Frequency of Loud Snoring and Metabolic Syndrome among Korean Adults: Results from the Health Examinees (HEXA) Study

 and
and 
Abstract
:1. Introduction
2. Materials and Methods
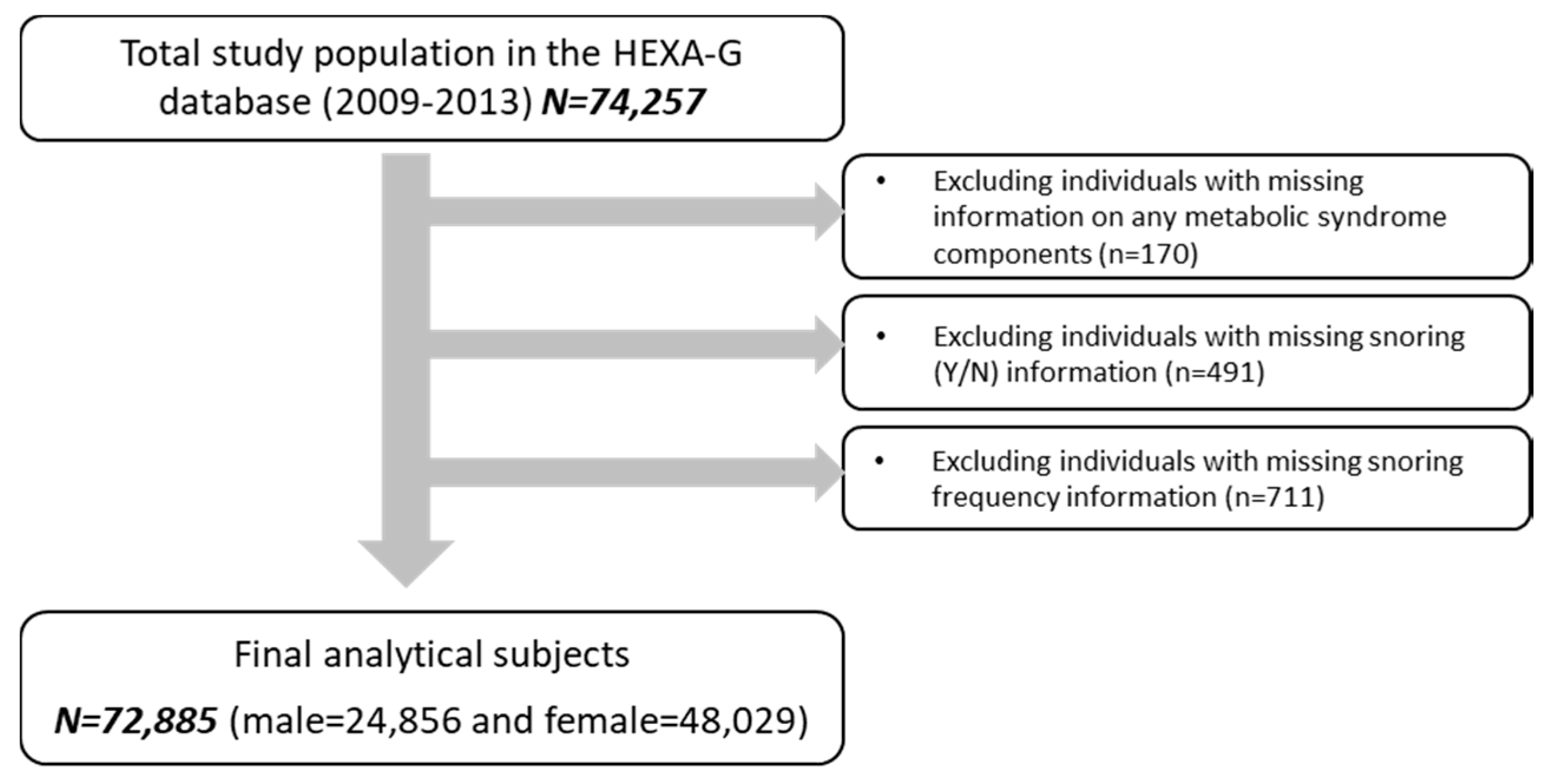
2.1. Study Population
2.2. Assessment of Snoring Frequency and Symptoms
2.3. Definition of Metabolic Syndrome (MetS)
2.4. Covariates
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Pevernagie, D.; Aarts, R.M.; De Meyer, M. The acoustics of snoring. Sleep Med. Rev. 2010, 14, 131–144. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharyya, N. Sleep and Health Implications of Snoring: A Populational Analysis. Laryngoscope 2015, 125, 2413–2416. [Google Scholar] [CrossRef] [PubMed]
- Sands, M.; Loucks, E.B.; Lu, B.; Carskadon, M.A.; Sharkey, K.; Stefanick, M.; Ockene, J.; Shah, N.; Hairston, K.G.; Robinson, J.; et al. Self-reported snoring and risk of cardiovascular disease among postmenopausal women (from the women’s health initiative). Am. J. Cardiol. 2013, 111, 540–546. [Google Scholar] [CrossRef] [PubMed]
- Partinen, M.; Gislason, T. Basic Nordic Sleep Questionnaire (BNSQ): A quantitated measure of subjective sleep complaints. J. Sleep Res. 1995, 4 (Supp. 1), 150–155. [Google Scholar] [CrossRef]
- Fedson, A.C.; Pack, A.I.; Gislason, T. Frequently used sleep questionnaires in epidemiological and genetic research for obstructive sleep apnea: A review. Sleep Med. Rev. 2012, 16, 529–537. [Google Scholar] [CrossRef] [PubMed]
- Xiong, X.; Zhong, A.; Xu, H.; Wang, C. Association between self-reported habitual snoring and diabetes mellitus: A systemic review and meta-analysis. J. Diabetes Res. 2016, 2016, 1958981. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.H.; Wong, B.M.; Tang, J.L.; Ng, D.K. Gender difference in snoring and how it changes with age: Systematic review and meta-regression. Sleep Breath. 2012, 16, 977–986. [Google Scholar] [CrossRef] [PubMed]
- Tsara, V.; Amfilochiou, A.; Papagrigorakis, M.J.; Georgopoulos, D.; Liolios, E. Guidelines for diagnosis and treatment of sleep-related breathing disorders in adults and children. Definition and classification of sleep related breathing disorders in adults: Different types and indications for sleep studies (part 1). Hippokratia 2009, 13, 187–191. [Google Scholar] [PubMed]
- Mbata, G.C.; Chukwuka, J.C. Obstructive Sleep Apnea Hypopnea Syndrome. Ann. Med. Health Sci. Res. 2012, 2, 74–77. [Google Scholar] [CrossRef] [PubMed]
- Niiranen, T.J.; Kronholm, E.; Rissanen, H.; Partinen, M.; Jula, A.M. Self-reported obstructive sleep apnea, simple snoring, and various markers of sleep-disordered breathing as predictors of cardiovascular risk. Sleep Breath. 2016, 20, 589–596. [Google Scholar] [CrossRef] [PubMed]
