
Quality of Life and Its Related Factors in Chinese Unemployed People: A Population-Based Cross-Sectional Study

Abstract
:1. Introduction
2. Methods
2.1. Study Design and Sample
2.2. Ethics Statement
2.3. Demographic Characteristics
2.4. QOL
2.5. Coping
2.6. Self-Efficacy
2.7. Statistical Analysis
3. Results
3.1. Description of the Demographic Characteristics
3.2. Description of QOL
3.3. Predictors of QOL
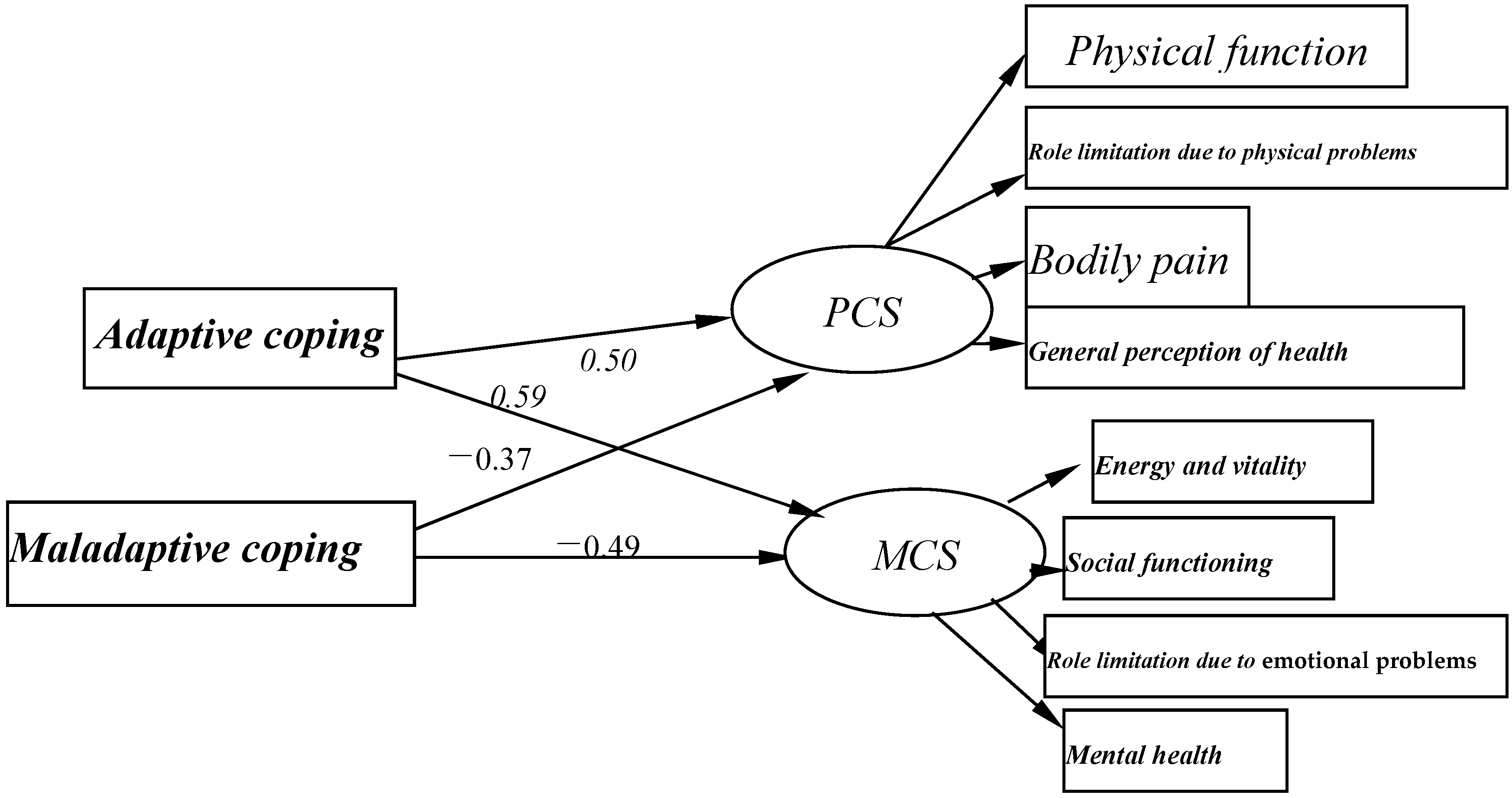
3.4. Association of Coping with QOL
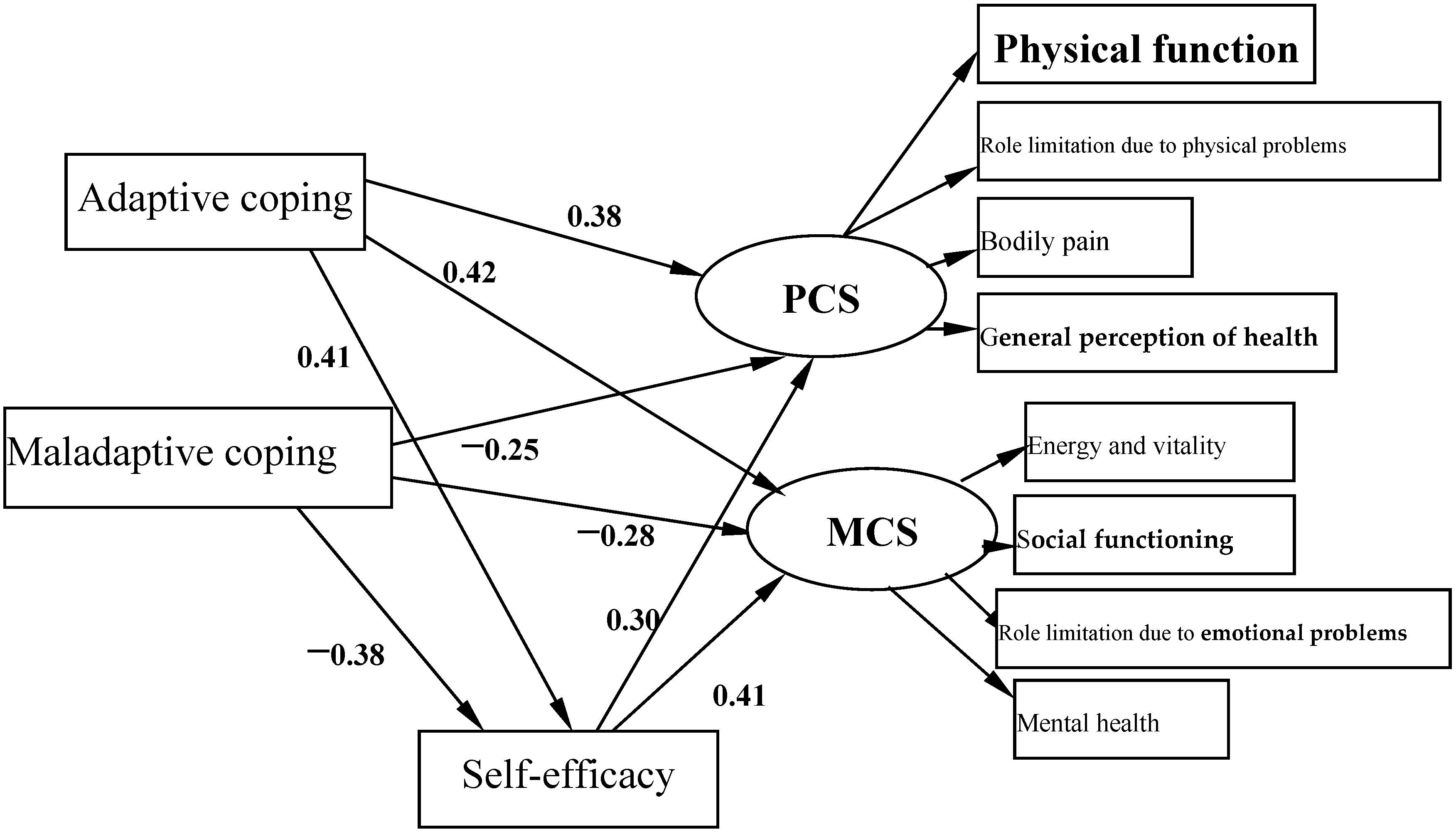
3.5. Mediating Role of Self-Efficacy on the Associations of Coping with QOL
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| QOL | Quality of life |
| SF-36 | the 36-item Short-Form Health Survey |
| PCS | physical component summary |
| MCS | mental component summary |
| ANOVA | one-way analysis of variance |
| HMR | Hierarchical multiple regression |
| SEM | Structural equation model |
References
- Zhang, H.Y. Research on China’s current unemployment. J. Jiamusi Educ. Inst. 2011, 106, 14–16. (In Chinese) [Google Scholar]
- Audhoe, S.S.; Hoving, J.L.; Sluiter, J.K.; Frings-Dresen, M.H. Vocational interventions for unemployed: Effects on work participation and mental distress: A systematic review. J. Occup. Rehabil. 2010, 20, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Stankūnas, M.; Kalediene, R.; Starkuviene, S. Sense of coherence and its associations with psychosocial health: Results of survey of the unemployed in Kaunas. Medicina (Kaunas) 2009, 45, 807–813. [Google Scholar] [PubMed]
- McLeod, C.B.; Lavis, J.N.; MacNab, Y.C.; Hertzman, C. Unemployment and mortality: A comparative study of Germany and the United States. Am. J. Public Health 2012, 102, 1542–1550. [Google Scholar] [CrossRef] [PubMed]
