
Development and Validation of an Instrument Measuring Theory-Based Determinants of Monitoring Obesogenic Behaviors of Pre-Schoolers among Hispanic Mothers

Abstract
:1. Introduction
2. Methods
2.1. Planning Procedures for the IBM Instrument
2.2. Development of the IBM Instrument
2.3. Measuring the Validity and Reliability of the IBM Instrument
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Ogden, C.L.; Carroll, M.D.; Kit, B.K.; Flegal, K.M. Prevalence of childhood and adult obesity in the United States, 2011–2012. JAMA 2014, 311, 806–814. [Google Scholar] [CrossRef] [PubMed]
- Caprio, S.; Daniels, S.R.; Drewnowski, A.; Kaufman, F.R.; Palinkas, L.A.; Rosenbloom, A.L.; Schwimmer, J.B. Influence of race, ethnicity, and culture on childhood obesity: Implications for prevention and treatment a consensus statement of shaping America’s health and the obesity society. Diabetes Care 2008, 31, 2211–2221. [Google Scholar] [CrossRef] [PubMed]
- Davison, K.K.; Birch, L.L. Weight status, parent reaction, and self-concept in five-year-old girls. Pediatrics 2001, 107, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Bleich, S.N.; Segal, J.; Wu, Y.; Wilson, R.; Wang, Y. Systematic review of community-based childhood obesity prevention studies. Pediatrics 2013, 132, e201–e210. [Google Scholar] [CrossRef] [PubMed]
- Anzman, S.L.; Rollins, B.Y.; Birch, L.L. Parental influence on children’s early eating environments and obesity risk: implications for prevention. Int. J. Obes. 2010, 34, 1116–1124. [Google Scholar] [CrossRef] [PubMed]
- Knowlden, A.P.; Sharma, M. Systematic review of family and home-based interventions targeting paediatric overweight and obesity. Obes. Rev. 2012, 13, 499–508. [Google Scholar] [CrossRef] [PubMed]
- Fishbein, M.; Bandura, A.; Triandis, H.C.; Kanfer, P.H.; Becker, M.H.; Middlestadt, S.E.; Eichler, A. Factors influencing behavior and behavior change. In Handbook of Health Psychology; Baum, A., Revenson, T.A., Singer, J.E., Eds.; Lawrence Erlbaum: Mawah, NJ, USA, 2001; pp. 3–18. [Google Scholar]
- Emerging Theories in Health Promotion Practice and Research; DiClemente, R.J.; Crosby, R.A.; Kegler, M. (Eds.) John Wiley & Sons: New York, NY, USA, 2009.
- Fishbein, M.; Ajzen, I. Predicting and Changing Behavior: The Reasoned Action Approach; Taylor & Francis: New York, NY, USA, 2011. [Google Scholar]
- Sharma, M.; Petosa, R.L. Measurement and Evaluation for Health Educators; Jones & Bartlett: Sudbury, MA, USA, 2014. [Google Scholar]
- Sharma, M.; Branscum, P.; Atri, A. Introduction to Community and Public Health; Jossey-Bass: San Francisco, CA, USA, 2014. [Google Scholar]
- George, D.; Mallery, P. SPSS for Windows Step by Step Guide: A Simple Guide and Reference, 11.0 Update, 4th ed.; Allyn and Bacon: Boston, MA, USA, 2003. [Google Scholar]
- Schreiber, J.B.; Nora, A.; Stage, F.K.; Barlow, E.A.; King, J. Reporting structural equation modeling and confirmatory factor analysis results: A review. J. Educ. Res. 2006, 99, 323–338. [Google Scholar] [CrossRef]
- Marin, G.; Sabogal, F.; Marin, B.V.; Otero-Sabogal, R.; Perez-Stable, E.J. Development of a short acculturation scale for Hispanics. Hisp. J. Behav. Sci. 1987, 9, 183–205. [Google Scholar] [CrossRef]
- Marin, G.; VanOss Marin, B. Research with Hispanic Populations; SAGE Publications: Newbury Park, CA, USA, 2001. [Google Scholar]
- USDA Food and Nutrition Service. (November 25, 2015). Supplemental Nutrition Assistance Program-Eligibility. Available online: http://www.fns.usda.gov/snap/eligibility (accessed on 11 February 2016).
