. Environmental biodiversity, human microbiota, and allergy are interrelated. Proc. Natl. Acad. Sci. USA 2012, 109, 8334–8339. [Google Scholar] [CrossRef] [PubMed]
- Bratman, G.N.; Hamilton, J.P.; Hahn, K.S.; Daily, G.C.; Gross, J.J. Nature experience reduces rumination and subgenual prefrontal cortex activation. Proc. Natl. Acad. Sci. USA 2015, 112, 8567–8572. [Google Scholar] [CrossRef] [PubMed]
- Shanahan, D.F.; Fuller, R.A.; Bush, R.; Lin, B.B.; Gaston, K.J. The health benefits of urban nature: How much do we need? BioScience 2015, 65, 476–485. [Google Scholar] [CrossRef]
- Miller, J.R.; Hobbs, R.J. Conservation where people live and work. Conserv. Biol. 2002, 16, 330–337. [Google Scholar] [CrossRef]
- Lachowycz, K.; Jones, A.P. Towards a better understanding of the relationship between greenspace and health: Development of a theoretical framework. Landsc. Urban Plan. 2013, 118, 62–69. [Google Scholar] [CrossRef]
- Pretty, J. How nature contributes to mental and physical health. Spiritual. Health Int. 2004, 5, 68–78. [Google Scholar] [CrossRef]
- Gaston, K.J.; Fuller, R.A.; Loram, A.; MacDonald, C.; Power, S.; Dempsey, N. Urban domestic gardens (XI): Variation in urban wildlife gardening in the United Kingdom. Biodivers. Conserv. 2007, 16, 3227–3238. [Google Scholar] [CrossRef]
- Goddard, M.A.; Dougill, A.J.; Benton, T.G. Scaling up from gardens: Biodiversity conservation in urban environments. Trends Ecol. Evol. 2010, 25, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Gaston, K.J.; Warren, P.H.; Thompson, K.; Smith, R.M. Urban domestic gardens (IV): The extent of the resource and its associated features. Biodivers. Conserv. 2005, 14, 3327–3349. [Google Scholar] [CrossRef]
- Freeman, C.; Dickinson, K.J.M.; Porter, S.; van Heezik, Y. “My garden is an expression of me”: Exploring householders’ relationships with their gardens. J. Environ. Psychol. 2012, 32, 135–143. [Google Scholar] [CrossRef]
- Ulrich, R.S. Aesthetic and affective response to natural environment. In Behavior and the Natural Environment; Altman, I., Wohlwill, J.F., Eds.; Plenum Press: New York, NY, USA, 1983; pp. 85–125. [Google Scholar]
- Kaplan, S. The restorative benefits of nature—Toward an integrated framework. J. Environ. Psychol. 1995, 15, 169–182. [Google Scholar] [CrossRef]
- Berman, M.G.; Jonides, J.; Kaplan, S. The cognitive benefits of interacting with nature. Psychol. Sci. 2008, 19, 1207–1212. [Google Scholar] [CrossRef] [PubMed]
- Hartig, T.; Evans, G.W.; Jamner, L.D.; Davis, D.S.; Garling, T. Tracking restoration in natural and urban field settings. J. Environ. Psychol. 2003, 23, 109–123. [Google Scholar] [CrossRef]
- Barton, J.; Pretty, J. What is the best dose of nature and green exercise for improving mental health? A multi-study analysis. Environ. Sci. Technol. 2010, 44, 3947–3955. [Google Scholar] [CrossRef] [PubMed]
- Jiang, B.; Li, D.; Larsen, L.; Sullivan, W.C. A dose-response curve describing the relationship between urban tree over density and self-reported stress recovery. Environ. Behav. 2016, 48, 607–629. [Google Scholar] [CrossRef]
- Shanahan, D.F.; Lin, B.B.; Bush, R.; Gaston, K.J.; Dean, J.H.; Barber, E.; Fuller, R.A. Toward improved public health outcomes from urban nature. Am. J. Public Health 2015, 105, 470–477. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, W.C.; Frumkin, H.; Jackson, R.J.; Chang, C.Y. Gaia meets Asclepius: Creating healthy places. Landsc. Urban Plan. 2014, 127, 182–184. [Google Scholar] [CrossRef]