- Thomas, C.; Benzeval, M.; Stansfeld, S.A. Employment transitions and mental health: An analysis from the British household panel survey. J. Epidemiol. Community Health 2005, 59, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Hultman, B.; Hemlin, S. Self-rated quality of life among the young unemployed and the young in work in northern Sweden. Work 2008, 30, 461–472. [Google Scholar] [PubMed]
- Eden, D.; Aviram, A. Self-efficacy training to speed reemployment: Helping people to help themselves. J. Appl. Psychol. 1993, 78, 352–360. [Google Scholar] [CrossRef]
- Classen, T.J.; Dunn, R.A. The effect of job loss and unemployment duration on suicide risk in the United States: A new look using mass-layoffs and unemployment duration. Health Econ. 2012, 21, 338–350. [Google Scholar] [CrossRef] [PubMed]
- Lundin, A.; Lundberg, I.; Allebeck, P.; Hemmingsson, T. Unemployment and suicide in the Stockholm population: A register-based study on 771,068 men and women. Public Health 2012, 126, 371–377. [Google Scholar] [CrossRef] [PubMed]
- Kposowa, A.J. Unemployment and suicide: A cohort analysis of social factors predicting suicide in the U.S. National Longitudinal Mortality Study. Psychol. Med. 2001, 31, 127–138. [Google Scholar] [CrossRef] [PubMed]
- Fergusson, D.M.; Boden, J.M.; Horwood, L.J. Unemployment and suicidal behavior in a New Zealand birth cohort: A fixed effects regression analysis. Crisis 2007, 28, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Fergusson, D.M.; Horwood, L.J.; Woodward, L.J. Unemployment and psychosocial adjustment in young adults: Causation or selection? Soc. Sci. Med. 2001, 53, 305–320. [Google Scholar] [CrossRef]
- Smári, J.; Arason, E.; Hafsteinsson, H.; Ingimarsson, S. Unemployment, coping and psychological distress. Scand. J. Psychol. 1997, 38, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Hammer, T. Mental health and social exclusion among unemployed youth in Scandinavia, a comparative study. Int. J. Soc. Welf. 2000, 9, 53–63. [Google Scholar] [CrossRef]
