
BMI, Waist Circumference Reference Values for Chinese School-Aged Children and Adolescents

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Sample
2.2. Anthropometry
2.3. Statistical Analysis
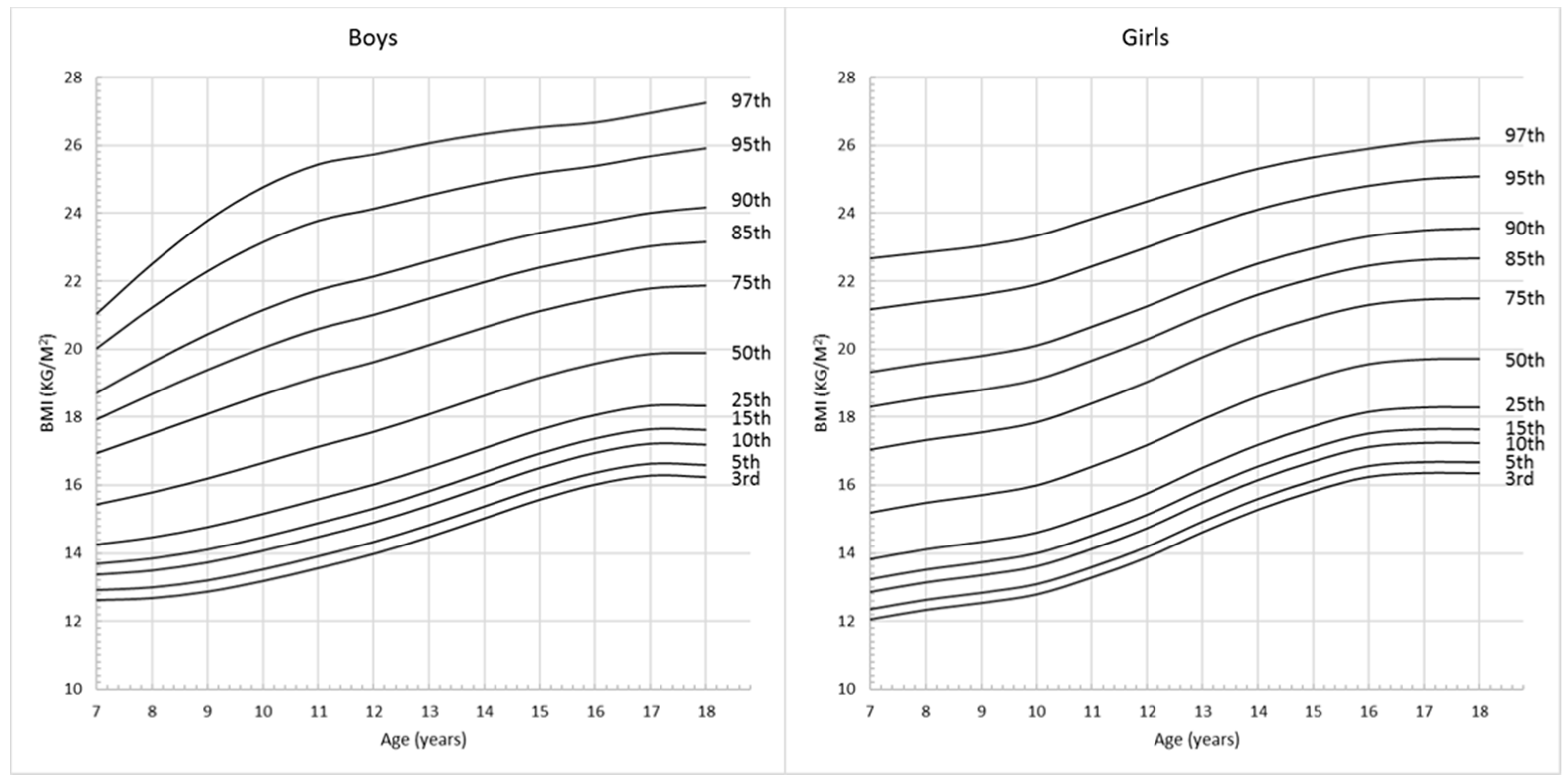
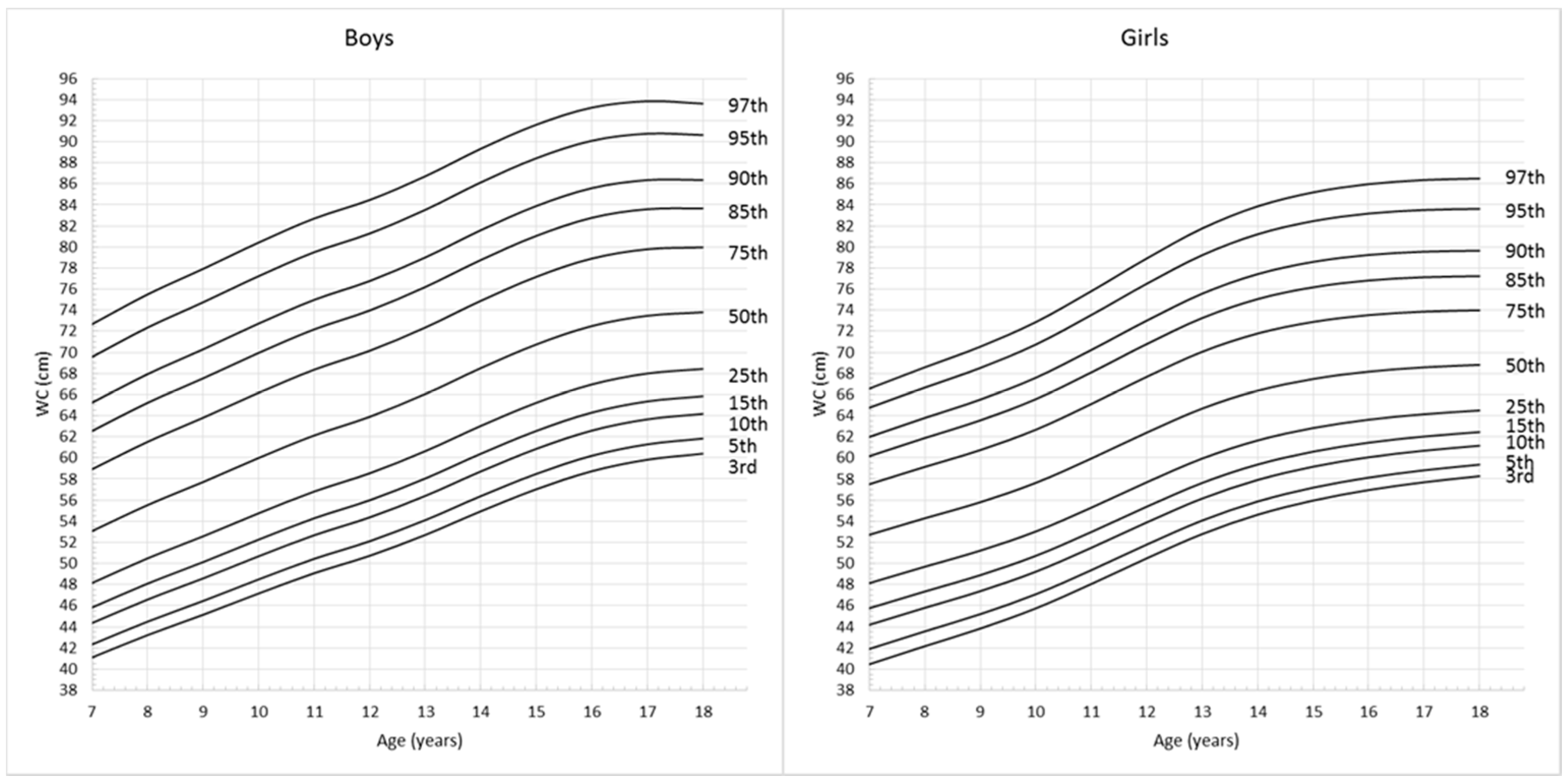
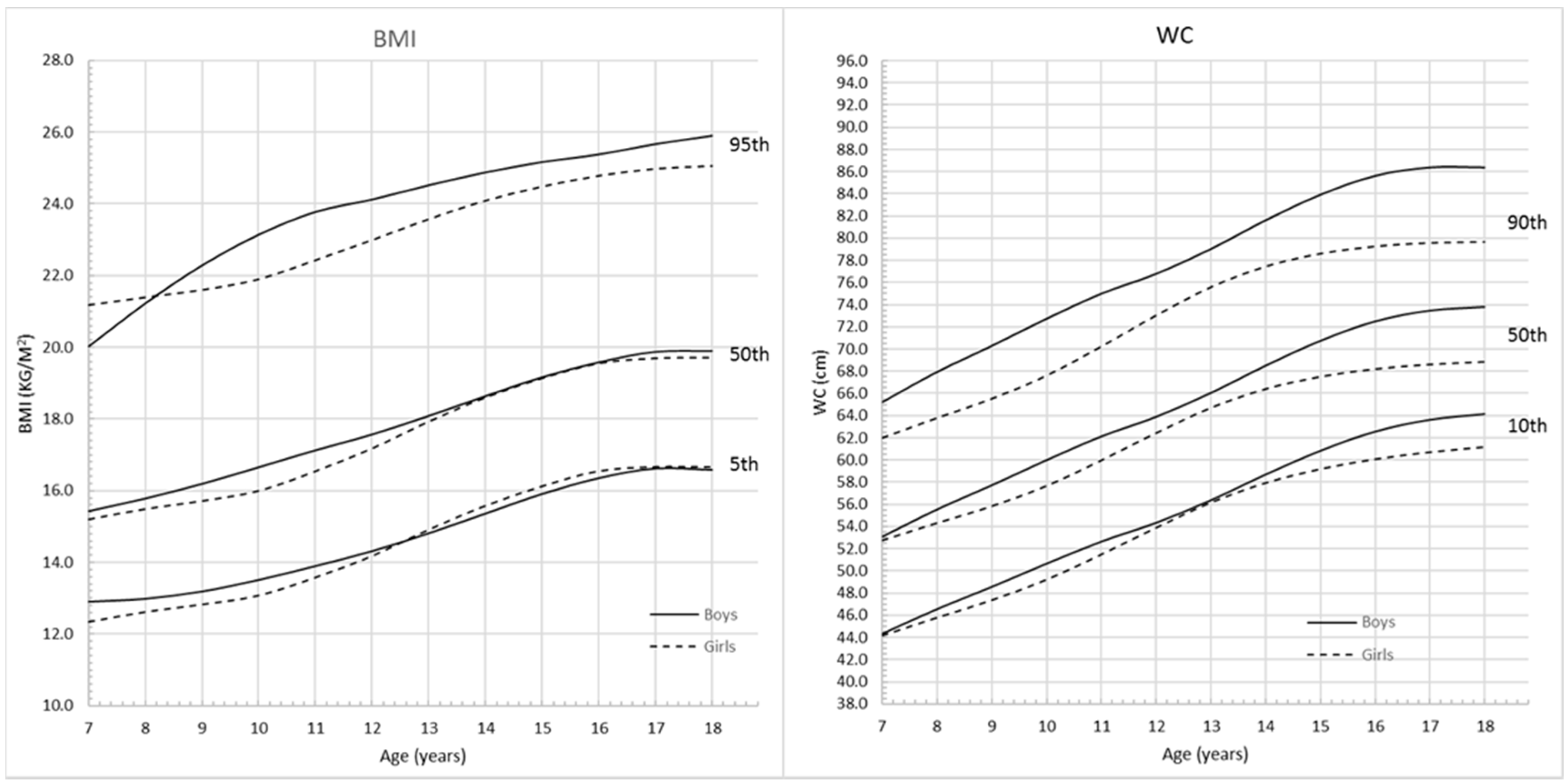
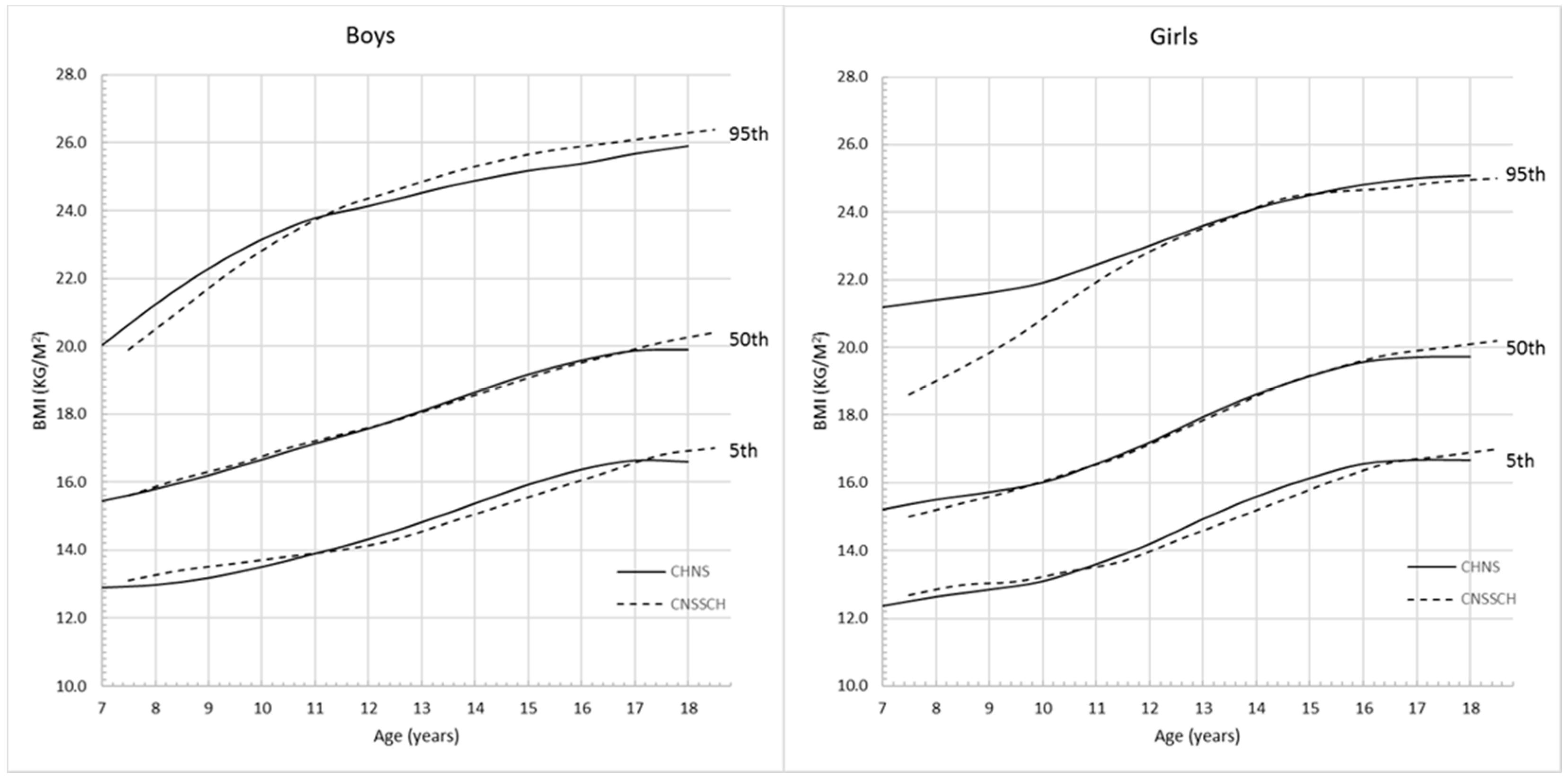
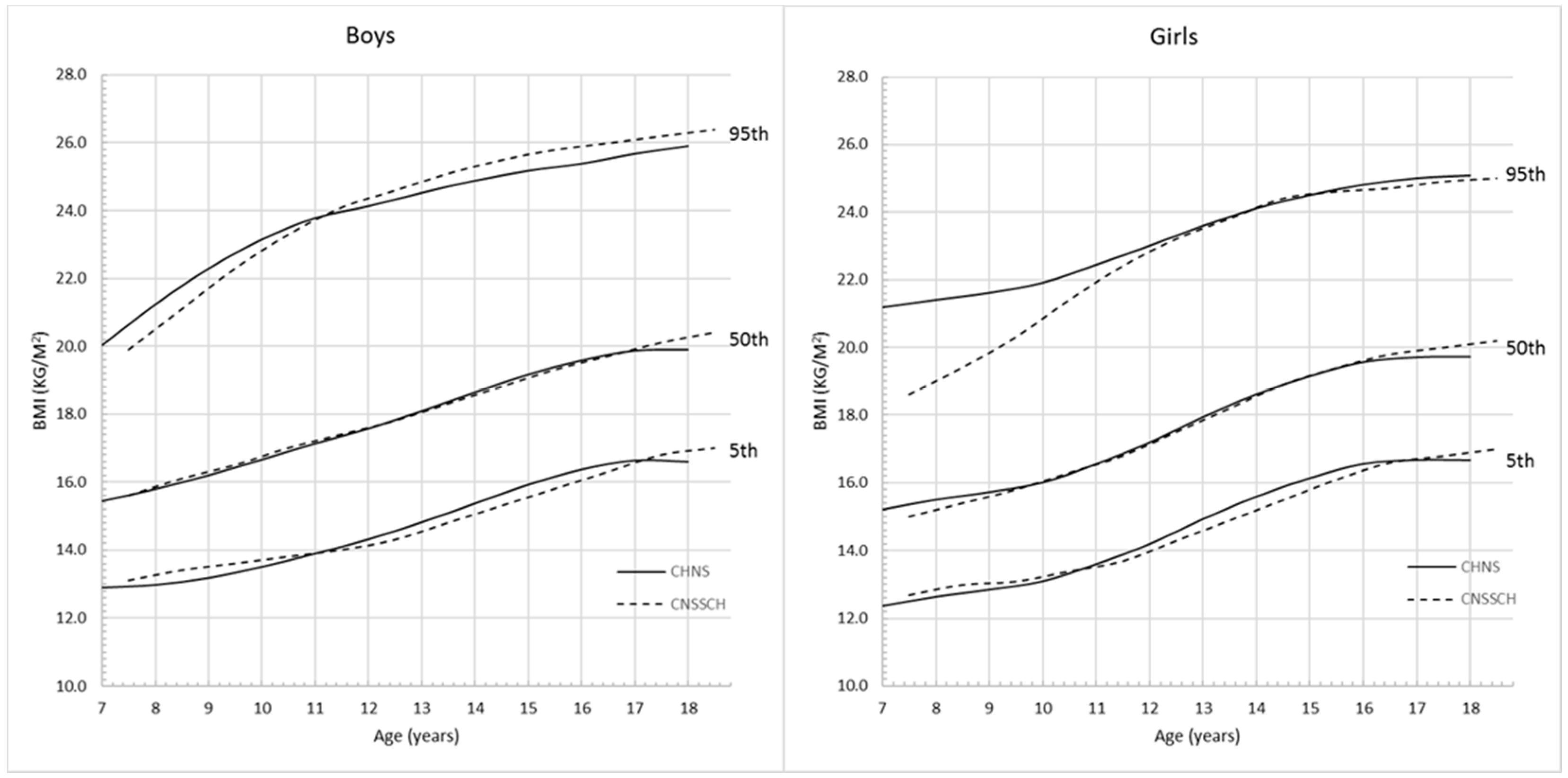
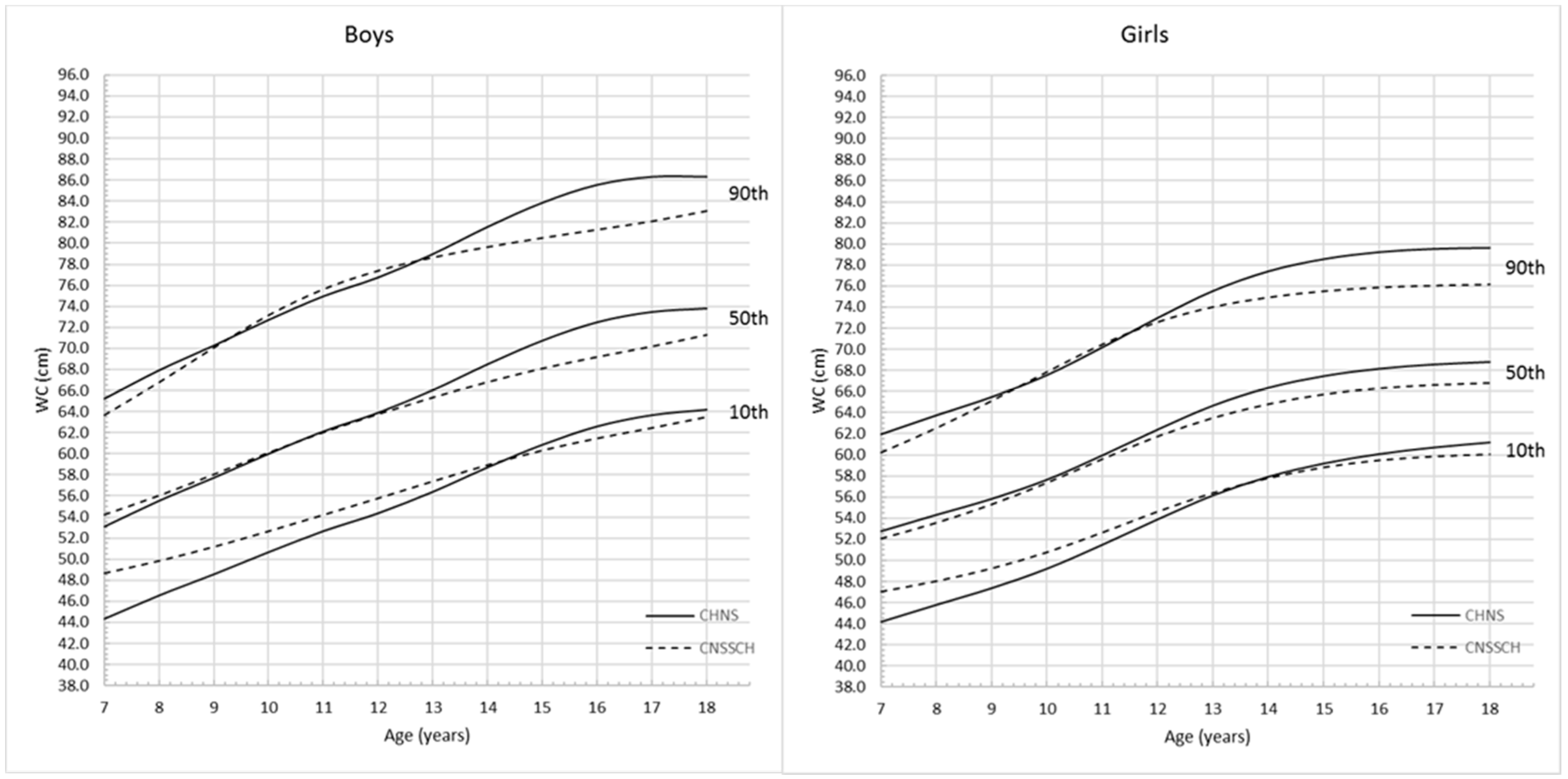
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
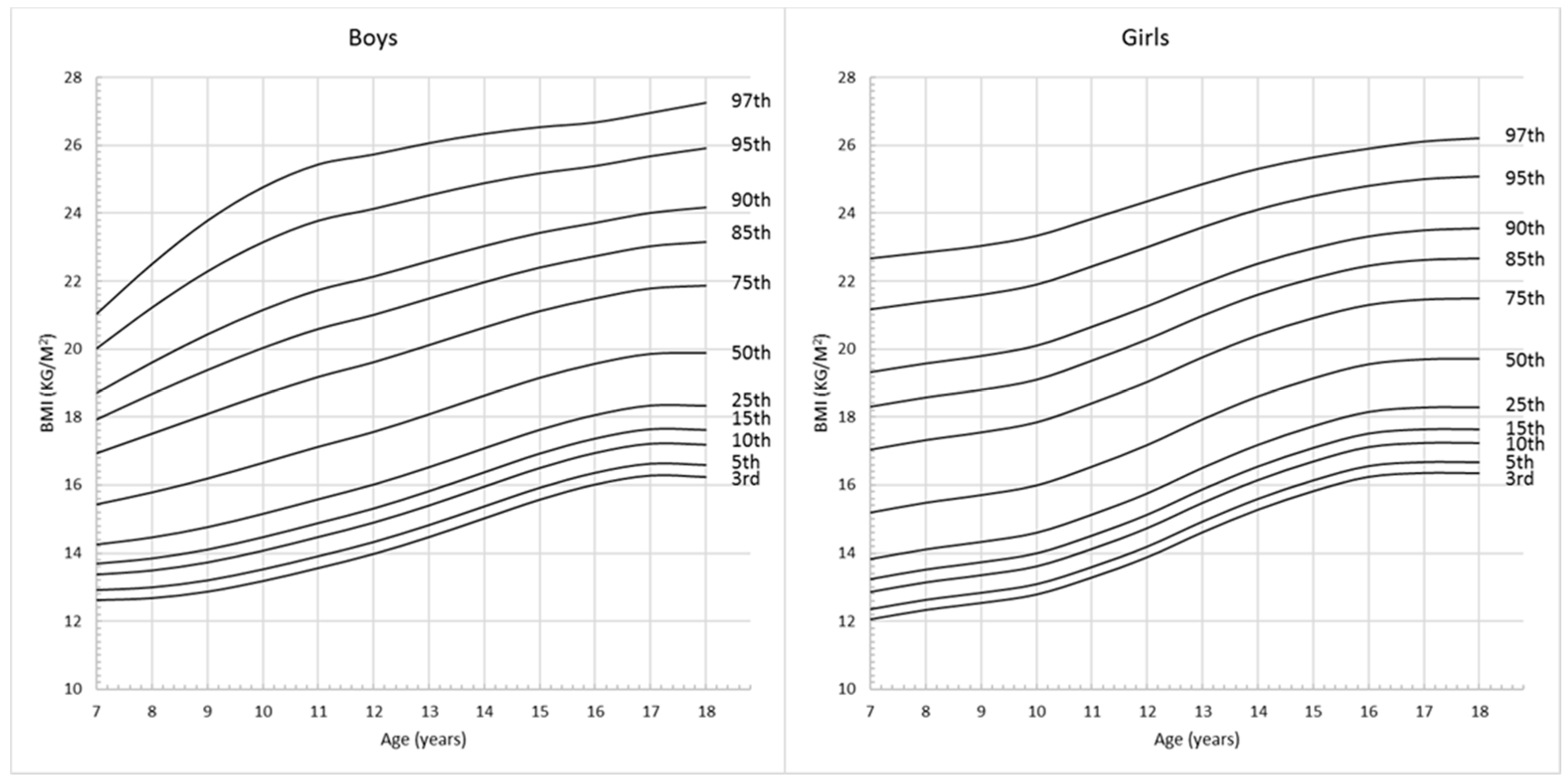
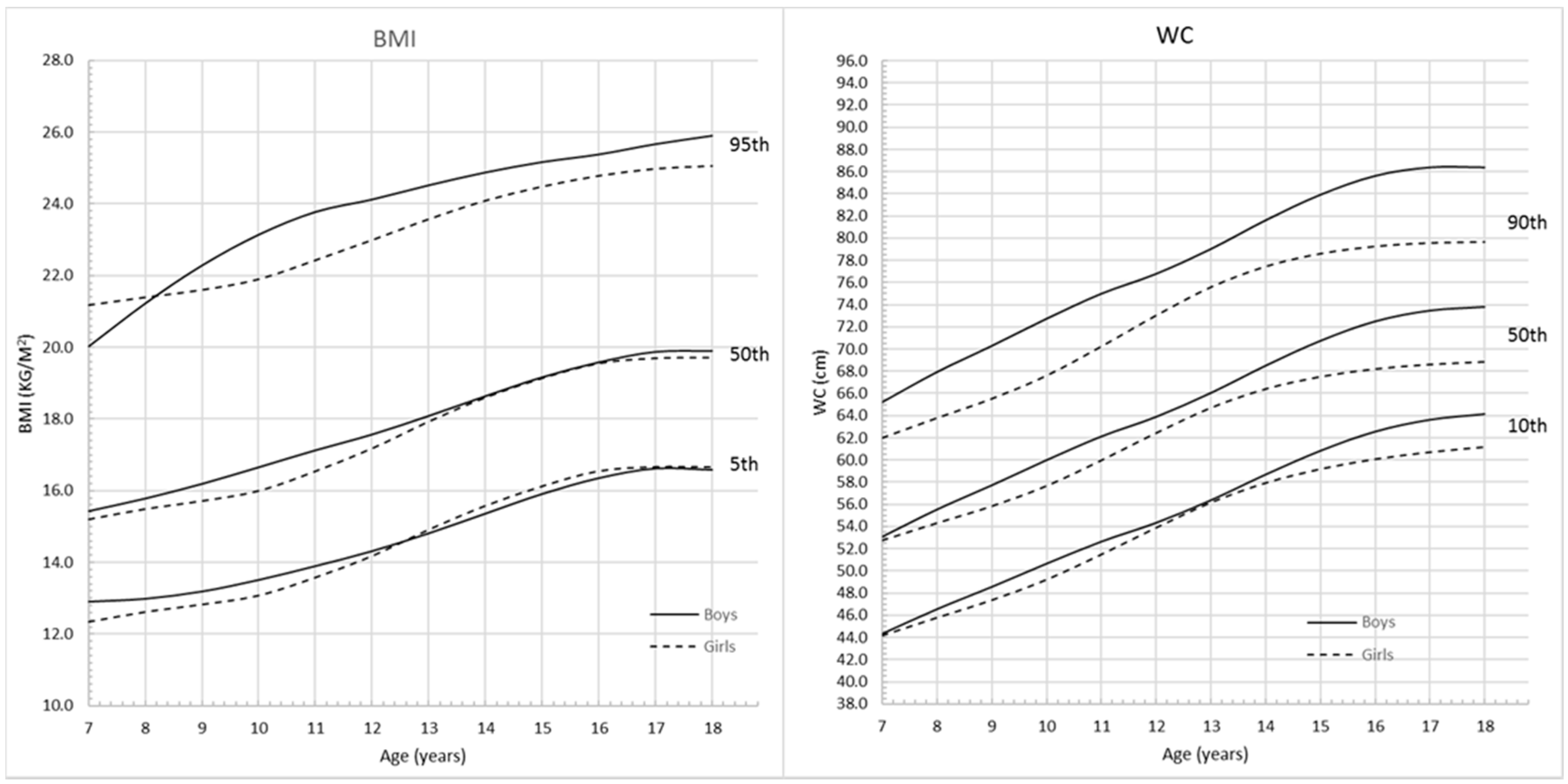
| BMI | Body Mass Index |
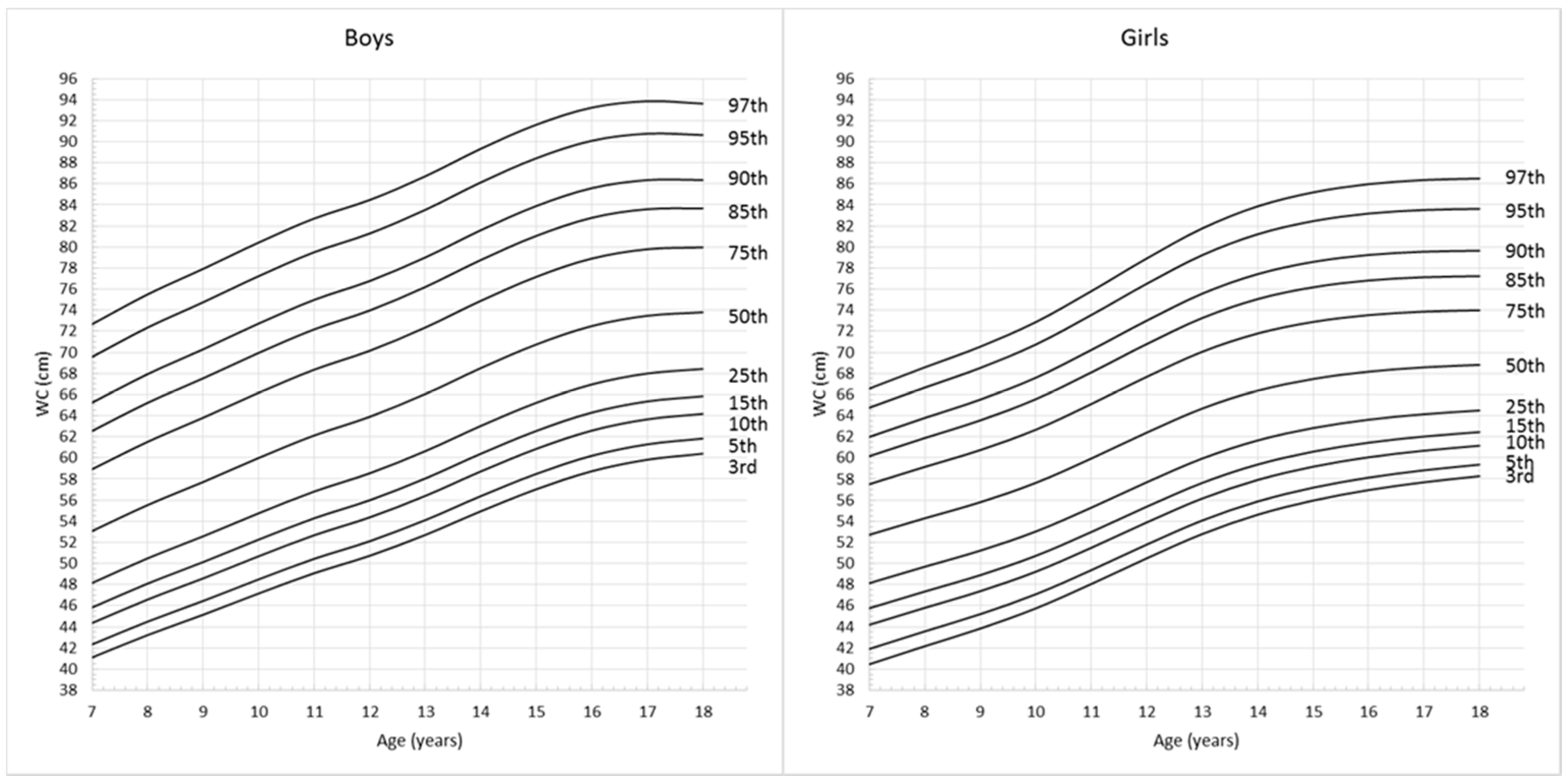
| WC | Waist Circumference |
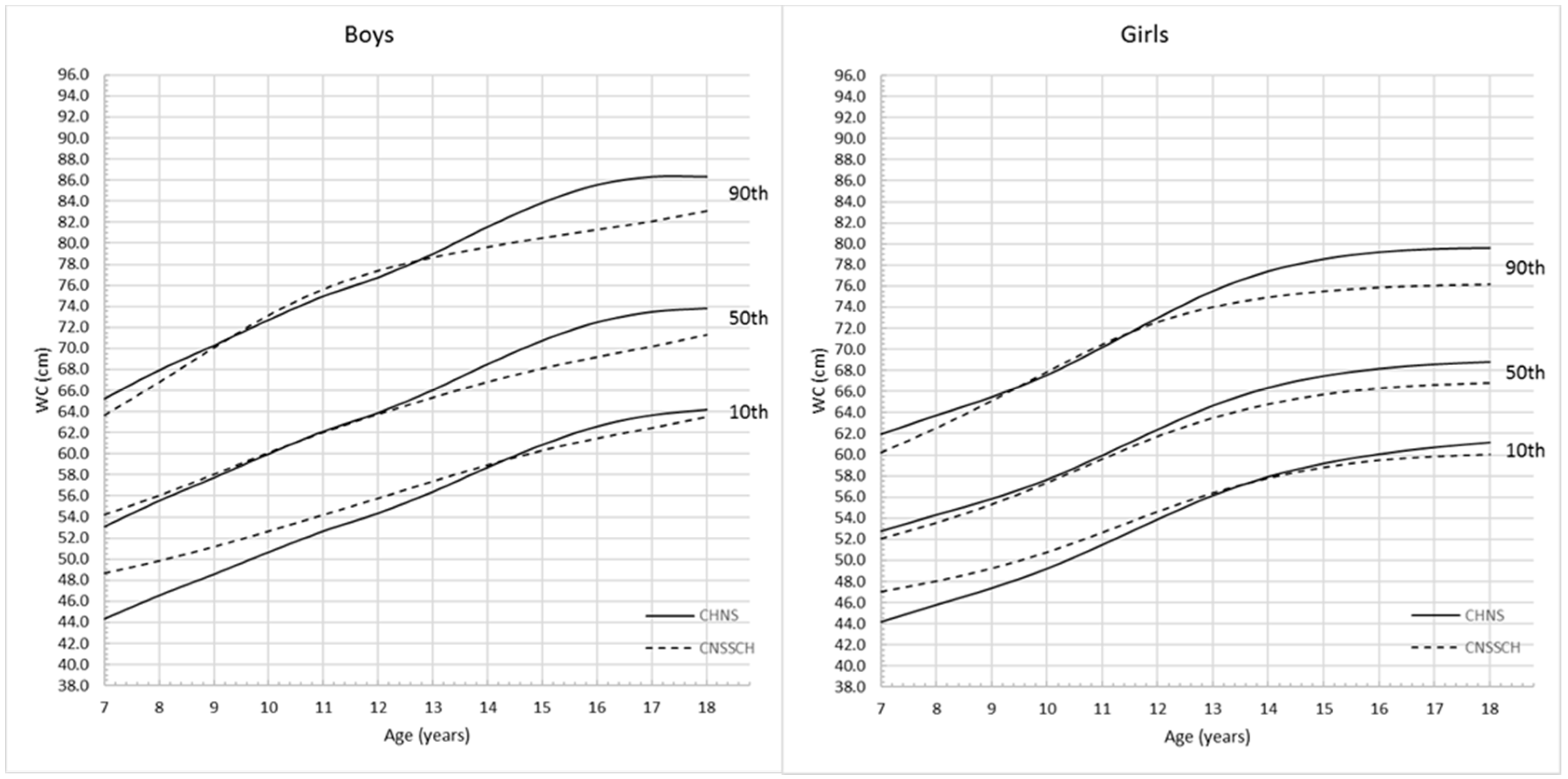
| CHNS | China Health and Nutrition Survey |
| LMS | Lambda-Mu-Sigma |
| CNSSCH | Chinese National Survey on Students’ Constitution and Health |
References
- Maggi, S.; Busetto, L.; Noale, M.; Limongi, F.; Crepaldi, G. Obesity: Definition and epidemiology. In Multidisciplinary Approach to Obesity; Springer: Heidelberg, Germany, 2015; pp. 31–39. [Google Scholar]
- Juni, M.H. Obesity: A public health threats in developing countries. Int. J. Public Health Clin. Sci. 2015, 2, 2. [Google Scholar]
- Commission on Ending Childhood Obesity. Report of the Commission on Ending Childhood Obesity; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- World Health Organization. Population-Based Approaches to Childhood Obesity Prevention; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- Sacks, G.; Shill, J.; Snowdon, W.; Swinburn, B.; Armstrong, T.; Irwin, R.; Randby, S.; Xuereb, G. Prioritizing Areas for Action in the Field of Population-Based Prevention of Childhood Obesity; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- Raj, M.; Kumar, R.K. Obesity in children & adolescents. Indian J. Med. Res. 2010, 132, 598. [Google Scholar] [PubMed]
- Lakshman, R.; Elks, C.E.; Ong, K.K. Childhood obesity. Circulation 2012, 126, 1770–1779. [Google Scholar] [CrossRef] [PubMed]
- Benson, T.; Shekar, M. Trends and issues in child undernutrition. In Disease and Mortality in Sub-Saharan Africa, 2nd ed.; Jamison, D.T., Feachem, R.G., Makgoba, M.W., Bos, E.R., Baingana, F.K., Hofman, K.J., Rogo, K.O., Eds.; World Bank: Washington, DC, USA, 2006. [Google Scholar]
- Ellulu, M.; Abed, Y.; Rahmat, A.; Ranneh, Y.; Ali, F. Epidemiology of obesity in developing countries: Challenges and prevention. Glob. Epidemic Obes. 2014, 2, 2. [Google Scholar] [CrossRef]
- Prentice, A.M. The emerging epidemic of obesity in developing countries. Int. J. Epidemiol. 2006, 35, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Onis, M.D.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef] [PubMed]
