
Adverse Events in Treating Smear-Positive Tuberculosis Patients in China

Abstract
:1. Introduction
2. Materials and Methods
2.1. Sampling Method
2.2. Data Collection
- (I)
- Liver injury, including elevated transaminase and jaundice.
- (II)
- Gastrointestinal reactions, including nausea, vomiting, loss of appetite and diarrhea.
- (III)
- Renal impairment, including decline of renal function, positive urine protein and renal failure.
- (IV)
- Blood system damage, including anemia, leukopenia, thrombocytopenia, and pancytopenia.
- (V)
- Auditory nerve damage, including tinnitus, dizziness and hearing loss.
- (VI)
- Optic nerve damage, including blurred vision, constriction of visual field, and color vision disorder.
- (VII)
- Drug allergy, including pruritus, rash, exfoliative dermatitis, and anaphylactic shock.
- (VIII)
- Neuropsychiatric symptoms, including sleep disorders, dizziness, headache, irritability, delirium and epilepsy.
- (IX)
- Joints or muscle pain, including arthralgia and Achilles pain.
- (X)
- Electrolyte abnormalities.
- (XI)
- Thyroid dysfunction.
- (XII)
- Other adverse events.
2.3. Bacteriological Examinations
2.4. Anti-Tuberculosis Therapy
2.5. Statistical Analysis
3. Results
3.1. Socio-Demographics Characteristics

{kind=link}
| Characteristics | Patients without AE | Patients with AE | Overall | p |
|---|---|---|---|---|
| No. (%) | No. (%) | No. (%) | ||
| Age, years | 1625 (100) | 460 (100) | 2085 (100) | |
| Mean ± SD | 42.3 ± 17.3 | 45.6 ± 17.3 | 43.1 ± 17.3 | |
| ≤18 | 52 (3.2) | 13 (2.8) | 65 (3.1) | 0.05 |
| 19–39 | 708 (43.6) | 167 (36.3) | 875 (42.0) | † § |
| 40–59 | 572 (35.2) | 180 (39.1) | 752 (36.1) | |
| ≥60 | 293 (18.0) | 100 (21.7) | 393 (18.8) | |
| Sex | 1629 (100) | 462 (100) | 2091 (100) | |
| Male | 1176 (72.2) | 335 (72.5) | 1511 (72.3) | 0.74 |
| Female | 453 (27.8) | 127 (27.5) | 580 (27.7) | †¶ |
| Treatment history | 1629 (100) | 462 (100) | 2091 (100) | |
| New cases | 1379 (84.7) | 398 (86.1) | 1777 (85.0) | 0.29 |
| Previously treated | 250 (15.3) | 64 (13.9) | 314 (15.0) | † |