- Powell, K.E.; Paluch, A.E.; Blair, S.N. Physical activity for health: What kind? How much? How Intense? On top of what? Annu. Rev. Public Health 2011, 32, 349–365. [Google Scholar] [CrossRef] [PubMed]
- Richardson, E.A.; Pearce, J.; Mitchell, R.; Kingham, S. Role of physical activity in the relationship between urban green space and health. Public Health 2013, 127, 318–324. [Google Scholar] [CrossRef] [PubMed]
- Nisbet, E.K.; Zelenski, J.M.; Murphy, S.A. The nature relatedness scale linking individuals’ connection with nature to environmental concern and behavior. Environ. Behav. 2009, 41, 715–740. [Google Scholar] [CrossRef]
- Shanahan, D.F.; Bush, R.; Gaston, K.J.; Lin, B.B.; Dean, J.; Barber, E.; Fuller, R.A. Health benefits from nature depend on dose. Sci. Rep. 2016. [Google Scholar] [CrossRef] [PubMed]
- Lovibond, S.H.; Lovibond, P.F. Manual for the Depression Anxiety Stress Scales; Psychology Foundation: Sydney, Australia, 1995. [Google Scholar]
- Berman, M.G.; Kross, E.; Krpan, K.M.; Askren, M.K.; Burson, A.; Deldin, P.J.; Kaplan, S.; Sherdell, L.; Gotlib, I.H.; Jonides, J. Interacting with nature improves cognition and affect for individuals with depression. J. Affect. Disord. 2012, 140, 300–305. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, S.V.; Huijts, T.; Avendano, M. Self-reported health assessments in the 2002 World Health Survey: How do they correlate with education? Bull. World Health Organ. 2010, 88, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Idler, E.L.; Benyamini, Y. Self-rated health and mortality: A review of twenty-seven community studies. J. Health Soc. Behav. 1997, 38, 21–37. [Google Scholar] [CrossRef] [PubMed]
- Salmond, J.A.; Tadaki, M.; Vardoulakis, S.; Arbuthnott, K.; Coutts, A.; Demuzere, M.; Dirks, K.N.; Heaviside, C.; Lim, S.; Macintyre, H.; et al. Health and climate related ecosystem services provided by street trees in the urban environment. Environ. Health 2016, 15, 95–111. [Google Scholar] [CrossRef] [PubMed]
- Sampson, R.J.; Raudenbush, S.W.; Earls, F. Neighborhoods and violent crime: A multilevel study of collective efficacy. Science 1997, 277, 918–924. [Google Scholar] [CrossRef] [PubMed]
- Bullen, P.; Onyx, J. Measuring Social Capital in Five Communities in NSW—A Practitioner's Guide; Centre for Australian Community Organisations and Management: Coogee, Australia, 1998. [Google Scholar]
- Sampson, R.J.; Morenoff, J.D.; Earls, F. Reciprocated Exchange. Available online: http://dcyfernetsearch.cehd.umn.edu/sites/default/files/PsychometricsFiles/Sampson−Reciprocated%20Exchange%20(Ages%2018−older).pdf (accessed on 6 June 2015).
- Weinstein, N.; Balmford, A.; Dehaan, C.R.; Gladwell, V.; Bradbury, R.B.; Amano, T. Seeing community for the trees: The links among contact with natural environments, community cohesion, and crime. Bioscience 2015, 65, 1141–1153. [Google Scholar] [CrossRef]
- Start Active, Stay Active: A Report on Physical Activity from the Four Homecountries’ Chief Medical Officers. 2011. Available online: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/216370/dh_128210.pdf. (accessed on 15 January 2016).
