
Hot of Not: Physiological versus Meteorological Heatwaves—Support for a Mean Temperature Threshold

Abstract
:1. Introduction
2. Methodology
2.1. Study Design and Context
2.2. Participants and Data Collection
- -
- The patient’s medical record number
- -
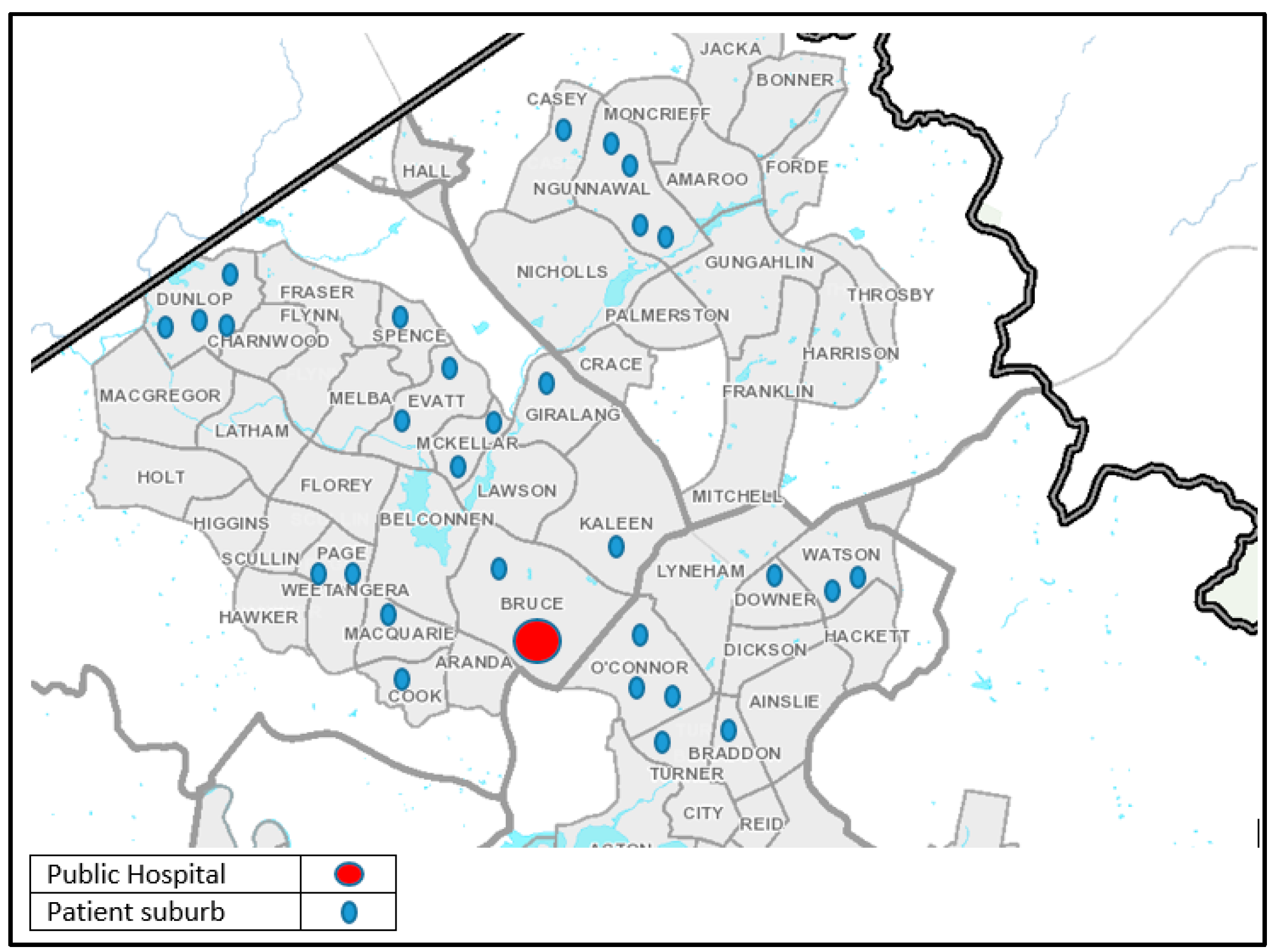
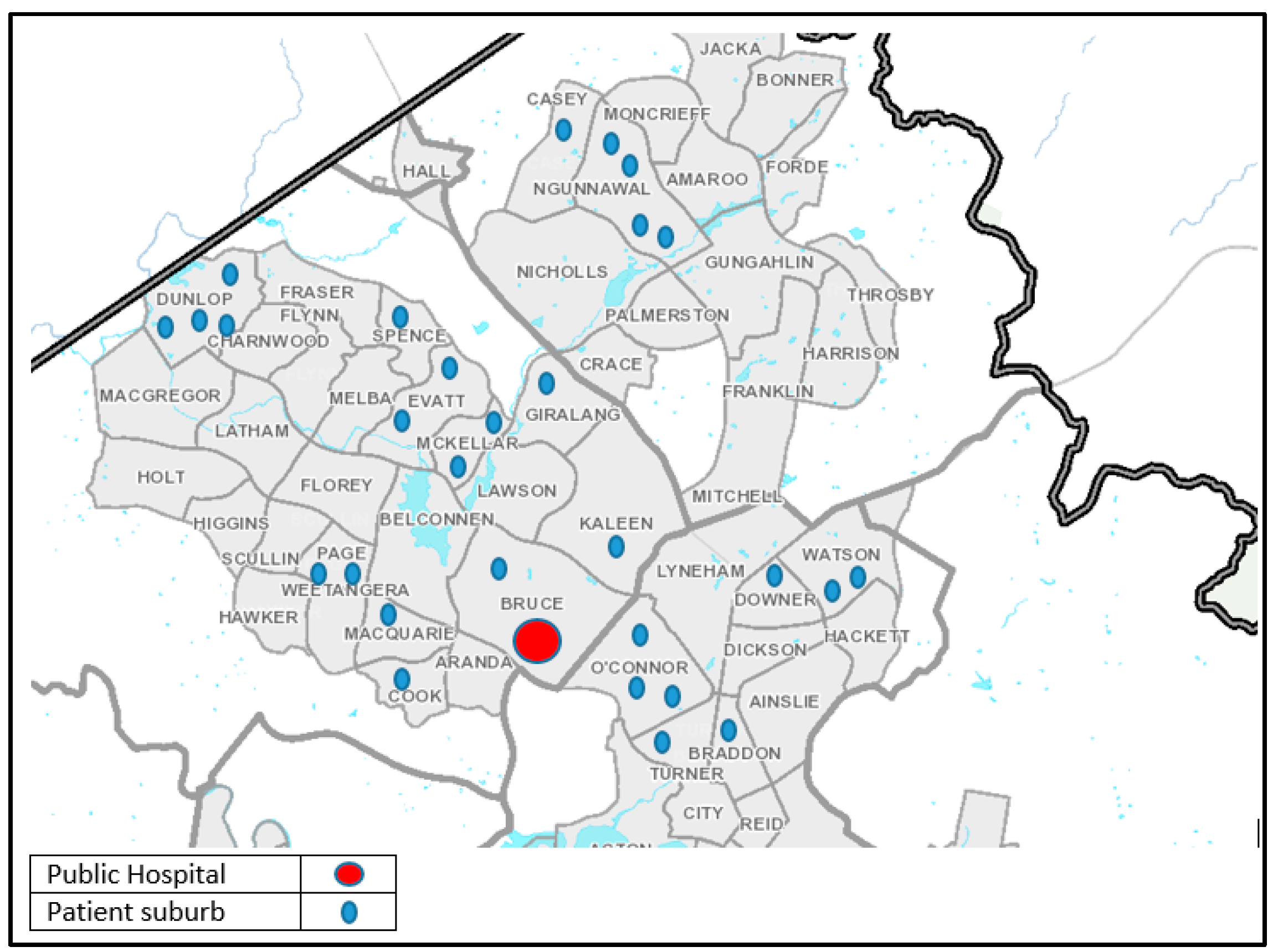
- Patient’s home demographics (suburb or town)
- -
- Arrival time and date
- -
- Did the presentation have signs and symptoms related and conducive to heat, and
- -
- Did the signs and symptoms result in treatment for a heat related illness, and
- -
- Was the final diagnosis upon discharge related to heat
- -
- -
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Nicholls, N.; Skinner, C.; Loughnan, M.E.; Tapper, N.J. A simple heat alert system for Melbourne, Australia. Int. J. Biometeorol. 2008, 52, 375–384. [Google Scholar]
- Whitman, S.; Good, G.; Donoghue, E.R.; Benbow, N.; Shou, W.; Mou, S. Mortality in Chicago attributed to the July 1995 heat wave. Am. J. Public Health Res. 1997, 87, 1515–1518. [Google Scholar]
- Vaneckova, P.; Beggs, P.J.; de Dear, R.J.; McCracken, K.W. Effect of temperature on mortality during the six warmer months in Sydney, Australia, between 1993 and 2004. Environ. Res. 2008, 108, 361–369. [Google Scholar] [PubMed]
- Akompab, D.A.; Bi, P.; Williams, S.; Grant, J.; Walker, I.A.; Augoustinos, M. Heat waves and climate change: Applying the health belief model to identify predictors of risk perception and adaptive behaviours in Adelaide, Australia. Int. J. Environ. Res. Public Health 2013, 10, 2164–2184. [Google Scholar]
