
Factors Influencing Health Knowledge and Behaviors among the Elderly in Rural China

 ,
, 
Abstract
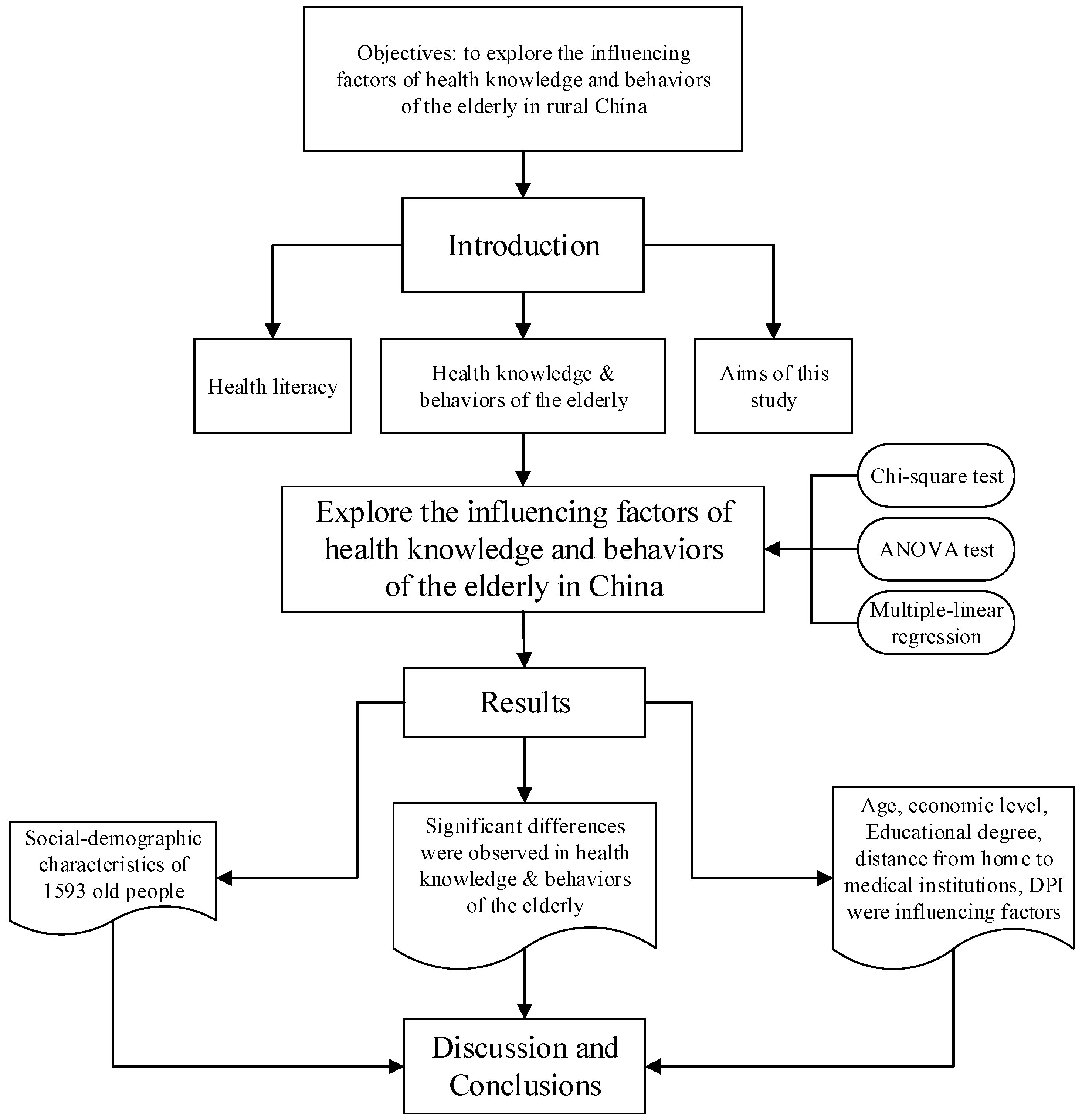
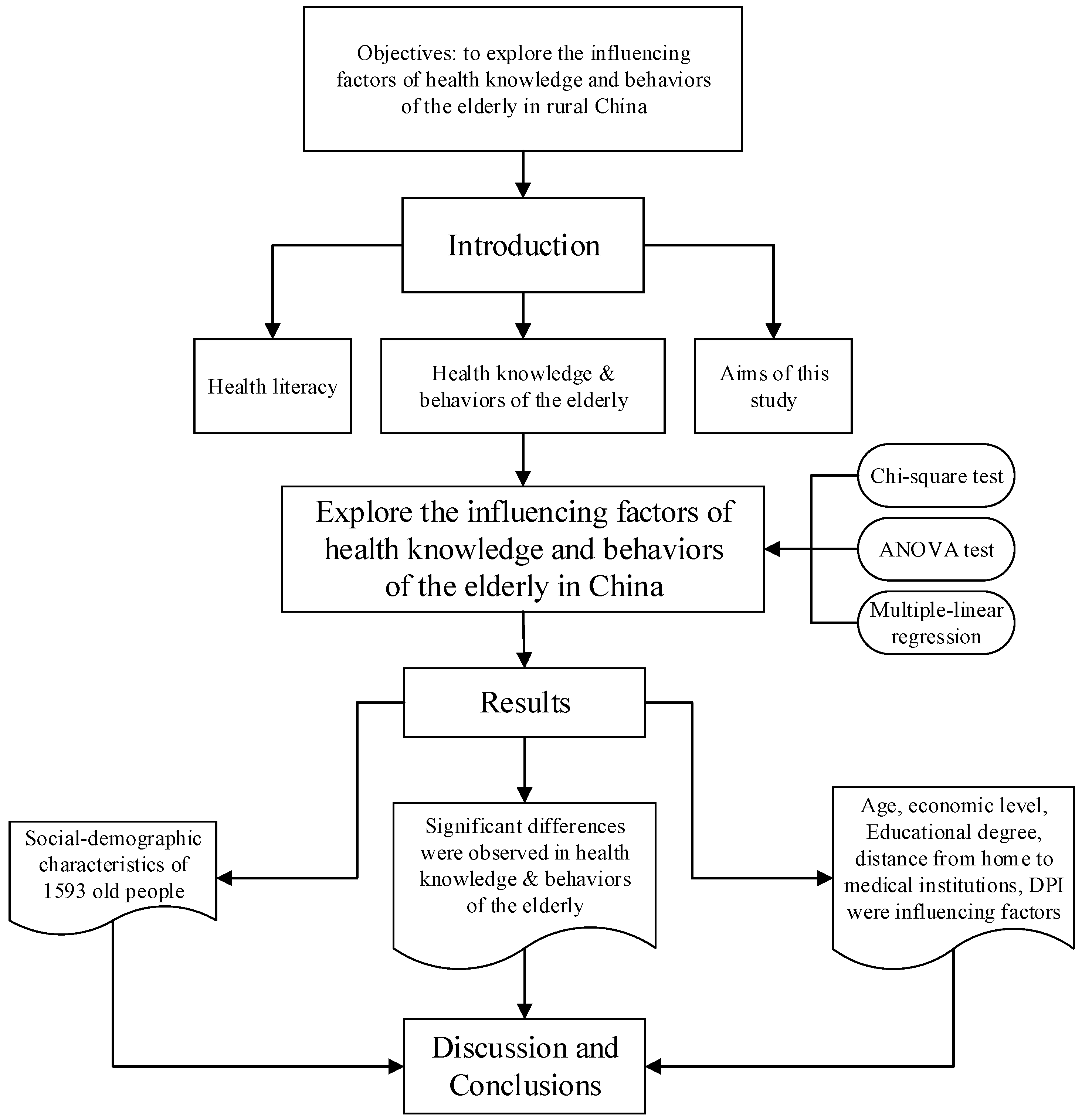
:1. Introduction
2. Methods
2.1. Study Design
2.2. Structure Model
2.3. Data Collection
2.4. Variables
2.5. Statistical Analysis
2.6. Ethics Approval
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| DPI | Disposable personal income |
| NCMS | New rural cooperative medical system |
| UEBMI | Urban Employee Basic Medical Insurance |
| URBMI | Urban Residents Basic Medical Insurance |
References
- Yusuf, M. The impact of self-efficacy, achievement motivation, and self-regulated learning strategies on students’ academic achievement. Procedia Soc. Behav. Sci. 2011, 15, 2623–2626. [Google Scholar] [CrossRef]
- Nutbeam, D.; Kickbusch, I. Advancing health literacy: A global challenge for the 21st century. Health Promot. Int. 2000, 15, 183–184. [Google Scholar] [CrossRef]
- Nutbeam, D. Health literacy as a public health goal: A challenge for contemporary health education and communication strategies into the 21st century. Health Promot. Int. 2006, 15, 259–267. [Google Scholar] [CrossRef]
- Chinn, D. Critical health literacy: A review and critical analysis. Soc. Sci. Med. 2011, 73, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, K.; Broucke, S.V.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H. Health literacy and public health: A systematic review and integration of definitions and modes. BMC Public Health 2012, 12. [Google Scholar] [CrossRef] [PubMed]
- Ryu, S.; Ho, S.H.; Han, I. Knowledge sharing behavior of physicians in hospitals. Expert Syst. Appl. 2003, 25, 113–122. [Google Scholar] [CrossRef]
- Petersen, P.E.; Kwan, S. Equity, social determinants and public health programmes—The case of oral health. Community Dent. Oral Epidemiol. 2011, 39, 481–487. [Google Scholar] [CrossRef] [PubMed]
- Hsu, M.; Ju, T.L.; Yen, C.; Chang, C. Knowledge sharing behavior in virtual communities: The relationship between trust, self-efficacy, and outcome expectations. Int. J. Hum.-Comput. Stud. 2007, 65, 153–169. [Google Scholar] [CrossRef]
- Lui, C.K.; Chung, P.J.; Wallace, S.P.; Aneshensel, C.S. Social status attainment during the transition to adulthood. J. Youth Adolesc. 2014, 43, 1134–1150. [Google Scholar] [CrossRef] [PubMed]
- Scott, R.; Michael, D.H. The concept of health literacy within the older adult population. Holist. Nurs. Pract. 2010, 24, 204–212. [Google Scholar]
- Yang, G.L.; Yang, J. The health literacy of the elderly people in China. J. Food Drug 2010, 2, 1564–1565. [Google Scholar]
- Wang, F.; Mason, A. Population Aging in China: Challenges, Opportunities, and Institutions; University of California: Irvine, CA, USA, 2005. [Google Scholar]
- Alonso, J.; Ferrer, M.; Gandek, B.; Ware, J.; Aaronson, N.K.; Mosconi, P.; Rasmussen, N.K.; Bullinger, M.; Fukuhara, S.; Kassa, S.; et al. Health-related quality of life associated with chronic conditions in eight countries: Results from the International Quality of Life Assessment (IQOLA) Project. Qual. Life Res. 2004, 13, 283–298. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, B.J. Self-Efficacy: An Essential Motive to Learn. Contemp. Educ. Psychol. 2000, 25, 82–91. [Google Scholar] [CrossRef] [PubMed]