- Giles-Corti, B.; Johnson, M.; Knuiman, M.; Donovan, R. Increasing walking—How important is distance to, attractiveness, and size of public open space? Am. J. Prev. Med. 2005, 28, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Feral, C.-H. The connectedness model and optimal development: Is ecopsychology the answer to emotional well-being? Hum. Psychol. 1998, 26, 243–274. [Google Scholar] [CrossRef]
- Martyn, P.; Brymer, E. The relationship between nature relatedness and anxiety. J. Health Psychol. 2014, 21, 1436–1445. [Google Scholar] [CrossRef] [PubMed]
- Capaldi, C.A.; Dopko, R.L.; Zelenski, J.M. The relationship between nature connectedness and happiness: A meta-analysis. Front. Psychol. 2014, 5, 976. [Google Scholar] [CrossRef] [PubMed]
- Zelenski, J.M.; Nisbet, E.K. Happiness and feeling connected: The distinct role of nature relatedness. Environ. Behav. 2014, 46, 3–23. [Google Scholar] [CrossRef]
- Liang, S. Quantitative Remote Sensing of Land Surfaces; Kong, J.A., Ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2004. [Google Scholar]
- Hancock, S.; Disney, M.; Muller, J.-P.; Lewis, P.; Foster, M. A threshold insensitive method for locating the forest canopy top with waveform lidar. Remote Sens. Environ. 2011, 115, 3286–3297. [Google Scholar] [CrossRef]
- Quantum GIS Development Team. Quantum GIS Geographic Information System v2.6. Open Source Geospatial Foundation Project. Available online: http://qgis.osgeo.org (accessed on 8 May 2016).
- R Development Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2016. Available online: http://R−project.org (accessed on 8 May 2016).
- Bartoń, K. MuMIn: Multi-Model Inference. R Package Version 1.13.4. 2015. Available online: http://CRAN.R-project.org/package=MuMIn (accessed on 8 December 2015).
- Richards, S.A. Testing ecological theory using the information-theoretic approach: Examples and cautionary results. Ecology 2005, 86, 2805–2814. [Google Scholar] [CrossRef]