- Ventura, A.K.; Birch, L.L. Does parenting affect children’s eating and weight status? Int. J. Behav. Nutr. Phys. Act. 2008, 5. [Google Scholar] [CrossRef] [PubMed]
- Stang, J.; Loth, K.A. Parenting style and child feeding practices: Potential mitigating factors in the etiology of childhood obesity. J. Am. Diet. Assoc. 2011, 111, 1301–1305. [Google Scholar] [CrossRef] [PubMed]
- Patrick, H.; Hennessy, E.; McSpadden, K.; Oh, A. Parenting styles and practices in children’s obesogenic behaviors: Scientific gaps and future research directions. Child. Obes. 2013, 9, S-73–S-86. [Google Scholar] [CrossRef] [PubMed]
- Baumrind, D. Current patterns of parental authority. Dev. Psychol. 1997, 4, 1–103. [Google Scholar] [CrossRef]
- Maccoby, E.E.; Martin, J.A. Socialization in the context of the family: Parent-child interaction. In Handbook of Child Psychology: Formerly Carmichael’s Manual of Child Psychology; Paul Henry, M., Ed.; Wiley: New York, NY, USA, 1983. [Google Scholar]
- Michie, S.; West, R.; Campbell, R.; Brown, J.; Gainforth, H. ABC of Behavior Change Theories; Silverback Publishing: London, UK, 2014. [Google Scholar]
- Rao, G. Childhood obesity: Highlights of AMA expert committee recommendations. Am. Fam. Physician 2008, 78, 56–63. [Google Scholar] [PubMed]
- Crespo, N.C.; Elder, J.P.; Ayala, G.X.; Slyman, D.J.; Campbell, N.R.; Sallis, J.F.; McKenzie, T.L.; Baquero, B.; Arredondo, E.M. Results of a multi-level intervention to prevent and control childhood obesity among Latino children: The Aventuras Para Ninos Study. Ann. Behav. Med. 2012, 43, 84–100. [Google Scholar] [CrossRef] [PubMed]
