
Effects of Short-Term Exposure to Particulate Air Pollutants on the Inflammatory Response and Respiratory Symptoms: A Panel Study in Schoolchildren from Rural Areas of Japan

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.1.1. Recording of Daily Respiratory Symptoms
2.1.2. Measurement of Air Pollutant Levels
2.1.3. Preparation of Airborne Particles
2.1.4. Cell Culture and Measurement of IL-6, IL-8, and TNF-α Production
2.2. Statistical Analysis
3. Results
3.1. Subject Characteristics
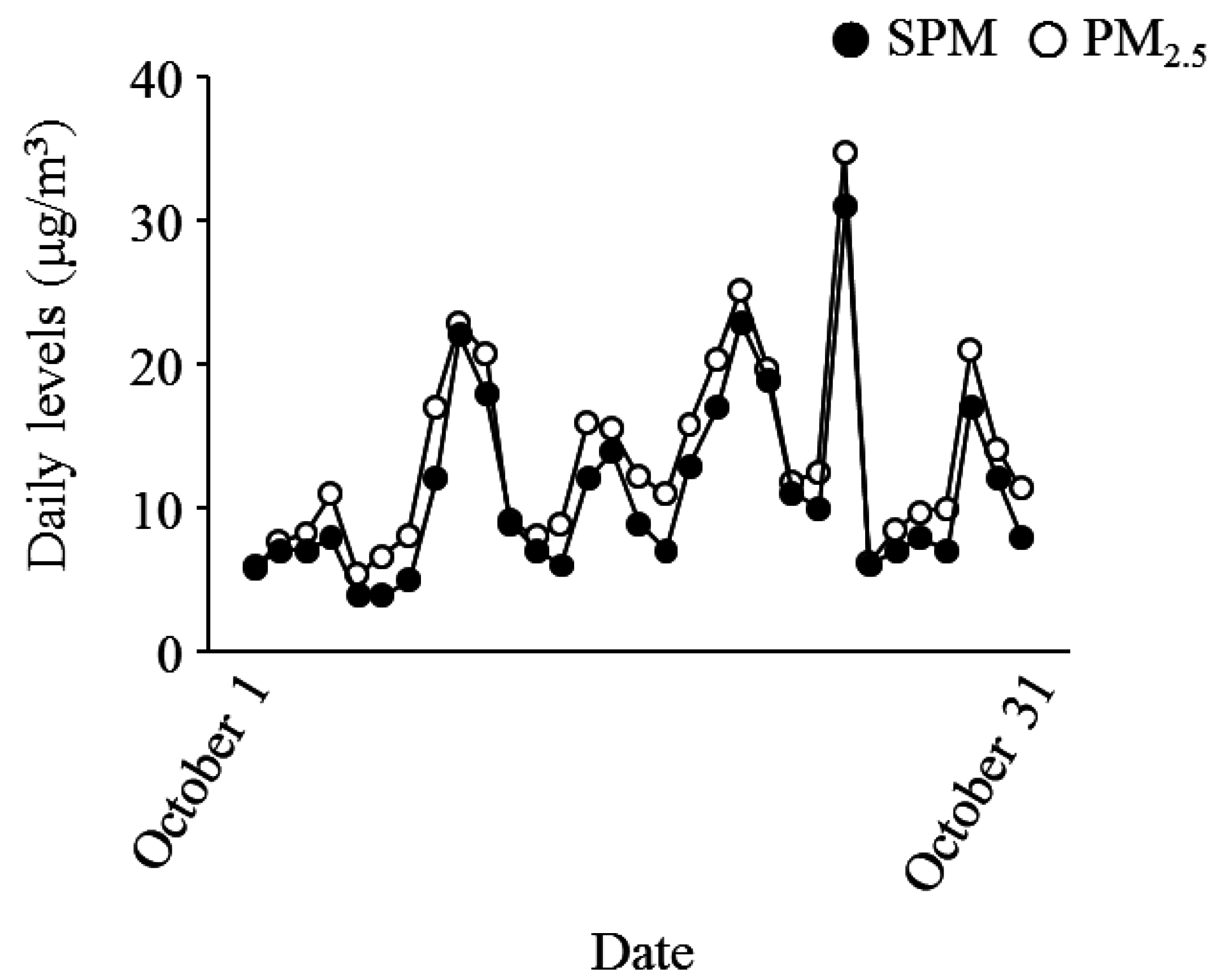
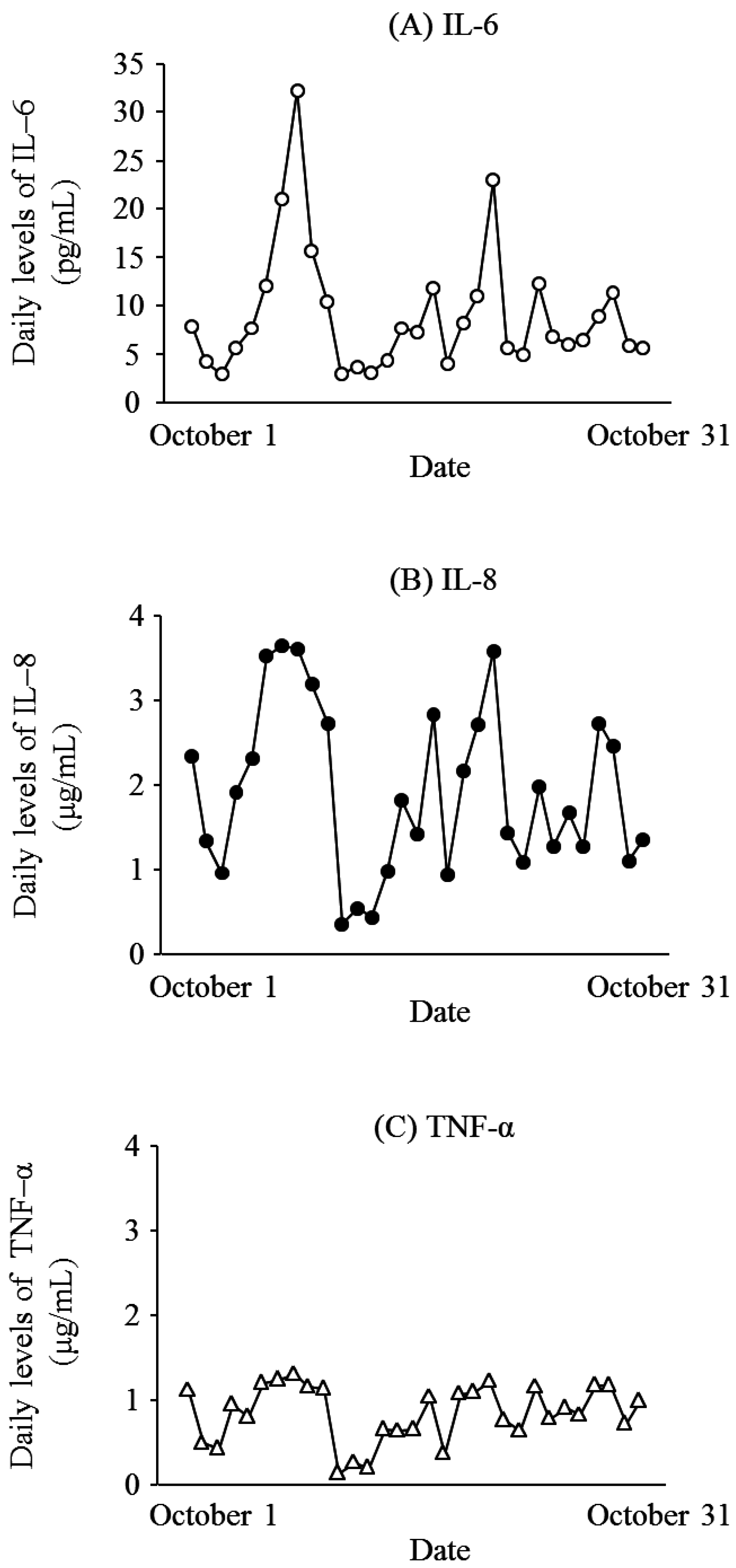
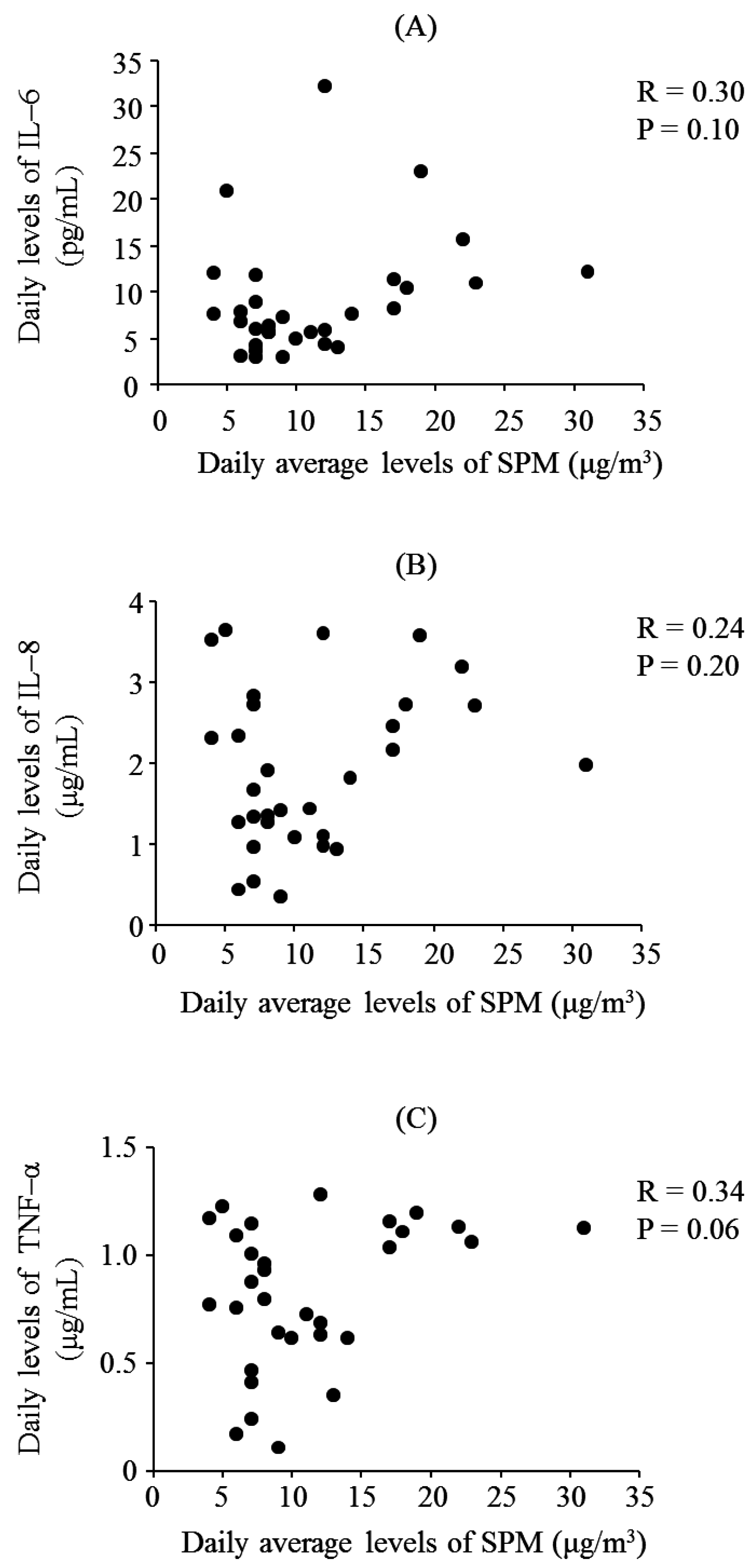
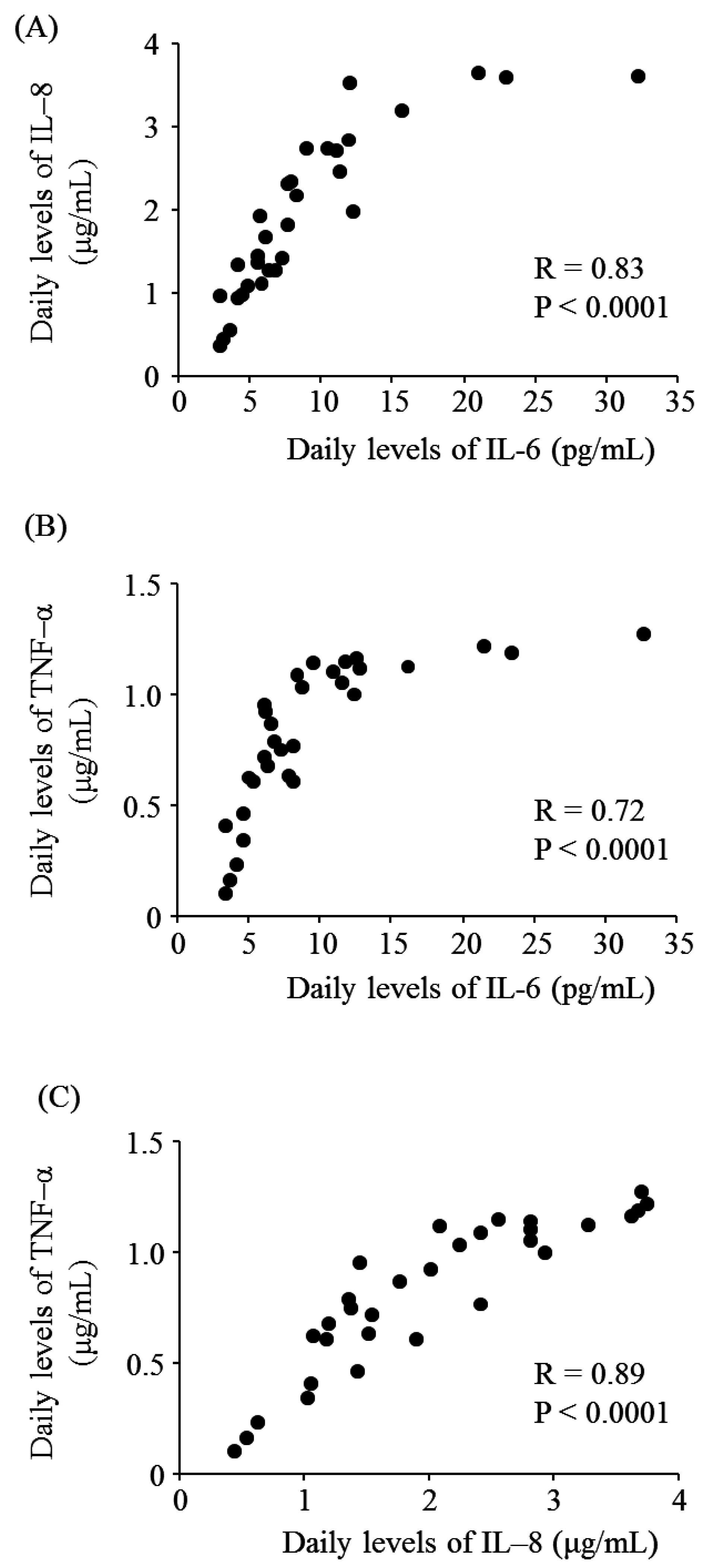
3.2. SPM and PM2.5 Levels and the Associations between SPM, PM2.5, IL-6, IL-8, and TNF-α Levels
3.3. Respiratory Symptoms
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Anderson, J.O.; Thundiyil, J.G.; Stolbach, A. Clearing the air: A review of the effects of particulate matter air pollution on human health. J. Med. Toxicol. 2012, 8, 166–175. [Google Scholar] [CrossRef] [PubMed]
- Lu, F.; Xu, D.; Cheng, Y.; Dong, S.; Guo, C.; Jiang, X.; Zheng, X. Systematic review and meta-analysis of the adverse health effects of ambient PM2.5 and PM10 pollution in the Chinese population. Environ. Res. 2015, 136, 196–204. [Google Scholar] [CrossRef] [PubMed]