- Burnham, K.P.; Anderson, D.R. Model Selection and Multimodel Inference: A Practical Information-Theoretic Approach; Springer: New York, NY, USA, 2002. [Google Scholar]
- World Health Organization. Global Strategy on Diet, Physical Activity and Health: Physical Inactivity: A Global Public Health Problem. Available online: http://www.who.int/dietphysicalactivity/factsheet_inactivity/en/ (accessed on 18 January 2016).
- Rueckinger, S.; von Kries, R.; Toschke, A.M. An illustration of and programs estimating attributable fractions in large scale surveys considering multiple risk factors. BMC Med. Res. Methodol. 2009. [Google Scholar] [CrossRef] [PubMed]
- Hill, A.B. Environment and disease-association or causation. Proc. R. Soc. Med. 1965, 58, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Das, J.; Do, Q.-T.; Friedman, J.; McKenzie, D.; Scott, K. Mental health and poverty in developing countries: Revisiting the relationship. Soc. Sci. Med. 2007, 65, 467–480. [Google Scholar] [CrossRef] [PubMed]
- Gibala, M.J.; Little, J.P.; van Essen, M.; Wilkin, G.P.; Burgomaster, K.A.; Safdar, A.; Raha, S.; Tarnopolsky, M.A. Short-term sprint interval versus traditional endurance training: Similar initial adaptations in human skeletal muscle and exercise performance. J. Physiol. 2006, 575, 901–911. [Google Scholar] [CrossRef] [PubMed]
- Maas, J.; Verheij, R.A.; Groenewegen, P.P.; de Vries, S.; Spreeuwenberg, P. Green space, urbanity, and health: How strong is the relation? J. Epidemiol. Community Health 2006, 60, 587–592. [Google Scholar] [CrossRef] [PubMed]
- Groenewegen, P.P.; van den Berg, A.E.; Maas, J.; Verheij, R.A.; de Vries, S. Is a green residential environment better for health? If So, why? Ann. Assoc. Am. Geogr. 2012, 102, 996–1003. [Google Scholar] [CrossRef]
- Richardson, E.; Pearce, J.; Mitchell, R.; Day, P.; Kingham, S. The association between green space and cause-specific mortality in urban New Zealand: An ecological analysis of green space utility. BMC Public Health 2010. [Google Scholar] [CrossRef] [PubMed]