- Pedersen, J.; Bjorner, J.B.; Burr, H.; Christensen, K.B. Transitions between sickness absence, work, unemployment, and disability in Denmark 2004–2008. Scand. J. Work Environ. Health 2012, 38, 516–526. [Google Scholar] [CrossRef] [PubMed]
- Moore, S.; Grunberg, L.; Greenberg, E. Repeated downsizing contact: The effects of similar and dissimilar layoff experiences on work and well-being outcomes. J. Occup. Health Psychol. 2004, 9, 247–257. [Google Scholar] [CrossRef] [PubMed]
- Howe, G.W.; Hornberger, A.P.; Weihs, K.; Moreno, F.; Neiderhiser, J.M. Higher-order structure in the trajectories of depression and anxiety following sudden involuntary unemployment. J. Abnorm. Psychol. 2012, 121, 325–338. [Google Scholar] [CrossRef] [PubMed]
- Kroll, L.E.; Lampert, T. Unemployment, social support and health problems: Results of the GEDA study in Germany, 2009. Dtsch. Arztebl. Int. 2011, 108, 47–52. [Google Scholar] [PubMed]
- Bilgiç, R.; Yılmaz, N. The correlates of psychological health among the Turkish unemployed: Psychological burden of financial help during unemployment. Int. J. Psychol. 2013, 48, 1000–1008. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer: New York, NY, USA, 1984; pp. 163–175. [Google Scholar]
- Chumbler, N.R.; Rittman, M.; Van Puymbroeck, M.; Vogel, W.B.; Qin, H. The sense of coherence, burden, and depressive symptoms in informal caregivers during the first month after stroke. Int. J. Geriatr. Psychiatry 2004, 19, 944–953. [Google Scholar] [CrossRef] [PubMed]
- Blalock, J.A.; Joiner, T.E. Interaction of cognitive avoidance coping and stress in predicting depression/anxiety. Cogn. Ther. Res. 2000, 24, 47–65. [Google Scholar] [CrossRef]
- Heppner, P.P.; Cook, S.W.; Wright, D.M.; Johnson, W.C. Progress in resolving problems: A problem-focused style of coping. J. Couns. Psychol. 1995, 42, 279–293. [Google Scholar] [CrossRef]
