Job Satisfaction among Health-Care Staff in Township Health Centers in Rural China: Results from a Latent Class Analysis

Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Descriptive Analysis
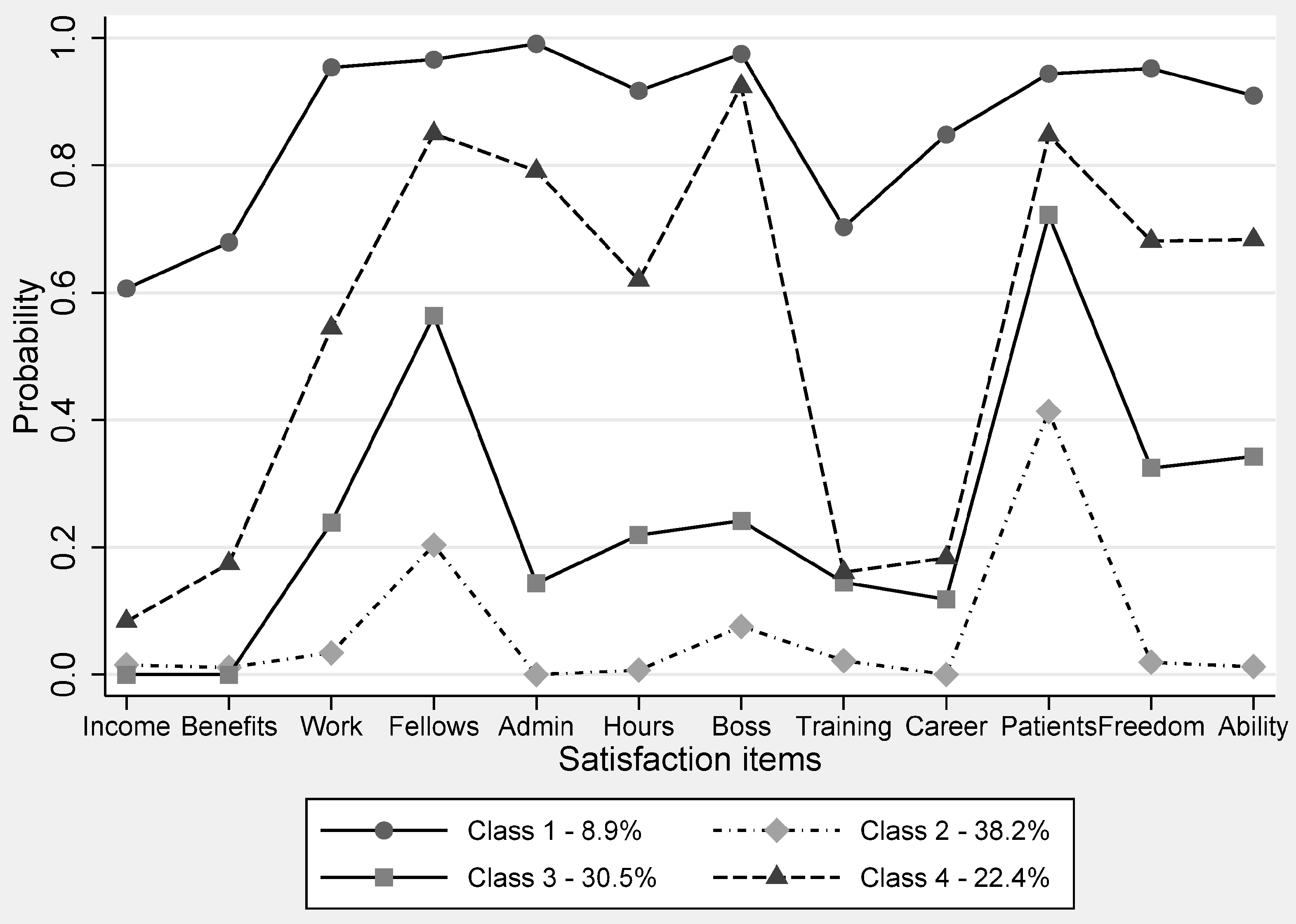
3.2. LCA (Latent Class Analysis) Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- 2014 Year Book of Health in the People’s Republic of China. Available online: http://tongji.cnki.net/kns55/navi/YearBook.aspx?id=N2014120147&floor=1 (accessed on 15 April 2017).
- Monitoring the Geographical Distribution of the Health Workforce in Rural and Underserved Areas. Available online: http://who.int/hrh/statistics/spotlight_8_en.pdf (accessed on 15 April 2017).