- Donovan, L.M.; Patel, S.R. Making the most of simplified sleep apnea testing. Ann. Intern. Med. 2017, 166, 366–367. [Google Scholar] [CrossRef] [PubMed]
- Shin, M.H.; Kweon, S.S.; Choi, B.Y.; Kim, M.K.; Chun, B.Y.; Shin, D.H.; Lee, Y.H. Self-reported snoring and metabolic syndrome: The Korean multi-rural communities cohort study. Sleep Breath. 2014, 18, 423–430. [Google Scholar] [CrossRef] [PubMed]
- Sabanayagam, C.; Zhang, R.; Shankar, A. Markers of sleep-disordered breathing and metabolic syndrome in a multiethnic sample of U.S. adults: Results from the national health and nutrition examination survey 2005–2008. Cardiol. Res. Pract. 2012, 2012. [Google Scholar] [CrossRef] [PubMed]
- Leineweber, C.; Kecklund, G.; Akerstedt, T.; Janszky, I.; Orth-Gomer, K. Snoring and the metabolic syndrome in women. Sleep Med. 2003, 4, 531–536. [Google Scholar] [CrossRef]
- Huang, J.; Qi, J.; Lin, Q.; Li, S.; Chen, G.; Ding, H.; Zhao, J. Snoring and components of metabolic syndrome in southeastern Chinese adults: A community-based study. Clin. Respir. J. 2017. [CrossRef] [PubMed]
- Brockmann, P.E.; Damiani, F.; Smith, D.L.; Castet, A.; Nunez, F.; Villarroel, L.; Gozal, D. Metabolic consequences of snoring in adolescents and younger adults: A population study in Chile. Int. J. Obes. 2016, 40, 1510–1514. [Google Scholar] [CrossRef] [PubMed]
- Cho, N.; Joo, S.; Kim, J.; Abbott, R.D.; Kim, J.; Kimm, K.; Shin, C. Relation of habitual snoring with components of metabolic syndrome in Korean adults. Diabetes Res. Clin. Pract. 2006, 71, 256–263. [Google Scholar] [CrossRef] [PubMed]
- Troxel, W.M.; Buysse, D.J.; Matthews, K.A.; Kip, K.E.; Strollo, P.J.; Hall, M.; Drumheller, O.; Reis, S.E. Sleep symptoms predict the development of the metabolic syndrome. Sleep 2010, 33, 1633–1640. [Google Scholar] [CrossRef] [PubMed]
- Tran, B.T.; Jeong, B.Y.; Oh, J.K. The prevalence trend of metabolic syndrome and its components and risk factors in Korean adults: Results from the Korean national health and nutrition examination survey 2008–2013. BMC Public Health 2017, 17, 71. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.; Nagubadi, S.; Kryger, M.H.; Mokhlesi, B. Epidemiology of Obstructive Sleep Apnea: A Population-based Perspective. Expert Rev. Respir. Med. 2008, 2, 349–364. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Han, B.G. Cohort profile: The Korean genome and epidemiology study (KOGES) consortium. Int. J. Epidemiol. 2017, 46, 1350. [Google Scholar] [CrossRef] [PubMed]
- Health Examinees Study Group. The health examinees (HEXA) study: Rationale, study design and baseline characteristics. Asian Pac. J. Cancer Prev. 2015, 16, 1591–1597. [Google Scholar]