- Madaniyazi, L.; Guo, Y.; Yu, W.; Tong, S. Projecting future air pollution-related mortality under a changing climate: Progress, uncertainties and research needs. Environ. Int. 2015, 75, 21–32. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, R.W.; Anderson, H.R.; Sunyer, J.; Ayres, J.; Baccini, M.; Vonk, J.M.; Boumghar, A.; Forastiere, F.; Forsberg, B.; Touloumi, G.; et al. Acute effects of particulate air pollution on respiratory admissions: Results from APHEA 2 project. Am. J. Respir. Crit. Care Med. 2001, 164, 1860–1866. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, J. Short term fluctuations in air pollution and hospital admissions of the elderly for respiratory disease. Thorax 1995, 50, 531–538. [Google Scholar] [CrossRef] [PubMed]
- Weinmayr, G.; Romeo, E.; De Sario, M.; Weiland, S.K.; Forastiere, F. Short-term effects of PM10 and NO2 on respiratory health among children with asthma or asthma-like symptoms: A systematic review and meta-analysis. Environ. Health Perspect. 2010, 118, 449–457. [Google Scholar] [CrossRef] [PubMed]
- Ward, D.J.; Ayres, J.G. Particulate air pollution and panel studies in children: A systematic review. Occup. Environ. Med. 2004, 61, e13. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Williams, G.; Jalaludin, B.; Baker, P. Panel studies of air pollution on children’s lung function and respiratory symptoms: A literature review. J. Asthma 2012, 49, 895–910. [Google Scholar] [CrossRef] [PubMed]