- Richardson, E.A.; Mitchell, R.; Hartig, T.; de Vries, S.; Astell-Burt, T.; Frumkin, H. Green cities and health: A question of scale? J. Epidemiol. Community Health 2012, 66, 160–165. [Google Scholar] [CrossRef] [PubMed]
- Kuo, F.E.; Sullivan, W.C.; Coley, R.L.; Brunson, L. Fertile Ground for community: Inner-city neighborhood common spaces. Am. J. Community Psychol. 1998, 26, 823–851. [Google Scholar]
- Sullivan, W.C.; Kuo, F.E.; DePooter, S.F. The fruit of urban nature—Vital neighborhood spaces. Environ. Behav. 2004, 36, 678–700. [Google Scholar] [CrossRef]
- Shanahan, D.F.; Franco, L.; Lin, B.B.; Gaston, K.J.; Fuller, R.A. The benefits of natural environments for physical activity. Sports Med. 2016. [Google Scholar] [CrossRef] [PubMed]
- Restall, B.; Conrad, E. A literature review of connectedness to nature and its potential for environmental management. J. Environ. Manag. 2015, 159, 264–278. [Google Scholar] [CrossRef] [PubMed]
- Harmatz, M.G.; Well, A.D.; Kawamura, K.Y.; Rosal, M.; Ockene, I.S. Seasonal variation of depression and other moods: A longitudinal approach. J. Biol. Rhythm. 2000, 15, 344–350. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variables | Mental Health | Physical Health | Social Health | Physical Behaviour | Nature Relatedness |
|---|---|---|---|---|---|
| Model (i) | R2 = 0.12 | # | R2 = 0.15 | R2 = 0.06 | R2 = 0.14 |
| Intercept | 4.62 (0.90) *** | NA | 3.40 (0.62) *** | −0.76 (0.25) ** | 2.71 (0.09) *** |
| Age | −0.23 (0.03) *** | −0.11 (0.03 ) *** | −0.05 (0.03) * | −0.03 (0.01) ** | 0.05 (0.01) *** |
| Gender_female | −0.16 (0.15) | −0.26 (0.13) * | −0.01 (0.13) | −0.05 (0.04) | 0.10 (0.03) ** |
| Children in home | −0.02 (0.07) | −0.05 (0.06) | 0.06 (0.06) | 0.06 (0.02) ** | 0.01 (0.01) |
| Language at home | 0.27 (0.20) | 0.08 (0.17) | 0.26 (0.17) | −0.07 (0.06) | 0.05 (0.04) |