- Akompab, D.A.; Bi, P.; Williams, S.; Grant, J.; Walker, I.A.; Augoustinos, M. Awareness of and attitudes towards heat waves within the context of climate change among a cohort of residents in Adelaide, Australia. Int. J. Environ. Res. Public Health 2012, 10, 1–17. [Google Scholar]
- Akompab, D.A.; Bi, P.; Williams, S.; Saniotis, A.; Walker, I.A.; Augoustinos, M. Engaging stakeholders in an adaptation process: Governance and institutional arrangements in heat-health policy development in Adelaide, Australia. Mitig. Adapt. Strateg. Glob. Chang. 2013, 18, 1001–1018. [Google Scholar]
- Wilson, L.A.; Morgan, G.G.; Hanigan, I.C.; Johnston, F.H.; Abu-Rayya, H.; Broome, R.; Gaskin, C.; Jalaludin, B. The impact of heat on mortality and morbidity in the Greater Metropolitan Sydney Region: A case crossover analysis. Environ. Health 2013, 12, 98. [Google Scholar] [PubMed]
- Loughnan, M.E.; Nicholls, M.; Tapper, N. Mortality-temperature thresholds for ten major population centres in rural Victoria, Australia. Health Place 2010, 16, 1287–1290. [Google Scholar] [CrossRef] [PubMed]
- Mayner, L.; Arbon, P.; Usher, K. Emergency department patient presentations during the 2009 heatwaves in Adelaide. Collegian 2010, 17, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Yardley, J.; Sigal, R.J.; Kenny, G.P. Heat health planning: The importance of social and community factors. Glob. Environ. Chang. 2011, 21, 670–679. [Google Scholar] [CrossRef]