| Ethnic groups | 1629 (100) | 462 (100) | 2091 (100) | |
| Han | 1331 (81.7) | 364 (78.8) | 1695 (81.1) | 0.13 |
| Minority | 298 (18.3) | 98 (21.2) | 396 (18.9) | § |
| Level of education | 1629 (100) | 462 (100) | 2091 (100) | |
| Illiteracy or primary school | 549 (33.7) | 187 (40.5) | 736 (35.2) | <0.01 |
| Middle school or higher | 1080 (66.3) | 275 (59.5) | 1355 (64.8) | † § |
| Region | 1629 (100) | 462 (100) | 2091 (100) | |
| East | 514 (31.6) | 144 (31.2) | 658 (31.5) | <0.01 |
| Center | 681 (41.8) | 143 (31.0) | 824 (39.4) | † § |
| West | 434 (26.6) | 175 (37.9) | 609 (29.1) | |
| Smoking status | 1594 (100) | 459 (100) | 2053 (100) | |
| Never smokers | 760 (47.7) | 195 (42.5) | 955 (46.5) | 0.02 |
| Ex-smokers | 573 (36.0) | 168 (36.6) | 741 (36.1) | †¶ |
| Current smokers | 261 (16.4) | 96 (20.9) | 357 (17.4) | |
| Drinking status | 1593 (100) | 458 (100) | 2051 (100) | |
| Never drinkers | 894 (56.1) | 239 (52.2) | 1133 (55.2) | 0.24 |
| Ex-drinkers | 569 (35.7) | 178 (38.9) | 747 (36.4) | † |
| Current drinkers | 130 (8.2) | 41 (9.0) | 171 (8.3) | |
| DOT distance, kilometer | 1588 (100) | 459 (100) | 2047 (100) | |
| <1 | 547 (34.5) | 118 (25.7) | 665 (32.5) | <0.01 |
| 1–5 | 566 (35.6) | 189 (41.2) | 755 (36.9) | † |
| 6–10 | 276 (17.4) | 79 (17.2) | 355 (17.3) | |
| >10 | 199 (12.5) | 73 (15.9) | 272 (13.3) | |
| DOT supervisor | 1591 (100) | 452 (100) | 2043 (100) | |
| Doctors | 889 (55.9) | 251 (55.5) | 1140 (55.8) | 0.91 |
| Others | 679 (42.7) | 194 (42.9) | 873 (42.7) | |
| Nobody | 23 (1.4) | 7 (1.6) | 30 (1.5) | |
| TB knowledge | 1629 (100) | 462 (100) | 2091 (100) | |
| Mean ± SD | 11.3 ± 3.6 | 10.4 ± 3.8 | 11.1 ± 3.6 | |
| ≤5 | 134 (8.2) | 63 (13.6) | 197 (9.4) | <0.01 |
| 6–10 | 458 (28.1) | 146 (31.6) | 604 (28.9) | †§ |
| >10 | 1037 (63.7) | 253 (54.8) | 1290 (61.7) | |
| Symptom score | 1629 (100) | 462 (100) | 2091 (100) | |
| Mean ± SD | 4.8 ± 2.9 | 5.7 ± 3.5 | 5.0 ± 3.1 | |
| ≤5 | 1082 (66.4) | 247 (53.5) | 1329 (63.6) | <0.01 |
| 6–10 | 476 (29.2) | 168 (36.4) | 644 (30.8) | § |