| Work days per week | −0.08 (0.04) | 0.08 (0.03) * | −0.02 (0.04) | 0.02 (0.01) | −0.02 (0.01) * |
| Income | −0.03 (0.04) | 0.13 (0.03) *** | 0.18 (0.03) *** | 0.02 (0.02) | −0.02 (0.01) ** |
| Frequency of 30-min exercise | −0.02 (0.04) | 0.19 (0.03) *** | 0.11 (0.03) *** | NA | 0.04 (0.01) *** |
| Social cohesion | −0.01 (0.04) | 0.20 (0.03) *** | NA | 0.05 (0.01) *** | 0.04 (0.01) *** |
| Nature relatedness | −0.28 (0.26) | −0.12 (0.14) | 0.73 (0.14) *** | 0.26 (0.05) *** | NA |
| Education (highest qual.) | |||||
| A-level | 0.2 (0.20) | 0.41 (0.16) * | 0.18 (0.17) | −0.11 (0.06) | 0.02 (0.04) |
| Undergraduate | −0.10 (0.25) | 0.47 (0.18) ** | 0.17 (0.18) | −0.04 (0.06) | 0.04 (0.04) |
| Postgraduate | 0.01 (0.25) | 1.05 (0.21) *** | 0.38 (0.21) | −0.09 (0.07) | 0.08 (0.05) |
| Self-assessment health | |||||
| Poor | −1.01 (0.59) | NA | −0.05 (0.44) | −0.04 (0.18) | −0.06 (0.01) |
| Average | −1.66 (0.56) ** | NA | 0.18 (0.40) | −0.04 (0.16) | −0.10 ( 0.10) |
| Good | −2.55 (0.59) *** | NA | 0.81 (0.40) * | 0.29 (0.16) | −0.10 (0.10) |
| Very good | −2.58 (0.57) *** | NA | 1.29 (0.41) ** | 0.44 (0.16) ** | −0.10 (0.10) |
| Relative time outdoors | |||||
| About the same | −0.83 (0.19) *** | −0.07 (0.16) | −0.16 (0.16) | 0.15 (0.06) *** | 0.02 (0.04) |
| More time | −1.15 (0.22) *** | −0.05 (0.18) | −0.22 (0.18) | 0.28 (0.07) *** | 0.11 (0.04) ** |
| Model (ii) | R2 = 0.13 | # | R2 = 0.17 | R2 = 0.06 | R2 = 0.17 |
| Nature exposure frequency exposure | −0.2 (0.05) *** | 0.03 (0.05) | 0.23 (0.05) *** | 0.09 (0.02) *** | 0.07 (0.01) *** |
| Model (iii) | R2 = 0.13 | # | R2 = 0.16 | R2 = 0.06 | R2 = 0.18 |
| Nature exposure duration | −0.06 (0.03) * | 0.01 (0.02) | 0.07 (0.02) ** | 0.03 (0.01) *** | 0.04 (0.01) *** |
| Model (iv) | R2 = 0.17 | # | R2 = 0.15 | R2 = 0.08 | R2 = 0.14 |
| Nature exposure intensity | −0.04 (0.01) ** | 0.01 (0.01) | 0.01 (0.01) | 0.004 (0.003) | 0.004 (0.002) * |
| Variable | Risk Factor | Odds Ratio (95% CI) | Average Population Fraction |