- Wagstaff, A.; Lindelow, M.; Gao, J.; Xu, L.; Qian, J.C. Extending health insurance to the rural population: An impact evaluation of China’s new cooperative medical scheme. J. Health Econ. 2009, 28, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Harbaugh, C.W.; West, L.A. Aging trends—China. J. Cross-Cult. Psychol. 1993, 8, 271–280. [Google Scholar] [CrossRef] [PubMed]
- Kosberg, J. Opportunities for Social Workers in an Aging World; Florida International University: Miami, FL, USA, 1999. [Google Scholar]
- Yang, R.H.; Li, R.; Zhang, L. Analysis of health behavior and its influencing factors. J. Nurs. 2010, 3, 94–97. [Google Scholar]
- China National Statistical Bureau. A Statistic Compendium of the China 2011 National Census; China National Statistical Bureau: Beijing, China, 2011.
- Peng, L.H.; de Alan, B.; Scott, R. Working until you drop: The elderly of rural China. Chicago J. 2004, 52, 74–92. [Google Scholar]
- Griffiths, K.M.; Christensen, H.; Jorm, A.F. Mental health literacy as a function of remoteness of residence: An Australian national study. BMC Public Health 2009, 92, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Kondilis, B.K.; Kiriaze, I.J.; Athanasoulia, A.P.; Falagas, M.E. Mapping health literacy research in the European Union: A bibliometric analysis. PLoS ONE 2008, 6, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Birren, J.E.; George, L.K.; Cutler, S.J.; Hendricks, J.; Schulz, J.H. The Handbooks of Aging and the Social Sciences; Academic Press: San Diego, CA, USA, 2006; pp. 303–316. [Google Scholar]
- Zhang, J.C.; Xiang, Y.; Tang, D.J. Analysis of the health education in rural Sichuan, China. J. Preent. Med. Inform. 2004, 23, 633–636. [Google Scholar]
- Zhang, X.P.; Zhu, M.M.; Dib, H.H.; Hu, J.; Tang, S.C.; Zhong, T.; Ming, X. Knowledge, awareness, behavior (KAB) and control of hypertension among urban elderly in western China. Int. J. Cardiol. 2009, 137, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Skinner, C.S.; Arfken, C.L.; Sykes, R.K. Knowledge, perceptions, and mammography stage of adoption among old urban women. Am. J. Prev. Med. 1998, 14, 54–63. [Google Scholar] [CrossRef]
- Gray, N.J.; Klein, J.D.; Noyce, P.R.; Sesselberg, T.S.; Cantrill, J.A. The internet: A window on adolescent health literacy. J. Adolesc. Health 2005, 37, 243.e1–243.e7. [Google Scholar] [CrossRef] [PubMed]
- Gulliver, A.; Griffiths, K.M.; Christensen, H. Perceived barriers and facilitators to mental health healp-seeking in young people: A systematic review. BMC Psychiatry 2010, 10, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Patel, V.; Flisher, A.J.; Hetrick, S.; Gorry, P.M. Metal health of young people: A global public-health challenge. Lancet 2007, 369, 1302–1313. [Google Scholar] [CrossRef]
- Li, D.M.; Chen, M.J. Health behavior inhabitors of the aged in rural China. Chin. J. Gerontol. 2014, 5, 1336–1338. [Google Scholar]