- Chen, L.; Li, W.; He, J.; Wu, L.; Yan, Z.; Tang, W. Mental health, duration of unemployment, and coping strategy: A cross-sectional study of unemployed migrant workers in eastern China during the economic crisis. BMC Public Health 2012, 12, 597. [Google Scholar] [CrossRef] [PubMed]
- Grossi, G. Coping and emotional distress in a sample of Swedish unemployed. Scand. J. Psychol. 1999, 40, 157–165. [Google Scholar] [CrossRef] [PubMed]
- Jerusalem, M. Personal resources, environmental constraints, and adaptational processes: The predictive power of a theoretical stress model. Pers. Individ. Differ. 1993, 14, 15–24. [Google Scholar] [CrossRef]
- Bandura, A. Self-Efficacy: The Exercise of Control; Freeman: New York, NY, USA, 1997. [Google Scholar]
- Bonsaksen, T.; Lerdal, A.; Fagermoen, M.S. Factors associated with self-efficacy in persons with chronic illness. Scand. J. Psychol. 2012, 53, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Marks, R.; Allegrante, J.P.; Lorig, K. A review and synthesis of research evidence for self-efficacy-enhancing interventions for reducing chronic disability: Implications for health education practice (part I). Health Promot. Pract. 2005, 6, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Nairn, R.C.; Merluzzi, T.V. The role of religious coping in adjustment to cancer. Psychooncology 2003, 12, 428–441. [Google Scholar] [CrossRef] [PubMed]
- Wilczyńska-Kwiatek, A. Psychotherapy of the unemployed: Determinants of efficacy. J. Physiol. Pharmacol. 2006, 57 (Suppl. 4), 391–401. [Google Scholar] [PubMed]
- International Labor Organization. Resolution Concerning Statistics of the Economically Active Population, Employment, Unemployment, and Underemployment, Adopted by the Thirteenth International Conference of Labor Statisticians (October 1982). Available online: http://www.ilo.org/public/english/bureau/stat/download/res/ecacpop.pdf (accessed on 26 November 2007).