- Vaneckova, P.; Beggs, P.J.; Jacobson, C.R. Spatial analysis of heat-related mortality among the elderly between 1993 and 2004 in Sydney, Australia. Soc. Sci. Med. 2010, 70, 293–304. [Google Scholar] [CrossRef] [PubMed]
- Williams, S.; Nitschke, M.; Weinstein, P.; Pisaniello, D.L.; Parton, K.A.; Bi, P. The impact of summer temperatures and heatwaves on mortality and morbidity in Perth, Australia 1994–2008. Environ. Int. 2012, 40, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Loughnan, M.E.; Nicholls, N.; Tapper, N.J. When the heat is on: Threshold temperatures for AMI admissions to hospital in Melbourne Australia. Appl. Geogr. 2010, 30, 63–69. [Google Scholar] [CrossRef]
- Zhang, Y.; Nitschke, M.; Bi, P. Risk factors for direct heat-related hospitalization during the 2009 Adelaide heatwave: A case crossover study. Sci. Total Environ. 2013, 442, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Williams, S.; Nitschke, M.; Sullivan, T.; Tucker, G.R.; Weinstein, P.; Pisaniello, D.L.; Parton, K.A.; Bi, P. Heat and health in Adelaide, South Australia: Assessment of heat thresholds and temperature relationships. Sci. Total Environ. 2012, 414, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Australasian Fire and Emergency Service Authorities Council. A management system for any emergency. In the Australian Inter-Service Incident Management System, 4th ed.; Australasian Fire and Emergency Service Authorities Council: Melbourne, Australia, 2013. [Google Scholar]
- Daily Weather Observations. Australian Government: Bureau of Meteorology, 2013. Available online: http://www.bom.gov.au/climate/dwo/201312/html/IDCJDW2801.201312.shtml (accessed on 1 March 2014).