- He, J.F.; Li, Z. Research of promotion to health behaviors. Nursing 2007, 14, 28–30. [Google Scholar]
- Cook, P.A.; Bellis, M.A. Knowing the risk: Relationships between risk behavior and health knowledge. Public Health 2001, 115, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Camerini, L.; Schulz, P.J.; Nakamoto, K. Differential effects of health knowledge and health empowerment over patients’ self-management and health outcome: A cross-sectional evaluation. Patient Educ. Couns. 2012, 89, 334–337. [Google Scholar] [CrossRef] [PubMed]
- Catherien, W.; Donoghue, A.M. Impact of a health promotion magazine on employee’s health-knowledge. Occup. Med. 2010, 60, 90–93. [Google Scholar]
- Yin, Z.Q.; Geng, G.L.; Lan, X.F.; Zhang, L.M.; Wang, S.; Zang, Y.T.; Peng, M.D. Status and determinants of health behavior knowledge among the elderly in China: A community-based cross-sectional study. BMC Public Health 2013, 13, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Frank, M.R.; Heiby, E.M.; Lee, J.H. Assessment of determinants of compliance to twelve health behaviors: Psychometric evaluation of the health behavior schedule. Psychol. Rep. 2007, 100, 1281–1297. [Google Scholar] [PubMed]
- Mcnerney, J.; Andes, S.D. Self-Reported Health Behaviors of Osteopathic Physicians. J. Am. Osteopath. Assoc. 2007, 107, 537–546. [Google Scholar] [PubMed]
- Yip, W.; Hsiao, W.C. Non-evidence-based policy: How effective is China’s new cooperative medical scheme in reducing medical impoverishment? Soc. Sci. Med. 2009, 68, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Jankowska-Polanska, B.K.; Kamińska, M.; Uchmanowicz, I.; Rycombel, A. Quality of life and health behaviours of patients with tuberculosis-sex differences. Pneumonol, Alergol. Pol. 2015, 83, 256–265. [Google Scholar] [CrossRef] [PubMed]
- Perumal, S.S.; Prasad, S.; Surapaneni, K.M.; Joshi, A. Health Information–Seeking Behavior among Hypothyroid Patients at Saveetha Medical College and Hospital. Ethiop. J. Health Sci. 2015, 25, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.M.; Gu, D.D.; Deng, Y.J.; Wang, H.Y. Determinants of Participation, Satisfaction, and Sustainability of the New Cooperative Medical Scheme in Rural China. Chin. J. Popul. Sci. 2006, 5, 42–49. [Google Scholar]
- Michael, S.W.; Julie, A.G.; David, W.B. Health Literacy and functional health status among older adults. JAMA Intern. Med. 2005, 165, 1946–1952. [Google Scholar]
- Miranda, R.; Andrus, M.T.R. Health Literacy: A Review. J. Hum. Pharmacol. Drug Therapy 2002, 3, 282–302. [Google Scholar]
- Levy, B.R.; Slade, M.D.; Kasl, S.V. Longitudinal Benefit of Positive Self-Perceptions of Aging on Functional Health. J. Gerontol. Psychol. Sci. 2002, 57, 409–417. [Google Scholar] [CrossRef]
- Chisholm, A.; Nelson, P.A.; Pearce, C.J.; Keyworth, C.; Griffiths, C.E.M.; Cordingley, L.; Bundy, C. The role of personal models in clinical management: Exploring health care providers’ beliefs about psoriasis. Br. J. Health Psychol. 2016, 21, 114–134. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Jongbloed, L.; Dean, E. Stroke-Related Knowledge, Beliefs, and Behaviours of Chinese and European Canadians: Implications for Physical Therapists. Physiother. Can. 2014, 66, 187–196. [Google Scholar] [CrossRef] [PubMed]