|---|---|---|---|
| Age | Higher risk < 46 years | 2.94 | 0.41 |
| (1.96, 4.41) | |||
| Self-assessment of physical health | Higher risk < average health | 3.64 | 0.07 |
| (2.25, 5.90) | |||
| Relative time outdoors | Higher risk < less time outdoors | 2.51 | 0.08 |
| (1.76, 3.56) | |||
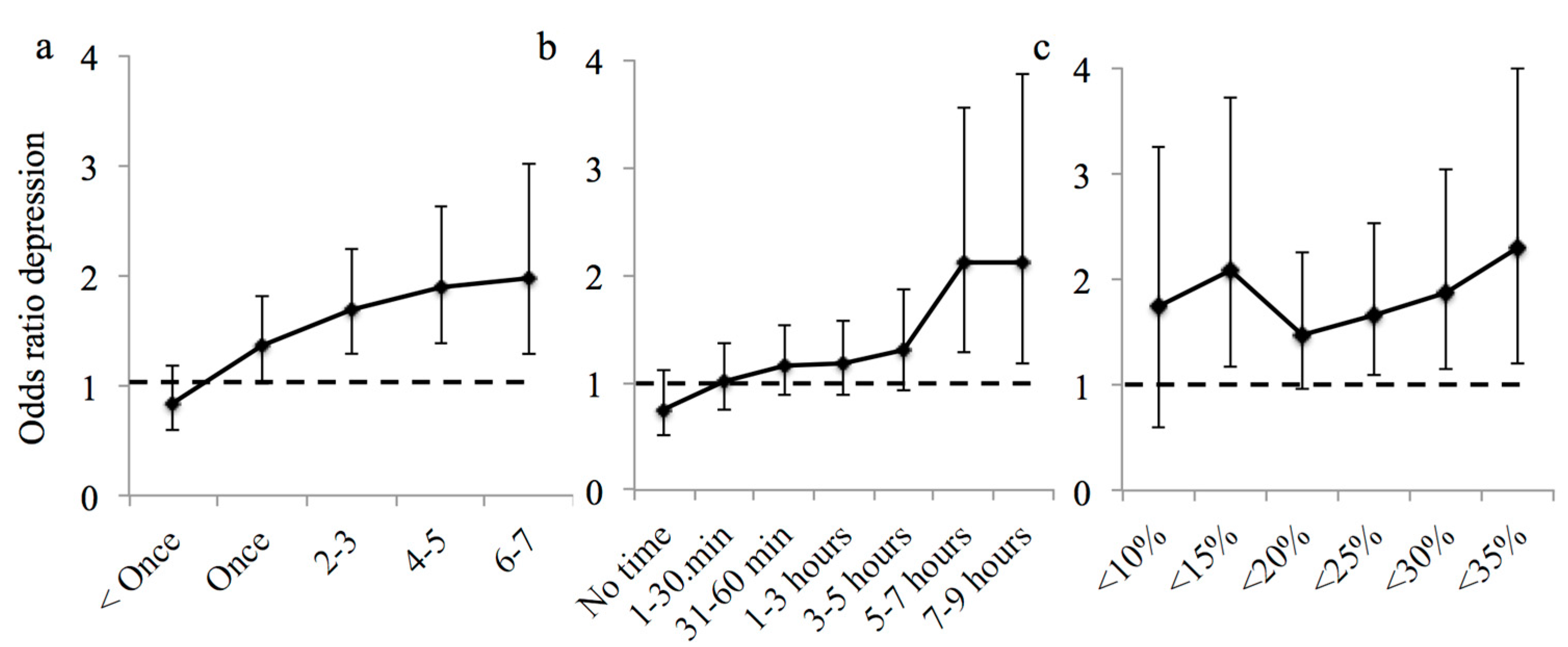
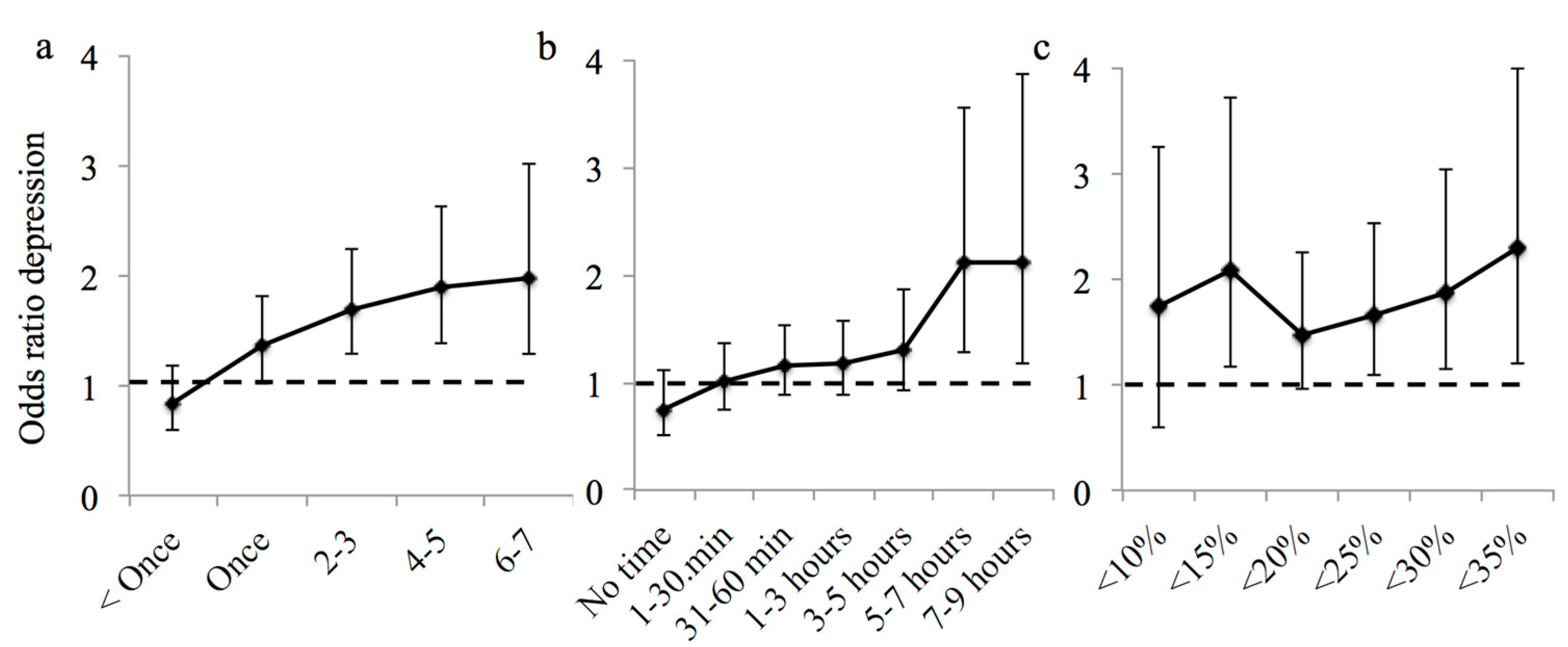
| Frequency of exposure | Higher risk < once per week | 1.36 | 0.05 |
| (1.02, 1.81) | |||
| Duration of exposure | Higher risk < five hours per week | 2.12 | 0.27 |
| (1.27, 3.54) | |||
| Intensity of exposure | High risk < 15% vegetation cover | 2.09 | 0.05 |
| (1.17, 3.72) |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cox, D.T.C.; Shanahan, D.F.; Hudson, H.L.; Fuller, R.A.; Anderson, K.; Hancock, S.; Gaston, K.J. Doses of Nearby Nature Simultaneously Associated with Multiple Health Benefits. Int. J. Environ. Res. Public Health 2017, 14, 172. https://doi.org/10.3390/ijerph14020172
Cox DTC, Shanahan DF, Hudson HL, Fuller RA, Anderson K, Hancock S, Gaston KJ. Doses of Nearby Nature Simultaneously Associated with Multiple Health Benefits. International Journal of Environmental Research and Public Health. 2017; 14(2):172. https://doi.org/10.3390/ijerph14020172
Chicago/Turabian StyleCox, Daniel T. C., Danielle F. Shanahan, Hannah L. Hudson, Richard A. Fuller, Karen Anderson, Steven Hancock, and Kevin J. Gaston. 2017. "Doses of Nearby Nature Simultaneously Associated with Multiple Health Benefits" International Journal of Environmental Research and Public Health 14, no. 2: 172. https://doi.org/10.3390/ijerph14020172
APA StyleCox, D. T. C., Shanahan, D. F., Hudson, H. L., Fuller, R. A., Anderson, K., Hancock, S., & Gaston, K. J. (2017). Doses of Nearby Nature Simultaneously Associated with Multiple Health Benefits. International Journal of Environmental Research and Public Health, 14(2), 172. https://doi.org/10.3390/ijerph14020172