| >10 | 71 (4.4) | 47 (10.2) | 118 (5.6) | |
| DST | 1041 (100) | 333 (100) | 1374 (100) | |
| Sensitive | 691 (66.4) | 232 (69.7) | 923 (67.2) | 0.17 |
| Resistant | 350 (33.6) | 101 (30.3) | 451 (32.8) |
3.2. Clinical Characteristics
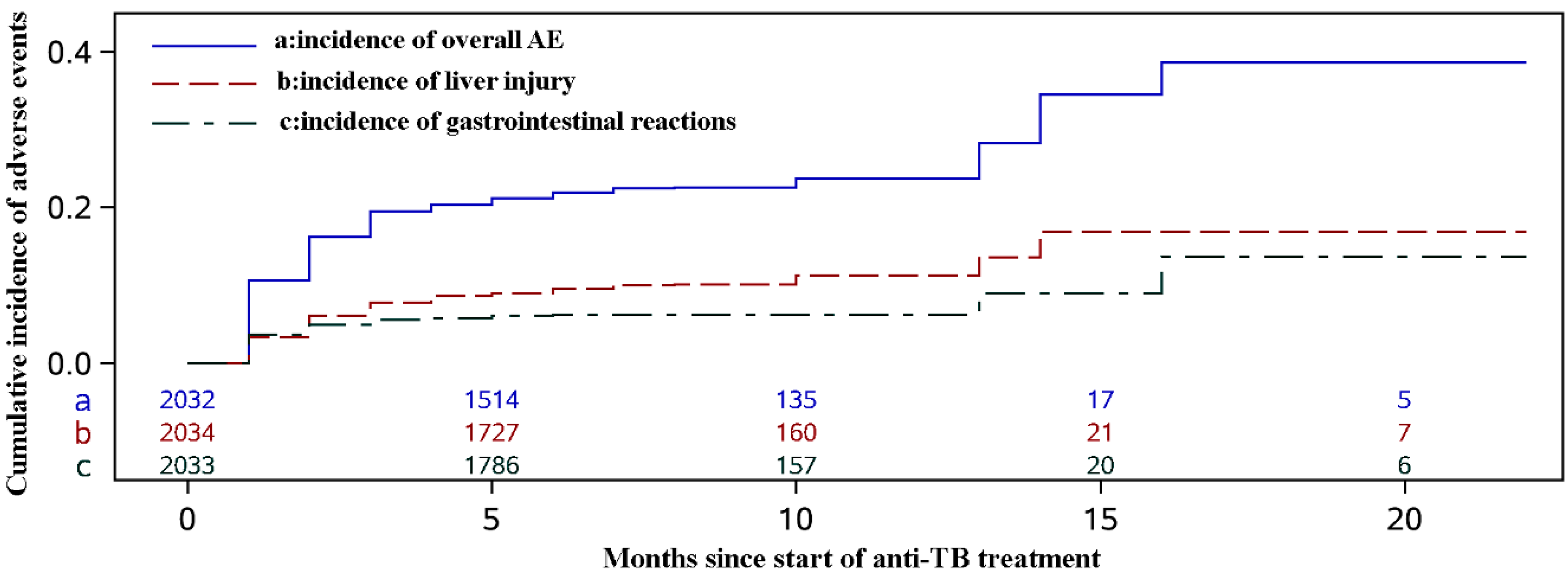
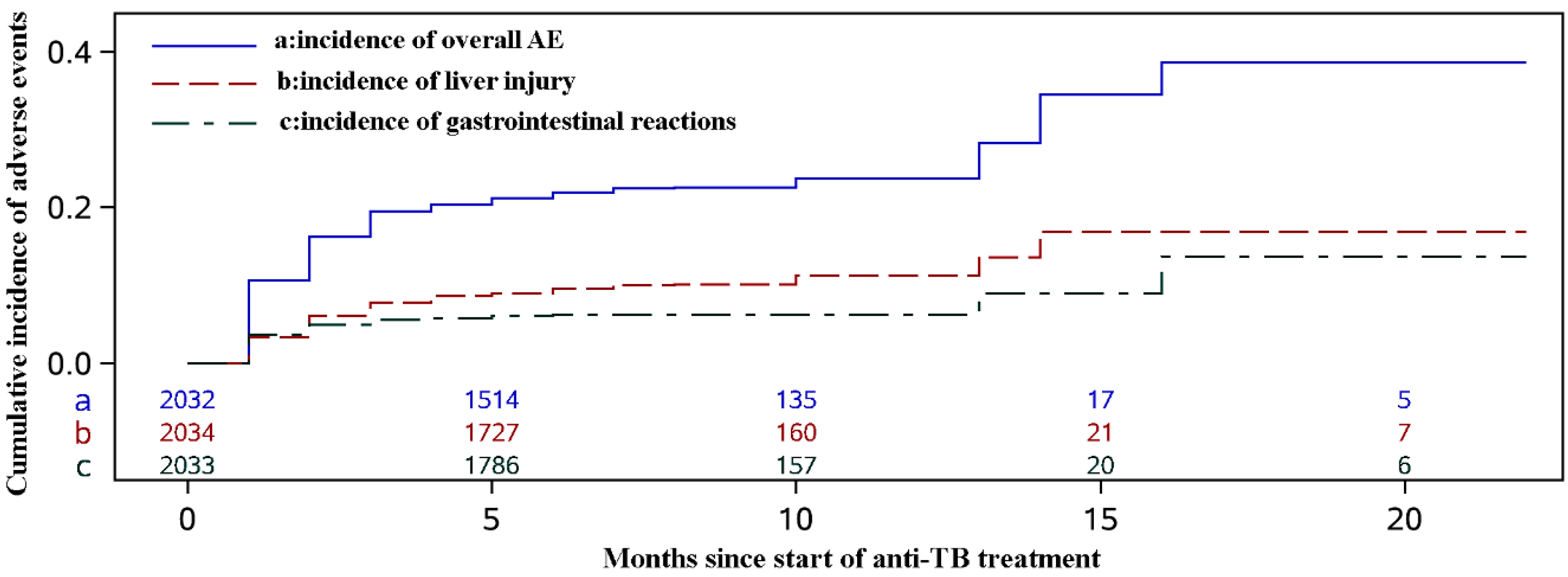
3.3. Adverse Events
| AE Groups | No. | % |
|---|---|---|
| Liver injury * | 205 | 36.94 |
| Gastrointestinal reactions * | 132 | 23.78 |
| Renal impairment | 28 | 5.05 |
| Blood system damage | 18 | 3.24 |
| Auditory nerve damage | 4 | 0.72 |
| Optic nerve damage | 15 | 2.70 |
| Drug allergy | 69 | 12.43 |
| Neuropsychiatric symptoms | 37 | 6.67 |
| Joints/Muscle pain | 35 | 6.31 |
| Electrolyte abnormalities | 1 | 0.18 |
| Thyroid dysfunction | 0 | 0 |
| Other adverse events | 11 | 1.98 |
3.4. Risk Factors for Adverse Events during Anti-TB Treatment
| Characteristics | Overall AE | Liver Injury | Gastrointestinal Reactions | ||||||
|---|---|---|---|---|---|---|---|---|---|
| HR | 95% CI | p | HR | 95% CI | p | HR | 95% CI | p | |
| Region | |||||||||
| East | 1.33 | 0.97–1.83 | 0.07 | 1.91 | 1.35–2.71 | < 0.01 | 0.34 | 0.19–0.62 | <0.01 |
| West | 1.82 | 1.35–2.45 | < 0.01 | 1.54 | 1.06–2.23 | 0.02 | 0.77 | 0.52–1.14 | 0.19 |
| Center | ref | ref | ref | ||||||
| Age, years | |||||||||
| ≤18 | – | – | – | 1.50 | 0.75–3.00 | 0.25 | – | – | – |
| 40–59 | – | – | – | 0.79 | 0.57–1.08 | 0.14 | – | – | – |
| ≥60 | – | – | – | 0.50 | 0.32–0.80 | < 0.01 | – | – | – |
| 19–39 | ref | ||||||||
| Sex (Male) | – | – | 1.66 | 1.08–2.54 | 0.02 | – | – | – | |
| Education level | – | – | – | – | – | 0.44 | 0.30–0.65 | <0.01 | |
| Smoking status | |||||||||
| ex-smokers | 1.20 | 0.94–1.55 | 0.15 | 1.27 | 0.87–1.85 | 0.21 | – | – | – |
| current smokers | 1.64 | 1.23–2.18 | < 0.01 | 1.71 | 1.12–2.59 | 0.01 | – | – | – |
| never smokers | ref | ref | |||||||
| Symptom score | 1.05 | 1.02–1.09 | 0.01 | – | – | – | 1.09 | 1.03–1.14 | <0.01 |
| TB Knowledge | 0.69 | 0.60–0.81 | < 0.01 | 0.79 | 0.65–0.97 | 0.02 | 0.66 | 0.52–0.84 | <0.01 |