- Dickens, G.L.; Hallett, N.; Lamont, E. Interventions to improve mental health nurses’ skills, attitudes, and knowledge related to people with a diagnosis of borderline personality disorder: Systematic review. Int. J. Nurs. Stud. 2016, 56, 114–127. [Google Scholar] [CrossRef] [PubMed]
- Lorence, D.; Park, H. Study of Education Disparities and Health Information Seeking Behavior. CyberPsychol. Behav. 2007, 10, 149–151. [Google Scholar] [CrossRef] [PubMed]
- Ansai, T.; Takata, Y.; Soh, I.; Awano, S.; Yoshida, A.; Sonoki, K.; Hamasaki, T.; Torisu, T.; Sogame, A.; Shimada, N.; et al. Relationship between tooth loss and mortality in 80-year-old Japanese community-dwelling subjects. BMC Public Health 2010, 10. [Google Scholar] [CrossRef] [PubMed]
- Richard, L.; Gauvin, L.; Gosselin, C.; Laforest, S. Staying connected: Neighbourhood correlates of social participation among older adults living in an urban environment in Montreal, Quebec. Health Promot. Int. 2008, 24, 46–57. [Google Scholar] [CrossRef] [PubMed]
- Michael, Y.L.; Colditz, G.A.; Coakley, E.; Kawachi, I. Health behaviors, social networks, and healthy aging: Cross-sectional evidence from the Nurses’ Health Study. Qual. Life Res. 1999, 8, 711–722. [Google Scholar] [CrossRef] [PubMed]
- Jianping, L.; Shaobing, Z. Health education of the elderly in rural China. Chin. J. Nurs. 2007, 42, 723–724. [Google Scholar]
- Christopher, J.; Armitage, M.C. Efficacy of the Theory of Planned Behaviour: A meta-analytic review. Br. J. Soc. Psycol. 2001, 40, 471–499. [Google Scholar]
- Chu, P.Y.; Maslow, G.R.; Isenburg, M.V.; Chung, R.J. Systematic Review of the Impact of Transition Interventions for Adolescents with Chronic Illness on Transfer from Pediatric to Adult Healthcare. J. Pediat. Nurs. 2015, 30, e19–e27. [Google Scholar] [CrossRef] [PubMed]
- Du, W.J.; Li, Y.H.; Nie, X.Q.; Li, L.; Tao, M.X.; Tian, X.Y. Analysis of status and influence factors of health literacy of Chinese residents aged 60–69 years. Chin. J. Health Educ. 2015, 31, 129–133. (In Chinese) [Google Scholar]
- David, W.B.; Wolf, M.S.; Joseph, F.; Jason, A.T.; Julie, A.G.; Jenny, H. Health Literacy and Mortality among Elderly Persons. JAMA Int. Med. 2007, 167, 1503–1509. [Google Scholar]
- Beach, M.C.; Price, E.G.; Gary, T.L.; Robinson, K.A.; Gozu, A.; Palacio, A.; Smarth, C.; Jenckes, M.W.; Feuerstein, C.; Bass, E.B.; et al. Cultural Competency: A Systematic Review of Health Care Provider Educational Interventions. Med. Care 2005, 43, 356–373. [Google Scholar] [CrossRef] [PubMed]
- Kuo, F.Y.; Young, M.L. Predicting knowledge sharing practices through intention: A test of competing models. Comput. Hum. Behav. 2008, 24, 2697–2722. [Google Scholar] [CrossRef]
- Feinstein, J.S. The relationship between socioeconomic status and health: A review of the literature. Milbank Q. 1993, 71, 279–322. [Google Scholar] [CrossRef]

{kind=link}
| Municipality/Province | Towns | Villages & Total Sample Size | Sample Size (the Elders %) |