- Roberts, K.C.; Shields, M.; de Groh, M.; Aziz, A.; Gilbert, J.-A. Overweight and obesity in children and adolescents: Results from the 2009 to 2011 Canadian Health Measures Survey. Health Rep. 2012, 23, 37–41. [Google Scholar] [PubMed]
- Harrington, D.M.; Staiano, A.E.; Broyles, S.T.; Gupta, A.K.; Katzmarzyk, P.T. BMI percentiles for the identification of abdominal obesity and metabolic risk in children and adolescents: Evidence in support of the CDC 95th percentile. Eur. J. Clin. Nutr. 2013, 67, 218–222. [Google Scholar] [CrossRef] [PubMed]
- Alberti, K.G.M.; Zimmet, P.; Shaw, J.; IDF Epidemiology Task Force Consensus Group. The metabolic syndrome—A new worldwide definition. Lancet 2005, 366, 1059–1062. [Google Scholar] [CrossRef]
- McCarthy, H.D.; Ellis, S.M.; Cole, T.J. Central overweight and obesity in British youth aged 11–16 years: Cross sectional surveys of waist circumference. BMJ 2003, 326, 624. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Ford, E.S.; Mokdad, A.H.; Cook, S. Recent trends in waist circumference and waist-height ratio among U.S. children and adolescents. Pediatrics 2006, 118, e1390–e1398. [Google Scholar] [CrossRef] [PubMed]
- Fernández, J.R.; Redden, D.T.; Pietrobelli, A.; Allison, D.B. Waist circumference percentiles in nationally representative samples of African-American, European-American, and Mexican-American children and adolescents. J. Pediatr. 2004, 145, 439–444. [Google Scholar] [CrossRef] [PubMed]
- Bacopoulou, F.; Efthymiou, V.; Landis, G.; Rentoumis, A.; Chrousos, G.P. Waist circumference, waist-to-hip ratio and waist-to-height ratio reference percentiles for abdominal obesity among Greek adolescents. BMC Pediatr. 2015, 15, 1. [Google Scholar] [CrossRef] [PubMed]
- Hu, F. Obesity Epidemiology; Oxford University Press: New York, NY, USA, 2008. [Google Scholar]
- ÇİÇEK, B.; Öztürk, A.; Mazicioğlu, M.M.; Inanc, N.; Kurtoğlu, S. A novel cut-off for abdominal obesity derived from various anthropometric indices to predict body composition: Arm fat area. Turk. J. Med. Sci. 2010, 40, 515–523. [Google Scholar]
- Mushtaq, M.U.; Gull, S.; Abdullah, H.M.; Shahid, U.; Shad, M.A.; Akram, J. Waist circumference, waist-hip ratio and waist-height ratio percentiles and central obesity among Pakistani children aged five to twelve years. BMC Pediatr. 2011, 11, 1. [Google Scholar] [CrossRef] [PubMed]
- Sung, R.Y.; So, H.-K.; Choi, K.-C.; Nelson, E.A.; Li, A.M.; Yin, J.A.; Kwok, C.W.; Ng, P.-C.; Fok, T.-F. Waist circumference and waist-to-height ratio of Hong Kong Chinese children. BMC Public Health 2008, 8, 1. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Ji, C.-Y.; Zong, X.-N.; Zhang, Y.-Q. Body mass index growth curves for Chinese children and adolescents aged 0 to 18 years. Chin. J. Pediatr. 2009, 47, 493–498. [Google Scholar]