- Narasimhan, V.; Brown, H.; Pablosmendez, A.; Adams, O.; Dussault, G.; Elzinga, G.; Elzinga, G.; Nordstrom, A.; Habte, D.; Jacobs, M.; et al. Responding to the global human resources crisis. Lancet 2004, 363, 1469–1472. [Google Scholar] [CrossRef]
- Hotchkiss, D.R.; Banteyerga, H.; Tharaney, M. Job satisfaction and motivation among public sector health workers: Evidence from Ethiopia. Hum. Resour. Health 2015, 13, 83–94. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.; Song, K.; Rane, S.; Sun, X.; Li, H.; Meng, Q. Factors associated with job satisfaction by Chinese primary care providers. Prim. Health Care Res. Dev. 2014, 15, 46–57. [Google Scholar] [CrossRef] [PubMed]
- Locke, E.A. The nature and causes of job satisfaction. In Handbook of Industrial and Organizational Psychology; Dunnette, M.D., Ed.; Rand McNally: Chicago, IL, USA, 1976; pp. 1297–1349. [Google Scholar]
- Locke, E.A.; Latham, G.P. Work motivation and satisfaction: Light at the end of the tunnel. Psychol. Sci. 1990, 1, 240–246. [Google Scholar] [CrossRef]
- Büssing, A.; Bissels, T.; Fuchs, V.; Perrar, K.-M. A dynamic model of work satisfaction: Qualitative approaches. Hum. Relat. 1999, 52, 999–1028. [Google Scholar] [CrossRef]
- Edwards, J.E. Employee attitudes and job satisfaction. Hum. Resour. Manag. 2004, 43, 395–407. [Google Scholar]
- Peters, D.H.; Chakraborty, S.; Mahapatra, P.K.; Steinhardt, L. Job satisfaction and motivation of health workers in public and private sectors: Cross-sectional analysis from two Indian states. Hum. Resour. Health 2010, 8, 27–37. [Google Scholar] [CrossRef] [PubMed]
- Büssing, A.; Bissels, T. Different forms of work satisfaction. Eur. Psychol. 1998, 3, 209–218. [Google Scholar] [CrossRef]
- Hardigan, P.C.; Sangasubana, N. A latent class analysis of job satisfaction and turnover among practicing pharmacists. Res. Soc. Adm. Pharm. 2010, 6, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Franco, L.M.; Bennett, S.; Kanfer, R. Health sector reform and public sector health worker motivation: A conceptual framework. Soc. Sci. Med. 2002, 54, 1255–1266. [Google Scholar] [CrossRef]
- Jadoo, S.A.; Aljunid, S.M.; Dastan, I.; Tawfeeq, R.S.; Mustafa, M.; Ganasegeran, K.; AlDubai, S.A.R. Job satisfaction and turnover intention among Iraqi doctors—A descriptive cross-sectional multicentre study. Hum. Resour. Health 2015, 13, 21–31. [Google Scholar] [CrossRef] [PubMed]
- Jiménez, P.; Dunkl, A.; Stolz, R. Anticipation of the development of job satisfaction—Construct and validation results of an indicator for well-being at the workplace. Psychology 2015, 6, 856–866. [Google Scholar] [CrossRef]
- Judge, T.A.; Thoresen, C.J.; Bono, J.E. The job satisfaction-job performance relationship: A qualitative and quantitative review. Psychol. Bull. 2001, 127, 376–407. [Google Scholar] [CrossRef] [PubMed]
- Hochwarter, W.A.; Perrewe, P.L.; Ferris, G.R. Job satisfaction and performance: The moderating effects of value attainment and affective disposition. J. Vocat. Behav. 1999, 54, 296–313. [Google Scholar] [CrossRef]
- London, M. Book review: Job satisfaction: How people feel about their jobs and how it affects their performance. J. Manag. 1992, 18, 810–811. [Google Scholar] [CrossRef]
- Jiménez, P.; Milfelner, B.; ŠarotarŽižek, S.; Dunkl, A. Moderating effects between job insecurity and intention to quit in samples of Slovene and Austrian workers. J. Contemp. Issue. Econ. Business 2017, 63, 27–37. [Google Scholar] [CrossRef]
- Lum, L.; Kervin, J.; Clark, K.; Reid, F.; Sirola, W. Explaining nursing turnover intent: Job satisfaction, pay satisfaction, or organizational commitment? J. Organ. Behav. 1998, 19, 305–320. [Google Scholar] [CrossRef]