|---|---|---|---|
| Chongqing (western) | 4 towns | 16 villages & 576 | 533 (92.53) |
| Henan (central) | 4 towns | 16 villages & 576 | 522 (90.63) |
| Zhejiang (eastern) | 4 towns | 16 villages & 576 | 538 (93.40) |
| Variables | Total | Chongqing | Henan | Zhejiang | χ2 | p | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| n = 1593 | % | n = 533 | % | n = 522 | % | n = 538 | % | |||
| Age groups | ||||||||||
| 60–65 | 201 | 12.62 | 67 | 12.57 | 46 | 8.81 | 88 | 16.36 | 96.39 | 0.000 *** |
| 66–70 | 514 | 32.27 | 138 | 25.89 | 161 | 30.84 | 215 | 39.96 | ||
| 71–75 | 390 | 24.48 | 119 | 22.33 | 131 | 25.10 | 140 | 26.02 | ||
| 76–80 | 321 | 20.15 | 120 | 22.51 | 118 | 22.61 | 83 | 15.43 | ||
| Above 80 | 167 | 10.48 | 89 | 16.70 | 66 | 12.64 | 12 | 2.23 | ||
| Gender | ||||||||||
| Male | 826 | 51.85 | 239 | 44.84 | 287 | 54.98 | 300 | 55.76 | 15.84 | 0.000 *** |
| Female | 767 | 48.15 | 294 | 55.16 | 235 | 45.02 | 238 | 44.24 | ||
| Degree of education | ||||||||||
| Illiteracy | 811 | 50.91 | 285 | 53.47 | 258 | 49.43 | 268 | 49.81 | 24.10 | 0.002 *** |
| Primary school | 516 | 32.39 | 187 | 35.08 | 158 | 30.27 | 171 | 31.78 | ||
| Junior high school | 212 | 13.31 | 47 | 8.82 | 82 | 15.71 | 83 | 15.43 | ||
| Senior high school | 37 | 2.32 | 10 | 1.88 | 13 | 2.48 | 14 | 2.61 | ||
| College | 17 | 1.07 | 4 | 0.75 | 11 | 2.11 | 2 | 0.37 | ||
| Profession | ||||||||||
| Farmer | 1189 | 74.63 | 494 | 92.68 | 328 | 62.84 | 367 | 68.22 | 203.19 | 0.000 *** |
| Migrant-workers | 74 | 4.65 | 3 | 0.56 | 60 | 11.49 | 11 | 2.05 | ||
| The self-employed | 56 | 3.52 | 3 | 0.56 | 32 | 6.13 | 21 | 3.90 | ||
| Retirees | 184 | 11.55 | 24 | 4.51 | 71 | 13.60 | 89 | 16.54 | ||
| Others | 90 | 5.65 | 9 | 1.69 | 31 | 5.94 | 50 | 9.29 | ||
| Types of healthcare insurance | ||||||||||
| NCMS | 1475 | 92.59 | 502 | 94.18 | 495 | 94.83 | 478 | 88.85 | 19.40 | 0.001 *** |
| URBMI | 53 | 3.33 | 17 | 3.19 | 13 | 2.49 | 23 | 4.28 | ||
| UEBMI | 65 | 4.08 | 14 | 2.63 | 14 | 2.68 | 37 | 6.87 | ||
| Distance from home to medical institutions | ||||||||||
| <1 km | 1340 | 84.12 | 401 | 75.23 | 424 | 81.23 | 515 | 95.72 | 89.01 | 0.000 *** |
| ≥1 km | 253 | 15.88 | 132 | 24.77 | 98 | 18.77 | 23 | 4.28 | ||
| Disposable Personal Income (DPI: RMB yuan) | ||||||||||
| <5000 | 367 | 23.04 | 168 | 31.52 | 109 | 20.88 | 90 | 16.73 | 186.81 | 0.000 *** |
| 5001–10,000 | 230 | 14.44 | 111 | 20.83 | 64 | 12.26 | 55 | 10.22 | ||
| 10,001–15,000 | 346 | 21.72 | 160 | 30.02 | 91 | 17.43 | 95 | 17.66 | ||
| 15,001–20,000 | 121 | 7.60 | 26 | 4.88 | 43 | 8.24 | 52 | 9.67 | ||
| >20,000 | 529 | 33.20 | 68 | 12.75 | 215 | 41.19 | 246 | 45.72 | ||
| Health Knowledge | ||||||
| Items | Total (n = 1593) | a. Chongqing (n = 533) | b. Henan (n = 522) | c. Zhejiang (n = 538) | χ2 | p |
| Accuracy Rate (%) | Accuracy Rate (%) | Accuracy Rate (%) | Accuracy Rate (%) | |||
| 1. Whether the secondhand smoke is harmful to health | 1160 (72.82) | 365 (68.48) | 355 (68.01) | 440 (81.78) | 33.02 | 0.000 *** |
| 2. Whether too much salt cause high blood pressure | 1105 (69.37) | 304 (57.04) | 330 (63.22) | 471 (87.55) | 131.10 | 0.000 *** |