- Ware, J.E., Jr.; Kosinski, M.; Gandek, B.; Aaronson, N.K.; Apolone, G.; Bech, P.; Brazier, J.; Bullinger, M.; Kaasa, S.; Leplège, A.; et al. The factor structure of the SF-36 Health Survey in 10 countries: Results from the IQOLA Project. J. Clin. Epidemiol. 1998, 51, 1159–1165. [Google Scholar] [CrossRef]
- Woo, J.; Lau, E.; Lee, P.; Kwok, T.; Lau, W.C.; Chan, C.; Chiu, P.; Li, E.; Sham, A.; Lam, D. Impact of osteoarthritis on quality of life in a Hong Kong Chinese population. J. Rheumatol. 2004, 31, 2433–2438. [Google Scholar] [PubMed]
- Carver, C.S. You want to measure coping but your protocol’s too long: Consider the brief cope. Int. J. Behav. Med. 1997, 4, 92–100. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Song, Z.; Liu, H. Psychological researches on job search behaviors. Adv. Psychol. Sci. 2006, 14, 631–635. [Google Scholar]
- Barlow, J.H.; Williams, B.; Wright, C. The generalized self-efficacy scale in people with arthritis. Arthritis Care Res. 1996, 9, 189–196. [Google Scholar] [CrossRef]
- Tipton, R.M.; Worthington, E.L., Jr. The measurement of generalized self-efficacy: A study of construct validity. J. Pers. Assess. 1984, 48, 545–548. [Google Scholar] [PubMed]
- Kahn, H.A.; Sempos, C.T. Statistical Methods in Epidemiology; Oxford University Press: New York, NY, USA, 1989; pp. 147–157. [Google Scholar]
- Preacher, K.J.; Hayes, A.F. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav. Res. Meth. 2008, 40, 879–891. [Google Scholar] [CrossRef]
- Li, N.; Liu, C.; Li, J.; Ren, X. The norms of SF-36 scale scores in urban and rural residents of Sichuan province. J. West China Univ. Med. Sci. 2001, 32, 43–47. (In Chinese) [Google Scholar]
- Yan, L.; Kou, C.; Yao, Y.; Li, X.; Shi, J.; Shan, G.; Yu, Y. Investigation of health-related quality of life in incumbency residents of Changchun with SF-36 Chinese Edition. Chin. J. Dis. Control Prev. 2010, 14, 383–385. (In Chinese) [Google Scholar]
- Wang, D. Investigation on factors related to quality of life among 142 migrant workers in a university. Chin. J. Social Med. 2008, 25, 243–245. (In Chinese) [Google Scholar] [CrossRef]
- Jiang, E.; Yang, Y.; Tang, C.; Zhang, X.; Wang, Z.; Cheng, G. Analysis on life quality among workers who exposed to noise. Modern Prev. Med. 2008, 1, 39–42. (In Chinese) [Google Scholar]
- Ding, B.; Gong, J.; Zhu, B.; Zhang, H.; Yu, S.; Han, L. Investigation of factors related to quality of life of workers in the oil field. Modern Prev. Med. 2007, 34, 214–217. (In Chinese) [Google Scholar]
- Yang, X.; Ge, C.; Hu, B.; Chi, T.; Wang, L. Relationship between quality of life and occupational stress among teachers. Public Health 2009, 123, 750–755. [Google Scholar] [CrossRef] [PubMed]
- Kroll, L.E.; Lampert, T. Changing health inequalities in Germany from 1994 to 2008 between employed and unemployed adults. Int. J. Public Health 2011, 56, 329–339. [Google Scholar] [CrossRef] [PubMed]
- Madianos, M.; Economou, M.; Alexiou, T.; Stefanis, C. Depression and economic hardship across Greece in 2008 and 2009: Two cross-sectional surveys nationwide. Soc. Psychiatry Psychiatr. Epidemiol. 2011, 46, 943–952. [Google Scholar] [CrossRef] [PubMed]