- Shin, S.; Lee, H.W.; Kim, C.E.; Lim, J.; Lee, J.K.; Lee, S.A.; Kang, D. Egg consumption and risk of metabolic syndrome in Korean adults: Results from the health examinees study. Nutrients 2017, 9, 687. [Google Scholar] [CrossRef] [PubMed]
- Grundy, S.M.; Cleeman, J.I.; Daniels, S.R.; Donato, K.A.; Eckel, R.H.; Franklin, B.A.; Gordon, D.J.; Krauss, R.M.; Savage, P.J.; Smith, S.C., Jr.; et al. Diagnosis and management of the metabolic syndrome: An American heart association/national heart, lung, and blood institute scientific statement. Circulation 2005, 112, 2735–2752. [Google Scholar] [CrossRef] [PubMed]
- Jordan, A.S.; McEvoy, R.D. Gender differences in sleep apnea: Epidemiology, clinical presentation and pathogenic mechanisms. Sleep Med. Rev. 2003, 7, 377–389. [Google Scholar] [CrossRef] [PubMed]
- Bixler, E.O.; Vgontzas, A.N.; Lin, H.M.; Ten Have, T.; Rein, J.; Vela-Bueno, A.; Kales, A. Prevalence of sleep-disordered breathing in women: Effects of gender. Am. J. Respir. Crit. Care Med. 2001, 163, 608–613. [Google Scholar] [CrossRef] [PubMed]
- De Sousa, A.G.; Cercato, C.; Mancini, M.C.; Halpern, A. Obesity and obstructive sleep apnea-hypopnea syndrome. Obes. Rev. 2008, 9, 340–354. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Pan, A.; Yu, Z.; Li, H.; Shi, A.; Yu, D.; Zhang, G.; Zong, G.; Liu, Y.; Lin, X. Snoring, inflammatory markers, adipokines, and metabolic syndrome in apparently healthy Chinese. PLoS ONE 2011, 6, e27515. [Google Scholar] [CrossRef] [PubMed]
- Krol, R.C.; Knuth, S.L.; Bartlett, D., Jr. Selective reduction of genioglossal muscle activity by alcohol in normal human subjects. Am. Rev. Respir. Dis. 1984, 129, 247–250. [Google Scholar] [PubMed]
- Li, D.; Liu, D.; Wang, X.; He, D. Self-reported habitual snoring and risk of cardiovascular disease and all-cause mortality. Atherosclerosis 2014, 235, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Endeshaw, Y.; Rice, T.B.; Schwartz, A.V.; Stone, K.L.; Manini, T.M.; Satterfield, S.; Cummings, S.; Harris, T.; Pahor, M.; Health, A.B.C.S. Snoring, daytime sleepiness, and incident cardiovascular disease in the health, aging, and body composition study. Sleep 2013, 36, 1737–1745. [Google Scholar] [CrossRef] [PubMed]
- Marshall, N.S.; Wong, K.K.; Cullen, S.R.; Knuiman, M.W.; Grunstein, R.R. Snoring is not associated with all-cause mortality, incident cardiovascular disease, or stroke in the Busselton health study. Sleep 2012, 35, 1235–1240. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.A.; Amis, T.C.; Byth, K.; Larcos, G.; Kairaitis, K.; Robinson, T.D.; Wheatley, J.R. Heavy snoring as a cause of carotid artery atherosclerosis. Sleep 2008, 31, 1207–1213. [Google Scholar] [PubMed]