- Padula, A.M.; Balmes, J.R.; Eisen, E.A.; Mann, J.; Noth, E.M.; Lurmann, F.W.; Pratt, B.; Tager, I.B.; Nadeau, K.; Hammond, S.K. Ambient polycyclic aromatic hydrocarbons and pulmonary function in children. J. Expo. Sci. Environ. Epidemiol. 2015, 25, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Rosa, M.J.; Yan, B.; Chillrud, S.N.; Acosta, L.M.; Divjan, A.; Jacobson, J.S.; Miller, R.L.; Goldstein, I.F.; Perzanowski, M.S. Domestic airborne black carbon levels and 8-isoprostane in exhaled breath condensate among children in New York City. Environ. Res. 2014, 135, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Wilson, W.E.; Chow, J.C.; Claiborn, C.; Fusheng, W.; Engelbrecht, J.; Watson, J.G. Monitoring of particulate matter outdoors. Chemosphere 2002, 49, 1009–1043. [Google Scholar] [CrossRef]
- Kumar, R.K.; Shadie, A.M.; Bucknall, M.P.; Rutlidge, H.; Garthwaite, L.; Herbert, C.; Halliburton, B.; Parsons, K.S.; Wark, P.A. Differential injurious effects of ambient and traffic-derived particulate matter on airway epithelial cells. Respirology 2015, 20, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Hetland, R.B.; Cassee, F.R.; Låg, M.; Refsnes, M.; Dybing, E.; Schwarze, P.E. Cytokine release from alveolar macrophages exposed to ambient particulate matter: Heterogeneity in relation to size, city and season. Part. Fibre Toxicol. 2005, 2, 4. [Google Scholar] [CrossRef] [PubMed]