- Nairn, J.; Fawcett, R. Defining Heatwaves: Heatwave Defined as a Heat-Impact Servicing All Community and Business Sectors in Australia; Bureau of Meterology CSIRO: Kent Town, Australia, 2013.
- ACT Government Emergency Service Agency. Extreme Heat Management Plan: A Supporting Plan of the ACT Emergency Plan That Outlines the Standing and Emergency Arrangements for an All Agencies Approach to an Extreme Heat Event in the Australian Capital Territory; Emergency Service Agency: Canberra, Australia, 2010.
- ACT Government Health Directorate. Health Emergency Plan Appendix IV: Part A—Summer Plan (for Extreme Heat Events and Elevated Fire Conditions); Version 1 July 2013; ACT Government, Health Directorate: Canberra, Australia, 2013.
- PricewaterhouseCoopers Australia. Protecting Human Health and Safety during Severe and Extreme Heat Events: A National Framework; PwC Australia: Canberra, Australia, 2011. [Google Scholar]
- Australian Bureau of Statistics. 3101.0—Australian Demograpic Statistics; Australian Bureau of Statistics: Canberra, Australia, 2013.
- Bi, P.; Williams, S.; Loughnan, M.; Lloyd, G.; Hansen, A.; Kjellstrom, T.; Dear, K.; Saniotis, A. The Effects of Extreme Heat on Human Mortality and Morbidity in Australia: Implications for Public Health. Asia Pac. J. Public Health 2011, 23, 27S–36S. [Google Scholar] [PubMed]
- Khalaj, B.; Lloyd, G.; Sheppeard, V.; Dear, K. The health impacts of heat waves in five regions of New South Wales, Australia: A case-only analysis. Int. Arch. Occup. Environ. Health 2010, 83, 833–842. [Google Scholar] [CrossRef] [PubMed]
- Nairn, J.R.; Fawcett, R.J.B. The Excess Heat Factor: A Metric for Heatwave Intensity and Its Use in Classifying Heatwave Severity. Int. J. Environ. Res. Public Health 2015, 12, 227–253. [Google Scholar] [CrossRef] [PubMed]
- Climate Data Online: Bureau of Meterorology, 2014. Available online: http://www.bom.gov.au/climate/data/?ref=ftr (accessed on 13 April 2016).
- Barnett, A.G.; Tong, S.; Clements, A.C. What measure of temperature is the best predictor of mortality? Environ. Res. 2010, 110, 604–611. [Google Scholar] [CrossRef] [PubMed]
- Victoria State Government. Heat Health Plan for Victoria: Victoria State Government; Health and Human Services: Melbourne, Australia, 2015.
- Government of South Australia. Extreme Heat Operational Plan; South Australian Health: Adelaide, Australia, 2013.