- Rich, J.; Raviv, A.; Raviv, N.; Brietzke, S.E. An epidemiologic study of snoring and all-cause mortality. Otolaryngol. Head Neck Surg. 2011, 145, 341–346. [Google Scholar] [CrossRef] [PubMed]
- Rapoport, D.M. Snoring-obnoxious (but medically innocent) noise or wakeup call for sleep medicine? Sleep Med. Rev. 2014, 18, 451–452. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, E.C. Sympathetic over activity in the etiology of hypertension of obstructive sleep apnea. Sleep 2003, 26, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Iiyori, N.; Alonso, L.C.; Li, J.; Sanders, M.H.; Garcia-Ocana, A.; O’Doherty, R.M.; Polotsky, V.Y.; O’Donnell, C.P. Intermittent hypoxia causes insulin resistance in lean mice independent of autonomic activity. Am. J. Respir. Crit. Care Med. 2007, 175, 851–857. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, A.R.; Rubinos, C.G.; Alonso, A.R.; Cascon, H.J.A.; Palomo, A.B.; Iscar, U.M.; Casan, C.P. Snoring as a determinant factor of oxidative stress in the airway of patients with obstructive sleep apnea. Lung 2016, 194, 469–473. [Google Scholar] [CrossRef] [PubMed]
- Shin, C.; Kim, J.; Kim, J.; Lee, S.; Shim, J.; In, K.; Kang, K.; Yoo, S.; Cho, N.; Kimm, K.; et al. Association of habitual snoring with glucose and insulin metabolism in nonobese Korean adult men. Am. J. Respir. Crit. Care Med. 2005, 171, 287–291. [Google Scholar] [CrossRef] [PubMed]
- Facco, F.L.; Grobman, W.A.; Kramer, J.; Ho, K.H.; Zee, P.C. Self-reported short sleep duration and frequent snoring in pregnancy: Impact on glucose metabolism. Am. J. Obstet. Gynecol. 2010, 203, 142.e1–142.e5. [Google Scholar] [CrossRef] [PubMed]
- Marchesini, G.; Pontiroli, A.; Salvioli, G.; Novi, R.F.; Vitacolonna, E.; Taboga, C.; Ciccarone, A.M.; Grossi, E.; Group, Q.S. Snoring, hypertension and type 2 diabetes in obesity. Protection by physical activity. J Endocrinol. Investig. 2004, 27, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Ozol, D.; Carlioglu, A.; Karamanli, H.; Akgedik, R.; Karakurt, F.; Yildirim, Z. Influence of snoring on microalbuminuria in diabetic patients. Sleep Breath. 2011, 15, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Joo, S.; Lee, S.; Choi, H.A.; Kim, J.; Kim, E.; Kimm, K.; Kim, J.; Shin, C. Habitual snoring is associated with elevated hemoglobin a1c levels in non-obese middle-aged adults. J. Sleep Res. 2006, 15, 437–444. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.H.; Kuo, S.W.; Wu, D.A. Relationships between hemoglobin and each component of metabolic syndrome: A special focus on elderly without medication. Int. J. Gerontol. 2016, 10, 22–27. [Google Scholar] [CrossRef]