- Jalava, P.I.; Hirvonen, M.R.; Sillanpää, M.; Pennanen, A.S.; Happo, M.S.; Hillamo, R.; Cassee, F.R.; Gerlofs-Nijland, M.; Borm, P.J.; Schins, R.P.; et al. Associations of urban air particulate composition with inflammatory and cytotoxic responses in RAW 246.7 cell line. Inhal. Toxicol. 2009, 21, 994–1006. [Google Scholar] [CrossRef] [PubMed]
- Salonen, R.O.; Hälinen, A.I.; Pennanen, A.S.; Hirvonen, M.R.; Sillanpää, M.; Hillamo, R.; Shi, T.; Borm, P.; Sandell, E.; Koskentalo, T.; et al. Chemical and in vitro toxicologic characterization of wintertime and springtime urban-air particles with an aerodynamic diameter below 10 microm in Helsinki. Scand. J. Work Environ. Health 2004, 30, 80–90. [Google Scholar] [PubMed]
- Ovrevik, J.; Låg, M.; Holme, J.A.; Schwarze, P.E.; Refsnes, M. Cytokine and chemokine expression patterns in lung epithelial cells exposed to components characteristic of particulate air pollution. Toxicology 2009, 259, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, M.; Noma, H.; Kurai, J.; Kato, K.; Sano, H.; Tatsukawa, T.; Nakazaki, H.; Yamasaki, A.; Shimizu, E. Association between pulmonary function and daily levels of sand dust particles assessed by light detection and ranging in schoolchildren in western Japan: A panel study. Allergol. Int. 2016, 65, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Holgate, S.T.; Sandström, T.; Frew, A.J.; Stenfors, N.; Nördenhall, C.; Salvi, S.; Blomberg, A.; Helleday, R.; Söderberg, M. Health