- Conlon, B.A.; McGinn, A.P.; Lounsbury, D.W.; Diamantis, P.M.; Groisman-Perelstein, A.E.; Wylie-Rosett, J.; Isasi, C.R. The role of parenting practices in the home environment among underserved youth. Child. Obes. 2015, 11, 394–405. [Google Scholar] [CrossRef] [PubMed]
- Barry, A.E.; Chaney, B.; Piazza-Gardner, A.K.; Chavarria, E.A. Validity and reliability reporting practices in the field of health education and behavior: A review of seven journals. Health Educ. Behav. 2014, 41, 12–18. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
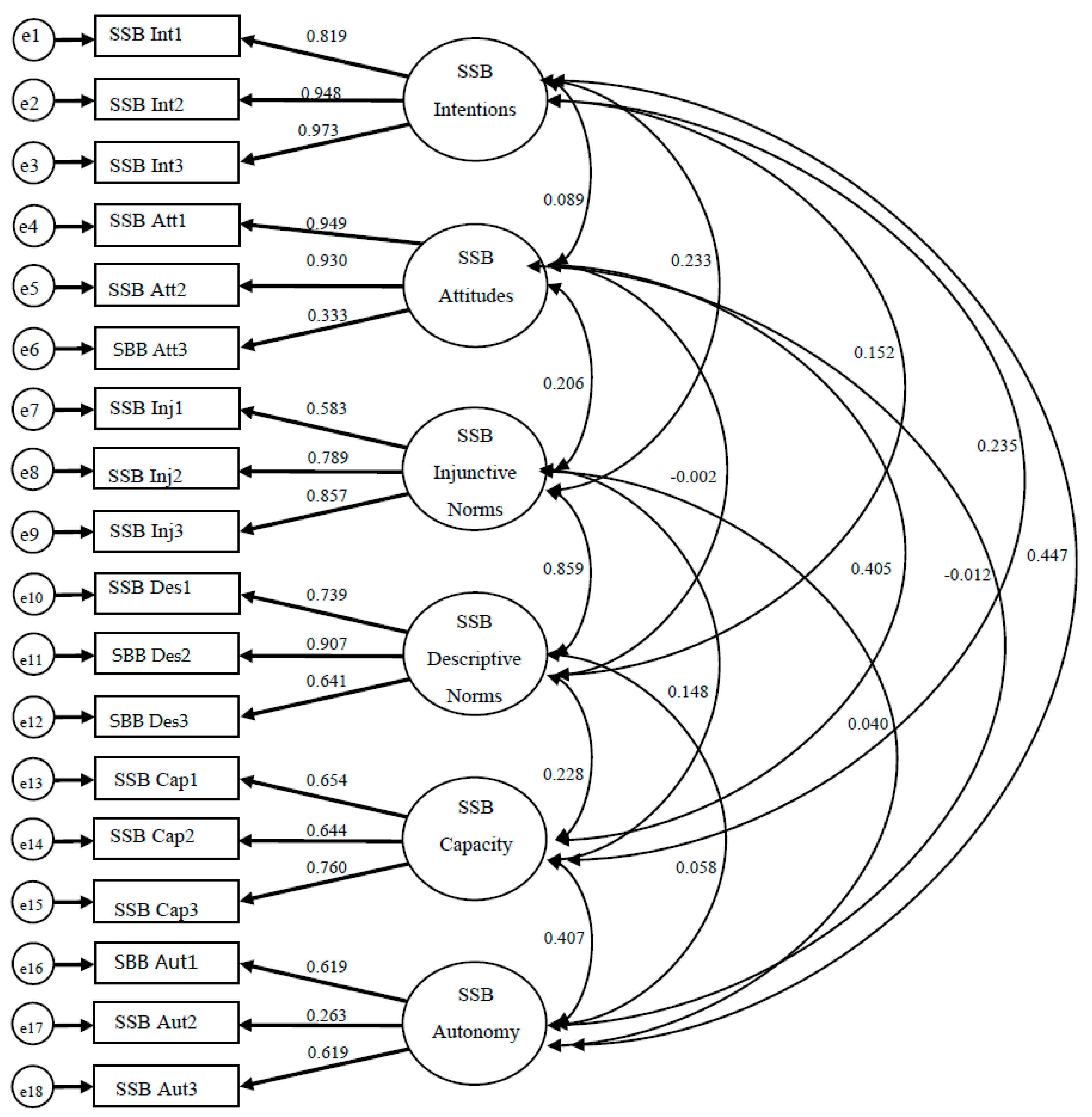
| Observed Variable | Latent Variable | β | B | SE |
|---|---|---|---|---|
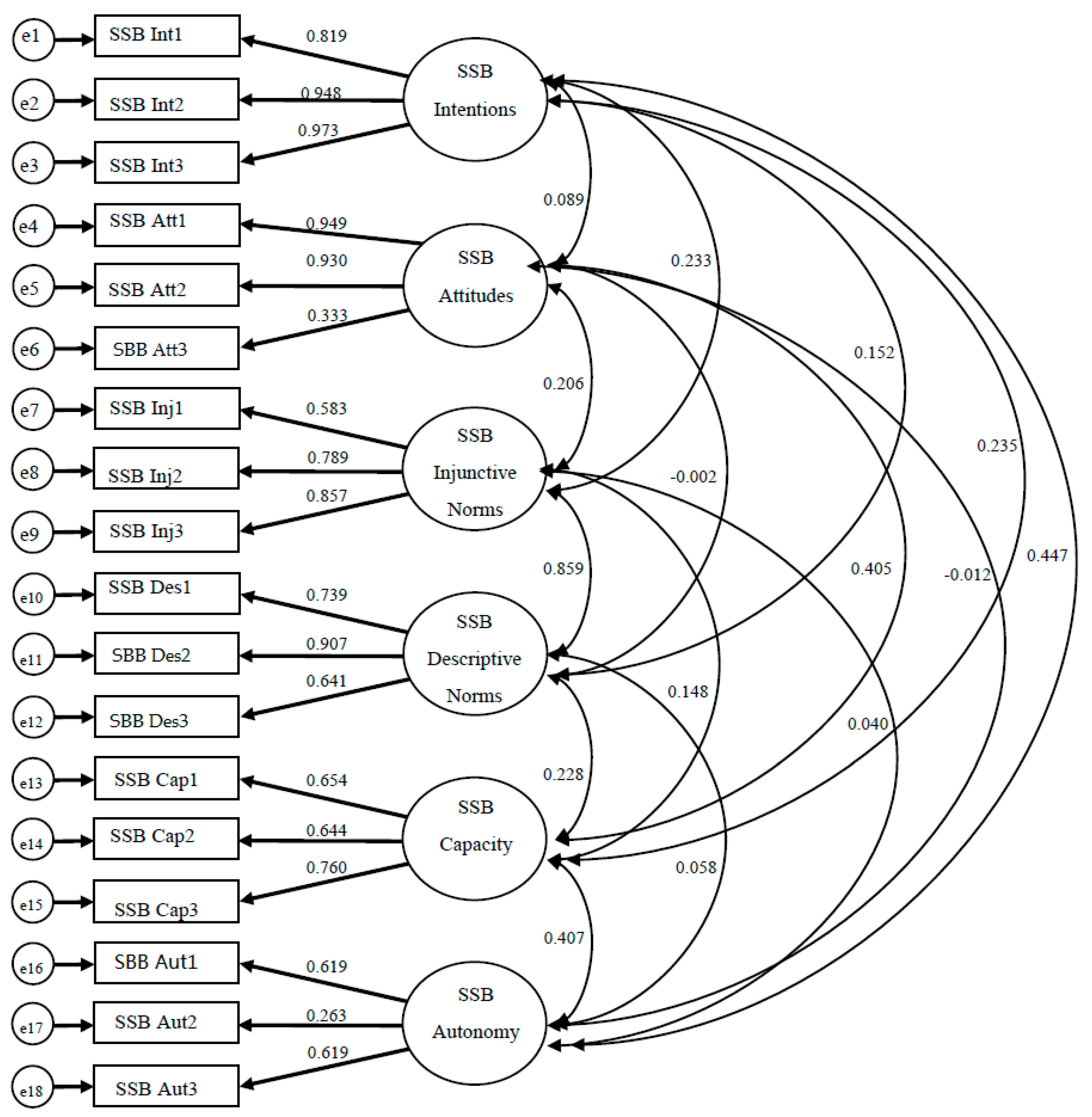
| I intend to do this behavior every time I feed my preschooler (SSB Int1 *) | SSB Intentions | 0.82 | 1 | |
| I will try to do this behavior every time I feed my preschooler (SSB Int2 *) | SSB Intentions | 0.95 | 1.19 | 0.06 |
| I will to do this behavior every time I feed my preschooler (SSB Int3 *) | SSB Intentions | 0.97 | 1.22 | 0.06 |
| Doing this behavior will help my preschooler… | ||||
| Not become overweight * My preschooler being overweight is <Extremely Bad/Extremely Good> a (SSB Att1 *) | SSB Attitudes | 0.95 | 1 | |
| Not develop diabetes * My preschooler developing diabetes is <Extremely Bad/Extremely Good> (SSB Att2 *) | SSB Attitudes | 0.93 | 1.03 | 0.07 |
| Have less sugar * My preschooler having less sugar is <Extremely Bad/Extremely Good>(SSB Att3 *) | SSB Attitudes | 0.33 | 0.33 | 0.07 |