{kind=link}
| Snoring Frequency | |||||||
|---|---|---|---|---|---|---|---|
| Total | Never | 1–3/month | 1–3/week | 4–5/week | 6+/week | p-Value b | |
| Men, n | 24856 | 9555 (38.4) | 4857 (19.5) | 5190 (20.9) | 1634 (6.6) | 3620 (14.6) | |
| Age, years | 53.8 ± 8.5 | 53.6 ± 8.8 | 53.7 ± 8.4 | 53.5 ± 8.2 | 54.9 ± 8.1 | 53.9 ± 8.4 | <0.0001 |
| BMI, kg/m2 | 24.4 ± 2.8 | 23.7 ± 2.6 | 24.4 ± 2.6 | 24.8 ± 2.7 | 25.1 ± 2.8 | 25.5 ± 2.9 | <0.0001 |
| Current smokers | 18642 (75.0) | 6916 (72.4) | 3573 (73.6) | 4069 (78.4) | 1274 (78.0) | 2810 (77.6) | <0.0001 |
| Current drinkers | 18219 (73.3) | 6651 (69.6) | 3577 (73.7) | 4061 (78.3) | 1245 (76.2) | 2685 (74.2) | <0.0001 |
| Regular exercisers | 14407 (58.0) | 5398 (56.5) | 2939 (60.5) | 3127 (60.3) | 910 (55.7) | 2033 (56.2) | <0.0001 |
| College or above | 9316 (37.5) | 3540 (37.1) | 1878 (38.7) | 1999 (38.5) | 572 (35.0) | 1327 (36.7) | 0.0276 |
| Manual occupation | 11,964 (48.1) | 4571 (47.8) | 2360 (48.6) | 2473 (47.7) | 777 (47.6) | 1783 (49.3) | 0.0701 |
| Married | 23,180 (93.3) | 8686 (90.9) | 4585 (94.4) | 4934 (95.1) | 1551 (94.9) | 3424 (94.6) | <0.0001 |
| Sleep duration, hours | 6.9 ± 1.2 | 6.9 ± 1.2 | 6.9 ± 1.1 | 6.9 ± 1.1 | 6.9 ± 1.1 | 6.9 ± 1.2 | 0.0091 |
| Women, n | 48,029 | 25,590 (53.3) | 10,420 (21.7) | 6736 (14.0) | 1779 (3.7) | 3504 (7.3) | |
| Age, years | 52.6 ± 7.8 | 51.5 ± 7.9 | 53.0 ± 7.5 | 54.2 ± 7.5 | 54.7 ± 7.4 | 55.1 ± 7.4 | <0.0001 |
| BMI, kg/m2 | 23.6 ± 3.0 | 23.0 ± 2.7 | 23.8 ± 2.9 | 24.3 ± 3.1 | 24.7 ± 3.3 | 25.3 ± 3.3 | <0.0001 |
| Current smokers | 1875 (3.9) | 942 (3.7) | 380 (3.7) | 288 (4.3) | 76 (4.3) | 189 (5.4) | <0.0001 |
| Current drinkers | 15,522 (32.3) | 8229 (32.2) | 3437 (33.0) | 2224 (33.0) | 558 (31.4) | 1074 (30.7) | 0.0676 |
| Regular exercisers | 24,826 (51.7) | 13,026 (50.9) | 5691 (54.6) | 3489 (51.8) | 886 (49.8) | 1734 (49.5) | <0.0001 |
| College or above | 10,065 (21.0) | 6197 (24.2) | 2031 (19.5) | 1109 (16.5) | 267 (15.0) | 461 (13.2) | <0.0001 |
| Manual occupation | 13,046 (27.2) | 6706 (26.2) | 2787 (26.8) | 1948 (28.9) | 533 (30.0) | 1072 (30.6) | <0.0001 |
| Married | 41,688 (86.8) | 22,112 (86.4) | 9205 (88.3) | 5861 (87.0) | 1539 (86.5) | 2971 (84.8) | <0.0001 |
| Post-menopausal | 28,239 (58.8) | 13,504 (52.8) | 6455 (62.0) | 4551 (67.6) | 1243 (69.9) | 2486 (71.0) | <0.0001 |
| Sleep duration, hours | 6.9 ± 1.2 | 6.9 ± 1.2 | 6.9 ± 1.2 | 6.9 ± 1.2 | 6.9 ± 1.2 | 6.9 ± 1.3 | 0.0079 |
| Snoring Frequency | |||||||
|---|---|---|---|---|---|---|---|
| Total | Never | 1–3/month | 1–3/week | 4–5/week | 6+/week | p-Value c | |