4. Discussion
5. Conclusions
Supplementary Files
Supplementary File 1Acknowledgments
Author Contributions
Conflicts of Interest
References
- Global Tuberculosis Control: Who Report 2011; World Health Organization: Geneva, Switzerland, 2011.
- Technical Guidance Group of the Fifth National TB Epidemiological Survey; The Office of the Fifth National TB Epidemiological Survey. The Fifth National Tuberculosis Epidemiological Survey in 2010. J. Chin. Antituberc. Assoc. 2012, 34, 485–508. [Google Scholar]
- Global Tuberculosis Report 2014; 9240693297; World Health Organization: Geneva, Switzerland, 2014.
- CDC. Update: Fatal and severe liver injuries associated with rifampin and pyrazinamide for latent tuberculosis infection, and revisions in American Thoracic Society/CDC Recommendations-United States, 2001. MMWR Morb. Mortal. Wkly. Rep. 2001, 50, 733–735. [Google Scholar]
- Furin, J.; Mitnick, C.; Shin, S.; Bayona, J.; Becerra, M.; Singler, J.; Alcantara, F.; Castaneda, C.; Sanchez, E.; Acha, J. Occurrence of serious adverse effects in patients receiving community-based therapy for multidrug-resistant tuberculosis. Int. J. Tuberc. Lung Dis. 2001, 5, 648–655. [Google Scholar] [PubMed]
- Lorent, N.; Sebatunzi, O.; Mukeshimana, G.; Van den Ende, J.; Clerinx, J. Incidence and risk factors of serious adverse events during antituberculous treatment in rwanda: A prospective cohort study. PloS ONE 2011, 6. [Google Scholar] [CrossRef] [PubMed]
- Shang, P.; Xia, Y.; Liu, F.; Wang, X.; Yuan, Y.; Hu, D.; Tu, D.; Chen, Y.; Deng, P.; Cheng, S.; et al. Incidence, clinical features and impact on anti-tuberculosis treatment of anti-tuberculosis drug induced liver injury (ATLI) in China. PLoS ONE 2011, 6. [Google Scholar] [CrossRef] [PubMed]
- Lv, X.; Tang, S.; Xia, Y.; Wang, X.; Yuan, Y.; Hu, D.; Liu, F.; Wu, S.; Zhang, Y.; Yang, Z.; et al. Adverse reactions due to directly observed treatment strategy therapy in Chinese tuberculosis patients: A prospective study. PLoS ONE 2013, 8. [Google Scholar] [CrossRef] [PubMed]