- Williams, S.; Nitschke, M.; Tucker, G.; Bi, P. Extreme heat arrangements in South Australia: An assessment of trigger temperatures. Health Promot. J. Aust. 2011, 22, 21–27. [Google Scholar]
- Baseman, J.G.; Revere, D.; Painter, I.; Toyoji, M.; Thiede, H.; Duchin, J. Public health communications and alert fatigue. BMC Health Serv. Res. 2013, 13, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Montero, J.C.; Miron, I.J.; Criado, J.J.; Linares, C.; Diaz, J. Difficulties of defining the term, “heat wave”, in public health. Int. J. Environ. Health Res. 2013, 23, 377–379. [Google Scholar] [PubMed]
- Kovats, R.S.; Kristie, L.E. Heatwaves and public health in Europe. Eur. J. Public Health 2006, 16, 592–599. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| City | 2011 | 2030 | 2050 |
|---|---|---|---|
| Brisbane | 19 | 32 | 49 |
| Perth | 10 | 17 | 25 |
| Sydney | 18 | 25 | 34 |
| ACT (Canberra) | 2 | 4 | 6 |
| Adelaide | 11 | 16 | 21 |
| Melbourne | 23 | 33 | 48 |
| Tasmania | 3 | 4 | 5 |
| Total | 86 | 131 | 188 |
| Type | Symptoms | Signs | Emergency Treatment |
|---|---|---|---|
| Mild illness (cramps, exhaustion) | Diarrhoea, dizziness, headache, irritability, loss of coordination, nausea/vomiting, syncope, weakness | Core temperature <40 °C, normal mentation, goose flesh, pallor, tachycardia, hypotension | Oral rehydration Symptom management Monitoring |
| Heat stroke | Confusion, dizziness, hallucination, headache, nausea/vomiting, syncope | Core temperature >40 °C, altered mental status, hot skin with or without perspiration, hypotension, seizure, tachycardia | Intravenous rehydration Electrolyte monitoring Active cooling Seizure management Management/prophylaxis Monitoring |
| Physiological and Environmental |
|---|
| Age older then >64 year old or younger then <2 year old |
| Cognitive impairment |
| Heart and lung disease |