effects of acute exposure to air pollution. Part I: Healthy and asthmatic subjects exposed to diesel exhaust. Res. Rep. Health Eff. Inst. 2003, 112, 1–30. [Google Scholar] [PubMed]
- Sierra-Vargas, M.P.; Guzman-Grenfell, A.M.; Blanco-Jimenez, S.; Sepulveda-Sanchez, J.D.; Bernabe-Cabanillas, R.M.; Cardenas-Gonzalez, B.; Ceballos, G.; Hicks, J.J. Airborne particulate matter PM2.5 from Mexico City affects the generation of reactive oxygen species by blood neutrophils from asthmatics: An in vitro approach. J. Occup. Med. Toxicol. 2009, 4, 17. [Google Scholar] [CrossRef] [PubMed]
- McCreanor, J.; Cullinan, P.; Nieuwenhuijsen, M.J.; Stewart-Evans, J.; Malliarou, E.; Jarup, L.; Harrington, R.; Svartengren, M.; Han, I.K.; Ohman-Strickland, P.; et al. Respiratory effects of exposure to diesel traffic in persons with asthma. N. Engl. J. Med. 2007, 357, 2348–2358. [Google Scholar] [CrossRef] [PubMed]
- Hosseini, A.; Hirota, J.A.; Hackett, T.L.; McNagny, K.M.; Wilson, S.J.; Carlsten, C. Morphometric analysis of inflammation in bronchial biopsies following exposure to inhaled diesel exhaust and allergen challenge in atopic subjects. Part. Fibre Toxicol. 2016, 13, 2. [Google Scholar] [CrossRef] [PubMed]