- Carroll, M.; Lee, M.; Cai, Y.; Hallahan, C.; Shaw, P.; Min, J.; Goldfeder, L.; Alekseyev, V.; Grinkrug, S.; Kang, H. Frequency of adverse reactions to first-and second-line anti-tuberculosis chemotherapy in a Korean cohort. Int. J. Tuberc. Lung Dis. 2012, 16, 961–966. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Tu, D.H.; Li, B.; Yang, Z.B.; Wang, J.L.; Zhao, F.J.; Wang, Z.Z.; Zhang, Z.J. The incidence of the adverse reactions of the first-line anti-tuberculosis drugs in Beijing and its influence on the chemotherapy. J. Chin. Antituberc. Assoc. 2008, 4, 271–274. [Google Scholar]
- Xia, Y.Y.; Zhan, S.Y. Systematic review of anti-tuberculosis drug induced adverse reactions in China. Chin. J. Tuberc. Respir. Dis. 2007, 30, 419–423. [Google Scholar]
- Pubmed. Available online: http://www.ncbi.nlm.nih.gov/pubmed/ (accessed on 20 March 2015).
- Chang, K.C.; Leung, C.C.; Yew, W.W.; Lau, T.Y.; Tam, C.M. Hepatotoxicity of pyrazinamide: Cohort and case-control analyses. Am. J. Respir. Crit. Care Med. 2008, 177, 1391–1396. [Google Scholar] [CrossRef] [PubMed]
- Younossian, A.B.; Rochat, T.; Ketterer, J.P.; Wacker, J.; Janssens, J.P. High hepatotoxicity of pyrazinamide and ethambutol for treatment of latent tuberculosis. Eur. Respir. J. 2005, 26, 462–464. [Google Scholar] [CrossRef] [PubMed]
- Shu, C.; Lee, C.; Lee, M.; Wang, J.; Yu, C.; Lee, L. Hepatotoxicity due to first-line anti-tuberculosis drugs: A five-year experience in a Taiwan medical centre. Int. J. Tuberc. Lung Dis. 2013, 17, 934–939. [Google Scholar] [CrossRef] [PubMed]
- Leung, C.C.; Li, T.; Lam, T.H.; Yew, W.W.; Law, W.S.; Tam, C.M.; Chan, W.M.; Chan, C.K.; Ho, K.S.; Chang, K.C. Smoking and tuberculosis among the elderly in Hong Kong. Am. J. Respir. Crit. Care Med. 2004, 170, 1027–1033. [Google Scholar] [CrossRef] [PubMed]
- Guidelines for Implementing the National Tuberculosis Control Program in China (2008); Department of Disease Control, MOH; Department of Medical Administration, MOH; Chinese Center for Disease Control and Prevention: Beijing, China, 2008.