| Limited access to air-conditioning |
| Mental illness |
| Obesity |
| Physical disability/impaired mobility |
| Poor fitness level |
| Sickle cell trait |
| Strenuous outdoor physical activity during hottest day-time hours |
| Urban built-up residence or living on higher floors |
| Medication and/or Substances | |
|---|---|
| Alcohol | Laxatives |
| Alpha-adrenergic agonist | Neuroleptics |
| Amphetamines | Phenothiazine |
| Anticholinergics | Other stimulants |
| Antihistamines | Thyroid receptor agonists |
| Benzodiazepines | Tricyclic antidepressants |
| Beta Blockers | Diuretics |
| Calcium channel blockers | Ephedra-containing supplements |
| Cocaine | |
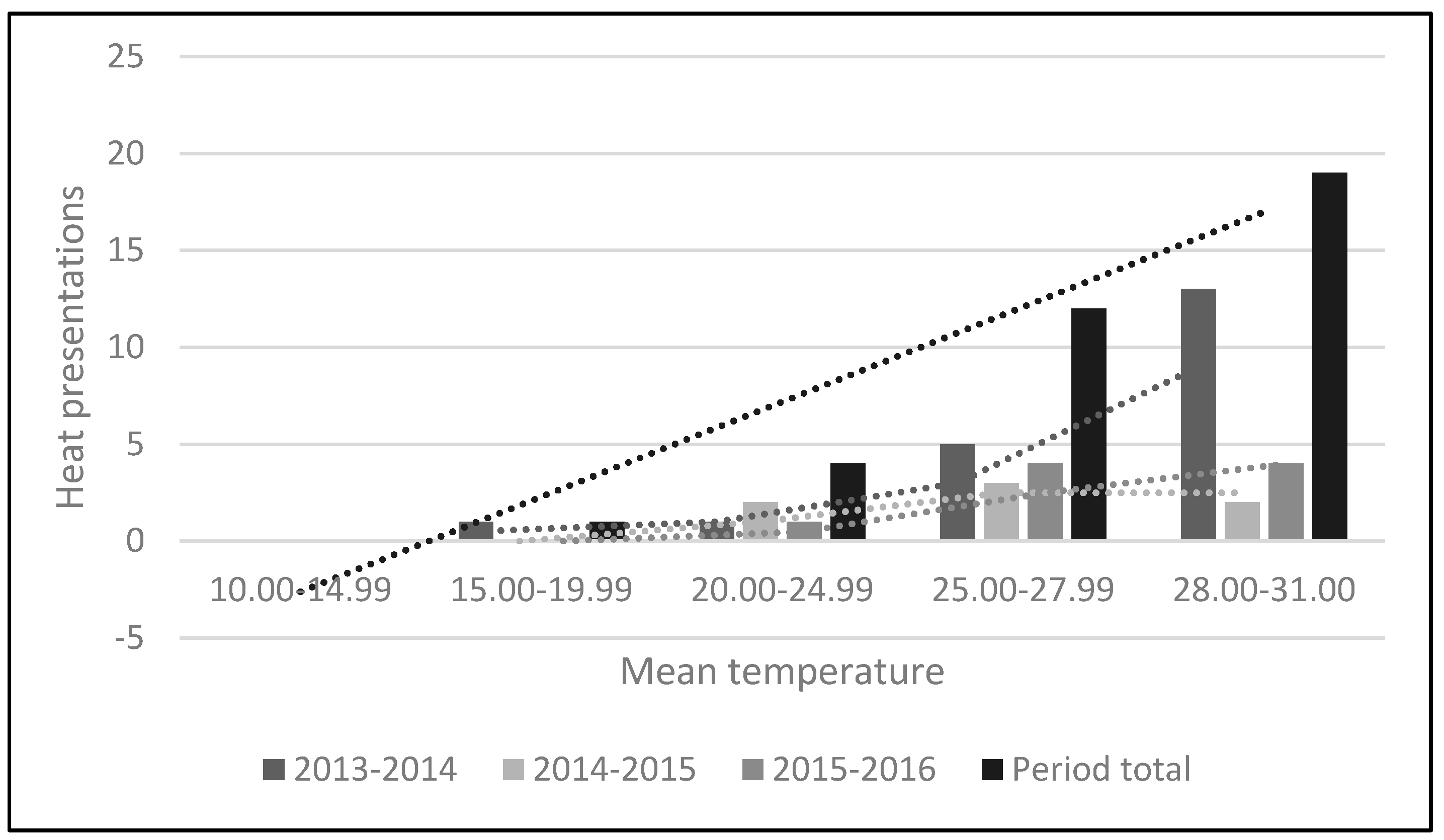
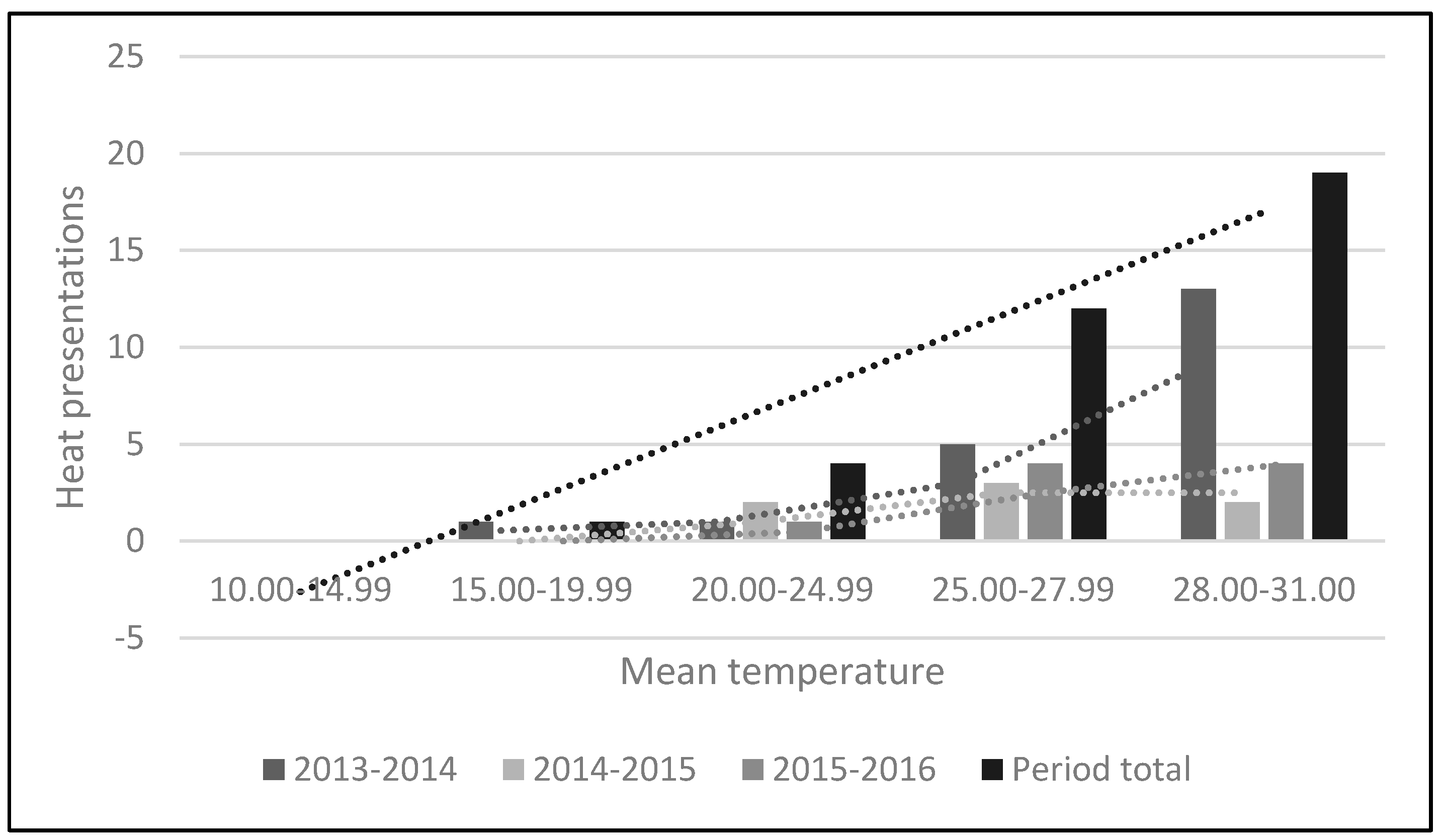
| Heat Related Presentations | ||||
|---|---|---|---|---|
| Mean Temperature (°C) | 2013–2014 | 2014–2015 | 2015–2016 | Period Total |
| 10.0–14.9 | 0 | 0 | 0 | 0 |
| 15.0–19.9 | 1 | 0 | 0 | 1 |
| 20.0–24.9 | 1 | 2 | 1 | 4 |
| 25.0–27.9 | 5 | 3 | 4 | 12 |
| 28.0–31.0 | 13 | 2 | 4 | 19 |
| Total | 20 | 7 | 9 | 36 |
| Summer mean temperature (°C) | 21.1 | 20.48 | 20.95 | |
| Year | Summer Month | Mean Monthly Temperature | Max Temperature | Min Temperature | Number of Days Reaching 35 °C or Greater |
|---|---|---|---|---|---|
| 2013 | December | 20.0 | 38.1 | 2.7 | 3 |
| 2014 | January | 21.8 | 40.2 | 6.1 | 9 |
| February | 21.5 | 39.3 | 5.1 | 7 | |
| December | 20.2 | 32.7 | 7.2 | 0 | |
| 2015 | January | 20.7 | 35.2 | 7.5 | 1 |
| February | 20.6 | 34.4 | 6.7 | 0 | |
| December | 20.3 | 36.3 | 3.8 | 3 | |
| 2016 | January | 21.2 | 39.3 | 8.0 | 6 |
| February | 21.3 | 38.0 | 8.4 | 2 | |
| Total | 20.8 (m) | 37.1 (m) | 6.2 (m) | 31 |
| Related Specialty | Total Number | Percentage | General Description |
|---|---|---|---|
| Allergy and immunology | 4 | 9.5 | Insect bites (n = 1); Allergic reaction (n = 3) |