| My husband/partner thinks I should do this * When it comes to feeding my preschooler | SSB Injunctive Norms | 0.58 | 1 | |
| I want to do what my husband/partner thinks I should do. (SSB Inj1 *) | ||||
| The grandparents of my preschooler thinks I should do this * When it comes to feeding my preschooler I want to do what the grandparents of my preschooler thinks I should do. (SSB Inj2 *) | SSB Injunctive Norms | 0.79 | 1.36 | 0.15 |
| My close family members thinks I should do this*When it comes to feeding my preschooler. I want to do what my close family members thinks I should do. (SSB Inj3 *) | SSB Injunctive Norms | 0.86 | 1.40 | 0.16 |
| Most stay at home mothers who do not work would do this * When it comes to feeding my preschooler I want to be like other stay at home mothers who also have preschoolers. (SSB Des1 *) | SSB Descriptive Norms | 0.74 | 1 | |
| My close family members who also have preschoolers would do this * When it comes to feeding my preschooler I want to be like my close family members who also have preschoolers (SSB Des2 *) | SSB Descriptive Norms | 0.91 | 1.12 | 0.09 |
| Other mothers who really care that their preschooler stays healthy would do this * When it comes to feeding my preschooler I want to be like other mothers who really care that their preschooler is healthy. (SSB Des3 *) | SSB Descriptive Norms | 0.64 | 0.94 | 0.10 |
| My preschooler gets sugary drinks if other people take care of him/her * If my preschooler is being taken care of by other people it makes harder. (SSB Cap1 *) | SSB Capacity | 0.65 | 1 | |