- Ma, J.; Wang, Z.; Song, Y.; Hu, P.; Zhang, B. BMI percentile curves for Chinese children aged 7–18 years, in comparison with the WHO and the U.S. Centers for Disease Control and Prevention references. Public Health Nutr. 2010, 13, 1990–1996. [Google Scholar] [CrossRef] [PubMed]
- Sung, R.; Yu, C.; Choi, K.; McManus, A.; Li, A.; Xu, S.; Chan, D.; Lo, A.; Chan, J.; Fok, T. Waist circumference and body mass index in Chinese children: Cutoff values for predicting cardiovascular risk factors. Int. J. Obes. 2007, 31, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Liu, A.; Hills, A.P.; Hu, X.; Li, Y.; Du, L.; Xu, Y.; Byrne, N.M.; Ma, G. Waist circumference cut-off values for the prediction of cardiovascular risk factors clustering in Chinese school-aged children: A cross-sectional study. BMC Public Health 2010, 10, 1. [Google Scholar] [CrossRef] [PubMed]
- Cheng-Ye, J.; Rita, Y.; Guan-Sheng, M.; Jun, M.; Zhong-Hu, H.; Tian-Jiao, C. Waist circumference distribution of Chinese school-age children and adolescents. Biomed. Environ. Sci. 2010, 23, 12–20. [Google Scholar]
- Ji, C.Y.; Cheng, T.O. Prevalence and geographic distribution of childhood obesity in China in 2005. Int. J. Cardiol. 2008, 131, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Khadilkar, V.; Yadav, S.; Agrawal, K.; Tamboli, S.; Banerjee, M.; Cherian, A.; Goyal, J.P.; Khadilkar, A.; Kumaravel, V.; Mohan, V. Revised IAP growth charts for height, weight and body mass index for 5- to 18-year-old Indian children. Indian Pediatr. 2015, 52, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Khadilkar, V.; Khadilkar, A. Growth charts: A diagnostic tool. Indian J. Endocrinol. Metab. 2011, 15, 166. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Zhai, F.; Du, S.; Popkin, B.M. The China health and nutrition survey, 1989–2011. Obes. Rev. 2014, 15, 2–7. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q. Smoking and body weight: Evidence from China health and nutrition survey. BMC Public Health 2015, 15, 1. [Google Scholar] [CrossRef] [PubMed]
- Jaacks, L.M.; Gordon-Larsen, P.; Mayer-Davis, E.J.; Adair, L.S.; Popkin, B. Age, period and cohort effects on adult body mass index and overweight from 1991 to 2009 in China: The China Health and Nutrition Survey. Int. J. Epidemiol. 2013, 42, 828–837. [Google Scholar] [CrossRef] [PubMed]
- The China Health and Nutrition Survey. Longitudinal Data Master Files. Available online: http://www.cpc.unc.edu/projects/china/data/datasets/longitudinal (accessed on 1 June 2016).