| Bacterial infection/infectious disease | 4 | 9.5 | Cellulitis (n = 4) |
| Cardiovascular | 2 | 4.8 | Chest pain (n = 2) |
| Gastrointestinal | 3 | 7.1 | Constipation (n = 1); Gastroenteritis (n = 1); Epigastric pain (n = 1) |
| Musculoskeletal | 18 | 42.9 | Abdominal pain (n = 1); Meniscus tear (n = 1); General limb and joint pain (n = 1); Hip pain (n = 1); Knee pain (n = 3); Foot/ankle pain and swelling (n = 1); Wry neck (n = 1); Bruising (n = 1); Back pain (n = 5); Muscle sprain (n = 1); Arm pain (n = 1); Leg pain (n = 1) |
| Orthopaedic | 1 | 2.4 | Orthopaedic joint effusion (n = 1) |
| Respiratory | 4 | 9.5 | Viral illness (n = 2); Pneumonia (n = 1); Upper respiratory tract infection (n = 1) |
| Rheumatology | 1 | 2.4 | Gout (n = 1) |
| Trauma | 4 | 9.5 | Severe burn (n = 2); Laceration (n = 1); Penetrating stab wound (n = 1) |
| Urology | 1 | 2.4 | Urinary retention (n = 1) |
| Total | 42 | 100.0 |
| Discharge Diagnosis | Patient Number | Percentage |
|---|---|---|
| Heat related dehydration | 10 | 27.8 |
| Heat related illness | 9 | 25.0 |
| Heat stress | 7 | 19.4 |
| Chest infection and heat stress | 1 | 2.8 |
| Heat related illness and cellulitis | 1 | 2.8 |
| Heat related lethargy | 1 | 2.8 |
| Heat related nausea and vomiting | 1 | 2.8 |
| Heat related syncope | 1 | 2.8 |
| Heat stress and dehydration | 1 | 2.8 |
| Heat stress related to mental disorder | 1 | 2.8 |
| Heat stroke and UTI | 1 | 2.8 |
| Heat related nausea and vomiting | 1 | 2.8 |
| Heat and viral illness | 1 | 2.8 |
| Total | 36 | 100.0 |
| Physiological and Environmental | Total Number of Patients with the Following Risk Factors | Percentage |
|---|---|---|
| Strenuous outdoor physical activity during hottest day-time hours | 18 | 33.3 |
| Age older then >64 year old or younger then <2 year old | 14 | 25.9 |
| Limited access to air-conditioning | 10 | 18.5 |
| Medication and substance use (alcohol) | 3 | 5.5 |