- Zheng, T.; Boffetta, P.; Boyle, P. Epidemiology and Biostatistics; The International Prevention Research Institute: Lyon, France, 2011; p. 563. [Google Scholar]
- Huang, M.Y.; Luo, D.; Liu, F.Y.; Li, J. Research on adverse drug reactions of anti-tuberculosis in Guangxi. Mod. Prev. Med. 2013, 40, 1146–1148. (In Chinese) [Google Scholar]
- Zaverucha-do-Valle, C.; Monteiro, S.P.; El-Jaick, K.B.; Rosadas, L.A.; Costa, M.J.; Quintana, M.S.; de Castro, L. The role of cigarette smoking and liver enzymes polymorphisms in anti-tuberculosis drug-induced hepatotoxicity in Brazilian patients. Tuberculosis (Edinb.) 2014, 94, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Lu, J.; Cheng, J.; Wang, L.; Matsubara, T.; Csanaky, I.L.; Klaassen, C.D.; Gonzalez, F.J.; Ma, X. Human PXR modulates hepatotoxicity associated with rifampicin and isoniazid co-therapy. Nat. Med. 2013, 19, 418–420. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.L.; Song, K.H.; Lee, J.H.; Lee, K.Y.; Kim, S.K. Rifampin-induced hypothyroidism without underlying thyroid disease. Thyroid 2007, 17, 793–795. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Zhang, H.; Ruan, Y.; Chin, D.P.; Xia, Y.; Cheng, S.; Chen, M.; Zhao, Y.; Jiang, S.; Du, X. Tuberculosis prevalence in China, 1990–2010; a longitudinal analysis of national survey data. Lancet 2014, 383, 2057–2064. [Google Scholar] [CrossRef]
- O’Malley, K.; Crooks, J.; Duke, E.; Stevenson, I.H. Effect of age and sex on human drug metabolism. Br. Med. J. 1971, 3, 607–609. [Google Scholar] [CrossRef] [PubMed]
- Archer, S.N.; Oster, H. How sleep and wakefulness influence circadian rhythmicity: Effects of insufficient and mistimed sleep on the animal and human transcriptome. J. Sleep Rec. 2015, 24, 476–493. [Google Scholar] [CrossRef] [PubMed]
- Przybylski, G.; Dabrowska, A.; Trzcinska, H. Alcoholism and other socio–demographic risk factors for adverse tb-drug reactions and unsuccessful tuberculosis treatment—Data from ten years' observation at the Regional Centre of Pulmonology, Bydgoszcz, Poland. Med. Sci. Monit. 2014, 20, 444–453. [Google Scholar] [PubMed]
- Hofman, M.; Morrow, G.R.; Roscoe, J.A.; Hickok, J.T.; Mustian, K.M.; Moore, D.F.; Wade, J.L.; Fitch, T.R. Cancer patients’ expectations of experiencing treatment-related side effects. Cancer 2004, 101, 851–857. [Google Scholar] [CrossRef] [PubMed]
- Shang, S.; Ordway, D.; Henao–Tamayo, M.; Bai, X.; Oberley-Deegan, R.; Shanley, C.; Orme, I.M.; Case, S.; Minor, M.; Ackart, D. Cigarette smoke increases susceptibility to tuberculosis—Evidence from in vivo and in vitro models. J. Infect. Dis. 2011, 203, 1240–1248. [Google Scholar] [CrossRef] [PubMed]
- Shaler, C.R.; Horvath, C.N.; McCormick, S.; Jeyanathan, M.; Khera, A.; Zganiacz, A.; Kasinska, J.; Stampfli, M.R.; Xing, Z. Continuous and discontinuous cigarette smoke exposure differentially affects protective TH1 immunity against pulmonary tuberculosis. PloS ONE 2013, 8. [Google Scholar] [CrossRef]
- Feng, Y.; Kong, Y.; Barnes, P.F.; Huang, F.-F.; Klucar, P.; Wang, X.; Samten, B.; Sengupta, M.; Machona, B.; Donis, R. Exposure to cigarette smoke inhibits the pulmonary T-cell response to influenza virus and mycobacterium tuberculosis. Infect. Immun. 2011, 79, 229–237. [Google Scholar] [CrossRef] [PubMed]
- Chan, E.D.; Kinney, W.H.; Honda, J.R.; Bishwakarma, R.; Gangavelli, A.; Mya, J.; Bai, X.; Ordway, D.J. Tobacco exposure and susceptibility to tuberculosis: Is there a smoking gun? Tuberculosis 2014, 94, 544–550. [Google Scholar] [CrossRef] [PubMed]
- National TB Control Program Implementation Guide in China (2008 Edition); Ministry of Health of PRC: Beijing, China, 2009.
- Dick, J.; Lombard, C. Shared vision—A health education project designed to enhance adherence to anti-tuberculosis treatment [planning and practice]. Int. J. Tuberc. Lung Dis. 1997, 1, 181–186. [Google Scholar] [PubMed]
- Treatment of Tuberculosis: Guidelines; 9241547839; World Health Organization: Geneva, Switzerland, 2009; p. 420.