- Chen, C. Growth charts of Body Mass Index (BMI) with quantile regression. In Proceedings of the 2005 International Conference on Algorithmic Mathematics and Computer Science, Las Vegas, NV, USA, 20–23 June 2005; pp. 114–120.
- Xi, B.; He, D.; Hu, Y.; Zhou, D. Prevalence of metabolic syndrome and its influencing factors among the Chinese adults: The China Health and Nutrition Survey in 2009. Prev. Med. 2013, 57, 867–871. [Google Scholar] [CrossRef] [PubMed]
- Tudor-Locke, C.; Ainsworth, B.E.; Adair, L.; Du, S.; Popkin, B. Physical activity and inactivity in Chinese school-aged youth: The China Health and Nutrition Survey. Int. J. Obes. 2003, 27, 1093–1099. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Green, P.J. Smoothing reference centile curves: The LMS method and penalized likelihood. Stat. Med. 1992, 11, 1305–1319. [Google Scholar] [CrossRef] [PubMed]
- Bertino, E.; Gilli, G.; Occhi, L.; Giuliani, F.; Di Nicola, P.; Spada, E.; Fabris, C. Postnatal growth of preterm infants: Which reference charts? Minerva Pediatr. 2010, 62, 71–74. [Google Scholar] [PubMed]
- Kêkê, L.; Samouda, H.; Jacobs, J.; di Pompeo, C.; Lemdani, M.; Hubert, H.; Zitouni, D.; Guinhouya, B. Body mass index and childhood obesity classification systems: A comparison of the French, International Obesity Task Force (IOTF) and World Health Organization (WHO) references. Rev. Epidemiol. Sante Publique 2015, 63, 173–182. [Google Scholar] [CrossRef] [PubMed]
- Zogg, S.; Dürr, S.; Miedinger, D.; Steveling, E.H.; Maier, S.; Leuppi, J.D. Differences in classification of COPD patients into risk groups AD: A cross-sectional study. BMC Res. Notes 2014, 7, 562. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age | Boys (n = 2679) | Girls (n = 2383) | ||||
|---|---|---|---|---|---|---|
| n (%) | BMI (kg/m2) | WC (cm) | n (%) | BMI (kg/m2) | WC (cm) | |
| 7 (7.0–7.9) | 261 (9.74) | 15.8 (2.44) | 54.1 (7.33) | 203 (8.52) | 16.0 (3.71) | 52.9 (6.30) |
| 8 (8.0–8.9) | 223 (8.32) | 16.4 (3.00) | 57.0 (7.96) | 203 (8.52) | 16.1 (2.93) | 54.9 (6.76) |
| 9 (9.0–9.9) | 236 (8.81) | 16.8 (3.30) | 58.4 (7.55) | 241 (10.11) | 16.3 (3.11) | 56.1 (7.22) |
| 10 (10.0–10.9) | 257 (9.59) | 17.2 (3.15) | 60.9 (8.57) | 219 (9.19) | 16.5 (2.85) | 57.9 (7.62) |
| 11 (11.0–11.9) | 278 (10.38) | 18.0 (3.36) | 63.8 (9.29) | 239 (10.03) | 17.2 (2.98) | 60.8 (8.17) |
| 12 (12.0–12.9) | 235 (8.77) | 17.9 (2.89) | 64.2 (8.92) | 231 (9.69) | 17.7 (3.00) | 63.1 (8.46) |
| 13 (13.0–13.9) | 243 (9.07) | 18.8 (3.24) | 66.9 (8.82) | 211 (8.85) | 18.4 (2.58) | 65.4 (7.05) |
| 14 (14.0–14.9) | 231 (8.62) | 19.1 (2.96) | 69.7 (9.09) | 274 (11.50) | 19.1 (2.66) | 67.3 (8.10) |
| 15 (15.0–15.9) | 227 (8.47) | 19.8 (3.14) | 71.9 (10.25) | 186 (7.81) | 19.6 (2.70) | 68.3 (7.97) |