| 3. Fat people are vulnerable in diabetes | 919 (57.69) | 217 (40.71) | 302 (57.85) | 400 (74.35) | 124.10 | 0.000 *** |
| 4. Whether people suffer from hepatitis B after eating together with hepatitis B patients | 757 (47.52) | 222 (41.65) | 239 (45.79) | 296 (55.02) | 20.12 | 0.000 *** |
| 5. Whether excessive drinking is harmful to the liver | 1175 (73.76) | 392 (73.55) | 352 (67.43) | 431 (80.11) | 22.02 | 0.000 *** |
| 6. Whether fruits can be eaten without washing | 1331 (83.55) | 451 (84.62) | 400 (76.63) | 480 (89.22) | 31.22 | 0.000 *** |
| 7. Whether vaccinate is protected from infectious disease | 692 (43.44) | 280 (52.53) | 291 (55.75) | 121 (22.49) | 146.20 | 0.000 *** |
| 8. Whether the anemia related with the iron-deficiency | 572 (35.91) | 136 (25.52) | 230 (44.06) | 206 (38.29) | 41.42 | 0.000 *** |
| 9. Whether health is defined as not being fat or thin | 523 (32.83) | 86 (16.14) | 194 (37.16) | 243 (45.17) | 109.00 | 0.000 *** |
| Average accuracy | (57.43) | (51.14) | (57.32) | (63.78) | ||
| Health Behavior | ||||||
| Items | Total (n = 1593) | a. Chongqing (n = 533) | b. Henan (n = 522) | c. Zhejiang (n = 538) | p | LSD |
| Mean | Mean | Mean | Mean | |||
| 1. Heavy taste | 2.17 | 2.14 | 2.01 | 2.36 | 0.000 *** | c > a > b ** |
| 2. Frequency of tooth brushing | 1.78 | 1.80 | 1.74 | 1.79 | 0.462 | |
| 3. Cigarette per day | 2.45 | 2.36 | 2.43 | 2.57 | 0.002 ** | c > a **; c > b ** |
| 4. Drinking per day | 2.66 | 2.59 | 2.57 | 2.83 | 0.000 *** | c > a ***; c > b *** |
| 5. Physical examination | 1.77 | 1.58 | 1.37 | 2.35 | 0.000 *** | c > a > b ** |
| 6. Frequency of physical exercise | 1.19 | 0.87 | 1.02 | 1.68 | 0.000 *** | c > b > a ** |
| 7.Purchase times of expired food | 2.55 | 2.48 | 2.40 | 2.75 | 0.000 *** | c > a ***; c > b *** |
| 8. Frequency of blood pressure measurement | 1.69 | 1.52 | 1.39 | 2.14 | 0.000 *** | c > a > b ** |
| 9. Frequency of obtaining health knowledge | 1.61 | 1.33 | 1.42 | 2.06 | 0.000 *** | c > a ***; c > b *** |
| 10. Frequency of consulting health knowledge from doctors | 1.85 | 1.63 | 1.69 | 2.23 | 0.000 *** | c > a ***; c > b *** |
| 11. Frequency of disseminating health knowledge to others | 0.70 | 0.43 | 0.59 | 1.07 | 0.000 *** | c > b > a ** |
| Characteristic Variables | n | Scores of Health Knowledge | Scores of Health Behavior | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | F | p | LSD | Mean | SD | F | p | LSD | ||
| a. Chongqing | 533 | 4.60 | 2.29 | 31.52 | 0.000 *** | a < b < c *** | 18.74 | 4.28 | 360.01 | 0.000 *** | c > a ***; c > b *** |
| b. Henan | 522 | 5.16 | 2.75 | 18.63 | 3.64 | ||||||
| c. Zhejiang | 538 | 5.74 | 1.94 | 23.86 | 2.88 | ||||||
| a. 60–65 | 201 | 5.54 | 2.07 | 19.29 | 0.000 *** | a > d > e **; b > d > e **; c > d > e ** | 20.85 | 4.11 | 24.65 | 0.000 *** | a > d > e **; b > d > e **; c > d > e ** |
| b. 66–70 | 514 | 5.40 | 2.33 | 21.23 | 4.35 | ||||||
| c. 71–75 | 390 | 5.43 | 2.36 | 20.88 | 4.39 | ||||||
| d. 76–80 | 321 | 4.98 | 2.42 | 19.73 | 4.28 | ||||||
| e. over 80 | 167 | 3.77 | 2.46 | 17.76 | 3.81 | ||||||