- Kunkel, S.L.; Standiford, T.; Kasahara, K.; Strieter, R.M. Interleukin-8 (IL-8): The major neutrophil chemotactic factor in the lung. Exp. Lung Res. 1991, 17, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Mitschik, S.; Schierl, R.; Nowak, D.; Jörres, R.A. Effects of particulate matter on cytokine production in vitro: A comparative analysis of published studies. Inhal. Toxicol. 2008, 20, 399–414. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, M.; Noma, H.; Kurai, J.; Sano, H.; Kitano, H.; Saito, R.; Kimura, Y.; Aiba, S.; Oshimura, M.; Shimizu, E. Variation in the effect of particulate matter on pulmonary function in schoolchildren in western Japan and its relation with interleukin-8. Int. J. Environ. Res. Public Health 2015, 12, 14229–14243. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, M.; Noma, H.; Kurai, J.; Sano, H.; Saito, R.; Abe, S.; Kimura, Y.; Aiba, S.; Oshimura, M.; Yamasaki, A.; et al. Decreased pulmonary function in school children in Western Japan after exposures to Asian desert dusts and its association with interleukin-8. Biomed. Res. Int. 2015, 2015, 583293. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, M.; Noma, H.; Kurai, J.; Sano, H.; Hantan, D.; Ueki, M.; Kitano, H.; Shimizu, E. A Panel Study of Airborne Particulate Matter Composition versus Concentration: Potential for Inflammatory Response and Impaired Pulmonary Function in Children. Available online: http://www.allergologyinternational.com/article/S1323-8930%2816%2930052-1/pdf (accessed on 30 August 2016).