- Chamorro, J.G.; Castagnino, J.P.; Musella, R.M.; Nogueras, M.; Aranda, F.M.; Frías, A.; Visca, M.; Aidar, O.; Perés, S.; Larrañaga, G.F. Sex, ethnicity, and slow acetylator profile are the major causes of hepatotoxicity induced by antituberculosis drugs. J. Gastroenterol. Hepatol. Res. 2013, 28, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Abbasi, M.A.; Ahmed, N.; Suleman, A.; Zaman, H.; Tariq, S.; Anwar, S.A.; Khan, N. Common risk factors for the development of ant-tuberculosis treatment induced hepatotoxicity. J. Ayub. Med. Coll. Abbottabad. 2014, 26, 384–388. [Google Scholar] [PubMed]
- Xiang, Y.; Ma, L.; Wu, W.D.; Liu, W.; Li, Y.G.; Zhu, X.; Wang, Q.; Ma, J.F.; Cao, M.Q.; Wang, Q.; et al. The incidence of liver injury in Uyghur patients treated for TB in Xinjiang Uyghur Autonomous Region, China, and its association with hepatic enzyme polymorphisms NAT2, CYP2E1, GSTM1 and GSTT1. PloS ONE 2014, 9. [Google Scholar] [CrossRef] [PubMed]
- Sistanizad, M.; Azizi, E.; Khalili, H.; Hajiabdolbaghi, M.; Gholami, K.; Mahjub, R. Antituberculosis drug-induced hepatotoxicity in Iranian tuberculosis patients: Role of isoniazid metabolic polymorphism. Iran. J. Pharm. Res. 2011, 10, 633–639. [Google Scholar] [PubMed]
- Yee, D.; Valiquette, C.; Pelletier, M.; Parisien, I.; Rocher, I.; Menzies, D. Incidence of serious side effects from first–line antituberculosis drugs among patients treated for active tuberculosis. Am. J. Respir. Crit. Care Med. 2003, 167, 1472–1477. [Google Scholar] [CrossRef] [PubMed]
- Schaberg, T.; Rebhan, K.; Lode, H. Risk factors for side-effects of isoniazid, rifampin and pyrazinamide in patients hospitalized for pulmonary tuberculosis. Eur. Respir. J. 1996, 9, 2026–2030. [Google Scholar] [CrossRef] [PubMed]
- Padmapriyadarsini, C.; Bhavani, P.K.; Tang, A.; Kumar, H.; Ponnuraja, C.; Narendran, G.; Hannah, E.; Ramesh, C.; Chandrasekar, C.; Wanke, C.; et al. Early changes in hepatic function among HIV-tuberculosis patients treated with nevirapine or efavirenz along with rifampin-based anti-tuberculosis therapy. Int. J. Infect. Dis. 2013, 17, e1154–e1159. [Google Scholar] [CrossRef] [PubMed]
- Mahmud, O.; Dates, C.; Akil, L.; Ahmad, H.A. HIV and tuberculosis trends in the United States and select Sub-Saharan Africa countries. Int. J. Environ. Res. Public Health 2011, 8, 2524–2532. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, T.; Du, J.; Yin, X.; Xue, F.; Liu, Y.; Li, R.; Luo, C.; Li, L.; Li, X. Adverse Events in Treating Smear-Positive Tuberculosis Patients in China. Int. J. Environ. Res. Public Health 2016, 13, 86. https://doi.org/10.3390/ijerph13010086
Zhang T, Du J, Yin X, Xue F, Liu Y, Li R, Luo C, Li L, Li X. Adverse Events in Treating Smear-Positive Tuberculosis Patients in China. International Journal of Environmental Research and Public Health. 2016; 13(1):86. https://doi.org/10.3390/ijerph13010086
Chicago/Turabian StyleZhang, Tao, Jian Du, Xiaoyan Yin, Fuzhong Xue, Yanxun Liu, Runzi Li, Cheng Luo, Liang Li, and Xiujun Li. 2016. "Adverse Events in Treating Smear-Positive Tuberculosis Patients in China" International Journal of Environmental Research and Public Health 13, no. 1: 86. https://doi.org/10.3390/ijerph13010086
APA StyleZhang, T., Du, J., Yin, X., Xue, F., Liu, Y., Li, R., Luo, C., Li, L., & Li, X. (2016). Adverse Events in Treating Smear-Positive Tuberculosis Patients in China. International Journal of Environmental Research and Public Health, 13(1), 86. https://doi.org/10.3390/ijerph13010086