| Men, n | 24,856 | 9555 | 4857 | 5190 | 1634 | 3620 | |
| MetS | 7276 (29.3) | 2216 (23.2) | 1355 (27.9) | 1709 (32.9) | 598 (36.6) | 1398 (38.6) | <0.0001 |
| WC ≥ 90 cm | 6911 (27.8) | 1990 (20.8) | 1305 (26.9) | 1603 (30.9) | 546 (33.4) | 1467 (40.5) | <0.0001 |
| Serum TG ≥ 150 mg/dL | 10,077 (40.5) | 3428 (35.9) | 1923 (39.6) | 2299 (44.3) | 729 (44.6) | 1698 (46.9) | <0.0001 |
| Serum HDL-C ≤ 40 mg/dL | 5793 (23.3) | 2011 (21.1) | 1101 (22.7) | 1207 (23.3) | 429 (26.3) | 1045 (28.9) | <0.0001 |
| BP ≥ 130/85 mmHg | 13,323 (53.6) | 4613 (48.3) | 2582 (53.2) | 2982 (57.5) | 990 (60.6) | 2156 (59.6) | <0.0001 |
| Fasting glucose ≥ 100 mg/dL | 8517 (34.3) | 2998 (31.4) | 1648 (33.9) | 1879 (36.2) | 637 (39.0) | 1355 (37.4) | <0.0001 |
| Women, n | 48,029 | 25,590 | 104,20 | 6736 | 1779 | 3504 | |
| MetS | 11,980 (24.9) | 4874 (19.1) | 2796 (26.8) | 2205 (32.7) | 657 (36.9) | 1448 (41.3) | <0.0001 |
| WC ≥ 80 cm | 19,121 (39.8) | 8172 (31.9) | 4538 (43.6) | 3313 (49.2) | 934 (52.5) | 2164 (61.8) | <0.0001 |
| Serum TG ≥ 150 mg/dL | 11,730 (24.4) | 5288 (20.7) | 2656 (25.5) | 2020 (30.0) | 567 (31.9) | 1199 (34.2) | <0.0001 |
| Serum HDL-C ≤ 50 mg/dL | 17,047 (35.5) | 8206 (32.1) | 3872 (37.2) | 2637 (39.2) | 740 (41.6) | 1592 (45.4) | <0.0001 |
| BP ≥ 130/85 mmHg | 18,380 (38.3) | 8249 (32.2) | 4280 (41.1) | 3148 (46.7) | 882 (49.6) | 1821 (52.0) | <0.0001 |
| Fasting glucose ≥ 100 mg/dL | 9330 (19.4) | 4127 (16.1) | 2128 (20.4) | 1602 (23.8) | 474 (26.6) | 999 (28.5) | <0.0001 |
| Snoring Frequency | ||||||
|---|---|---|---|---|---|---|
| Never | 1–3/month | 1–3/week | 4–5/week | 6+/week | p-Trend c | |
| Men n = 24,856 d | 9555 | 4857 | 5190 | 1634 | 3620 | |
| MetS | Ref. | 1.29 (1.19–1.40) | 1.63 (1.51–1.75) | 1.85 (1.65–2.07) | 2.07 (1.91–2.25) | <0.0001 |
| WC ≥ 90 cm | Ref. | 1.40 (1.29–1.52) | 1.69 (1.57–1.83) | 1.86 (1.66–2.09) | 2.57 (2.37–2.79) | <0.0001 |
| Serum TG ≥ 150 mg/dL | Ref. | 1.18 (1.09–1.26) | 1.39 (1.30–1.49) | 1.44 (1.29–1.60) | 1.56 (1.45–1.69) | <0.0001 |
| Serum HDL-C ≤ 40 mg/dL | Ref. | 1.04 (0.95–1.13) | 1.04 (0.96–1.13) | 1.12 (0.99–1.27) | 1.22 (1.11–1.34) | <0.0001 |
| BP ≥ 130/85 mmHg | Ref. | 1.21 (1.13–1.30) | 1.44 (1.35–1.55) | 1.57 (1.41–1.75) | 1.57 (1.45–1.70) | <0.0001 |
| Fasting glucose ≥ 100 mg/dL | Ref. | 1.12 (1.04–1.21) | 1.23 (1.14–1.32) | 1.32 (1.19–1.48) | 1.29 (1.19–1.40) | <0.0001 |
| Women n = 48,029 d | 25,590 | 10,420 | 6736 | 1779 | 3504 | |
| MetS | Ref. | 1.22 (1.15–1.29) | 1.34 (1.25–1.44) | 1.40 (1.25–1.57) | 1.45 (1.33–1.58) | <0.0001 |
| WC ≥ 80 cm | Ref. | 1.55 (1.48–1.63) | 1.81 (1.71–1.92) | 1.98 (1.79–2.19) | 2.87 (2.66–3.09) | <0.0001 |