| If I’m at home, I give my preschooler sugary drinks * Being home with my preschooler most of the time makes it easier to do this behavior. (SSB Cap2 *) | SSB Capacity | 0.64 | 0.90 | 0.13 |
| My preschooler nags me about giving him/her sugary drinks * If my preschooler nags me about giving him/her sugary drinks it makes it harder for me to do this behavior. (SSB Cap3 *) | SSB Capacity | 0.76 | 1.19 | 0.14 |
| It is up to me for making sure my preschooler does this. (SSB Aut1 *) | SSB Autonomy | 0.62 | 1 | |
| How much control do you have for making sure your preschooler does this <No Control/Total Control> (SSB Aut2) | SSB Autonomy | 0.26 | 0.28 | 0.23 |
| Making sure my preschooler does this behavior is <Not up to my/Totally up to me> (SSB Aut3) | SSB Autonomy | 0.36 | 0.49 | 0.37 |
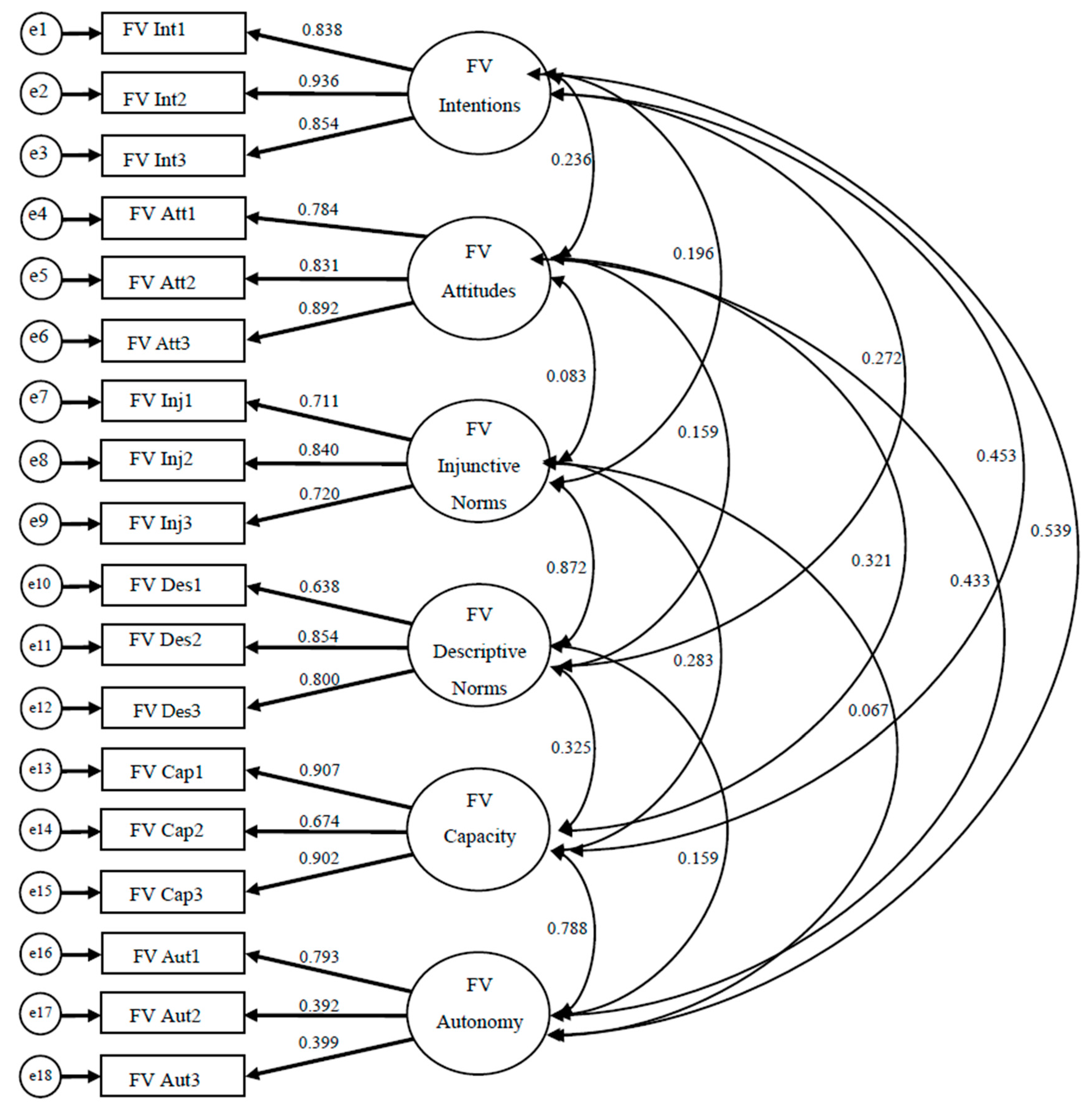
| Observed Variable | Latent Variable | β | B | SE |
|---|---|---|---|---|
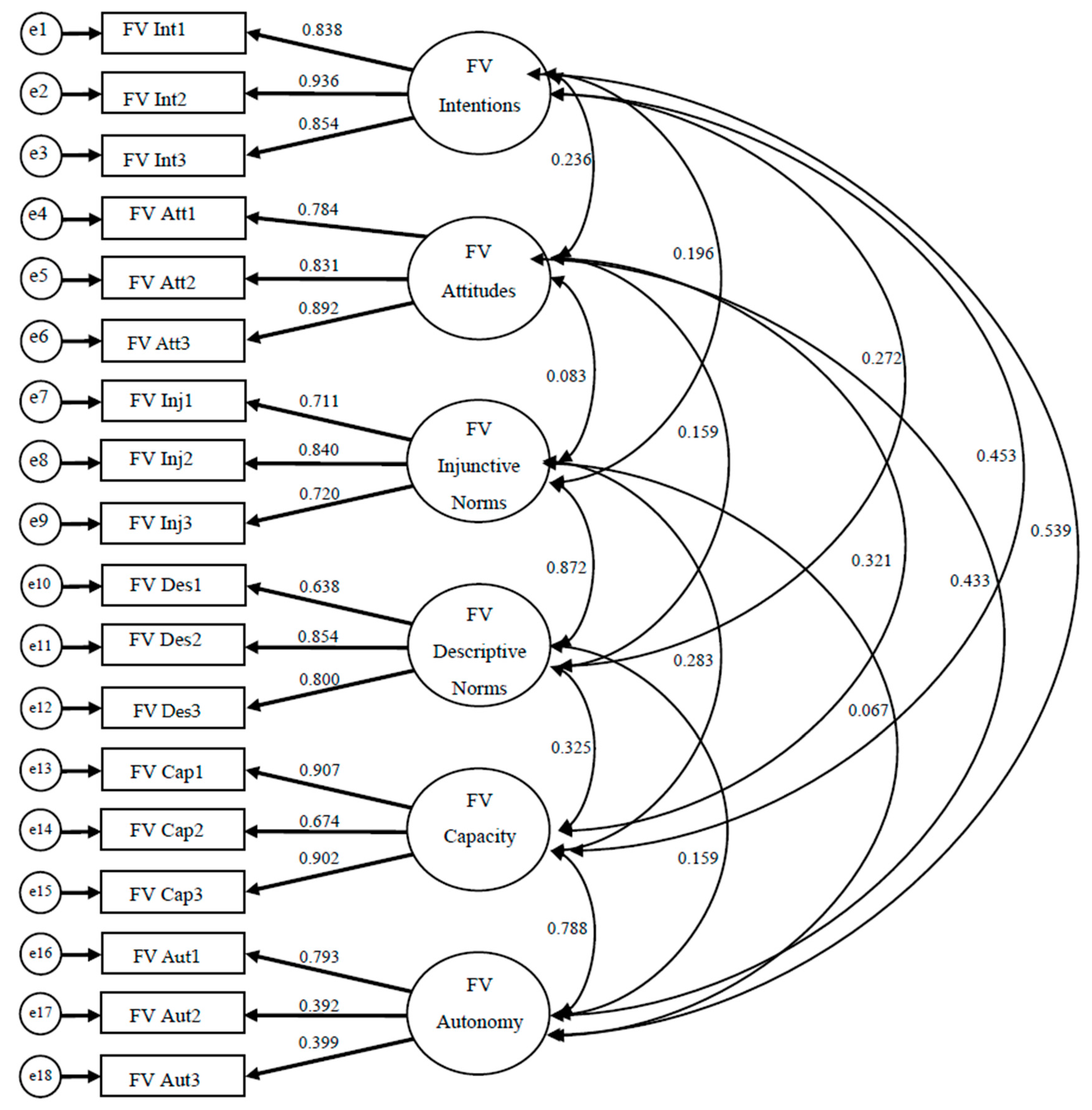
| I intend to do this behavior every time I feed my preschooler (FV Int1 *) | F/V Intentions | 0.84 | 1 | |
| I will try to do this behavior every time I feed my preschooler (FV Int2 *) | F/V Intentions | 0.94 | 1.12 | 0.062 |
| I will to do this behavior every time I feed my preschooler (FV Int3 *) | F/V Intentions | 0.85 | 1.03 | 0.064 |
| Doing this behavior will help my preschooler… | ||||
| Be healthy * My preschooler being healthy is <Extremely Bad/Extremely Good> (FV Att1 *) | F/V Attitudes | 0.78 | 1 | |
| Develop properly * My preschooler developing properly is <Extremely Bad/Extremely Good> (FV Att2 *) | F/V Attitudes | 0.83 | 1.19 | 0.089 |