- Liwowsky, I.; Kramer, D.; Mergl, R.; Bramesfeld, A.; Allgaier, A.K.; Pöppel, E.; Hegerl, U. Screening for depression in the older long-term unemployed. Soc. Psychiatry Psychiatr. Epidemiol. 2009, 44, 622–627. [Google Scholar] [CrossRef] [PubMed]
- Nuttman-Shwartz, O.; Gadot, L. Social factors and mental health symptoms among women who have experienced involuntary job loss. Anxiety Stress Coping 2012, 25, 275–290. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y. The survey and study of the mental state of unemployed women. Women’s Acad. Shandong 2007, 73, 15–119. [Google Scholar]
- Booker, C.L.; Sacker, A. Psychological well-being and reactions to multiple unemployment events: Adaptation or sensitisation? J. Epidemiol. Community Health 2012, 66, 832–838. [Google Scholar] [CrossRef] [PubMed]
- Aittomäki, A.; Martikainen, P.; Laaksonen, M.; Lahelma, E.; Rahkonen, O. Household economic resources, labour-market advantage and health problems—A study on causal relationships using prospective register data. Soc. Sci. Med. 2012, 75, 1303–1310. [Google Scholar] [CrossRef] [PubMed]
- Morimoto, T.; Schreiner, A.S.; Asano, H. Caregiver burden and health-related quality of life among Japanese stroke caregivers. Age Ageing 2003, 32, 218–223. [Google Scholar] [CrossRef] [PubMed]
- Garcy, A.M.; Vågerö, D. The length of unemployment predicts mortality, differently in men and women, and by cause of death: A six year mortality follow-up of the Swedish 1992–1996 recession. Soc. Sci. Med. 2012, 74, 1911–1920. [Google Scholar] [CrossRef] [PubMed]
- Winefield, A.H.; Tiggemann, M. Length of unemployment and psychological distress: Longitudinal and cross-sectional data. Soc. Sci. Med. 1990, 31, 461–465. [Google Scholar] [CrossRef]
- Baum, A.; Fleming, R.; Reddy, D.M. Unemployment stress: Loss of control, reactance and learned helplessness. Soc. Sci. Med. 1986, 22, 509–516. [Google Scholar] [CrossRef]
- Stankunas, M.; Kalediene, R.; Starkuviene, S.; Kapustinskiene, V. Duration of unemployment and depression: A cross-sectional survey in Lithuania. BMC Public Health 2006, 6, 174. [Google Scholar] [CrossRef] [PubMed]
- Leana, C.R.; Feldman, D.C. Individual reactions to job loss: Emprirical findings from two field studies. Hum. Relat. 1995, 11, 1155–1181. [Google Scholar]
- Mantler, J.; Matejicek, A.; Matheson, K.; Anisman, H. Coping with employment uncertainty: A comparison of employed and unemployed workers. J. Occup. Health Psychol. 2005, 10, 200–209. [Google Scholar] [CrossRef] [PubMed]
- Turner, J.B.; Kessler, R.C.; House, J.S. Factors facilitating adjustment to unemployment: Implications for intervention. Am. J. Community Psychol. 1991, 19, 521–542. [Google Scholar] [CrossRef] [PubMed]
- Kreitler, S.; Peleg, D.; Ehrenfeld, M. Stress, self-efficacy and quality of life in cancer patients. Psychooncology 2007, 16, 329–341. [Google Scholar] [CrossRef] [PubMed]