| a. Male | 826 | 5.17 | 2.38 | 0.00 | 0.991 | 20.33 | 4.39 | 0.91 | 0.34 | ||
| b. Female | 767 | 5.17 | 2.40 | 20.54 | 4.38 | ||||||
| a. Illiteracy | 811 | 4.96 | 2.49 | 15.56 | 0.000 *** | a < c ***; a < c ***; a < d **; b < c ***; b < c ***; b < e ** | 20.03 | 4.40 | 8.61 | 0.000 *** | a < c ***; a < d ***; a < e **; b < c **; b < d **; b < e ** |
| b. Primary school | 516 | 4.99 | 2.23 | 20.39 | 4.30 | ||||||
| c. Junior high school | 212 | 6.04 | 2.20 | 21.46 | 4.36 | ||||||
| d. Senior high school | 37 | 6.59 | 1.64 | 22.76 | 4.03 | ||||||
| e. College | 17 | 6.94 | 1.20 | 22.76 | 3.56 | ||||||
| a. Farmer | 1189 | 4.97 | 2.31 | 15.00 | 0.000 *** | b > a ***; c > a ***; b > d ***; b > e ***; c > d **; c > e ** | 20.26 | 4.29 | 18.68 | 0.000 *** | b < a < d < e **; b < c *** |
| b. Migrant-worker | 74 | 6.84 | 2.26 | 17.28 | 3.82 | ||||||
| c. The self-employed | 56 | 6.30 | 2.32 | 21.34 | 4.10 | ||||||
| d. Retirees | 184 | 5.29 | 2.70 | 22.01 | 4.36 | ||||||
| e. Others | 90 | 5.41 | 2.22 | 21.50 | 4.72 | ||||||
| a. NCMS | 1475 | 5.17 | 2.40 | 0.01 | 0.993 | 20.34 | 4.40 | 5.51 | 0.004 ** | c > a ** | |
| b. URBMI | 53 | 5.21 | 1.78 | 20.96 | 3.99 | ||||||
| c. UEBMI | 65 | 5.17 | 2.61 | 22.11 | 4.18 | ||||||
| a. <1 km | 1340 | 5.30 | 2.38 | 24.63 | 0.000 *** | a > b *** | 20.86 | 4.30 | 87.40 | 0.000 *** | a > b *** |
| b. ≥1 km | 253 | 4.49 | 2.34 | 18.13 | 4.14 | ||||||
| a. <5000 RMB | 367 | 4.84 | 2.51 | 11.03 | 0.000 *** | e > a ***; e > b ***; e > c ***; e > d ** | 19.94 | 4.32 | 11.30 | 0.000 *** | d > a **; d > b **; d > c **; e > a ***; e > b ***; e > c *** |
| b. 5001–10,000 RMB | 230 | 4.86 | 2.26 | 19.52 | 4.09 | ||||||
| c. 10,001–15,000 RMB | 346 | 4.90 | 2.42 | 19.94 | 4.44 | ||||||
| d. 15,001–20,000 RMB | 121 | 5.16 | 2.31 | 21.08 | 4.37 | ||||||
| e. >20,000 RMB | 529 | 5.71 | 2.27 | 21.34 | 4.36 | ||||||
| Influencing Factors of Health Knowledge | Influencing Factors of Health Behaviors | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Characteristic Variables | Unstandardized Coefficients | Standardized Coefficients | t Value | p | 95% Confidence | Unstandardized Coefficients | Standardized Coefficients | t Value | p | 95% Confidence | ||||
| B | SE | Beta | Lower | Upper | B | SE | Beta | Lower | Upper | |||||
| Constant | 5.515 | 0.285 | 19.343 | 0.000 *** | 4.956 | 6.074 | 20.199 | 0.448 | 45.079 | 0.000 *** | 19.320 | 21.078 | ||
| Henan | −0.036 | 0.150 | −0.007 | −0.243 | 0.808 | −0.330 | 0.257 | −0.408 | 0.235 | −0.044 | −1.733 | 0.083 | −0.869 | 0.054 |
| Zhejiang | 0.484 | 0.155 | 0.096 | 3.113 | 0.002 ** | 0.179 | 0.788 | 4.254 | 0.244 | 0.459 | 17.427 | 0.000 *** | 3.775 | 4.733 |
| 66–70 | −0.067 | 0.187 | −0.013 | −0.360 | 0.719 | −0.433 | 0.299 | 0.406 | 0.293 | 0.043 | 1.383 | 0.167 | −0.170 | 0.981 |
| 71–75 | 0.029 | 0.196 | 0.005 | 0.148 | 0.882 | −0.355 | 0.413 | 0.436 | 0.308 | 0.043 | 1.417 | 0.157 | −0.167 | 1.039 |
| 76–80 | −0.311 | 0.203 | −0.052 | −1.528 | 0.127 | −0.710 | 0.088 | −0.218 | 0.320 | −0.020 | −0.682 | 0.495 | −0.845 | 0.409 |
| Above 80 | −1.278 | 0.242 | −0.164 | −5.274 | 0.000 ** | −1.753 | −0.803 | −1.324 | 0.381 | −0.092 | −3.477 | 0.001 ** | −2.071 | −0.577 |