| 16 (16.0–16.9) | 212 (7.91) | 19.9 (2.62) | 73.3 (8.34) | 176 (7.39) | 19.9 (2.25) | 68.7 (6.88) |
| 17 (17.0–17.9) | 181 (6.76) | 20.4 (2.63) | 74.6 (8.88) | 132 (5.54) | 20.2 (2.76) | 69.6 (7.49) |
| 18 (18.0–18.9) | 95 (3.55) | 20.3 (2.98) | 74.2 (9.42) | 68 (2.85) | 20.0 (2.35) | 69.8 (7.96) |
| Total (7.0–18.9) | 2679 (100.00) | 18.2 (3.33) | 64.9 (10.89) | 2383 (100.00) | 17.9 (3.24) | 62.2 (9.42) |
| Age | Percentiles for Boys | Percentiles for Girls | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 3rd | 5th | 10th | 15th | 25th | 50th | 75th | 85th | 90th | 95th | 97th | 3rd | 5th | 10th | 15th | 25th | 50th | 75th | 85th | 90th | 95th | 97th | |
| 7 | 12.6 | 12.9 | 13.4 | 13.7 | 14.2 | 15.4 | 16.9 | 17.9 | 18.7 | 20.0 | 21.0 | 12.1 | 12.4 | 12.9 | 13.2 | 13.8 | 15.2 | 17.0 | 18.3 | 19.3 | 21.2 | 22.7 |
| 8 | 12.7 | 13.0 | 13.5 | 13.9 | 14.5 | 15.8 | 17.5 | 18.7 | 19.6 | 21.2 | 22.5 | 12.3 | 12.6 | 13.1 | 13.5 | 14.1 | 15.5 | 17.3 | 18.6 | 19.6 | 21.4 | 22.9 |
| 9 | 12.9 | 13.2 | 13.7 | 14.1 | 14.8 | 16.2 | 18.1 | 19.4 | 20.4 | 22.3 | 23.8 | 12.5 | 12.8 | 13.3 | 13.7 | 14.3 | 15.7 | 17.5 | 18.8 | 19.8 | 21.6 | 23.1 |
| 10 | 13.2 | 13.5 | 14.1 | 14.5 | 15.1 | 16.7 | 18.7 | 20.0 | 21.2 | 23.1 | 24.8 | 12.8 | 13.1 | 13.6 | 14.0 | 14.6 | 16.0 | 17.8 | 19.1 | 20.1 | 21.9 | 23.3 |
| 11 | 13.6 | 13.9 | 14.5 | 14.9 | 15.6 | 17.1 | 19.2 | 20.6 | 21.7 | 23.8 | 25.4 | 13.3 | 13.6 | 14.1 | 14.5 | 15.1 | 16.6 | 18.4 | 19.7 | 20.7 | 22.4 | 23.8 |
| 12 | 14.0 | 14.3 | 14.9 | 15.3 | 16.0 | 17.6 | 19.6 | 21.0 | 22.1 | 24.1 | 25.7 | 13.9 | 14.2 | 14.7 | 15.1 | 15.8 | 17.2 | 19.0 | 20.3 | 21.3 | 23.0 | 24.4 |
| 13 | 14.5 | 14.8 | 15.4 | 15.8 | 16.5 | 18.1 | 20.1 | 21.5 | 22.6 | 24.5 | 26.1 | 14.6 | 14.9 | 15.5 | 15.9 | 16.5 | 17.9 | 19.8 | 21.0 | 21.9 | 23.6 | 24.9 |
| 14 | 15.0 | 15.4 | 16.0 | 16.4 | 17.1 | 18.6 | 20.6 | 22.0 | 23.0 | 24.9 | 26.3 | 15.3 | 15.6 | 16.1 | 16.5 | 17.2 | 18.6 | 20.4 | 21.6 | 22.5 | 24.1 | 25.3 |
| 15 | 15.6 | 15.9 | 16.5 | 16.9 | 17.6 | 19.2 | 21.1 | 22.4 | 23.4 | 25.2 | 26.5 | 15.8 | 16.1 | 16.7 | 17.1 | 17.7 | 19.1 | 20.9 | 22.1 | 23.0 | 24.5 | 25.7 |
| 16 | 16.0 | 16.4 | 16.9 | 17.4 | 18.1 | 19.6 | 21.5 | 22.7 | 23.7 | 25.4 | 26.7 | 16.2 | 16.6 | 17.1 | 17.5 | 18.2 | 19.6 | 21.3 | 22.4 | 23.3 | 24.8 | 25.9 |
| 17 | 16.3 | 16.6 | 17.2 | 17.7 | 18.3 | 19.9 | 21.8 | 23.0 | 24.0 | 25.7 | 26.9 | 16.3 | 16.7 | 17.2 | 17.6 | 18.3 | 19.7 | 21.5 | 22.6 | 23.5 | 25.0 | 26.1 |
| 18 | 16.2 | 16.6 | 17.2 | 17.6 | 18.3 | 19.9 | 21.9 | 23.2 | 24.2 | 25.9 | 27.2 | 16.3 | 16.7 | 17.2 | 17.6 | 18.3 | 19.7 | 21.5 | 22.7 | 23.6 | 25.1 | 26.2 |