- Zeiss, A.M.; Gallagher-Thompson, D.; Lovett, S.; Pose, J.; McKibbin, C. Self-efficacy as a mediator of caregiver coping: Development and testing of an assessment model. J. Clin. Geropsychol. 1999, 5, 221–230. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variables | Number (N) | Percent (%) |
|---|---|---|
| Gender | ||
| Male | 1022 | 56.00 |
| Female | 803 | 44.00 |
| Age | ||
| <25 | 367 | 20.11 |
| 25–39 | 806 | 44.16 |
| >39 | 652 | 35.73 |
| Marital status | ||
| Married | 1073 | 58.79 |
| Others | 752 | 41.21 |
| Educational level | ||
| ≤senior high school | 1156 | 63.34 |
| >senior high school | 669 | 36.66 |
| Household monthly income (Yuan) | ||
| ≤1000 | 417 | 22.85 |
| 1001–1500 | 391 | 21.42 |
| 1501–2000 | 420 | 23.01 |
| >2000 | 597 | 32.71 |
| Chronic diseases | ||
| Yes | 994 | 54.47 |
| No | 831 | 45.53 |
| Unemployed time (months) | ||
| 1–2 | 387 | 21.21 |
| 3–5 | 372 | 20.38 |
| 6–11 | 454 | 24.88 |
| ≥12 | 612 | 33.53 |
| Mean ± S.D. | ||
| Physical function | 84.3 ± 19.7 | |
| Role limitation due to physical problems | 65.4 ± 33.3 | |
| Bodily pain | 72.9 ± 22.0 | |
| General perception of health | 61.4 ± 18.4 | |
| Energy and vitality | 61.0 ± 17.8 | |
| Social functioning | 70.1 ± 20.4 | |
| Role limitation due to emotional problems | 58.4 ± 36.6 | |
| Mental health | 59.6 ± 17.6 |
| Variables | PCS | MCS |
|---|---|---|
| Gender | ||
| Male | 71.8 ± 17.6 | 62.9 ± 17.1 |
| Female | 70.2 ± 17.2 * | 61.9 ± 16.5 |
| Age | ||
| <25 | 77.6 ± 14.8 ** | 64.5 ± 15.6 * |
| 25–39 | 71.4 ± 16.7 * | 61.7 ± 16.2 |
| >39 | 66.9 ± 18.5 | 62.1 ± 18.3 |
| Marital status | ||
| Married | 69.2 ± 17.4 ** | 62.5 ± 17.2 |
| Others | 73.8 ± 16.3 | 62.3 ± 15.9 |
| Education level | ||
| ≤senior high school | 69.6 ± 17.3 ** | 62.1 ± 17.0 |
| >senior high school | 73.6 ± 16.4 | 63.1 ± 16.3 |
| Household monthly income (Yuan) | ||
| ≤1000 | 67.0 ± 18.1 ** | 58.7 ± 17.1 ** |
| 1001–1500 | 70.3 ± 17.3 * | 61.5 ± 16.8 * |
| 1501–2000 | 71.0 ± 17.5 * | 63.1 ± 16.3 |
| >2000 | 74.4 ± 16.4 | 65.1 ± 16.7 |
| Chronic diseases | ||
| Yes | 64.0 ± 17.3 ** | 59.2 ± 16.8 ** |
| No | 76.8 ± 15.4 | 65.0 ± 16.5 |
| Unemployed time | ||
| 1–2 month | 76.2 ± 15.7 | 65.1 ± 16.8 |
| 3–5month | 73.8 ± 16.0 * | 63.8 ± 15.2 * |
| 6–11 month | 70.2 ± 17.5 ** | 62.0 ± 15.6 * |
| ≥12 month | 66.9 ± 18.2 ** | 60.0 ± 18.4 ** |
| Mean | SD | PCS | MCS | Adaptive Coping | Maladaptive Coping | Self-Efficacy | |
|---|---|---|---|---|---|---|---|
| PCS | 71.1 | 17.4 | 1 | ||||
| MCS | 62.4 | 16.9 | 0.620 ** | 1 | |||
| Adaptive coping | 45.7 | 7.2 | 0.275 ** | 0293 ** | 1 | ||
| Maladaptive coping | 40.6 | 6.9 | −0.140 ** | −0.193 ** | 0.400 ** | 1 | |
| Self-efficacy | 38.3 | 5.7 | 0.332 ** | 0.450 ** | 0.259 ** | −0.220 ** | 1 |
| Variables | PCS | MCS | ||||
|---|---|---|---|---|---|---|
| Model 1 b(B) | Model 2 b(B) | Model 3 b(B) | Model 1 b(B) | Model 2 b(В) | Model 3 b(B) | |
| Intercept | 77.334 ** | 61.775 ** | 42.673 ** | 73.377 ** | 61.306 ** | 28.244 ** |
| Block 1 Demographic characteristics | ||||||
| Gender | −1.800 * (−0.051) | −1.891 * (−0.054) | −1.541 * (−0.044) | −1.289 (−0.038) | −1.366 (−0.040) | −0.822 (−0.024) |
| Age | ||||||