| Serum TG ≥ 150 mg/dL | Ref. | 1.12 (1.06–1.18) | 1.25 (1.17–1.33) | 1.25 (1.12–1.39) | 1.27 (1.17–1.38) | <0.0001 |
| Serum HDL-C ≤ 50 mg/dL | Ref. | 1.10 (1.05–1.16) | 1.09 (1.02–1.15) | 1.11 (1.00–1.23) | 1.21 (1.12–1.30) | <0.0001 |
| BP ≥ 130/85 mmHg | Ref. | 1.21 (1.15–1.27) | 1.31 (1.24–1.39) | 1.34 (1.20–1.48) | 1.32 (1.22–1.43) | <0.0001 |
| Fasting glucose ≥ 100 mg/dL | Ref. | 1.13 (1.07–1.21) | 1.23 (1.14–1.31) | 1.32 (1.18–1.48) | 1.33 (1.22–1.45) | <0.0001 |
| Presence of Breathing Interruptions | ||
| Men (n = 4062) | Women c (n = 1596) | |
| MetS | 1.58 (1.47–1.70) | 1.32 (1.18–1.49) |
| WC ≥ 90 cm (M)/≥80 cm (W) | 1.72 (1.60–1.84) | 1.06 (0.92–1.21) |
| Serum TG ≥ 150 mg/dL | 1.28 (1.19–1.37) | 1.28 (1.15–1.43) |
| Serum HDL-C ≤ 40 mg/dL (M)/≤50 mg/dL (W) | 1.07 (0.99–1.16) | 1.18 (1.06–1.31) |
| BP ≥ 130/85 mmHg | 1.40 (1.31–1.51) | 1.30 (1.17–1.45) |
| Fasting glucose ≥ 100 mg/dL | 1.22 (1.13–1.31) | 1.26 (1.12–1.41) |
| Presence of Awakenings | ||
| Men (n = 2999) | Women c (n = 6226) | |
| MetS | 1.39 (1.28–1.50) | 1.21 (1.13–1.29) |
| WC ≥ 90 cm (M)/≥80 cm (W) | 1.48 (1.37–1.61) | 0.99 (0.90–1.07) |
| Serum TG ≥ 150 mg/dL | 1.24 (1.15–1.34) | 1.17 (1.10–1.25) |
| Serum HDL-C ≤ 40 mg/dL (M)/≤50 mg/dL (W) | 0.99 (0.91–1.09) | 1.08 (1.00–1.15) |
| BP ≥ 130/85 mmHg | 1.28 (1.18–1.38) | 1.19 (1.10–1.26) |
| Fasting glucose ≥ 100 mg/dL | 1.16 (1.07–1.25) | 1.18 (1.10–1.26) |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, C.E.; Shin, S.; Lee, H.-W.; Lim, J.; Lee, J.-K.; Kang, D. Frequency of Loud Snoring and Metabolic Syndrome among Korean Adults: Results from the Health Examinees (HEXA) Study. Int. J. Environ. Res. Public Health 2017, 14, 1294. https://doi.org/10.3390/ijerph14111294
Kim CE, Shin S, Lee H-W, Lim J, Lee J-K, Kang D. Frequency of Loud Snoring and Metabolic Syndrome among Korean Adults: Results from the Health Examinees (HEXA) Study. International Journal of Environmental Research and Public Health. 2017; 14(11):1294. https://doi.org/10.3390/ijerph14111294
Chicago/Turabian StyleKim, Claire E., Sangah Shin, Hwi-Won Lee, Jiyeon Lim, Jong-Koo Lee, and Daehee Kang. 2017. "Frequency of Loud Snoring and Metabolic Syndrome among Korean Adults: Results from the Health Examinees (HEXA) Study" International Journal of Environmental Research and Public Health 14, no. 11: 1294. https://doi.org/10.3390/ijerph14111294
APA StyleKim, C. E., Shin, S., Lee, H.-W., Lim, J., Lee, J.-K., & Kang, D. (2017). Frequency of Loud Snoring and Metabolic Syndrome among Korean Adults: Results from the Health Examinees (HEXA) Study. International Journal of Environmental Research and Public Health, 14(11), 1294. https://doi.org/10.3390/ijerph14111294