| Get all the nutrients he/she needs * My preschooler getting the nutrients he/she needs is <Extremely Bad/Extremely Good> (FV Att3 *) | F/V Attitudes | 0.89 | 1.15 | 0.084 |
| My husband/partner thinks I should do this * When it comes to feeding my preschooler | F/V Injunctive Norms | 0.71 | 1 | |
| I want to do what my husband/partner thinks I should do. (FV Inj1 *) | ||||
| The grandparents of my preschooler thinks I should do this * When it comes to feeding my preschooler I want to do what the grandparents of my preschooler thinks I should do. (FV Inj2 *) | F/V Injunctive Norms | 0.84 | 1.10 | 0.10 |
| My close family members thinks I should do this*When it comes to feeding my preschooler | F/V Injunctive Norms | 0.72 | 1.03 | 0.10 |
| I want to do what my close family members thinks I should do. (FV Inj3 *) | ||||
| Most stay at home mothers who do not work would do this * When it comes to feeding my preschooler I want to be like other stay at home mothers who also have preschoolers. (FV Des1 *) | F/V Descriptive Norms | 0.64 | 1 | |
| My close family members who also have preschoolers would do this * When it comes to feeding my preschooler I want to be like my close family members who also have preschoolers (FV Des2 *) | F/V Descriptive Norms | 0.85 | 1.32 | 0.13 |
| Other mothers who really care that their preschooler stays healthy would do this * When it comes to feeding my preschooler I want to be like other mothers who really care that their preschooler is healthy. (FV Des3 *) | F/V Descriptive Norms | 0.80 | 1.22 | 0.13 |