| 25–39 vs. <25 | −3.287 ** (−0.094) | −1.574 (−0.045) | −1.630 (−0.046) | −2.437 * (−0.072) | −0.493 (−0.015) | −0.454 (−0.013) |
| >39 vs. <25 | −2.615 (−0.072) | −1.182 (−0.032) | −1.375 (−0.038) | 0.414 (0.012) | 2.336 (0.066) | 1.974 (0.056) |
| Marital status | −0.045 (−0.001) | 0.687 (0.019) | 0.756 (0.021) | −2.486 * (−0.073) | −1.628 (−0.048) | −1.449 (−0.042) |
| Educational level | 0.847 (0.023) | 0.609 (0.017) | 0.347 (0.010) | −0.251 (−0.007) | −0.564 (−0.016) | −1.027 (−0.029) |
| Chronic diseases | −10.876 ** (−0.311) | −10.159 ** (−0.290) | −9.891 ** (−0.282) | −5.737 ** (−0.170) | −5.049 ** (−0.149) | −4.562 ** (−0.135) |
| Household monthly income (yuan) | ||||||
| 1001–1500 vs. ≤1000 | 2.300 (0.054) | 2.295 * (0.054) | 2.332 * (0.055) | 2.386 * (0.058) | 2.252 * (0.055) | 2.403 * (0.059) |
| 1501–2000 vs. ≤1000 | 3.043 ** (0.074) | 2.100 (0.051) | 2.211 * (0.053) | 4.005 ** (0.100) | 2.718 * (0.068) | 3.016 ** (0.076) |
| >2000 vs. ≤1000 | 5.031 ** (0.136) | 3.627 ** (0.098) | 3.116 ** (0.084) | 5.206 ** (0.145) | 3.211 ** (0.089) | 2.476 * (0.069) |
| Unemployed time (months) | ||||||
| 3–5 vs. 1–2 | −0.317 (−0.007) | 0.474 (0.011) | 0.698 (0.016) | −0.698 (−0.017) | 0.415 (0.010) | 0.771 (0.019) |
| 6–11 vs. 1–2 | −2.487 * (−0.061) | −1.567 (−0.039) | −1.256 (−0.031) | −1.973 (−0.050) | −0.844 (−0.022) | −0.258 (−0.007) |
| ≥12 vs. 1–2 | −3.763 ** (−0.102) | −3.541 ** (−0.096) | −3.283 ** (−0.089) | −3.807 ** (−0.107) | −3.576 ** (−0.100) | −3.009 ** (−0.084) |
| Block 2 Coping | ||||||
| Adaptive coping | 0.856 ** (0.344) | 0.684 ** (0.275) | 0.973 ** (0.407) | 0.682 ** (0.285) | ||
| Maladaptive coping | −0.639 ** (−0.248) | −0.473 ** (−0.184) | −0.860 ** (−0.348) | −0.573 ** (−0.232) | ||
| Block 3 Self-efficacy | 0.531 ** (0.174) | 0.906 ** (0.306) | ||||
| R2 | 0.167 | 0.281 | 0.304 | 0.061 | 0.235 | 0.308 |
| △R2 | 0.167 | 0.114 | 0.023 | 0.061 | 0.174 | 0.073 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, X.; Yao, L.; Wu, H.; Wang, Y.; Liu, L.; Wang, J.; Wang, L. Quality of Life and Its Related Factors in Chinese Unemployed People: A Population-Based Cross-Sectional Study. Int. J. Environ. Res. Public Health 2016, 13, 797. https://doi.org/10.3390/ijerph13080797
Yang X, Yao L, Wu H, Wang Y, Liu L, Wang J, Wang L. Quality of Life and Its Related Factors in Chinese Unemployed People: A Population-Based Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2016; 13(8):797. https://doi.org/10.3390/ijerph13080797
Chicago/Turabian StyleYang, Xiaoshi, Lutian Yao, Hui Wu, Yang Wang, Li Liu, Jiana Wang, and Lie Wang. 2016. "Quality of Life and Its Related Factors in Chinese Unemployed People: A Population-Based Cross-Sectional Study" International Journal of Environmental Research and Public Health 13, no. 8: 797. https://doi.org/10.3390/ijerph13080797
APA StyleYang, X., Yao, L., Wu, H., Wang, Y., Liu, L., Wang, J., & Wang, L. (2016). Quality of Life and Its Related Factors in Chinese Unemployed People: A Population-Based Cross-Sectional Study. International Journal of Environmental Research and Public Health, 13(8), 797. https://doi.org/10.3390/ijerph13080797