- Tett, R.P.; Meyer, J.P. Job satisfaction, organizational commitment, turnover intention, and turnover: Path analyses based on meta-analytic findings. Pers. Psychol. 1993, 46, 259–293. [Google Scholar] [CrossRef]
- Mpembeni, R.; Bhatnagar, A.; Lefevre, A.; Chitama, D.; Urassa, D.P.; Kilewo, C.; Mdee, R.M.; Semu, H.; Winch, P.J.; Killewo, J.; et al. Motivation and satisfaction among community health workers in Morogoro Region, Tanzania: Nuanced needs and varied ambitions. Hum. Resour. Health 2015, 13, 44–53. [Google Scholar] [CrossRef] [PubMed]
- Landon, B.E. Career satisfaction among physicians. JAMA 2004, 291, 634. [Google Scholar] [CrossRef] [PubMed]
- Scheurer, D.; Mckean, S.C.; Miller, J.A.; Wetterneck, T.B. U.S. physician satisfaction: A systematic review. J. Hosp. Med. 2009, 4, 560–568. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Hu, H.; Zhou, H.; He, C.; Fan, L.; Liu, X.; Zhang, Z.; Li, H.; Sun, T. Work stress, work motivation and their effects on job satisfaction in community health workers: A cross-sectional survey in China. BMJ Open 2014, 4, e004897. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Tao, H.; Ellenbecker, C.H.; Liu, X. Job satisfaction, occupational commitment and intent to stay among Chinese nurses: A cross-sectional questionnaire survey. J. Adv. Nurs. 2012, 68, 539–549. [Google Scholar] [CrossRef] [PubMed]
- Joyce, C.M.; Schurer, S.; Scott, A.; Humphreys, J.S.; Kalb, G. Australian doctors’ satisfaction with their work: Results from the MABEL longitudinal survey of doctors. Med. J. Aust. 2011, 194, 30–33. [Google Scholar] [PubMed]
- Warr, P.; Cook, J.; Wall, T. Scales for the measurement of some work attitudes and aspects of psychological well-being. J. Occup. Psychol. 1979, 52, 129–148. [Google Scholar] [CrossRef]
- Yesilyaprak, B.; Boysan, M. Latent class analysis of job and life satisfaction among school counselors: A national survey. J. Happiness Stud. 2015, 16, 1–15. [Google Scholar] [CrossRef]
- Vermunt, J.K. Latent class modeling with covariates: Two improved three-step approaches. Polit. Anal. 2010, 18, 450–469. [Google Scholar] [CrossRef]
- Joyce, C.M.; Wang, W.C. Job satisfaction among Australian doctors: The use of latent class analysis. J. Health Serv. Res. Policy 2015, 20, 224–230. [Google Scholar] [CrossRef] [PubMed]
- Hung, L.; Shi, L.; Wang, H.; Nie, X.; Meng, Q. Chinese primary care providers and motivating factors on performance. Fam. Pract. 2013, 30, 576–586. [Google Scholar] [CrossRef] [PubMed]
- Lu, L.; Dai, T.; Ma, X.; Yang, X. Effects of pay for performance program on the income of health professional in township health center. Med. Soc. 2013, 26, 1–4. [Google Scholar]
- Nojima, Y.; Kumakura, S.; Onoda, K.; Hamano, T.; Kimura, K. Job and life satisfaction and preference of future practice locations of physicians on remote islands in Japan. Hum. Resour. Health 2015, 13, 39–49. [Google Scholar] [CrossRef] [PubMed]
- Fang, P.; Luo, Z.; Fang, Z. What is the job satisfaction and active participation of medical staff in public hospital reform: A study in Hubei province of China. Hum. Resour. Health 2015, 13, 34–47. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Dimension | Items | Definition |
|---|---|---|
| Extrinsic factors | Income | Wage or salary |
| Benefits | Benefits and allowances beyond income | |
| Work | Physical working conditions | |
| Fellows | Relationship with colleagues and fellow workers | |
| Administration | Management level within the township health centers (THCs) | |
| Hours | Assigned hours of work | |
| Boss | Immediate boss | |
| Intrinsic factors | Training | On-the-job training |
| Career | Professional development | |
| Patients | Recognition for work from patients | |