| I my preschooler to do this behavior * Encouraging my preschooler makes it easier for me to do this. (FV Cap1 *) | F/V Capacity | 0.67 | 1 | |
| I pay close attention to what my preschooler eat when I am with him/her * Paying close attention to what my preschooler eat makes it easier for me to do this. (FV Cap2 *) | F/V Capacity | 0.91 | 1.04 | 0.09 |
| I plan to be with my preschooler when he/she eats meals when possible * Being with my preschooler | F/V Capacity | 0.90 | 1.09 | 0.09 |
| When he/she eat meals makes it easier for me to do this. (FV Cap3 *) | ||||
| It is up to me for making sure my preschooler does this. (FV Aut1 *) | F/V Autonomy | 0.79 | 1 | |
| How much control do you have for making sure your preschooler does this <No Control/Total Control> FV Aut2 *) | F/V Autonomy | 0.39 | 0.50 | 0.10 |
| Making sure my preschooler does this behavior is <Not up to my/Totally up to me> (FV Aut3 *) | F/V Autonomy | 0.40 | 0.45 | 0.08 |
| SSB Instrument | |||||||
|---|---|---|---|---|---|---|---|
| FV Instrument | 1 | 2 | 3 | 4 | 5 | 6 | |
| Intentions | - | 0.089 | 0.233 | 0.152 | 0.235 | 0.447 | |
| Attitudes | 0.236 | - | 0.206 | −0.002 | 0.405 | −0.012 | |
| In. Norms | 0.196 | 0.083 | - | 0.859 | 0.148 | 0.040 | |
| Des. Norms | 0.272 | 0.159 | 0.872 | - | 0.228 | 0.058 | |
| Capacity | 0.453 | 0.321 | 0.283 | 0.325 | - | 0.407 | |
| Autonomy | 0.539 | 0.433 | 0.067 | 0.159 | 0.788 | - | |
| Theoretical Construct | Cronbach’s α |
|---|---|
| Fruit and Vegetables (F/V) | |
| Intentions | 0.91 |
| Attitudes towards the behavior | 0.87 |