| Primary school | −0.005 | 0.127 | −0.001 | −0.043 | 0.966 | −0.254 | 0.243 | 0.184 | 0.199 | 0.020 | 0.924 | 0.356 | −0.207 | 0.575 |
| Junior high school | 0.914 | 0.175 | 0.130 | 5.214 | 0.000 *** | 0.570 | 1.258 | 1.151 | 0.275 | 0.089 | 4.179 | 0.000 *** | 0.611 | 1.691 |
| Senior high school | 1.529 | 0.376 | 0.096 | 4.066 | 0.000 *** | 0.792 | 2.267 | 2.182 | 0.591 | 0.075 | 3.693 | 0.000 *** | 1.023 | 3.341 |
| College | 1.882 | 0.551 | 0.081 | 3.417 | 0.001 ** | 0.802 | 2.963 | 3.267 | 0.866 | 0.077 | 3.773 | 0.000 *** | 1.569 | 4.965 |
| Migrant-workers | 1.689 | 0.279 | 0.149 | 6.062 | 0.000 *** | 1.143 | 2.236 | −2.259 | 0.438 | −0.108 | −5.157 | 0.000 *** | −3.118 | −1.400 |
| The self-employed | 1.144 | 0.310 | 0.088 | 3.686 | 0.000 *** | 0.535 | 1.753 | 0.810 | 0.488 | 0.034 | 1.660 | 0.097 | −0.147 | 1.767 |
| Retirees | −0.099 | 0.183 | −0.013 | −0.544 | 0.587 | −0.457 | 0.259 | 0.651 | 0.287 | 0.047 | 2.270 | 0.023 * | 0.088 | 1.214 |
| Others | 0.282 | 0.249 | 0.027 | 1.135 | 0.257 | −0.206 | 0.771 | 0.158 | 0.391 | 0.008 | 0.404 | 0.686 | −0.609 | 0.925 |
| Distance from home to healthcare institutions | −0.675 | 0.158 | −0.103 | −4.263 | 0.000 *** | −0.986 | −0.364 | −1.280 | 0.249 | −0.107 | −5.146 | 0.000 *** | −1.768 | −0.792 |
| 5001–10,000 RMB | 0.047 | 0.188 | 0.007 | 0.249 | 0.803 | −0.322 | 0.416 | −0.332 | 0.296 | −0.027 | −1.122 | 0.262 | −0.911 | 0.248 |
| 10,001–15,000 RMB | −0.001 | 0.168 | 0.000 | −0.008 | 0.994 | −0.331 | 0.329 | −0.135 | 0.264 | −0.013 | −0.510 | 0.610 | −0.653 | 0.384 |
| 15,001–20,000 RMB | 0.167 | 0.236 | 0.019 | 0.708 | 0.479 | −0.296 | 0.630 | 0.348 | 0.371 | 0.021 | 0.938 | 0.348 | −0.380 | 1.076 |
| >20,000 RMB | 0.536 | 0.158 | 0.106 | 3.382 | 0.001 ** | 0.225 | 0.847 | 0.306 | 0.249 | 0.033 | 1.230 | 0.219 | −0.182 | 0.795 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
He, Z.; Cheng, Z.; Shao, T.; Liu, C.; Shao, P.; Bishwajit, G.; Feng, D.; Feng, Z. Factors Influencing Health Knowledge and Behaviors among the Elderly in Rural China. Int. J. Environ. Res. Public Health 2016, 13, 975. https://doi.org/10.3390/ijerph13100975
He Z, Cheng Z, Shao T, Liu C, Shao P, Bishwajit G, Feng D, Feng Z. Factors Influencing Health Knowledge and Behaviors among the Elderly in Rural China. International Journal of Environmental Research and Public Health. 2016; 13(10):975. https://doi.org/10.3390/ijerph13100975
Chicago/Turabian StyleHe, Zhifei, Zhaohui Cheng, Tian Shao, Chunyan Liu, Piaopiao Shao, Ghose Bishwajit, Da Feng, and Zhanchun Feng. 2016. "Factors Influencing Health Knowledge and Behaviors among the Elderly in Rural China" International Journal of Environmental Research and Public Health 13, no. 10: 975. https://doi.org/10.3390/ijerph13100975
APA StyleHe, Z., Cheng, Z., Shao, T., Liu, C., Shao, P., Bishwajit, G., Feng, D., & Feng, Z. (2016). Factors Influencing Health Knowledge and Behaviors among the Elderly in Rural China. International Journal of Environmental Research and Public Health, 13(10), 975. https://doi.org/10.3390/ijerph13100975