| Age | Percentiles for Boys | Percentiles for Girls | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 3rd | 5th | 10th | 15th | 25th | 50th | 75th | 85th | 90th | 95th | 97th | 3rd | 5th | 10th | 15th | 25th | 50th | 75th | 85th | 90th | 95th | 97th | |
| 7 | 41.1 | 42.3 | 44.4 | 45.8 | 48.2 | 53.1 | 58.9 | 62.6 | 65.2 | 69.6 | 72.7 | 40.5 | 41.9 | 44.2 | 45.8 | 48.1 | 52.7 | 57.5 | 60.2 | 62.0 | 64.8 | 66.6 |
| 8 | 43.2 | 44.5 | 46.6 | 48.1 | 50.5 | 55.5 | 61.5 | 65.2 | 67.9 | 72.4 | 75.5 | 42.2 | 43.6 | 45.8 | 47.4 | 49.7 | 54.3 | 59.2 | 61.9 | 63.8 | 66.7 | 68.6 |
| 9 | 45.2 | 46.5 | 48.6 | 50.1 | 52.6 | 57.7 | 63.8 | 67.5 | 70.3 | 74.8 | 77.9 | 43.8 | 45.2 | 47.4 | 48.9 | 51.2 | 55.8 | 60.7 | 63.6 | 65.5 | 68.5 | 70.5 |
| 10 | 47.2 | 48.5 | 50.7 | 52.3 | 54.8 | 60.0 | 66.2 | 70.0 | 72.7 | 77.2 | 80.4 | 45.8 | 47.1 | 49.2 | 50.7 | 53.0 | 57.6 | 62.7 | 65.6 | 67.6 | 70.7 | 72.9 |
| 11 | 49.1 | 50.4 | 52.7 | 54.3 | 56.8 | 62.1 | 68.4 | 72.2 | 75.0 | 79.5 | 82.7 | 48.1 | 49.4 | 51.5 | 53.0 | 55.3 | 59.9 | 65.1 | 68.1 | 70.2 | 73.5 | 75.8 |
| 12 | 50.7 | 52.1 | 54.4 | 56.0 | 58.5 | 63.9 | 70.2 | 74.0 | 76.8 | 81.3 | 84.5 | 50.5 | 51.8 | 53.9 | 55.4 | 57.7 | 62.4 | 67.7 | 70.8 | 73.0 | 76.5 | 78.9 |
| 13 | 52.7 | 54.1 | 56.4 | 58.0 | 60.6 | 66.0 | 72.4 | 76.2 | 79.0 | 83.5 | 86.7 | 52.8 | 54.1 | 56.2 | 57.6 | 59.9 | 64.7 | 70.1 | 73.3 | 75.6 | 79.2 | 81.8 |
| 14 | 54.9 | 56.4 | 58.7 | 60.4 | 63.0 | 68.5 | 74.9 | 78.8 | 81.6 | 86.1 | 89.3 | 54.6 | 55.9 | 57.9 | 59.4 | 61.7 | 66.4 | 71.8 | 75.1 | 77.4 | 81.2 | 83.9 |
| 15 | 57.0 | 58.5 | 60.9 | 62.5 | 65.2 | 70.7 | 77.2 | 81.1 | 83.9 | 88.4 | 91.6 | 56.0 | 57.2 | 59.2 | 60.6 | 62.8 | 67.5 | 72.9 | 76.2 | 78.6 | 82.5 | 85.2 |
| 16 | 58.7 | 60.2 | 62.6 | 64.3 | 67.0 | 72.5 | 78.9 | 82.8 | 85.6 | 90.1 | 93.2 | 57.0 | 58.1 | 60.1 | 61.4 | 63.6 | 68.2 | 73.5 | 76.8 | 79.3 | 83.2 | 86.0 |
| 17 | 59.8 | 61.3 | 63.7 | 65.3 | 68.0 | 73.5 | 79.8 | 83.6 | 86.4 | 90.8 | 93.8 | 57.7 | 58.8 | 60.7 | 62.0 | 64.1 | 68.6 | 73.9 | 77.1 | 79.6 | 83.5 | 86.4 |
| 18 | 60.4 | 61.8 | 64.2 | 65.8 | 68.4 | 73.8 | 80.0 | 83.7 | 86.4 | 90.6 | 93.6 | 58.3 | 59.4 | 61.2 | 62.4 | 64.5 | 68.8 | 74.0 | 77.2 | 79.7 | 83.6 | 86.5 |
| Gender | Prevalence of Overall Obesity (%) | Agreement of Prevalence by Different Cut-offs | |||
|---|---|---|---|---|---|
| CHNS | CNSSCH | p Value | κ | Agreement | |
| Boys | |||||
| 7 | 5.4 | 5.4 | 1.000 | 1.00 ** | almost perfect |
| 8 | 7.6 | 9.0 | 0.250 | 0.91 ** | almost perfect |
| 9 | 7.2 | 8.9 | 0.125 | 0.89 ** | almost perfect |
| 10 | 5.1 | 5.4 | 1.000 | 0.88 ** | almost perfect |
| 11 | 7.6 | 8.3 | 0.625 | 0.90 ** | almost perfect |
| 12 | 5.5 | 5.1 | 1.000 | 0.96 ** | almost perfect |
| 13 | 5.8 | 5.3 | 1.000 | 0.96 ** | almost perfect |