| Injunctive Norms | 0.80 |
| Descriptive Norms | 0.80 |
| Capacity | 0.85 |
| Autonomy | 0.59 |
| Sugar Sweetened Beverages (SSB) | |
| Intentions | 0.94 |
| Attitudes towards the behavior | 0.76 |
| Injunctive Norms | 0.79 |
| Descriptive Norms | 0.80 |
| Capacity | 0.72 |
| Autonomy | 0.41 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Branscum, P.; Lora, K.R. Development and Validation of an Instrument Measuring Theory-Based Determinants of Monitoring Obesogenic Behaviors of Pre-Schoolers among Hispanic Mothers. Int. J. Environ. Res. Public Health 2016, 13, 554. https://doi.org/10.3390/ijerph13060554
Branscum P, Lora KR. Development and Validation of an Instrument Measuring Theory-Based Determinants of Monitoring Obesogenic Behaviors of Pre-Schoolers among Hispanic Mothers. International Journal of Environmental Research and Public Health. 2016; 13(6):554. https://doi.org/10.3390/ijerph13060554
Chicago/Turabian StyleBranscum, Paul, and Karina R. Lora. 2016. "Development and Validation of an Instrument Measuring Theory-Based Determinants of Monitoring Obesogenic Behaviors of Pre-Schoolers among Hispanic Mothers" International Journal of Environmental Research and Public Health 13, no. 6: 554. https://doi.org/10.3390/ijerph13060554
APA StyleBranscum, P., & Lora, K. R. (2016). Development and Validation of an Instrument Measuring Theory-Based Determinants of Monitoring Obesogenic Behaviors of Pre-Schoolers among Hispanic Mothers. International Journal of Environmental Research and Public Health, 13(6), 554. https://doi.org/10.3390/ijerph13060554