| Freedom | Freedom to choose methods of working | |
| Ability | Opportunity to use abilities |
| Variables | All (n = 603) |
|---|---|
| Gender | |
| Male, n (%) | 218 (36.15) |
| Female, n (%) | 385 (63.85) |
| Age, mean (SD) | 36.5 (8.40) |
| Marriage status | |
| Single, n (%) | 67 (11.11) |
| Living with a partner, n (%) | 536 (88.89) |
| Importance of training within the THC, mean (SD) | 1.82 (0.91) |
| Weekly working hours, mean (SD) | 53.75 (20.08) |
| Type of providers | |
| PHP, n (%) | 186 (30.85) |
| Non-PHP, n (%) | 417 (69.15) |
| Income inequality within the THC, mean (SD) | 2.83 (0.99) |
| Permanent job | |
| Yes, n (%) | 476 (78.94) |
| No, n (%) | 127 (21.06) |
| Length of working experience, mean (SD) | 14.66 (8.59) |
| Urban residence in childhood | |
| Yes, n (%) | 157 (26.04) |
| No, n (%) | 446 (73.96) |
| Intention to leave the current job, mean (SD) | 2.86 (1.13) |
| Job satisfaction items in binary | |
| Income, n (%) | 66 (10.95) |
| Benefits, n (%) | 80 (13.27) |
| Work, n (%) | 198 (32.84) |
| Fellows, n (%) | 332 (55.06) |
| Administration, n (%) | 213 (35.32) |
| Hours, n (%) | 198 (32.84) |
| Boss, n (%) | 262 (43.45) |
| Training, n (%) | 110 (18.24) |
| Career, n (%) | 115 (19.07) |
| Patients, n (%) | 413 (68.49) |
| Freedom, n (%) | 223 (36.98) |
| Ability, n (%) | 230 (38.14) |
| 1 | 2 | 3 | 4 | |
|---|---|---|---|---|
| 1 | 0.948 | 0.000 | 0.000 | 0.052 |
| 2 | 0.000 | 0.897 | 0.102 | 0.000 |
| 3 | 0.000 | 0.085 | 0.842 | 0.072 |
| 4 | 0.019 | 0.000 | 0.072 | 0.909 |
| Characteristics/Attitudes | Class 2 | Class 3 | Class 4 | |||
|---|---|---|---|---|---|---|
| Coefficients | S.E. | Coefficients | S.E. | Coefficients | S.E. | |
| Gender | −0.124 | 0.468 | −0.337 | 0.471 | −0.705 | 0.469 |
| Marriage status | 1.506 ** | 0.690 | 1.408 ** | 0.673 | 1.405 ** | 0.708 |
| Urban background | 0.237 | 0.553 | 0.261 | 0.557 | 0.476 | 0.566 |
| Weekly working hours | 0.005 | 0.019 | 0.016 | 0.017 | 0.002 | 0.017 |
| Specialty | 0.795 *** | 0.231 | 0.568 ** | 0.222 | 0.414 * | 0.225 |
| Permanent job | −0.240 | 0.752 | −0.727 | 0.731 | −1.004 | 0.736 |
| Length of working experience | −0.006 | 0.157 | −0.068 | 0.156 | −0.098 | 0.154 |
| Appropriateness of compensation structure within the THC | −2.740 *** | 0.387 | −2.234 *** | 0.401 | −1.403 *** | 0.403 |
| Higher importance of training within the THC | 1.169 *** | 0.237 | 0.909 *** | 0.235 | 0.566 *** | 0.223 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, H.; Tang, C.; Zhao, S.; Meng, Q.; Liu, X. Job Satisfaction among Health-Care Staff in Township Health Centers in Rural China: Results from a Latent Class Analysis. Int. J. Environ. Res. Public Health 2017, 14, 1101. https://doi.org/10.3390/ijerph14101101
Wang H, Tang C, Zhao S, Meng Q, Liu X. Job Satisfaction among Health-Care Staff in Township Health Centers in Rural China: Results from a Latent Class Analysis. International Journal of Environmental Research and Public Health. 2017; 14(10):1101. https://doi.org/10.3390/ijerph14101101
Chicago/Turabian StyleWang, Haipeng, Chengxiang Tang, Shichao Zhao, Qingyue Meng, and Xiaoyun Liu. 2017. "Job Satisfaction among Health-Care Staff in Township Health Centers in Rural China: Results from a Latent Class Analysis" International Journal of Environmental Research and Public Health 14, no. 10: 1101. https://doi.org/10.3390/ijerph14101101
APA StyleWang, H., Tang, C., Zhao, S., Meng, Q., & Liu, X. (2017). Job Satisfaction among Health-Care Staff in Township Health Centers in Rural China: Results from a Latent Class Analysis. International Journal of Environmental Research and Public Health, 14(10), 1101. https://doi.org/10.3390/ijerph14101101