| 14 | 4.3 | 4.3 | 1.000 | 1.00 ** | almost perfect |
| 15 | 6.2 | 5.3 | 0.500 | 0.92 ** | almost perfect |
| 16 | 3.3 | 2.8 | 1.000 | 0.92 ** | almost perfect |
| 17 | 3.9 | 3.3 | 1.000 | 0.92 ** | almost perfect |
| 18 | 5.3 | 4.2 | 1.000 | 0.88 ** | almost perfect |
| Total (7–18) | 5.7 | 5.8 | 0.664 | 0.93 ** | almost perfect |
| Girls | |||||
| 7 | 7.4 | 14.3 | <0.001 * | 0.65 ** | substantial |
| 8 | 6.4 | 13.8 | <0.001 * | 0.60 ** | moderate |
| 9 | 5.4 | 11.2 | <0.001 * | 0.62 ** | substantial |
| 10 | 4.6 | 10.0 | <0.001 * | 0.60 ** | moderate |
| 11 | 4.2 | 6.3 | 0.063 | 0.79 ** | substantial |
| 12 | 6.9 | 7.8 | 0.625 | 0.87 ** | almost perfect |
| 13 | 3.8 | 3.8 | 1.000 | 1.00 ** | almost perfect |
| 14 | 4.7 | 5.1 | 1.000 | 0.96 ** | almost perfect |
| 15 | 3.8 | 4.3 | 1.000 | 0.93 ** | almost perfect |
| 16 | 3.4 | 3.4 | 1.000 | 1.00 ** | almost perfect |
| 17 | 4.5 | 6.1 | 0.500 | 0.85 ** | almost perfect |
| 18 | 1.5 | 1.5 | 1.000 | 1.00 ** | almost perfect |
| Total (7–18) | 5.0 | 7.7 | <0.001 * | 0.76 ** | substantial |
| Both genders | |||||
| 7 | 6.3 | 9.3 | <0.001 * | 0.79 ** | substantial |
| 8 | 7.0 | 11.3 | <0.001 * | 0.75 ** | substantial |
| 9 | 6.3 | 10.1 | <0.001 * | 0.75 ** | substantial |
| 10 | 4.8 | 7.6 | 0.001 * | 0.73 ** | substantial |
| 11 | 6.0 | 7.4 | 0.039 * | 0.86 ** | almost perfect |
| 12 | 6.2 | 6.4 | 1.000 | 0.91 ** | almost perfect |
| 13 | 4.8 | 4.6 | 1.000 | 0.98 ** | almost perfect |
| 14 | 4.6 | 4.8 | 1.000 | 0.98 ** | almost perfect |
| 15 | 5.1 | 4.8 | 1.000 | 0.92 ** | almost perfect |
| 16 | 3.4 | 3.1 | 1.000 | 0.96 ** | almost perfect |
| 17 | 4.2 | 4.5 | 1.000 | 0.88 ** | almost perfect |
| 18 | 3.7 | 3.1 | 1.000 | 0.91 ** | almost perfect |
| Total (7–18) | 5.3 | 6.7 | <0.001 * | 0.84 ** | almost perfect |
| Gender | Prevalence of Overall Obesity (%) | Agreement (κ) of Prevalence by Different Cut-offs | |||
|---|---|---|---|---|---|
| CHNS | CNSSCH | p Value | κ | Agreement | |
| Boys | |||||
| 7 | 3.8 | 7.3 | 0.004 * | 0.67 ** | substantial |
| 8 | 11.7 | 12.6 | 0.500 | 0.96 ** | almost perfect |
| 9 | 5.9 | 6.4 | 1.000 | 0.96 ** | almost perfect |
| 10 | 8.9 | 8.2 | 0.500 | 0.95 ** | almost perfect |
| 11 | 13.7 | 12.6 | 0.250 | 0.95 ** | almost perfect |
| 12 | 10.6 | 10.6 | 1.000 | 1.00 ** | almost perfect |
| 13 | 11.5 | 11.5 | 1.000 | 1.00 ** | almost perfect |
| 14 | 11.3 | 14.3 | 0.016 * | 0.86 ** | almost perfect |
| 15 | 12.3 | 16.3 | 0.004 * | 0.84 ** | almost perfect |
| 16 | 9.9 | 14.2 | 0.004 * | 0.80 ** | substantial |
| 17 | 8.8 | 16.6 | <0.001 * | 0.66 ** | substantial |
| 18 | 9.5 | 14.7 | 0.063 | 0.75 ** | substantial |