- Watanabe, M.; Noma, H.; Kurai, J.; Shimizu, A.; Sano, H.; Kato, K.; Mikami, M.; Ueda, Y.; Tatsukawa, T.; Ohga, H.; et al. Association of sand dust particles with pulmonary function and respiratory symptoms in adult patients with asthma in Western Japan using light detection and ranging: A panel study. Int. J. Environ. Res. Public Health 2015, 12, 13038–13052. [Google Scholar] [CrossRef] [PubMed]
- Higashi, T.; Kambayashi, Y.; Ohkura, N.; Fujimura, M.; Nakai, S.; Honda, Y.; Saijoh, K.; Hayakawa, K.; Kobayashi, F.; Michigami, Y.; et al. Effects of Asian dust on daily cough occurrence in patients with chronic cough: A panel study. Atmos. Environ. 2014, 92, 506–513. [Google Scholar] [CrossRef]
- Omori, T.; Fujimoto, G.; Yoshimura, I.; Nitta, H.; Ono, M. Effects of particulate matter on daily mortality in 13 Japanese cities. J. Epidemiol. 2003, 13, 314–322. [Google Scholar] [CrossRef] [PubMed]
- Hasei, T.; Watanabe, T.; Hirayama, T. Determination of 3,6-dinitrobenzo[e]pyrene in surface soil and airborne particles by high-performance liquid chromatography with fluorescence detection. J. Chromatogr. A 2006, 1135, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Laird, N.M.; Ware, J.H. Random-effects models for longitudinal data. Biometrics 1982, 38, 963–974. [Google Scholar] [CrossRef] [PubMed]
- Verbeke, G.; Molenberghs, G. Linear Mixed Models for Longitudinal Data, 2nd ed.; Springer: New York, NY, USA, 2009. [Google Scholar]
- Cesaroni, G.; Badaloni, C.; Porta, D.; Forastiere, F.; Perucci, C.A. Comparison between various indices of exposure to traffic-related air pollution and their impact on respiratory health in adults. Occup. Environ. Med. 2008, 65, 683–690. [Google Scholar] [CrossRef] [PubMed]
- Gehring, U.; Wijga, A.H.; Brauer, M.; Fischer, P.; de Jongste, J.C.; Kerkhof, M.; Oldenwening, M.; Smit, H.A.; Brunekreef, B. Traffic-related air pollution and the development of asthma and allergies during the first 8 years of life. Am. J. Respir. Crit. Care Med. 2010, 181, 596e603. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Shima, M.; Yoda, Y.; Yamamoto, H.; Nakai, S.; Tamura, K.; Nitta, H.; Watanabe, H.; Nishimuta, T. Effects of airborne particulate matter on respiratory morbidity in asthmatic children. J. Epidemiol. 2008, 18, 97–110. [Google Scholar] [CrossRef] [PubMed]
- Rubin, D.B. Multiple Imputation for Nonresponse in Surveys; John Wiley: New York, NY, USA, 1987. [Google Scholar]
- Schwarze, P.E.; Ovrevik, J.; Låg, M.; Refsnes, M.; Nafstad, P.; Hetland, R.B.; Dybing, E. Particulate matter properties and health effects: Consistency of epidemiological and toxicological studies. Hum. Exp. Toxicol. 2006, 25, 559–579. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Cheng, J.; Lv, J.; Wu, L.; Wu, J. Comparison of chemical compositions in air particulate matter during summer and winter in Beijing, China. Environ. Geochem. Health 2016. [Google Scholar] [CrossRef] [PubMed]
- Thurston, G.D.; Burnett, R.T.; Turner, M.C.; Shi, Y.; Krewski, D.; Lall, R.; Ito, K.; Jerrett, M.; Gapstur, S.M.; Diver, W.R.; et al. Ischemic heart disease mortality and long-term exposure to source-related components of U.S. fine particle air pollution. Environ. Health Perspect. 2016, 124, 785–794. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Xin, J.; Wang, Y.; Li, G.; Pan, X.; Wang, S.; Cheng, M.; Wen, T.; Wang, G.; Liu, Z. Association between particulate matter and its chemical constituents of urban air pollution and daily mortality or morbidity in Beijing City. Environ. Sci. Pollut. Res. Int. 2015, 22, 358–368. [Google Scholar] [CrossRef] [PubMed]