| Mental illness | 3 | 5.5 |
| Physical disability/impaired mobility | 3 | 5.5 |
| Cognitive impairment | 2 | 3.7 |
| Heart and lung disease | 1 | 1.8 |
| Total | 54 | 100.0 |
| Primary Heat Related Symptoms | Number | Percentage | Secondary Symptoms | Number | Percentage |
|---|---|---|---|---|---|
| Confusion | 3 | 8.3 | Confusion | 2 | 5.6 |
| Dizziness | 3 | 8.3 | Diarrhoea | 1 | 2.8 |
| Headache | 3 | 8.3 | Dizziness | 9 | 25.0 |
| Irritability | 2 | 5.6 | Hallucination | 1 | 2.8 |
| Nausea/vomiting | 7 | 19.4 | Headache | 2 | 5.6 |
| Syncope | 17 | 47.2 | Loss of coordination | 5 | 13.9 |
| Weakness | 1 | 2.8 | Nausea/vomiting | 10 | 27.8 |
| Weakness | 6 | 16.7 | |||
| Total | 36 | 100 | 36 | 100 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luther, M.; Gardiner, F.W.; Hansen, C.; Caldicott, D. Hot of Not: Physiological versus Meteorological Heatwaves—Support for a Mean Temperature Threshold. Int. J. Environ. Res. Public Health 2016, 13, 753. https://doi.org/10.3390/ijerph13080753
Luther M, Gardiner FW, Hansen C, Caldicott D. Hot of Not: Physiological versus Meteorological Heatwaves—Support for a Mean Temperature Threshold. International Journal of Environmental Research and Public Health. 2016; 13(8):753. https://doi.org/10.3390/ijerph13080753
Chicago/Turabian StyleLuther, Matt, Fergus W. Gardiner, Claire Hansen, and David Caldicott. 2016. "Hot of Not: Physiological versus Meteorological Heatwaves—Support for a Mean Temperature Threshold" International Journal of Environmental Research and Public Health 13, no. 8: 753. https://doi.org/10.3390/ijerph13080753
APA StyleLuther, M., Gardiner, F. W., Hansen, C., & Caldicott, D. (2016). Hot of Not: Physiological versus Meteorological Heatwaves—Support for a Mean Temperature Threshold. International Journal of Environmental Research and Public Health, 13(8), 753. https://doi.org/10.3390/ijerph13080753