| Total (7–18) | 9.9 | 11.8 | <0.001 * | 0.88 ** | almost perfect |
| Girls | |||||
| 7 | 9.4 | 10.8 | 0.250 | 0.92 ** | almost perfect |
| 8 | 10.8 | 12.8 | 0.125 | 0.91 ** | almost perfect |
| 9 | 9.1 | 10.4 | 0.250 | 0.93 ** | almost perfect |
| 10 | 11.0 | 11.0 | 1.000 | 1.00 ** | almost perfect |
| 11 | 12.6 | 11.3 | 0.250 | 0.94 ** | almost perfect |
| 12 | 12.1 | 12.6 | 1.000 | 0.98 ** | almost perfect |
| 13 | 7.6 | 7.6 | 1.000 | 1.00 ** | almost perfect |
| 14 | 10.2 | 16.4 | <0.001 * | 0.73 ** | Substantial |
| 15 | 11.3 | 14.5 | 0.031 * | 0.86 ** | almost perfect |
| 16 | 5.7 | 13.1 | <0.001 * | 0.57 ** | moderate |
| 17 | 10.6 | 15.9 | 0.016 * | 0.77 ** | Substantial |
| 18 | 14.7 | 19.1 | 0.025 | 0.84 ** | almost perfect |
| Total (7–18) | 10.2 | 12.5 | <0.001 * | 0.88 ** | almost perfect |
| Both genders | |||||
| 7 | 6.3 | 8.8 | <0.001 * | 0.82 ** | almost perfect |
| 8 | 11.3 | 12.7 | 0.031 * | 0.93 ** | almost perfect |
| 9 | 7.5 | 8.4 | 0.125 | 0.94 ** | almost perfect |
| 10 | 9.9 | 9.5 | 0.500 | 0.98 ** | almost perfect |
| 11 | 13.2 | 12.0 | 0.031 * | 0.95 ** | almost perfect |
| 12 | 11.4 | 11.6 | 1.000 | 0.99 ** | almost perfect |
| 13 | 9.7 | 9.7 | 1.000 | 1.00 ** | almost perfect |
| 14 | 10.7 | 15.4 | <0.001 * | 0.79 ** | substantial |
| 15 | 11.9 | 15.5 | <0.001 * | 0.85 ** | almost perfect |
| 16 | 8.0 | 13.7 | <0.001 * | 0.71 ** | substantial |
| 17 | 9.6 | 16.3 | <0.001 * | 0.71 ** | substantial |
| 18 | 11.7 | 16.6 | 0.008 * | 0.80 ** | substantial |
| Total (7–18) | 10.0 | 12.1 | <0.001 * | 0.88 ** | almost perfect |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, P.; Li, X.; Gasevic, D.; Flores, A.B.; Yu, Z. BMI, Waist Circumference Reference Values for Chinese School-Aged Children and Adolescents. Int. J. Environ. Res. Public Health 2016, 13, 589. https://doi.org/10.3390/ijerph13060589
Song P, Li X, Gasevic D, Flores AB, Yu Z. BMI, Waist Circumference Reference Values for Chinese School-Aged Children and Adolescents. International Journal of Environmental Research and Public Health. 2016; 13(6):589. https://doi.org/10.3390/ijerph13060589
Chicago/Turabian StyleSong, Peige, Xue Li, Danijela Gasevic, Ana Borges Flores, and Zengli Yu. 2016. "BMI, Waist Circumference Reference Values for Chinese School-Aged Children and Adolescents" International Journal of Environmental Research and Public Health 13, no. 6: 589. https://doi.org/10.3390/ijerph13060589
APA StyleSong, P., Li, X., Gasevic, D., Flores, A. B., & Yu, Z. (2016). BMI, Waist Circumference Reference Values for Chinese School-Aged Children and Adolescents. International Journal of Environmental Research and Public Health, 13(6), 589. https://doi.org/10.3390/ijerph13060589