- Hamasaki, Y.; Kohno, Y.; Ebisawa, M.; Kondo, N.; Nishima, S.; Nishimuta, T.; Morikawa, A.; Japanese Society of Allergology; Japanese Society of Pediatric Allergy and Clinical Immunology. Japanese Guideline for Childhood Asthma 2014. Allergol. Int. 2014, 63, 335–356. [Google Scholar] [CrossRef] [PubMed]
- Shturman-Ellstein, R.; Zeballos, R.J.; Buckley, J.M.; Souhrada, J.F. The beneficial effect of nasal breathing on exercise-induced bronchoconstriction. Am. Rev. Respir. Dis. 1978, 118, 65–73. [Google Scholar] [PubMed]
- Yoda, Y.; Takagi, H.; Wakamatu, J.; Otani, N.; Shima, M. Short-term effects of air pollutants on pulmonary function in adolescent with a history of asthma or allergies. Arerugi 2015, 64, 128–135. [Google Scholar] [PubMed]
- Delfino, R.J.; Quintana, P.J.; Floro, J.; Gastañaga, V.M.; Samimi, B.S.; Kleinman, M.T.; Liu, L.J.; Bufalino, C.; Wu, C.F.; McLaren, C.E. Association of FEV1 in asthmatic children with personal and microenvironmental exposure to airborne particulate matter. Environ. Health Perspect. 2004, 112, 932–941. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, N.J.; Hinds, W.C. Inhalability of large solid particles. J. Aerosol. Sci. 2002, 33, 237–255. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Value | |
|---|---|---|
| Boy/Girl | 172/188 | |
| Age (Years) | 11 | 139 (38.6) |
| 12 | 220 (61.1) | |
| 13 | 1 (0.3) | |
| Height (cm) | 148.6 ± 7.4 | |
| Weight (kg) | 39.0 ± 7.7 | |
| Allergic Disease | Sthma | 39 (10.8) |
| Allergic Rhinitis | 72 (20.0) | |
| Allergic Conjunctivitis | 10 (2.8) | |
| Atopic Dermatitis | 26 (7.2) | |
| Food Allergies | 15 (4.2) | |
| Exposure Metric | IQR | Odds Ratio | 95% CI | p-Value |
|---|---|---|---|---|
| SPM | 6.0 μg/m3 | 0.97 | 0.91–1.02 | NS |
| PM2.5 | 7.6 μg/m3 | 0.96 | 0.91–1.02 | NS |
| IL-6 | 6.16 pg/mL | 1.05 | 1.01–1.09 | 0.02 |
| IL-8 | 1.46 μg/mL | 1.12 | 1.04–1.20 | 0.002 |
| TNF-α | 0.47 μg/mL | 1.11 | 1.03–1.19 | 0.004 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Watanabe, M.; Noma, H.; Kurai, J.; Sano, H.; Hantan, D.; Ueki, M.; Kitano, H.; Shimizu, E. Effects of Short-Term Exposure to Particulate Air Pollutants on the Inflammatory Response and Respiratory Symptoms: A Panel Study in Schoolchildren from Rural Areas of Japan. Int. J. Environ. Res. Public Health 2016, 13, 983. https://doi.org/10.3390/ijerph13100983
Watanabe M, Noma H, Kurai J, Sano H, Hantan D, Ueki M, Kitano H, Shimizu E. Effects of Short-Term Exposure to Particulate Air Pollutants on the Inflammatory Response and Respiratory Symptoms: A Panel Study in Schoolchildren from Rural Areas of Japan. International Journal of Environmental Research and Public Health. 2016; 13(10):983. https://doi.org/10.3390/ijerph13100983
Chicago/Turabian StyleWatanabe, Masanari, Hisashi Noma, Jun Kurai, Hiroyuki Sano, Degejirihu Hantan, Masaru Ueki, Hiroya Kitano, and Eiji Shimizu. 2016. "Effects of Short-Term Exposure to Particulate Air Pollutants on the Inflammatory Response and Respiratory Symptoms: A Panel Study in Schoolchildren from Rural Areas of Japan" International Journal of Environmental Research and Public Health 13, no. 10: 983. https://doi.org/10.3390/ijerph13100983
APA StyleWatanabe, M., Noma, H., Kurai, J., Sano, H., Hantan, D., Ueki, M., Kitano, H., & Shimizu, E. (2016). Effects of Short-Term Exposure to Particulate Air Pollutants on the Inflammatory Response and Respiratory Symptoms: A Panel Study in Schoolchildren from Rural Areas of Japan. International Journal of Environmental Research and Public Health, 13(10), 983. https://doi.org/10.3390/ijerph13100983